
Abstract
Introduction
This study aimed to evaluate dentin wear after removal of fiberglass posts using microsonics and guided endodontic techniques.
Methods
Twenty extracted central and lateral human mandibular incisors were divided into two groups (n = 10): MS Group—removal of posts using the microsonic technique with E15 finder ultrasonic tips at 40% power, coupled with Gnatus ultrasound using 10× magnification in a dental microscope, until visualization of the gutta-percha; and EG group—removal of posts using guided endodontic technique with a 1.3 mm drill until a length of 14 mm was reached, at which point the gutta-percha was visualized through the surgical microscope. The time for removal was stopped.
Results
The results were subjected to statistical analysis using the Shapiro–Wilk normality test and the parametric analysis of variance (ANOVA) (Tukey) test at a 5% significance level. The tables demonstrate that guided endodontics (GE) resulted in a significantly lower final volume of dentin wear after post removal compared to the ultrasonic technique (16.21 mm³ vs. 21.41 mm³, p < .05). Additionally, post removal by GE was substantially faster, requiring only 322.30 s in contrast to the 1,707.10 s of the ultrasonic technique (p < .0001). Thus, the guided technique proved superior in terms of dentin preservation and temporal efficiency.
Conclusion
Removal of fiberglass posts with the guided endodontic technique promoted less dentin wear than ultrasonics with less clinical time.
Clinical Relevance
Guided endodontic technique is a predictable and precise method for efficient removal of fiber post.
Introduction
The preservation of natural dentin is paramount for maintaining the structural integrity and biomechanical properties of teeth, which are crucial for long-term fracture resistance. 1 Excessive removal of dentin during procedures can significantly compromise the tooth’s ability to withstand occlusal forces, leading to complications such as perforations and reduced longevity. 2 Therefore, techniques that minimize dentin wear are clinically important to enhance the prognosis and ensure the long-term survival of restored teeth.
The use of intraradicular posts is indicated when extensive loss of tooth structures occurs, especially due to carious lesions and dental trauma. 2
Currently, prefabricated fiberglass posts are widely used in conjunction with composite resin cores. Although both fiberglass posts and cast metal posts have good clinical performance, 3 fiberglass posts have advantages over metal posts. Not only are they more aesthetically pleasing, 4 but they also require less time for clinical intervention and reduce the number of visits. Because they have a modulus of elasticity similar to that of dentin elasticity, the tooth fracture index is significantly reduced. 1
In cases where reintervention becomes necessary during endodontic treatment, especially in cases where periapical pathologies are present, 5 the ability to remove intraradicular fiberglass retainers becomes a challenge.
The use of inserts coupled with the ultrasonic device, together with the magnification provided by the surgical microscope, offers advantages by improving the visualization of the surgical field, making the technique safer compared with conventional techniques without magnification. 6 Even with today’s resources and the aid of surgical microscopy, the risks associated with the removal of fiberglass posts are not completely under control. Removal of these posts can result in complications such as perforations, deviations, or excessive dentin wear, which affect the prognosis and preservation of the tooth. 2
The combination of ultrasonic tips and a dental microscope for intracanal post removal has been shown to offer superior precision and safety. Ultrasonic tips generate controlled vibrations that efficiently disrupt the cement layer, facilitating post removal while minimizing thermal and mechanical stress on the surrounding dentin. 7 The microscope provides enhanced magnification and illumination, allowing for meticulous visualization and preservation of the root structure. This approach significantly reduces iatrogenic damage and improves outcomes in endodontic retreatment procedures. 8
With cone beam computed tomography (CBCT) and intraoral scanning, it is possible to make access guides to the root canal, minimizing risks and optimizing clinical time. 9 Access in teeth with intraradicular fiberglass retainers by guided endodontics (GE) minimizes the risks associated with post removal. In addition, dentin wear is reduced due to the precision of wear, and surgical time is optimized. 10
To our knowledge, no studies have compared the guided endodontic technique and the use of ultrasonics in conjunction with microscopy for the removal of fiberglass posts. This study aimed to compare dentin wear after removal of a fiberglass post using GE or ultrasonics in conjunction with a microscope and the time required for the procedure. The null hypothesis was that there would be no statistically significant difference between the techniques used, both in terms of wear and duration of fiberglass post removal.
