
Abstract
Severe gynecomastia with ptosis and skin excess presents surgical challenges. Standard procedures including free nipple grafting and reduction mammoplasty may result in complications like necrosis or unwanted bulkiness. This report describes a novel single-stage technique preserving the nipple–areola complex (NAC) on an inferior flap while excising excess tissue en bloc. A 38-year-old male with Grade 3 gynecomastia underwent excision via inferior flap-based NAC transposition. The design included a semicircular superior flap and an ellipsoid excision zone, maintaining 1 cm flap thickness for viability. The NAC was repositioned anatomically using suprasternal notch measurements, avoiding dog ears. Postoperatively, the NAC survived completely with satisfactory contour. This technique offers a viable alternative to free grafting, particularly in resource-limited settings. It addresses ptosis and bulk without de-epithelialisation or liposuction, though scars remain unavoidable. Suitable for select gynecomastia and transgender cases, it balances aesthetics and surgical practicality.
Introduction
The enlargement of the male breast, commonly referred to as ‘gynecomastia’, may occur due to proliferation of fatty, stromal or glandular tissue. While it is a common condition affecting men (65%),1,2 a few opt for surgical therapy. Current trends in gynecomastia correction have evolved towards lesser invasive techniques with a view to reduce scarring and achieve better cosmetic results. 3 Small-sized gynecomastia subjected to liposuction through keyhole incisions gives good cosmetic results. In large breasts, a combination of techniques like liposuction, residual gland excision and the circumareolar skin reduction may give acceptable results. However, in large ptotic feminine appearing breasts the issue of skin and gland excess remains a daunting issue. Traditional reduction mammoplasty techniques have been used in some of these cases, but the results are often compromising as flaps designed for better vascularity tend to be bulky. In patients with large gynecomastia complicated with an excess of skin and glandular tissue, amputation and free nipple–areola graft continues to be one of the mode of treatment in recent times as other established methods fail to adequately address the issues of skin and glandular tissue excess. In an attempt to preserve the nipple–areola complex (NAC) in these patients, while at the same time not wanting to give up the benefits of breast amputation, the author has designed a new technique where the inferior breast flap is designed to support the NAC and also allow for the skin and gland amputation at the same time, thereby correcting the gynecomastia with acceptable cosmetic results.
Case Report
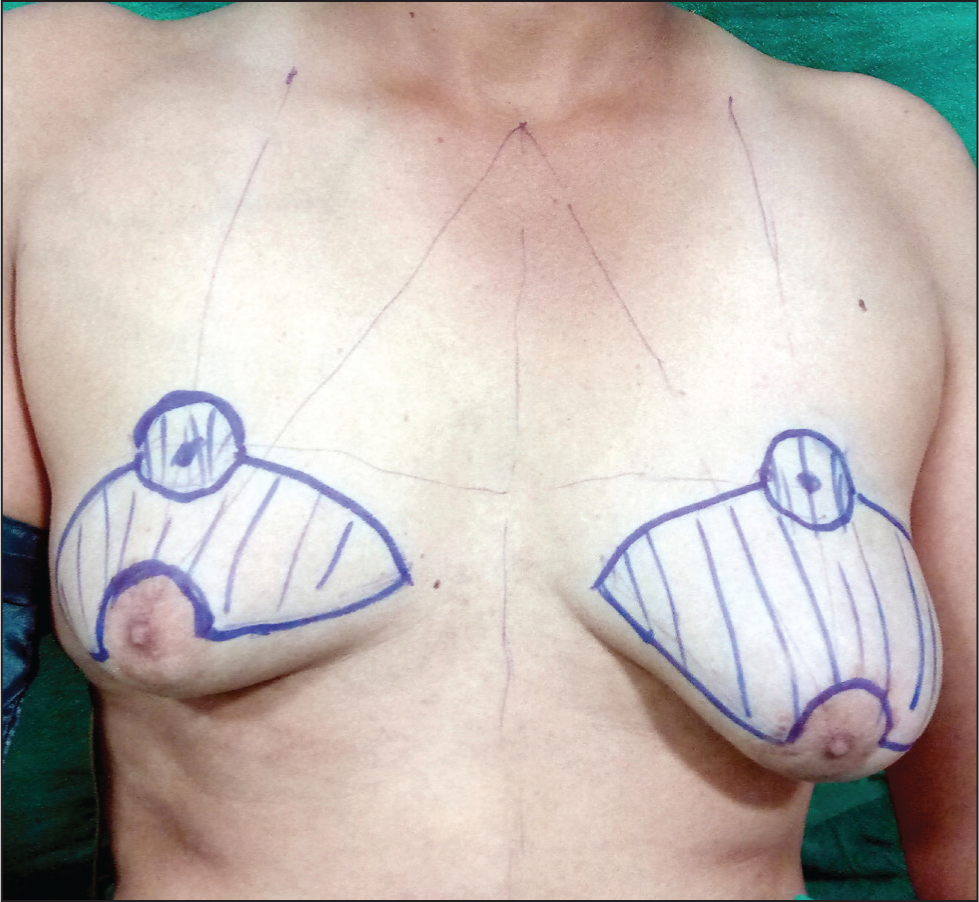
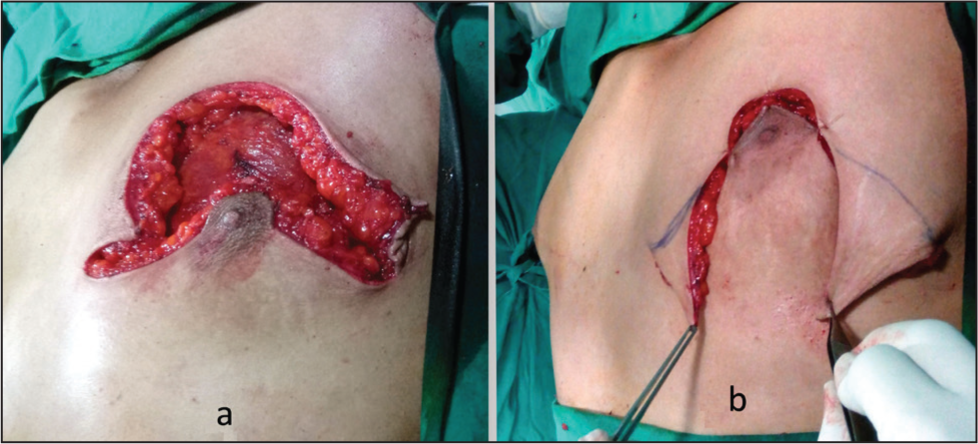
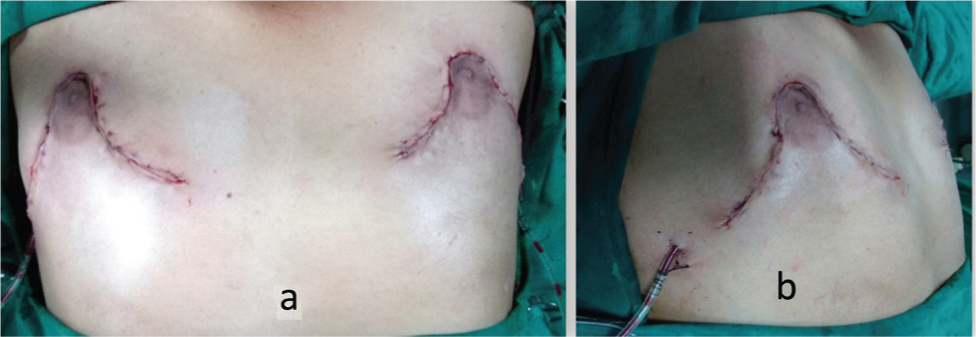
