
Abstract
Introduction:
Chin projection and symmetry are key determinants of lower facial harmony. Intraoral chin augmentation with alloplastic implants offers a scarless approach but presents challenges related to contamination, implant stability, mental nerve preservation and soft-tissue management. Variability in surgical technique may contribute to complications such as malposition and infection. This study proposes a standardised 14-point framework to enhance safety, predictability and aesthetic outcomes in intraoral chin augmentation.
Materials and Methods:
A prospective study was conducted on 30 patients undergoing intraoral chin augmentation over two years. All procedures adhered to a structured 14-point protocol incorporating preoperative oral optimisation, controlled subperiosteal dissection, rigid implant fixation, mentalis muscle re-approximation and standardised postoperative care. Implant selection was guided by gender-specific aesthetic preferences, with Hanson’s extended anatomical implants predominantly used in males and concave back button or customised implants in females. Outcomes were assessed over a minimum of one-year follow-up period.
Results:
The study included 18 females and 12 males. All procedures were completed successfully. One patient experienced transient postoperative swelling with painful mouth opening, which resolved spontaneously. No infections, implant displacement, extrusion, sensory disturbances or asymmetry were observed. Recovery time ranged from 5 to 7 days and all patients reported high satisfaction with aesthetic outcomes.
Conclusions:
The 14-point framework provides a safe, reproducible and gender-sensitive approach to intraoral chin augmentation, yielding stable, scar-free and predictable results with minimal complications.
Keywords
Introduction
The chin’s position, projection and symmetry are critical determinants of overall facial aesthetics and harmony, significantly influencing both frontal and profile facial appearance.1,2 Intraoral chin augmentation with alloplastic implants has become an integral adjunct in lower facial contouring, addressing microgenia, mandibular deficiency and profile disharmony in a predictable and minimally invasive manner. Chin augmentation is commonly performed to correct microgenia and retrognathia, providing a stronger, more defined jawline and improving overall facial balance.2–6
Intraoral chin augmentation using alloplastic implants is a well-established technique for enhancing lower facial balance; however, its proximity to the oral microbiome, dentition and regional neurovascular structures introduces unique safety and longevity concerns not encountered with other facial implant sites.
Current surgical modalities for chin augmentation include alloplastic implant placement and osteotomy-based procedures.7,8 Alloplastic chin implants, commonly fabricated from silicone, polytetrafluoroethylene or porous polyethylene, provide a relatively quick and customisable option for augmenting the chin’s bony framework.1,7,8 These implants may be placed through either an extraoral (submental) or intraoral incision.7,9
The intraoral approach offers the advantage of a scarless external appearance with direct subperiosteal access, thereby avoiding visible cutaneous scars.7–9 Reported complications include infection, implant displacement or extrusion, contour irregularities and delayed wound healing, events influenced by surgical approach, implant material and perioperative management (Figure 1).10–12
Despite a generally favourable safety profile, chin implant surgery remains associated with a spectrum of complications that may significantly affect aesthetic outcomes and patient satisfaction.10–13 Structured, multistep protocols have proven effective in other implant-based surgeries by reducing bacterial load and minimising biofilm formation, a leading cause of chronic implant failure and infection.14,15
Various Positions of the Implants Due to Malposition.
Although advantageous for scar concealment, the intraoral approach presents challenges related to bacterial contamination, soft-tissue handling, pocket design and mental nerve preservation. Improper incision planning, dissection or closure may increase the risk of mucosal dehiscence and implant exposure.11,12,16 Conversely, when combined with rigorous preoperative assessment, precise pocket creation and disciplined postoperative care, intraoral placement can provide stable implant positioning with high patient acceptance and minimal visible sequelae.16–18
Given the interplay of aesthetic goals, biomaterial behaviour and mandibular anatomy, there is a clear need for standardised, evidence-informed surgical frameworks. This article presents a systematic 14-point framework for safe intraoral chin implant placement, consolidating best practices from preoperative optimisation through postoperative care to improve predictability and reduce complications.
Materials and Methods
A prospective study was conducted on 30 patients undergoing intraoral chin augmentation using the proposed 14-point framework at C K Birla Hospital, Gurgaon, between January 2023 and January 2025. All patients were older than 18 years, had completed mandibular skeletal maturity and presented with concerns of microgenia, micrognathia or aesthetic chin deficiency with stable occlusion and adequate soft-tissue support. Patients with significant comorbidities, psychiatric illness, active infection, malocclusion, facial trauma or unwillingness to participate were excluded from the study.