Materials and Methods
This study was approved by the local Human Subjects Ethics and Research Committee (approval no. 38898920.50000.5374). Twenty extracted human mandibular central and lateral incisors with fully developed and single roots and single canals with no root fractures, resorptions, calcifications, or dilacerations were included in the study. Sample size was based on sample calculation using the ANOVA (one-way) test (G* Power 3.1.9.4, Franz Faul, College of Kiel, Germany), with α = 0.05 and β = 0.95, effect size f = 2.63. The minimum number of samples calculated for each group was eight. To minimize the effect of outliers, 10 samples were taken per group.
Preparation of the Specimens
Teeth were first examined under a surgical microscope (DF Vasconcelos, Valença, Brazil) at 10× magnification and radiographed with a digital radiographic sensor (Micro Imagem, Rio de Janeiro, Brazil) to verify that the inclusion and exclusion criteria were met.
Endodontic Treatment
The teeth were accessed on the lingual side with a 1,012 spherical diamond tip (KG Sorensen, São Paulo, Brazil). Root canal length determination was performed by inserting a #10 K-file (Dentsply Maillefer, Ballaigues, Switzerland) into the canal until it was visualized in the apical foramen using a surgical microscope at 10× magnification. The working length was determined 1 mm below the apical foramen.
Pre-enlargement was performed using the Orifice Shaper 17.08 instrument (MK Life, Porto Alegre, Brazil), and the root canal instrumentation was performed with the WaveOne Gold Primary 25.07 files (Dentsply Maillefer, Ballaigues, Switzerland). During the root canal instrumentation, 2.5% sodium hypochlorite (NaOCl) (Asfer, São Caetano do Sul, Brazil) was used as an irrigant solution.
Final irrigation was performed by agitating the irrigation substances with EasyClean (Bassi/Easy Equipamentos Odontológicos, Belo Horizonte, Brazil) in cycles of 20 s with three cycles of NaOCl, three cycles of 17% ethylenediaminetetraacetic acid (EDTA) (Formula and Action, São Paulo, Brazil), and a final three cycles of NaOCl. A total of 3 mL of EDTA and 20 mL of NaOCl were used. The canals were then dried using a capillary tip (Ultradent Products, Indaiatuba, Brazil) connected to a vacuum pump (Dabi-Atlante, Ribeirão Preto, Brazil) and an absorbent paper tip (Dentsply Maillefer).
The canals were obturated using the thermoplastic technique with a gutta-percha cone 25/.07 (Dentsply Maillefer) and AH Plus cement (Dentsply Maillefer). Thermal compaction of the filling material using the down-pack technique was performed with the Termo Pack II (Basi/Easy Equipamentos Odontológicos, Belo Horizonte, Brazil), maintaining a distance of 14 mm depth in the middle and coronal thirds for the placement of the fiberglass posts. After endodontic treatment, specimens were stored in a humid oven at 37 °C for 24 hours.
Preparation of the Teeth and Placement of the Posts
After endodontic treatment, teeth were prepared to a depth of 14 mm using wide drills 2 and 3 (MK Life, Porto Alegre, Brazil) and special white post DC kit drill number 1 (FGM, Joinville, Brazil), one new drill for every five teeth.
A random human dental arch was scanned with a CS 3600 scanner (Carestream Dental, Atlanta, USA) to serve as a model. Five models were printed using a 3D printer (Sethi3D S2, Campinas, Brazil). From these arches, the central and lower lateral incisors were removed using a Maxicut drill (American Burrs, Palhoça, Brazil), leaving a space in the region. The previously prepared teeth were fixed with additional silicone in these spaces created for bite registration (Scan Bite, Yller Biomaterials, Pelotas, Brazil).
A CBCT scan was performed using a CS 9600 CT scanner (Carestream Dental, São José dos Campos, Brazil) to evaluate the volume of the preparations made before the placement of the posts through volumetric measurements of the hypodense areas prepared using the Dental Slice program (Bioparts Biomedical Prototyping, Brasília, Brazil).
Cementation of the Fiberglass Posts and Coronal Restorations
The DC posts number 1 (FGM, Joinville, Brazil) were previously tried in the holes, cleaned with 70% alcohol, and then a layer of silane (3M do Brasil, São Paulo, Brazil) was applied.
The prepared spaces were rinsed with 0.9% saline (Mió, Belo Horizonte, Brazil) and dried with absorbent paper points (Dentsply Maillefer). RelyX U200 self-adhesive resin cement (3M ESPE, St Paul, MN, USA) was placed in the prepared space using a mixing tip and an intracanal applicator tip (3M ESPE). The posts were then inserted and held in position with digital pressure, and the excess cement was removed with a microbrush (FGM, Joinville, Brazil). Light curing was performed for 40 s using a Valo light curing unit (SDI, São Paulo, Brazil). The excess of the posts was cut off 1 mm below the coronal opening, and the restoration was carried out with composite resin.