A 38-year-old male gentleman came to our department with a history of gynecomastia for several years. He was married, had two offsprings and wished to have a correction of his bilateral Grade 3 severe gynecomastia. After offering him all the options including a breast amputation with NAC graft, he requested that the breast size be reduced significantly, but the nipple and areola were to be left intact. He confirmed that visible scarring did not actually bother him, since his main aim was to wear well-fitting dresses which would not reveal any feminine breasts. The patient underwent routine blood examination and ultrasound examination of the breasts, both of which did not reveal any abnormality. Since the gynecomastia was large (Figure 1a and 1b) and the patient’s request genuine, the author contemplated on designing the flaps in such a way that all his conditions be met. Careful consideration of the surgical approach led to the development of a technique that supports the NAC on the inferior flap. This method ensures robust vascularity while enabling the elevation of a ptotic NAC to its anatomically ideal position, as determined by standard measurements from the suprasternal notch. The restoration of the NAC position was further guided by patient aesthetic preferences and the precise placement of the inframammary fold. It should be noted that this approach achieved the desired correction without introducing excessive bulk to the NAC pedicle (Figure 2). The superior flap would have the semicircular design in the centre of the flap to receive the NAC from the inferior flap. The ellipsoid area in between the two flaps would be the amputation area which would encompass the excess skin and breast tissue excised down to the pectoral fascia. Both the superior flap and the inferior flap wound consist of skin and subcutaneous tissue with appropriate thickness (1 cm) to maintain viability of the flaps. The medial extent would be 2 cm away from the midline and the lateral extent would be limited by the anterior axillary line. With this design in mind, the patient was operated under general anaesthesia. After the en bloc excision of skin and breast tissue and leaving the NAC on the inferior flap, the NAC was drawn into the superior flap and excess skin was excised by drawing in the upper flap as shown in the Figure 3a and 3b, thereby avoiding a dog ear at the medial and lateral ends of the excision. This resulted in a fairly acceptable postoperative result as seen in Figure 4a and 4b. Post-operatively compression garments and scar creams were advised. While all incisions healed well and NAC survived in toto, the patient was quite pleased with the results and declined to come back for any long-term follows.
The Preoperative Front (a) and Side View (b) of the Patient’s Breasts.

The Flaps Marked Out for NAC Sparing Breast Amputation.
The Ellipsoidal Excision (a) and Extent and Direction of Additional Skin Excision During Wound Closure (b).
The Postoperative Front (a) and Side View (b) of Patient’s Breasts.
Discussion
