
Abstract
Background
Primary teeth are essential for mastication, phonetics, esthetics, and space maintenance. Their premature loss due to hypodontia, trauma, or caries can impair function, disturb alveolar growth, and create psychosocial concerns from compromised esthetics.
Rationale for Mini Implants in Children
Mini implants provide a fixed, esthetically acceptable, and functionally beneficial alternative to removable prostheses. Their small diameter (<3 mm) allows placement even in reduced alveolar ridges, making them suitable for pediatric conditions with transverse bone loss.
Clinical Advantages
Mini implants help preserve alveolar bone by reducing atrophy and preventing drifting of adjacent teeth. They are minimally invasive and versatile, with applications in both syndromic and non-syndromic patients. Their use as temporary anchorage also aids early orthodontic interventions and growth modification.
Considerations and Challenges
Success depends on careful patient selection, awareness of craniofacial growth, and interdisciplinary planning. Since growth may cause infraocclusion or occlusal discrepancies, mini implants should be regarded as temporary solutions until skeletal maturity allows definitive rehabilitation.
Limitations and Need for Research
Standardized protocols for pediatric mini-implant placement are lacking, and long-term evidence remains limited. Further studies, including randomized controlled trials, are required to establish survival rates, clinical outcomes, and long-term effects on growth.
Introduction
Primary teeth are a child’s most valuable oral asset. They are essential for mastication, speech, appearance, and most importantly, for maintaining arch space for the succeeding permanent teeth. 1 A considerable number of children experience tooth loss or absence because of congenital hypodontia or trauma, resulting in functional impairment, deficient alveolar development, and compromised esthetics, all of which may negatively affect the psychosocial growth of the child. 2 Since ancient times, the replacement of missing teeth in children has posed a significant challenge for clinicians. 3
Tooth loss management in children differs from that in adults due to ongoing craniofacial growth and distinct primary tooth morphology. The large pulp chambers and incomplete mineralization of immature teeth increase the risk of pulpal injury when complete coverage restorations are used. Therefore, clinicians often prefer partial coverage options such as Maryland bridges, resin-bonded restorations, or removable prostheses. However, these methods are not ideal—removable partial dentures rely heavily on child cooperation, can predispose to caries and gingival inflammation, and may necessitate periodic modification to accommodate growth changes. 2
Mini dental implants (MDIs) represent a modern advancement in tooth replacement therapy. Initially used mainly for overdenture stabilization, they are now also applied in pediatric cases involving congenitally missing teeth or tooth loss due to trauma. 4 With progress in digital workflows, bioengineered scaffolds, and temporary implant systems, the potential applications of pediatric implantology are expanding; however, current evidence still discourages implant placement in cases where primary teeth are lost due to caries. 5 MDIs can, nevertheless, be safely utilized for orthodontic purposes as temporary anchorage devices (TADs), since they can be easily removed once growth is complete. 6
Mini Implant
MDIs are small-diameter titanium fixtures that function as artificial tooth roots. They were first introduced in the mid-1980s by Dr. Victor I. Sendax of New York, with subsequent modification by Bulard, who developed the single one-piece O-ball design. 4 These implants typically measure 1.8–2.7 mm in diameter and are available in a variety of tip, thread, body, and head configurations. The thread design may range from fine to coarse, with variable thread spacing to suit different bone densities. Common head designs include square, rectangular, and O-ball types. The length, shape, and thickness of an MDI are selected based on the height and anatomical characteristics of the supporting bone. 4
MDIs are characterized by a reduced diameter (<3 mm), whereas narrow or conventional implants typically exceed 3 mm in diameter. Their smaller size allows for simplified surgical placement, especially in regions with limited alveolar bone width, eliminating the need for complex augmentation procedures. 7 The use of MDIs for overdenture retention offers several clinical advantages, including immediate primary stability, high survival rates, minimal marginal bone loss, and reduced postoperative discomfort, contributing to greater patient satisfaction and improved quality of life.
