
Abstract
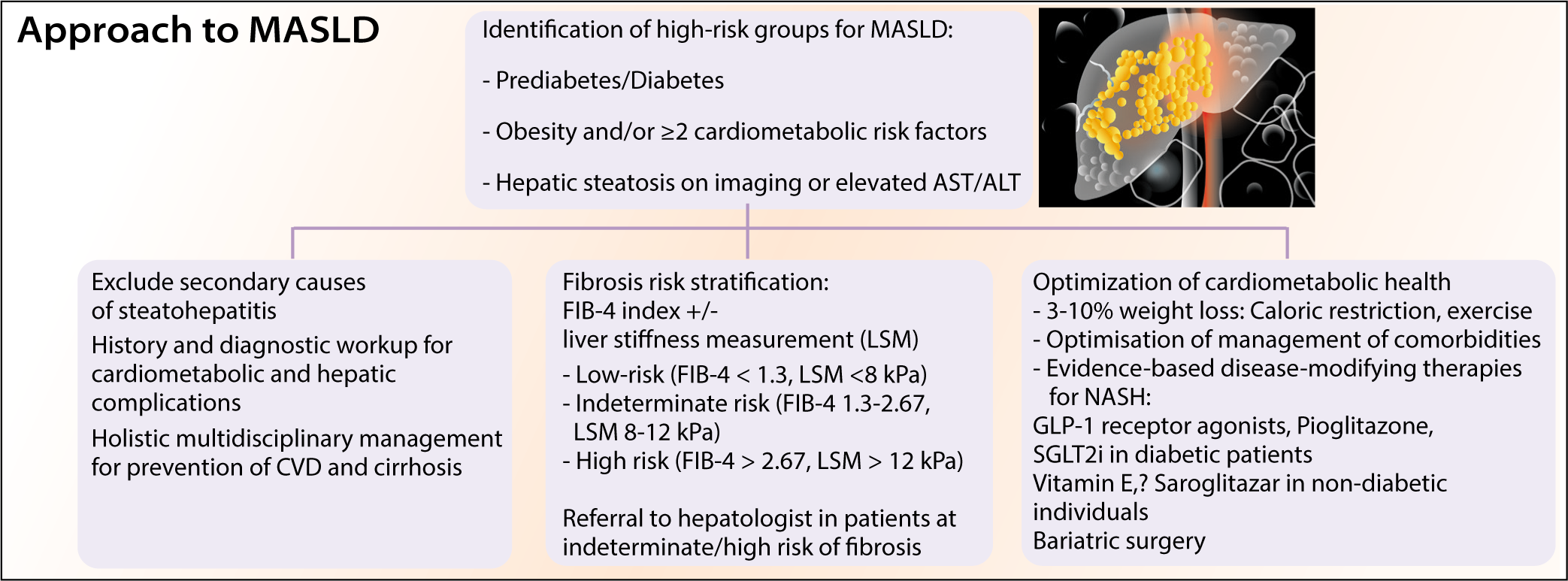
Metabolic dysfunction–associated steatotic liver disease (MASLD) has attained epidemic proportions in recent years, affecting nearly one-third of the general population and two-thirds of patients with type 2 diabetes (T2DM). It encompasses a wide spectrum of pathophysiological entities, ranging from simple steatosis to steatohepatitis to fibrosis and cirrhosis, with both hepatic and extrahepatic implications, including cardiovascular disease. The possibility of MASLD should be considered in high-risk groups such as T2DM, obesity, metabolic syndrome, polycystic ovarian syndrome (PCOS), etc., with/ without evidence of hepatic steatosis on imaging or persistently raised liver enzymes. Initial assessment should include a comprehensive evaluation of comorbidities, exclusion of secondary causes of steatosis, and fibrosis risk stratification. The presence of NASH and fibrosis is the most important predictor of adverse clinical outcomes, and non-invasive risk assessment has been an area of intense research in recent decades. FIB-4 can be used as a primary tool to effectively rule out significant fibrosis, followed by vibration-controlled transient elastography (VCTE) or enhanced liver fibrosis (ELF) tests as secondary tools if the FIB-4 score is indeterminate or high. The management of MASLD patients has shifted from a hepatocentric to a multicentric approach, with a focus on lifestyle interventions, disease-modifying pharmacotherapy in selected patients, and optimized management of comorbidities and complications.
Get full access to this article
View all access options for this article.