Preoperative optimisation included thorough intraoral and extraoral examination, dental assessment and management of any oral infection. Patients were instructed to stop smoking at least two weeks before surgery and to abstain for 4–6 weeks postoperatively. Prophylactic antibiotics were administered at induction.
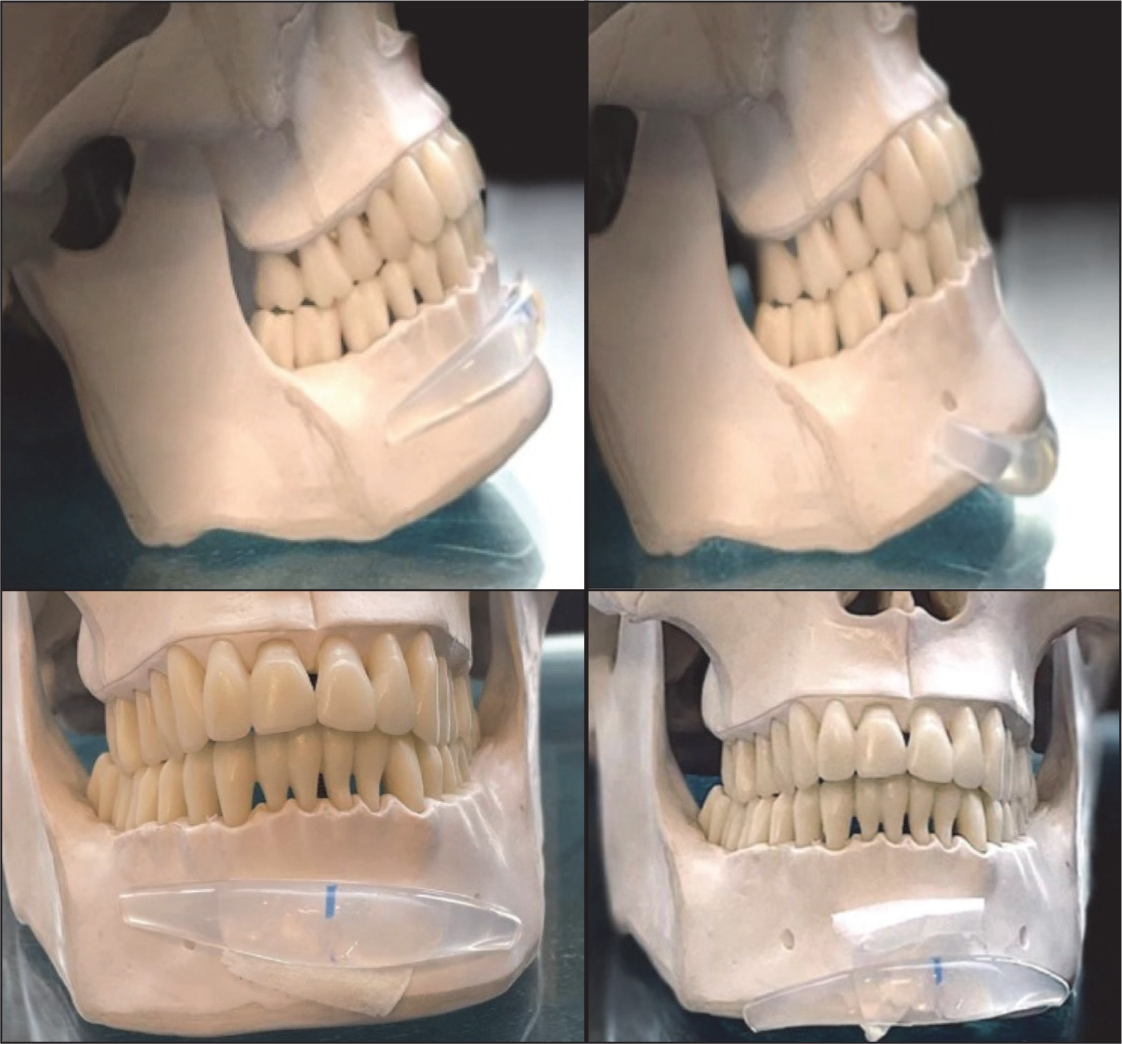
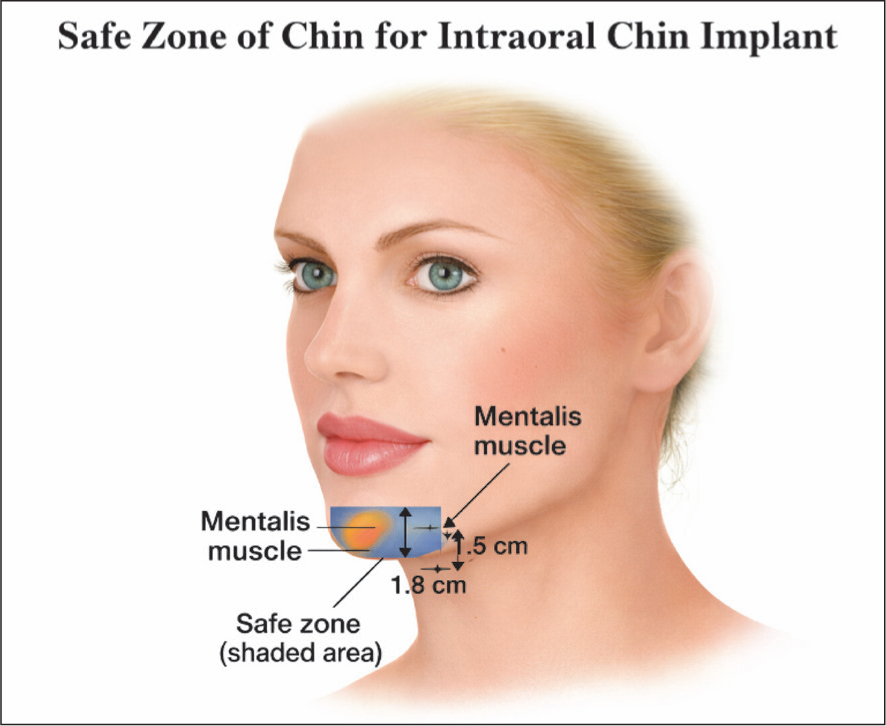
All procedures were performed via an intraoral approach. The incision was placed approximately 1–1.5 cm anterior to the gingivobuccal sulcus to allow adequate exposure while minimising contamination and soft-tissue trauma (Figures 2 and 3).
Safe Zone of Intraoral Chin Implant-preserving the Mental Nerve.
Preoperative Marking of the Chin Implant: AB = 4 cm, BC = 2 cm.

Subperiosteal dissection was performed in a controlled, atraumatic manner with meticulous haemostasis. The inferior extent of dissection was limited to the inferior mandibular border to prevent implant migration.
The implant pocket was irrigated with a triple-antibiotic solution. Before implant placement, both surgeon and assistant changed to powder-free gloves and the implant was placed promptly after opening to minimise contamination. Implants were positioned with precise midline orientation and secured using titanium screws to achieve rigid fixation.
Following confirmation of symmetry and stability, the mentalis muscle was meticulously re-approximated to prevent postoperative chin ptosis, lower lip incompetence and soft-tissue deformity. Layered closure was performed and postoperative antibiotics were continued for seven days with strict oral hygiene instructions.
Gender-specific aesthetic preferences guided implant selection. Female patients typically preferred a softer, concave, V-shaped chin contour, whereas male patients favoured broader, more prominent mandibular projection. Accordingly, two silicone implant designs were used: The Hansen extended anatomical chin implant (SHO01), predominantly in males and the concave button chin implant (SCH05), primarily in females (Figure 4). In selected female patients, Hansen implants were customised intraoperatively to achieve the desired projection.