A 37% acid etch (FGM, Joinville, Brazil) was performed for 30 s, followed by 1 min of rinsing and drying with absorbent papers. Adper Single Bond 2 adhesive (3M do Brasil) was applied, and light-cured for 20 s. Filtek Z250 composite resin (3M do Brasil) was then applied incrementally to achieve a complete coronal seal. A CBCT scan was performed, along with a 3D scan of the EG group models for planning and Endoguide impression.
Technique of Post Removal
Before the intervention, specimens were randomly assigned to either the microsonic or GE group to ensure balanced distribution. To minimize bias, the evaluator analyzing the cone beam CBCT scans and quantifying dentin wear would be rigorously blinded to the treatment group of each sample. Twenty teeth were randomly divided into two groups. In the MS Group, fiberglass posts were removed using a Profi Neo Gnatus ultrasonic unit (Dabi-Atlante, Ribeirão Preto, Brazil) with E15-Finder ultrasonic inserts (Helse ultrasonic, Santa Rosa do Viterbo, Brazil) at 40% power, using a new ultrasonic tip every five teeth. A surgical microscope with 10x magnification was used during the procedure. In the EG group, post removal was performed using plastic templates (Radiodontica, Chapeco, Brazil) made specifically for this study and 1.3-mm drills (Radiodontica, Chapeco, Brazil) connected to a Surgic Pro surgical motor (NSK, São Paulo, Brazil) with a torque of 40 N and a speed of 400 rpm for post removal. Templates were created using a CBCT of the models and a 3D scan of them.
During the removal of the posts, the times in both groups were stopped using a Samsung Galaxy S10e (Samsung, Campinas, Brazil) Android stopwatch application. Comparison of dentinal wear was performed by CBCT analysis of the teeth after preparation for the pin and after pin removal. Volumetric measurements of the intracanal hypodense spaces of the CT scans were performed to assess whether there was an increase in dentinal wear after pin removal with the two techniques used. Dental Slice software was used for this step.
Statistical Analysis
The results were analyzed using Biostat 5.3 software and subjected to the Shapiro–Wilk normality test. The sample showed normal behavior, and the results were subjected to the parametric ANOVA test (Tukey) with a significance level of 5%.
Results
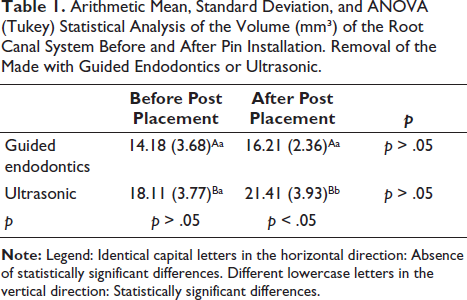
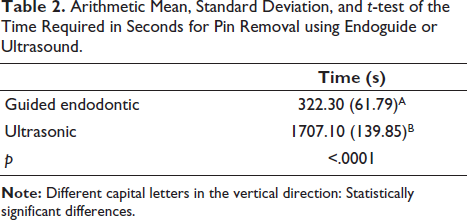
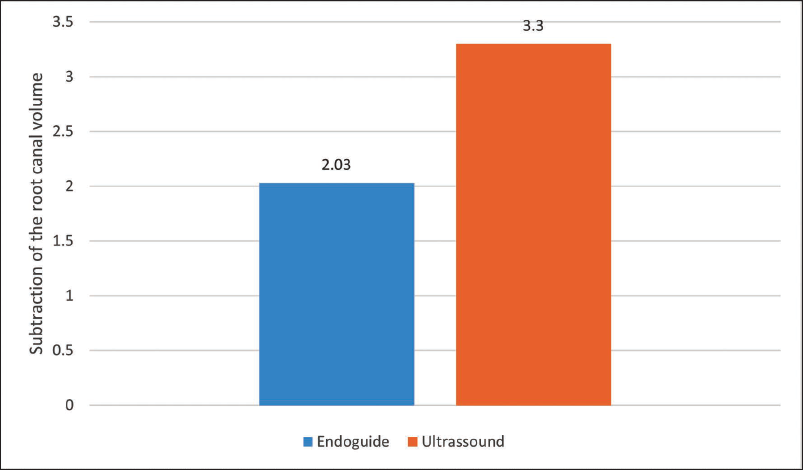
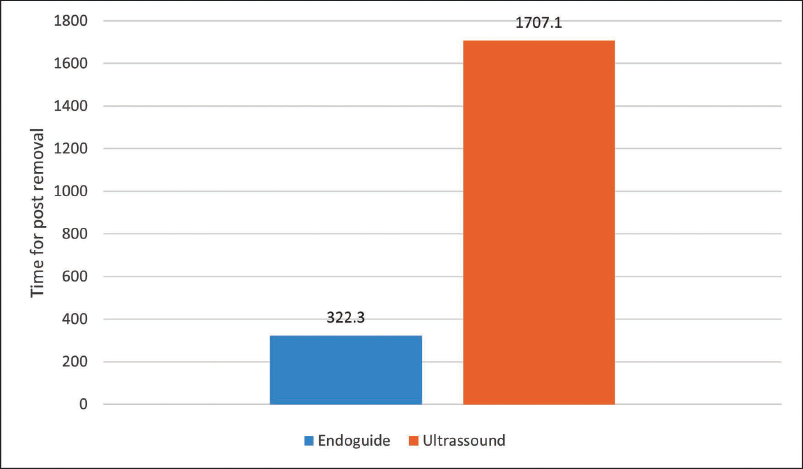