As MDIs can often be placed without flap elevation, they minimize surgical morbidity and healing time. Additional benefits include bone expansion during placement, reduced osteotomy size, and preservation of osseous blood supply, promoting enhanced angiogenesis and osseointegration. In the event of failure, removal and healing are straightforward with minimal tissue trauma. Studies evaluating overdentures supported by MDIs have consistently reported high levels of comfort, retention, masticatory efficiency, and speech improvement, making them a highly accepted treatment modality among patients. 7
Parts of Mini Implant 8
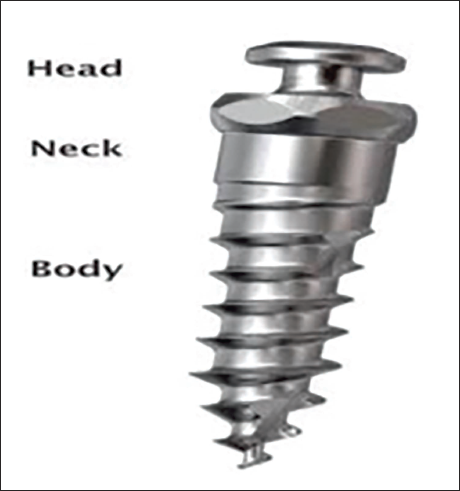
Head
The head section of the micro implant is in contact with the oral environment and is primarily intended to accept attachments such as elastics or wires.
Neck
The collar or neck portion of the mini implant forms the junction between the head and the body. It is manufactured in three height variants—1 mm, 2 mm, and 3 mm to adapt to the soft tissue thickness encountered at different implant placement sites.
Body
The implant body has a consistent shape. It is either self-tapping or self-drilling. Threads and grooves are used to facilitate the micro implant’s interlocking with the bone.
Case Selection Criteria for Mini Implants in Children
Age and Growth: Not placed as definitive replacements; only temporary anchorage/support until growth is complete. 9
Bone Quality/Quantity: Adequate alveolar bone height and thickness (≥4–5 mm in placement site) required. 10
Oral Hygiene & Caries Risk: High caries activity and poor hygiene are contraindications due to infection risk. 11
Children and adolescents with congenitally missing teeth, anodontia, partial anodontia, and trauma-related tooth loss.
Patients with congenital anomalies like ectodermal dysplasia (ED) and Down syndrome.
Patients with Cleft Palate and Alveolus.
Little ones who have trouble donning detachable devices. 8
The Insertion Site Selection12, 13
The practitioner should consider some factors while choosing a site for the implantation of a mini-implant. They are as follows: Fail-safe area: It is best to stay away from areas where there is a significant chance of seriously harming vital anatomic structures. Accessibility: It facilitates appropriate surgical techniques and adequate stability. Pain: Implants ought to be positioned in areas where patients experience the least degree of discomfort. Hard tissue features (amount and quality of cortical bone): The cortical bone must be thick enough to offer the required stability, especially mechanical stability immediately following implantation. Usability: The implant should be positioned in a way that is biomechanically favorable and allows the necessary orthodontic force to be applied.
Contra-indications & Drawbacks of Mini-implants
Mini Implant Failure and Management
In a six-year longitudinal follow-up, Jofré et al. (2015) reported repeated loss of the provisional crown, occurring once in the third, fourth, and fifth years, and three times during the sixth year. Each time, the crown was re-cemented and relined with acrylic by an external clinician. Owing to the frequent debonding episodes attributed to insufficient retention, the mini-implant was ultimately removed. Notably, removal required high torque values (approximately 50 Ncm), indicating strong osseointegration but resulting in significant deformation of the implant body during extraction.
At the six-year evaluation, a marked vertical discrepancy between the mini-implant and the adjacent natural teeth was evident, compromising crown retention and esthetics. This case highlights the limitations of mini-implants for replacing missing maxillary incisors in growing individuals. Alternative management strategies may include autotransplantation, resin-bonded bridges, or orthodontic space closure. 15 A critical factor in planning implant placement for children and adolescents is the assessment of skeletal maturity to prevent infraocclusion—typically evaluated using hand-wrist radiographs or cephalometric growth analysis. 15
Several management approaches for infraoccluded implants have been described in the literature, including the use of new implant-supported prosthetic restorations, orthodontic pretreatment involving intrusion of adjacent teeth and extrusion of opposing teeth, as well as distraction osteogenesis. 16 The authors emphasized that the maxillary incisor region, particularly the lateral incisor area, is highly susceptible to adverse outcomes owing to continued eruption of neighboring teeth and craniofacial growth changes after adolescence. This region is therefore considered a critical zone for implant placement.