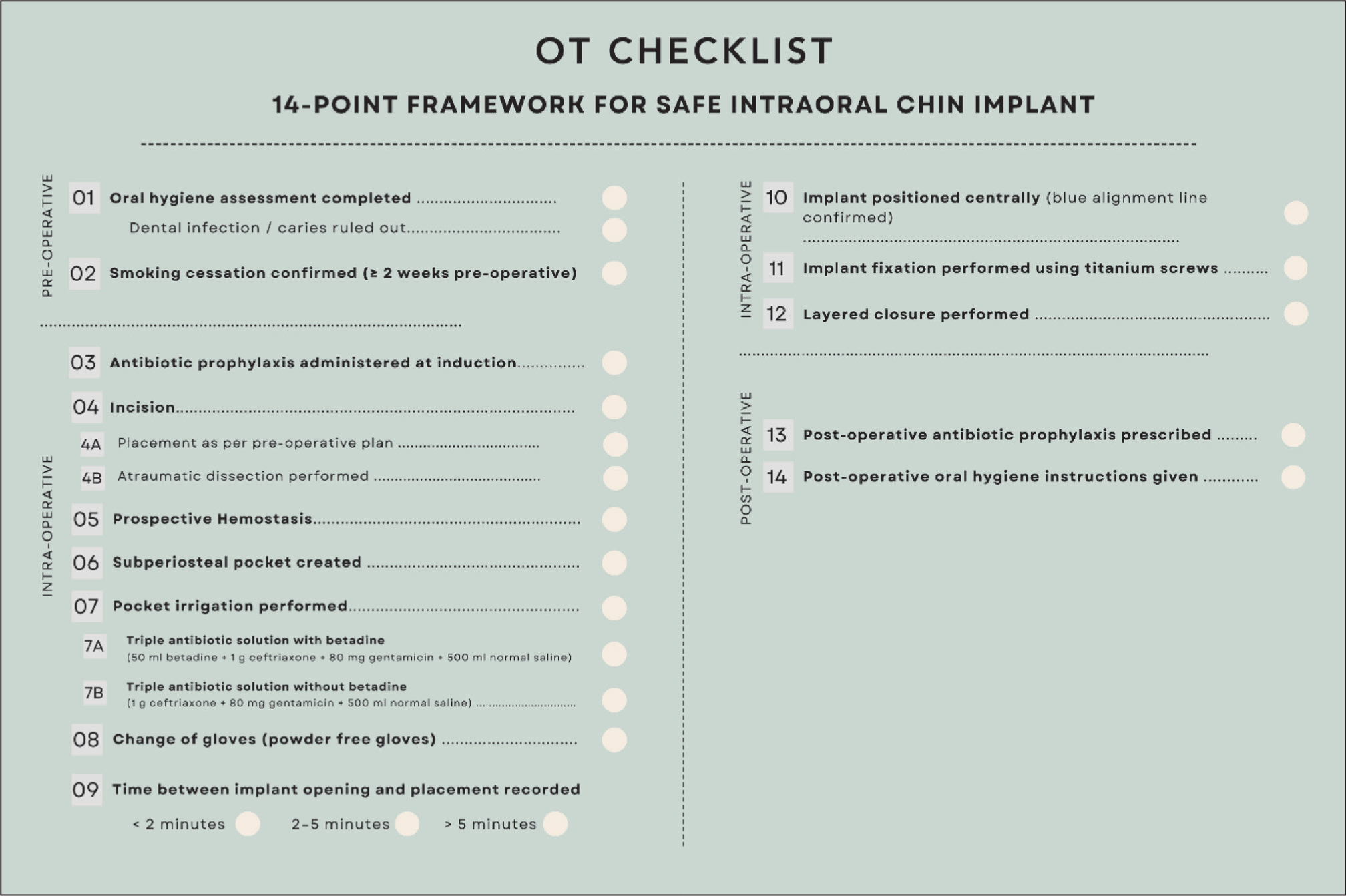
Presenting here the safety checklist for the 14-point framework for intraoral chin implants (Figure 5).
Safety Checklist for Intra-oral Chin Implants.
Results
All 30 patients underwent successful intraoral chin augmentation using the standardised 14-point framework. The cohort included 18 females and 12 males. All male patients received Hanson’s anatomical implants. Among female patients, 16 received concave back button chin implants, while two underwent customised Hanson’s anatomical implant placement.
Patients were evaluated for postoperative swelling, infection, painful mouth opening, malposition, paraesthesia, asymmetry, extrusion and need for revision surgery. One patient experienced transient swelling with painful mouth opening, which resolved spontaneously within three weeks. No infections, implant displacement, extrusion or sensory deficits were observed.
All patients reported high satisfaction with aesthetic outcomes. The recovery period ranged from 5 to 7 days. At one-year follow-up, none demonstrated implant palpability, displacement or asymmetry (Figures 6–10).
26 Years Old Female Underwent Concave Back Button Chin Implant, Before Surgery and One Month Post OP.

38 Years Old Patient, Preoperative Pic and Six Months Post Operative Picture, After Using Hanson Anatomical Implant.

41 Years Old Patient, Preoperative Pic and Nine Months Post Operative Picture, After Using Hanson Anatomical Implant.

29 Years Female, Shared a Preoperative Picture Before her First Surgery, Which She Performed Elsewhere and Final Postoperative Picture Taken at One-year Post Second Surgery. We used a Customised Hanson Anatomical Implant. Front Profile Depicting the Dramatic Difference.

