
Abstract
Periapical pathologies are encountered routinely on an endodontically compromised tooth which may or may not be painful. The lesions resulting from few millimeters to centimeters can be a cyst, granuloma or an abscess combinedly comprising up to more than 90% of all periapical lesions. Various methods can be used for the treatment of the periapical lesions using modern endodontic techniques including endodontic microscopes, ultrasonic irrigation tips, intra canal calcium hydroxide medicaments, advanced cleaning and shaping endodontic files and advanced obturation techniques. The goal of the endodontic treatment is to provide a complete aseptic environment with complete sealing of root canal and coronal restoration with absolute eradication of any microbial growth for successful resolution of the lesions. We are reporting here multiple cases where we used calcium hydroxide as an intra-canal medicament for its antibacterial properties and intra-canal medicament for the treatment of periapical lesions.
Introduction
The healing of any periapical lesion is achieved through accurately done root canal treatment eradicating any bacterial contamination from the cleansed and shaped root canal system, completely sealing the canals and coronal seal preventing any future micro leakage resulting in recontamination of the canal system. 1 Compromising at any of these steps may lead to retreatment or failure of the treatment taking into consideration of the preoperative status of the tooth, operative excellence and postoperative follow ups of the treatment. 2 The lack of circulation in the necrosed pulp area helps the bacterial growth and challenges the clearance of toxins produced as byproducts of the bacterial growth leading to formation of complex periapical pathologies to treat. Anyhow the periapical pathologies on endodontically compromised teeth must be treated first with a conservative approach without any surgical intervention. 3 Almost 94.4% success rate has been achieved in complete and partial healing of the periapical lesion with conservative treatments. 4 Various factors influence the treatment outcome of root canal therapy from preoperative evaluation of the tooth to the cleaning and shaping of the system. 1 Many intra-canal medicaments are used to inhibit bacterial growth which is suspected to be left in dentinal tubules and prevent any further colonization in the periapical region after cleaning and shaping of the root canals. Calcium hydroxide is one the best materials to be used as intra-canal medicament because of its anti-bacterial properties and its influence on hard tissue formation. 5 We are here presenting case reports in which we used calcium hydroxide as root canal medicament in consecutive appointments and as a sealer on completion of root canal therapy.
Case 1
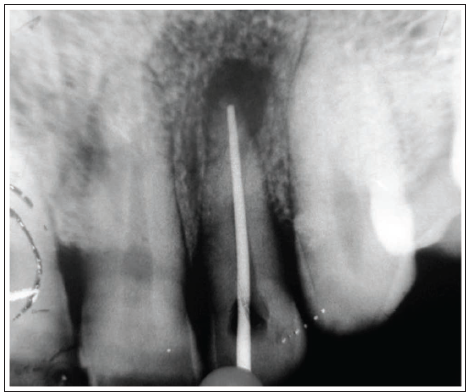
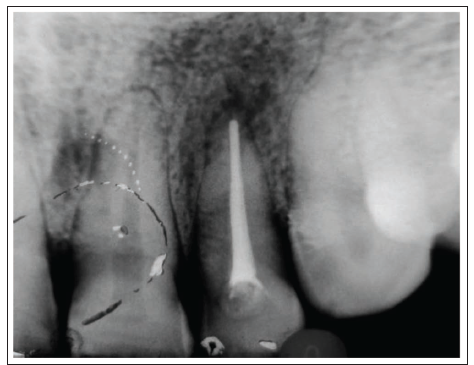
A male patient of age 35 years reached with periapical draining sinus with pus discharge in relation to lateral incisor of right maxillary quadrant. On inspection the tooth was non-vital. On intra oral radiograph a radiolucency with sharp margins was seen in relation to the involved tooth. Access opening done under local anesthesia with 2% lidocaine solution and tooth was isolated with rubber dam and canal was explored with size 15 K-files. The canal was prepared with step back technique reaching master file size 50. The canal was irrigated with 3% sodium hypochlorite solution with subsequent use of EDTA with k-files. After cleaning and shaping calcium hydroxide paste was placed in the canal for first week and repeated again for the next week. After the second calcium hydroxide dressing the tooth was asymptomatic and canal was dry. The obturation was done with a calcium hydroxide sealer with a lateral condensation technique. Six-month follow-up showed adequate response to the treatment and ongoing periapical healing of the lesion (Figures 1 & 2).
Pre-operative with Master Cone.
Post-operative after 6 months.