Another important consideration is the interdental distance between the implant and adjacent teeth, as smaller spacing has been correlated with increased crestal bone loss around the implant. Thus, achieving adequate mesiodistal space before implant placement is vital for long-term success. Uprighting and paralleling adjacent teeth through non-intrusive orthodontic movements are recommended to establish proper spacing prior to implant insertion. 16
In a case reported by Nupur et al. (2023), despite the patient’s regular use of a retention plate, a 1 mm midline diastema developed between teeth 11 and 21 during a nine-month follow-up. However, as the implant-supported prosthesis remained functionally and esthetically satisfactory, no further intervention was deemed necessary. 17
Mini Implant Versus Conventional Implant System
MDIs can be contrasted with conventional implant systems in several ways. Unlike conventional implants, which typically consist of two components—the implant and the abutment, MDIs are one-piece devices. They feature a titanium screw with a ball-shaped head for denture retention or a square prosthetic head for fixed restorations, replacing the need for a separate abutment. Certain bracket-like head designs can also facilitate orthodontic applications, serving as indirect anchorage. Mini implants are placed transmucosally, protruding above the gingival surface, whereas conventional implants are subgingival. The transmucosal neck of MDIs is designed to be smooth and varies in length according to the soft tissue thickness at the implant site. 5
MDIs have emerged as a potential alternative to conventional implants in selected clinical situations, though their performance differs in terms of longevity, durability, and treatment outcomes. Conventional implants remain the gold standard, demonstrating long-term survival rates exceeding 90% over 10–15 years of follow-up.18, 19 By comparison, mini implants show more variable survival, typically 70%–90% at five to seven years, with increased risk of fracture or early failure of osseointegration due to their smaller diameter.20–23
MDIs provide notable advantages, including lower cost, minimally invasive surgical procedures, and simplified prosthetic workflows, which make them suitable for overdenture stabilization, orthodontic anchorage, and temporary replacements in growing patients.24, 25 Nevertheless, concerns remain regarding long-term durability, prosthetic complications, and the limited evidence in pediatric populations, where ongoing craniofacial growth may affect implant stability and treatment success. 25 The cost-effectiveness of MDIs is largely attributable to their smaller size, simpler placement, and fewer prosthetic components, making them an attractive option for temporary or interim treatments.24, 25
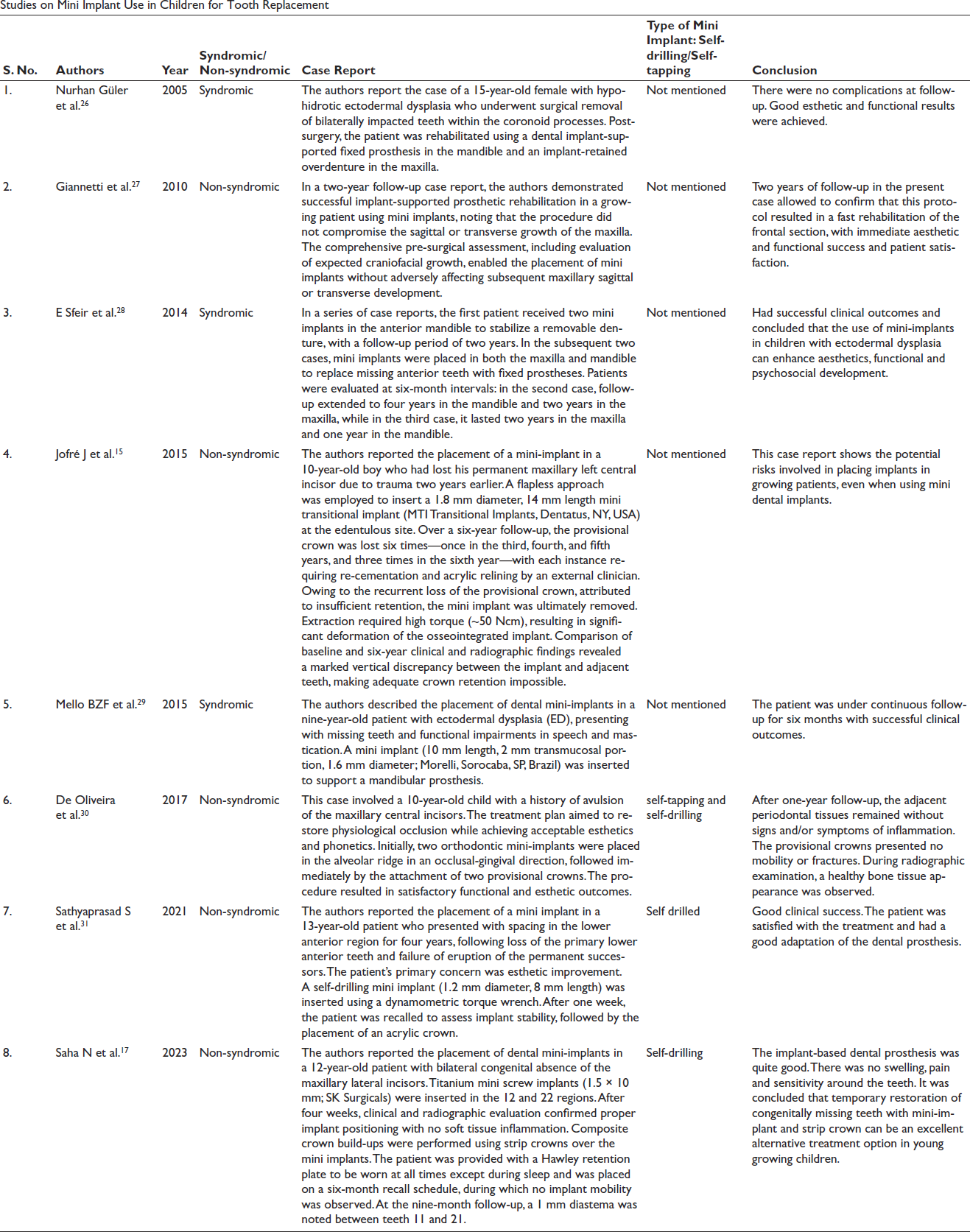
Studies on Mini Implant Use in Children for Tooth Replacement
Survival of an MDI-retained Overdenture in a Child with ED
Serdar Kilic et al. (2015) reported the rehabilitation of a six-year-old child with ED using a maxillary removable partial prosthesis and a mini-implant–retained mandibular overdenture. Over a six-year follow-up, there was no significant peri-implant bone resorption, and the prostheses functioned well without esthetic or functional complications. In this case, two mini implants were placed in the anterior mandible, supporting a ball-attachment–retained mandibular overdenture along with a removable partial maxillary prosthesis. Cephalometric evaluations at 15 months, 5 years, and 6 years guided the renewal of prostheses, ensuring maintenance of the normal growth pattern and allowing uneventful eruption of the maxillary second molars. The approach demonstrated that prosthetic rehabilitation during growth can satisfy both functional and esthetic needs, thereby motivating pediatric patients. 32