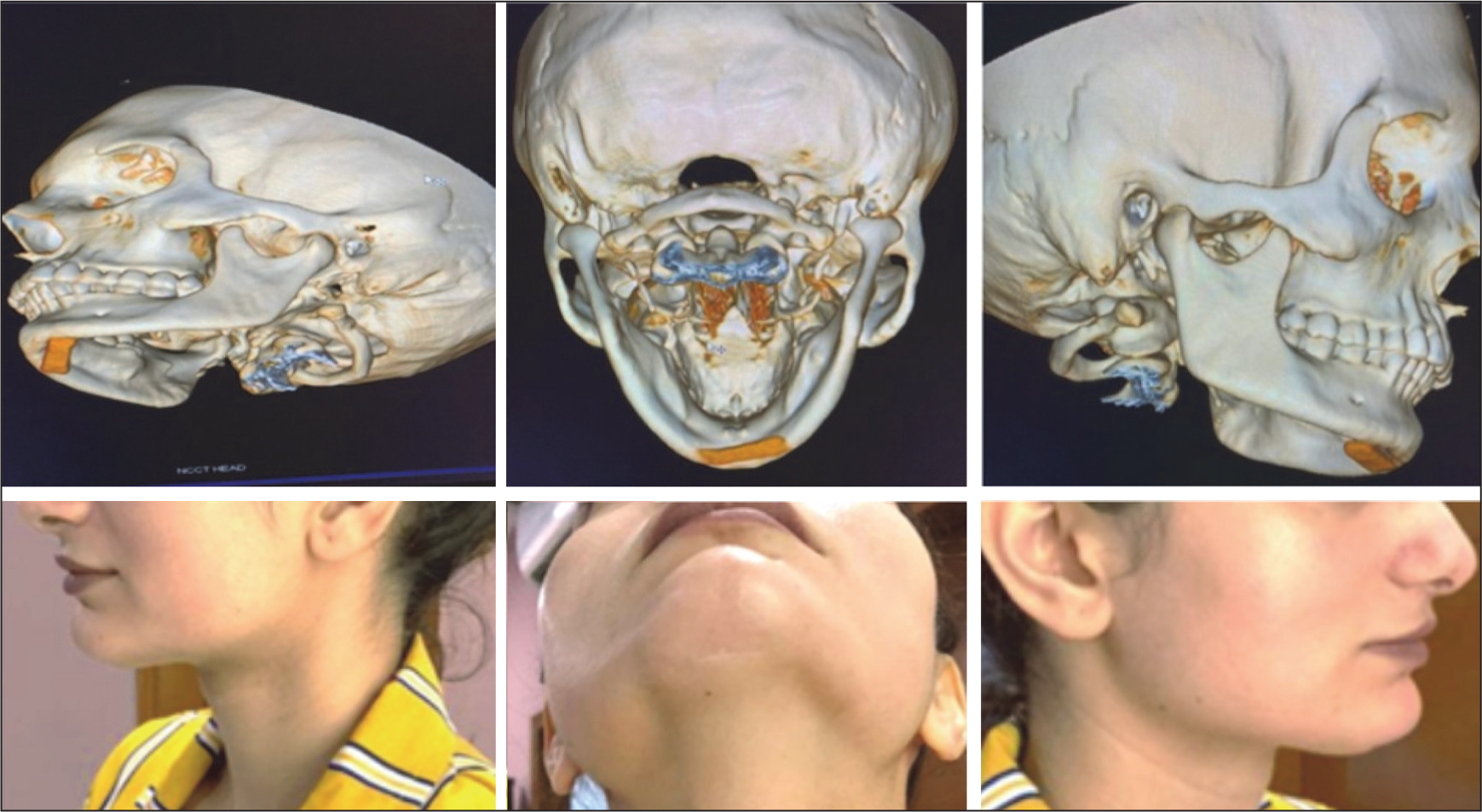
This 30-year-old Patient Had Come to Us for a Second Opinion Post Her Surgery, Where She Was Experiencing Altered Position and Mobile Implants. We Did a CT Scan, Which Showed Improper Implant Position, Over-dissection Leading to Inadequate Pocket Formation, With Non-fixation of the Implant. Also, the Patient was Dissatisfied Due to Poorly Visible Scar.