There was no significant difference in the volume of the root canal system before and after removal of the posts using GE or ultrasound (p > .05) when volumes were compared between teeth in the same groups. When comparing the volumes after pin removal between the EG and MS groups, the volume of the root canal system after pin removal with ultrasound was greater than the final volume after GE (p < .05) (Table 1 and Figure 1). Post removal with GE was significantly faster than removal with ultrasound (p < .0001) (Table 2 and Figure 2).
Arithmetic Mean, Standard Deviation, and ANOVA (Tukey) Statistical Analysis of the Volume (mm³) of the Root Canal System Before and After Pin Installation. Removal of the Made with Guided Endodontics or Ultrasonic.
Arithmetic Mean, Standard Deviation, and t-test of the Time Required in Seconds for Pin Removal using Endoguide or Ultrasound.
Arithmetic Means of the Root Canal System Volume Subtraction (mm³) Before and After Post Placement: Removal Performed with Endoguide or Ultrasound.
Arithmetic Mean Times (in Seconds) Required for Post Removal Using Endoguide or Ultrasound.
Discussion
The clinical implications of this study are significant, as they underscore the benefits of GE for fiber post removal, particularly in preserving tooth structure and enhancing procedural efficiency. The findings demonstrate that this technique promotes less dentin wear and significantly reduces clinical time compared to ultrasonic methods, thereby minimizing the risk of iatrogenic damage such as perforations or deviations, and improving the long-term prognosis of endodontically treated teeth. 7 This precision-driven approach supports conservative dental practice, ultimately contributing to better patient outcomes and the prolonged survival of restored teeth.
While comprehensive systematic reviews directly comparing GE with ultrasonics for fiber post removal are scarce, the principles validated by this study align with broader evidence advocating for dentin preservation and minimally invasive endodontic interventions. Existing systematic reviews emphasize the critical role of dentin quantity in determining tooth fracture resistance, reinforcing the importance of techniques that limit substance loss during retreatment procedures. 1 Moreover, the consistent findings regarding the accuracy and safety of GE are corroborated by reviews that highlight its role in complex cases and its potential to standardize challenging procedures, even suggesting its superiority in precision over conventional methods. 11
The purpose of this study was to evaluate dentin wear after removal of fiberglass posts using GE or ultrasonics with the microscope and the time required for the procedure. The null hypothesis was rejected because dentin wear was greater after post removal with ultrasound compared with GE. Removal of posts with GE was significantly faster than removal with ultrasonics.