The primary objectives of dental treatment in syndromic patients include replacement of missing teeth and lost hard and soft tissues, restoration of vertical dimension, and support of facial soft tissues. In ED, oligodontia (approximately 80%) is more prevalent than anodontia, and treatment options such as complete dentures, removable partial prostheses, fixed partial prostheses, or implant-retained prostheses can address both esthetic and functional deficits.33, 34
In cases with alveolar ridge atrophy or knife-edge crests due to congenital tooth absence, the retention and stability of removable prostheses can be compromised because of insufficient bone support. Several studies suggest that implant-retained prostheses, with their high success rates, may serve as a superior alternative to conventional removable dentures.35, 36
Patients with ED are prone to alveolar bone resorption in both jaws, especially when using removable prostheses from an early age, which may result in severe bone loss. Post-adolescence, implant-based rehabilitation not only supports the prosthesis but also preserves alveolar bone long-term. However, severe bone resorption can pose a challenge for implant placement in edentulous ED patients. Various bone augmentation techniques have been employed, including vertical distraction osteogenesis, autogenous, allogenic, and xenogenic grafts, or combinations thereof. Additionally, zygomatic implants can provide an alternative for oral rehabilitation. Previous studies have demonstrated that dental implants combined with bone grafting offer significant advantages in improving clinical outcomes in ED patients. 31
Despite the growing body of evidence for conventional dental implants in ED, reports on the use of MDIs in children with ED remain limited, although clinical success has been documented in the few available cases.26, 28
Immediate Loaded Mini-implant in Children and Its Effect on Quality of Life
Missing anterior teeth, whether due to trauma or congenital absence, represent a significant dental handicap in children, impacting aesthetics, phonetics, function, and overall quality of life (QoL). Traditional treatment modalities include removable partial dentures, resin-bonded bridges, autotransplantation, and orthodontic space closure. While conventional implants are the ideal solution, their placement is generally delayed until the completion of craniofacial growth. Mini implants, however, offer a promising alternative by preserving bone and space, restoring function and esthetics, and improving QoL. 35
To date, only one study by Abozena et al. 35 has evaluated this approach in children. The study included 15 patients aged 11–13 years with missing anterior teeth. Mini implants were inserted using a flapless technique and immediately loaded with ceramic-fused-to-metal crowns. Follow-up assessments, conducted every six months for two years, included the Modified Gingival Index, probing depth, periotest mobility, marginal bone loss via standardized periapical radiographs, and oral health impact profile questionnaires administered before and after implant placement. Over the 24-month period, there were no statistically significant changes in the gingival index, probing depth, periotest mobility, or marginal bone loss. In contrast, the QoL questionnaire revealed a statistically significant improvement following mini-implant placement.