Breast amputation and free nipple–areola grafting have been an established technique in the management of large ptotic male breasts. 3 However, this technique is fraught with the dangers of poor take and necrosis of the NAC as well as the transverse breast scars. Other techniques keeping the NAC intact have been described but tend to add some bulk where the pedicle is planned. 4 Liposuction is not done in this technique, since once the NAC based on the inferior flap is planned, the whole of the breast gland and excess breast skin are amputated en bloc, thereby reducing the need for an additional procedure. The breast does not appear bulky as neither the breast tissue is maintained nor the flap holding NAC is deepithelialised. The NAC is only vascularised by the inferior skin flap supporting it. The procedure is simple single staged one, as it avoids additional liposuction and de-epithelialisation. The main drawback of this technique is the presence of the scars that extends from the areola on either side which will occur even if a breast amputation and free NAC graft are done. The other issue is with the size of the areola which cannot be modified as only the upper semicircle of the areola is cut and this part is based on the inferior flap supporting it. This was specifically done as the patient wanted a single-stage fool-proof procedure. The NAC was already compromised as its new blood supply was only on the inferiorly designed flap and further de-epithelisation in the inferior part of the NAC could have further compromised the NAC circulation. For those patients who wish to have a uniform NAC radius, the NAC can be taken in toto in the initial marking. Further de-epithelisation and equalisation can be done simultaneously or for added safety at a later stage. While sensations of the NAC cannot be guaranteed, another drawback is that the height of the lower flap cannot be tinkered with as it carries the NAC with it, notwithstanding the fact that the flap would possibly settle down over time. The areola height as well as infra-NAC fullness if present as a problem may be tackled as a secondary procedure if the patient so wishes. I believe that this technique based on established surgical principles does not provide a panacea for all large gynecomastia corrections, but can be considered in selected cases, as a viable alternative to breast amputation and free NAC graft surgery and in selected female to male transgender breast amputation surgery patients who are willing to accept scars on the chest wall. In regions that has a large population of financially challenged people with no access to plastic surgeons, this simple technique that does not involve liposuction or skin grafting procedures could be a boon in the hands of any trained surgeon.
Footnotes
Data Availability
No privacy issues in the paper.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval and Informed Consent
Informed consent taken. Technique is a variation of standard established pedicled techniques in breast surgery.
Funding
The author received no financial support for the research, authorship and/or publication of this article.