Removal of fiberglass posts using drills with or without magnification carries risks such as excessive dentin wear and root perforation. 12 GE is a safe technique 13 that preserves tooth structure and helps avoid accidents such as deviation and perforation. 14 It also allows preoperative planning of the procedure, the ideal length and position of the posts with the help of software. 10 One of the advantages of the guided endodontic technique is that the operator does not need as much experience compared to the experience required by the technique of removing fiberglass posts with ultrasonic inserts15, 16 since the endodontic template guides the drill in the correct direction and contributes to a conservative preparation that preserves the tooth structure. 17 In contrast, the success of post removal with ultrasound depends directly on the experience of the operator and may require the use of a surgical microscope. 18 The use of ultrasonic inserts to remove fibrous posts carries risks, such as the likelihood of deviation from the root axis, excessive removal of tooth structure, and root perforation.12, 15, 19 GE reduces the risk of failure by preventing excessive removal of tooth structure, perforation, or weakening of the root. Digital planning maps the anatomy of the root so that changes can be predicted, leading to a better long-term prognosis. 17
Treating pulp canal obliteration presents challenges even for experienced endodontists. The GE used to remove the fiber post in this study contributed to less dentin wear than when ultrasonics were used. The fact that the root canal volume was greater after removal of the post with ultrasound than after the use of GE may be attributed to the correct direction of the drill through GE. The GE technique offers a precise alternative to conventional access preparation. Using cone beam CBCT and digital surface scans, GE allows virtual planning for accurate access to calcified canals, using either static templates or dynamic navigation systems. 11
The ultrasonic tip does not distinguish between dentin and the post and may cause dentin abrasion in either direction. Kim et al. 12 evaluated the volumetric changes in the pin space before and after pin removal using micro-CT and reported that only small amounts of dentin were removed when fiberglass posts were removed with ultrasonic. In another study that investigated the removal of Hi-Rem and D.T. Light-Post fiber posts using different methods (ultrasound, Largo drill, or rotary system), as well as the time and effectiveness of the procedures. The teeth were weighed before and after the procedure to identify potential excessive removal. The data showed no significant differences between the types of methods tested for post removal. 20 To reduce dentin removal, Schwindling et al. 10 suggested the development of a conical diamond drill instead of a parallel drill. While preoperative planning time will certainly increase, operative time can be significantly reduced once the ideal drills and pins become available.
A previous study assessed the conventional access cavity preparation (CONV) and GE in anterior teeth with pulp canal calcification (PCC), focusing on root canal detection, substance loss, procedure time, and the need for additional radiographs. A total of 108 extracted human teeth with PCC were paired and divided into two groups to create 18 clinical models. An endodontist performed CONV, whereas a general dentist used GE under simulated conditions. Procedural time and the number of additional radiographs were recorded, and cone beam CBCT scans measured substance loss. Both methods successfully accessed all root canals, with no significant differences in substance loss (CONV: 15.9–29.6 mm³ vs. GE: 17.6–27.5 mm³) or time (CONV: 163.3–248.5 s vs. GE: 231.9–326.8 s). However, GE required 31 additional radiographs, while none were needed for CONV. In conclusion, both CONV performed by a specialist and GE performed by a general dentist provided effective results in terms of substance loss and procedure time. 21
In terms of post removal time, the guided endodontic technique was significantly faster than ultrasonics, likely due to the endodontic guide used to direct the drill directly to the post.
There are limitations to GE, such as errors in intraoral scanning, 3D virtual planning, and template printing. The quality of the images may be affected by patient movement during scanning. During pin removal, irrigation may be affected by using the endodontic guide. To minimize this problem, Liu et al. 22 suggested the use of a drill with internal cooling. Another limitation is that immediate intervention is not possible because GE requires CBCT imaging and early intraoral scanning. Bolt removal with ultrasonic technology, on the other hand, requires the assistance of a surgical microscope for better visualization.
Clinically, GE for pin removal has shown promising results. Some published case reports have shown successful treatments.15, 16, 18
It was concluded that the removal of fiberglass posts with the guided endodontic technique resulted in less wear of the dentin than ultrasonic treatment, with less clinical time required.
Footnotes
Acknowledgments
The authors deny any conflicts of interest related to this study.
Authors’ Contribution
Conception and design were performed by M, MC; R, DG. Material preparation, data collection, and analysis were performed by M, MC; M, AS; L, AG; N, WM; MFVMA, TMCC; F, CE; P, RA; B, CE. The first draft of the manuscript was written by MFVMA, L, AG; C, BA; M, AS; and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Data Availability Statement
All data supporting the findings of this study are available in the article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval Institutional Statement
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Human teeth were used after São Leopoldo Mandic Ethics Committee (approval number: 38898920.50000.5374).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by grants from Fundação Carlos Chagas Filho de Amparo à Pesquisa do Estado do Rio de Janeiro (FAPERJ) (E-26/200.184/2023) and Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq) (446114/2024-3), Brazilian Governmental Institutions.
Informed Consent
Informed consent was obtained from all individual participants included in the study.