The study concluded that mini implants are a successful and promising solution for missing anterior teeth in children up to 11 years of age, but emphasized the need for careful case selection and long-term follow-up until growth completion to determine whether to maintain the mini implant or replace it with a conventional implant of appropriate size. 37
Limitations
Mini-implants should not be placed in situations with restricted inter-arch space, in ridges with inadequate vertical height, or in people with parafunctional habits. Because of their narrow diameter, implants are more likely to fracture during implantation. The one-piece design, implants lack parallelism, making the insertion of several implants necessary because of the unpredictable nature of failure and the lack of established scientific criteria and expertise in this area. Moreover, there is a dearth of reliable scientific information about the long-term viability of these implants. Mini-implant-supported fixed restorations require careful case selection, accurate treatment execution, and a thorough understanding of biomechanics to be clinically successful.36, 37
Lack of long-term evidence, as most existing literature comprises case reports or small case series; currently, there are no RCTs for mini-implant use for tooth replacement in children. Limited standardized protocols, as no universal clinical or radiographic guidelines exist for mini-implant placement in growing children. Success depends heavily on the clinician’s understanding of pediatric growth, surgical skills, and prosthodontic knowledge.
Mini implants demonstrate promising, high success rates and stability in growing patients, with studies reporting favorable outcomes and potential for alveolar bone preservation. However, long-term durability data are still limited for children, with research highlighting the need for further prospective studies to fully understand their long-term effectiveness and optimize clinical application in this demographic. 38
Future Perspectives
Future research should prioritize long-term studies and randomized controlled trials to determine the durability and success of mini implants in pediatric patients. There is a need for standardized protocols and evidence-based clinical guidelines regarding implant selection, placement techniques, and maintenance strategies. The integration of digital workflows such as CBCT, intraoral scanning, and CAD/CAM can enhance precision and efficiency. An interdisciplinary approach involving pediatric dentists, orthodontists, prosthodontists, and surgeons will be crucial for comprehensive management, especially in children with special needs or craniofacial anomalies. Research is progressing on bioengineered implants using MSCs, growth factors, and scaffolds for bone regeneration, and biosensor-integrated implants for monitoring occlusal forces and detecting peri-implant disease. 5
Conclusion
Mini implants provide an effective interim prosthetic solution in pediatric dentistry, meeting esthetic and psychological needs while preserving alveolar bone and preventing space loss. Their minimally invasive placement, affordability, and ease of removal make them particularly suitable during the growth phase. Importantly, they serve as functional space maintainers and support oral development until definitive prosthetic rehabilitation can be planned after growth completion.
Footnotes
Acknowledgment
None.
Authors’ Contribution
Literature review, article preparation: Ramya Ramanathan, Paul Chalakkal, and Siya Dukle.
Declaration
This manuscript has not been presented previously and has not been submitted elsewhere for publication.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval and Informed Consent
Not applicable.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.