Case 2
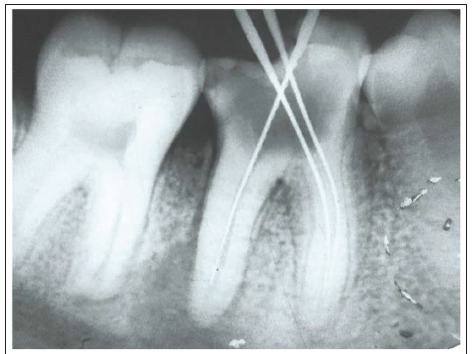
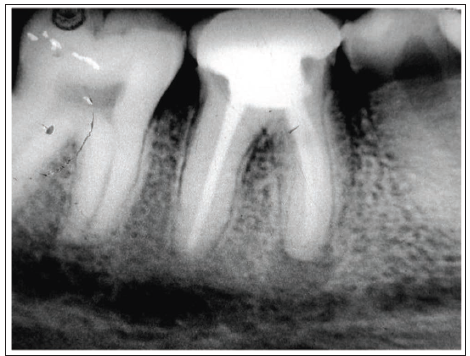
A male patient of age 16 presented with severe pain and swelling in relation to first molar of mandibular right quadrant. On examination swelling was in relation to the carious tooth with pulp exposure. The swelling was fluctuant and drained with pus on negotiation. On radiograph diffuse periapical radiolucency was seen in relation to the infected tooth. The proper access was prepared after the tooth was anesthetized with 2% lidocaine solution and isolated with rubber dam. The canals were explored with size 10 K files and working length was obtained using intra-oral radiographs. The canals were prepared with step back technique with subsequent recapitulation and master file size 40 was reached. The canals were debrided with 3% sodium hypochlorite solution and EDTA with K files for cleaning and lubrication of the canal. Obturation was done with lateral condensation technique. On two years of follow-up treatment was asymptomatic with no signs of any draining sinus or discomfort (Figures 3 and 4).
Pre-operative.
Post-operative Follow up after 1 year.
Discussion
Non-surgical approach must always be considered for treatment of periapical pathologies and should be treatment of choice as surgical option is not always necessary. More over patients medical and psychological conditions are sometimes not in favor of surgical approach. The intra-canal.6, 7 Complete cleaning of root canal system and creating absolute aseptic environment is difficult to achieve. The irrigation of canal is compromised sometimes because of anatomic complexity making access difficult of periapical one third of the canal.8, 9 Micro endodontics is superior to conventional endodontic surgical procedures and so the first line treatment option must always be a non-surgical approach. In 1965 Kakehashi et al. performed an experiment on rats demonstrating that periapical lesions can heal on themselves in the absence of bacterial growth and their byproducts.10, 11 During the root canal treatment, the chemical debridement and intra-canal dressings prevent further bacterial growth and recolonization of bacteria over a period of time. Calcium hydroxide is one of the best root canal medicaments used for its bactericidal properties, induction of hard tissue formation, highly alkaline pH-approx. 12 and tissue dissolving property. 5
The bactericidal property is due to disruption of bacterial cell wall, denaturation of protein and DNA damage due to release of hydroxyl ions. 12 Most of the pathogens are unable to survive in such a highly alkaline pH. 13 The thixotropic behavior of calcium hydroxide helps in mixing it in thick consistency and yet when it is agitated desirable flow can be obtained. The calcium hydroxide can be delivered in the canal system with a variety of instruments such as K files, intra-canal paste carriers, ultrasonic devises, rotary files and McSpadden compacter. 14 Intra-canal placement of calcium hydroxide has a direct effect on inflamed periapical tissue leading to periapical healing and bone formation. Calisken and Sen have demonstrated that the use of calcium hydroxide in the canal system as intra-canal dressing resulted in periapical healing and osseous regeneration. 15 It has been shown that application of calcium hydroxide for seven days is effective in removing bacteria from the canal system. 16 It has also been studied that even periapical cysts can be healed with calcium hydroxide intra-canal dressings by having a direct effect on the cystic lining and promoting osseous regeneration. 13
Conclusion
To completely eradicate microorganisms from the root canal system is difficult to achieve but with the help of modern endodontics and micro-endodontics with a basic understanding of the canal system can help in achieving excellent results for the treatment of periapical pathologies with a non-invasive approach. The intra-canal medicaments play an important role in inter-appointment dressings and help in providing an aseptic environment leading to better healing. The non-invasive approach should always be the first choice of the treatment.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Statement of Informed Consent and Ethical Approval
Necessary ethical clearances and informed consent was received and obtained respectively before initiating the study from all participants.