Discussion
Alloplastic chin augmentation remains a widely performed procedure for lower facial contour correction, yet outcomes are influenced by implant selection, surgical approach and fixation strategies. The current study introduces a structured 14-point intraoral framework to address these variables systematically and optimise aesthetic and functional results.
Mandibular morphology and aesthetic preferences differ between male and female patients, necessitating individualised implant selection. Although existing literature supports personalised facial implant planning, few studies explicitly stratify outcomes based on sex-specific aesthetic considerations. Bell et al. 10 reported broad implant-related outcomes without differentiating outcomes based on gender-specific shape preference or design selection
In clinical practice, extended anatomical implants are often favoured in males for increased width and projection, whereas concave or button-contoured implants may better suit female aesthetics. This approach aligns with modern aesthetic principles that prioritise harmony with underlying skeletal form, an aspect underscored in implant outcome analyses, though rarely quantified in gender-specific terms.
The intraoral approach is favoured by many surgeons and patients due to the absence of visible external scars.9,18 However, the oral cavity’s microbial environment may increase the risk of bacterial contamination compared with submental approaches.15,16 While some studies demonstrate comparable overall complication rates, certain reviews report higher implant removal rates with intraoral access.12,16,17 Complications such as infection and implant displacement, though uncommon (reported rates ranging from 0.8% to 7%), can necessitate revision surgery.15–17 Preventive strategies, including dental evaluation, antibiotic prophylaxis, meticulous surgical technique and postoperative oral hygiene are therefore critical.
Mental nerve injury, bone resorption and malposition resulting from mentalis muscle disruption have been well documented.6,12,15 The present framework emphasises precise subperiosteal pocket creation, rigid fixation and mentalis muscle re-approximation to mitigate these risks.
Chao et al. 18 demonstrated excellent outcomes with intraoral silicone implants without displacement or nerve injury. Meta-analyses suggest no clear superiority of intraoral or submental approaches regarding infection, asymmetry or extrusion.19,20
Another study by Rojas et al. 20 suggests that the approach of the incision does not affect the complication rate. While in our study we use silicone implants, since the Medpor implants have a tendency to form tight fibrotic ingrowths, which makes it difficult to replace or remove. Studies such as Rojas et al. suggest a 3.3% complication rate pertaining to Medpor implants in comparison to 1.1% of silicone implants.
Implant migration and palpability remain well-recognised postoperative concerns. Other studies 21 have discussed facial implants, emphasising that implant fixation reduces micro-movement, which is a known contributor to malposition and soft-tissue irregularity. Rigid fixation with a screw, as employed in the present framework, stabilises the implant at the inferior mandibular border and minimises movement during healing, improving long-term positional fidelity compared with non-fixated approaches. This strategy is indirectly supported by comparative outcomes where fixation or appropriate subperiosteal pocket control was associated with reduced displacement and asymmetry, although randomised comparisons within chin implant cohorts are limited in the current literature.
Our framework emphasises tailoring implant contour intraoperatively to match individual mandibular form and aesthetic goals. This personalised approach aligns with broader surgical principles that favour anatomy-guided augmentation over uniform implant application.
Visible scarring is an important consideration in populations prone to hypertrophic or pigmented scars, such as us Indians (Figure 11). The intraoral approach eliminates external incisions entirely, a benefit that has been repeatedly noted in large intraoral series such as the one by Chao et al. 18 where midline intraoral silicone augmentation avoided extraoral scars without compromising safety or outcomes.
Post Extra-oral Chin Implant, Patient Came to us for Scar Management, Indian Skin Scars Poorly with Hypertrophy and Scar Widening.

Comprehensive reviews, including Bell et al. 10 confirms that implant-based chin augmentation produces consistent satisfaction and relatively low complication rates when alloplastic materials are carefully selected and placed. However, few studies provide detailed guidance on standardised surgical steps. The present study has 100% satisfaction rate in the cohort, while producing standardised, consistent results.
By integrating gender-specific customised implant choice, meticulous intraoral access, controlled dissection and rigid fixation, the 14-point framework aims to build upon established evidence while reducing variability in outcomes, supporting a reproducible and patient-centred approach to chin augmentation.
Conclusions
A structured, gender-sensitive and anatomically customised intraoral approach to chin augmentation can achieve stable, scar-free and predictable results. The proposed 14-point framework represents a safe and effective evolution in intraoral chin implant surgery.
Study Limitations
This study reflects the experience of a single surgical team at one institution with a limited sample size. Larger multi-centre studies are needed to further validate the framework.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.