
Abstract
Introduction
By producing systemic nitric oxide (NO) from dietary inorganic nitrate, the enterosalivary nitrate–nitrite–nitric oxide pathway helps to promote vasodilation and regulate blood pressure (BP) and blood sugar levels. Nitrate reduction to nitrite, a crucial step in the production of NO, is facilitated by commensal bacteria in the mouth cavity. Consequently, regular mouthwash uses lowers oral cavity bacteria, which blocks the NO route.
Aim
The aim of this study was to know whether the regular mouthwash use increases risk of diabetes and hypertension.
Methodology
An electronic and manual search was performed on database like PubMed, Scopus, Google Scholar, and Science direct for search of publications with bolean operator “AND” & “OR” a total 210 articles were obtained out of these 7 study’s findings were found to require critical evaluation. Robvis tool and Joanna Briggs Institute (JBI) checklist were used for quality evidence.
Results
Out of seven studies, a rise in systolic and diastolic blood pressure was observed in four studies, one reported no change, one examined differential effects of mouthwash formulations on resting blood pressure, and one demonstrated an association with elevated diabetes levels. The quality of evidence varied across studies, ranging from high to moderate concern to low risk.
Conclusion
Considering the parameters in this review, these findings point to the possibility of distinct effects of commercially available mouthwashes with different concentrations. Frequent usage of an antibacterial mouthwash raises blood pressure and blood sugar levels while changing salivary and plasma nitrate/nitrite concentrations and NO pathway.
Keywords
Introduction
Commensals within the oral biofilm are implicated in the pathophysiology of conditions such as periodontal disease, dental caries, and halitosis. To prevent these problems, it is imperative to effectively control supragingival plaque. In addition to mechanical plaque reduction, mouthwash has become more popular as a way to lower oral flora and improve dental hygiene. 1 Mouthwash is widely accessible in many nations and dental health practitioners frequently encourage or recommend its use to help treat particular oral conditions. 2 It is found that mouthwash had beneficial effects in reducing gingivitis 3 and halitosis. The American Dental Association approves a few popular over-the-counter prescription antibacterial mouthwashes. About 90% of commercial mouthwash preparations include an antibacterial agent such as essential oils, triclosan, peroxide, cetylpyridinium chloride, alcohol, chlorhexidine, and fluoride. 4 At varying concentrations, these ingredients may act as bacteriostatic or bactericidal agents. According to a growing number of metagenomic research the oral microbiome may be related to systemic disorders including blood pressure control and diabetes. 5
The global prevalence of hypertension among individuals aged 30–79 years is estimated at 1.28 billion. According to the Global Burden of Disease (GBD) 2021 study, approximately 529 million people of all ages are living with diabetes, of whom nearly 485 million are adults aged 20–79 years. As per the World Health Organization (WHO) noncommunicable diseases (NCD) country profile (2018), 24% of Indian individuals aged 18 and above had elevated blood pressure with 24% of men and 23% of women having hypertension; the rates were nearly equal in both sexes. 6 According to the WHO, diabetes mellitus (DM) is among the top ten leading causes of death worldwide. Alongside other major NCDs such as cardiovascular diseases, chronic respiratory diseases, and cancer, diabetes represents a major global health emergency, accounting for approximately 1.6 million deaths and ranking as the ninth leading cause of mortality globally. 7
Nitric oxide (NO) plays a crucial role in regulating microvascular permeability, and impaired endothelial NO production via nitric oxide synthase (NOS) has been implicated in type 2 diabetes, 5 hypertension, 8 and cardiovascular diseases such as heart failure 1 and peripheral artery disease. 9 DM is particularly associated with the early onset of cardiovascular complications. Under physiological conditions, the endothelium provides protection against atherosclerosis, whereas pathological states are often characterized by reduced NO activity. The body’s two principal sources of NO are the endogenous l-arginine–NOS pathway and the exogenous nitrate–nitrite–NO pathway.10, 11 Reduced NO bioavailability may result from limited NOS substrate (l-arginine), depletion of essential cofactors, or impaired signal transduction due to NOS uncoupling. 12 Globally, hypertension remains one of the leading causes of premature mortality and disability. 13 Reduced NO bioavailability is related to hypertension14, 15 through loss of vasodilator directly along with indirect effects that magnify inflammation and oxidative stress which potentially result in vascular damage and hypertension. It is also a key element in maintaining cardiovascular homeostasis and metabolic activity and acts as a signaling molecule in many different types of physiological processes.16, 17
Due to the host’s active uptake of nitrate from the circulation and its production in saliva, the participation of oral bacteria in this process may actually reflect a symbiotic relationship. The bacteria convert nitrate to nitrite as a by-product, which is beneficial to the host because it is a source of NO and is crucial for numerous aspects of cellular function.18–20 A low-nitrate diet along with mouthwash use leads to disruption of the oral microbes, thus stopping lowering of oral nitrate and an elevation in blood pressure 21 and diabetes. It also draws attention to an unexpected function of the oral microbes in controlling blood pressure. 22
There have been some studies suggesting a possible link between frequent mouthwash use and an increased risk of diabetes and hypertension. The rationale behind such studies typically evaluated in this present systematic review with an aim to know whether the regular use of mouthwash increases the risk of diabetes and hypertension and also to know whether the concentration and type of mouthwash used influence the change in diabetes and blood pressure levels.
Methodology
Protocol and Registration
This systematic review was conducted in accordance with the PRISMA 2020 guidelines (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) and was prospectively registered in PROSPERO (CRD42023485664).
Research Question
Articles for this review are searched through the databases with incorporation of the PICO format in framing the research question “Does mouthwash use increases the risk of diabetes and hypertension?” where PICO refers to following:
Population (P): General population (adults without pre-existing diabetes or hypertension)
Intervention (I): Regular use of over-the-counter antibacterial mouthwash (e.g., twice daily)
Comparison (C): Infrequent or no use of mouthwash
Outcome (O): Impact on health (development of prediabetes/type 2 diabetes, or hypertension)
Search Strategy
An electronic and manual search was performed on PubMed, Science Direct and Google Scholar and Scopus database on studies related to the topic of “Over-the-contour/ regular usage of mouthwash increases the risk of pre-diabetes and hypertension” from the year 2011 to 2023. A total of 210 articles were found using keywords “over-the-counter,” “regular use,” “mouthwash use,” “risk of pre/diabetes,” “risk of pre/hypertension,” “impact on health,” “NO, nitrate–nitrite–nitric oxide pathway,” respectively, with a Boolean operator “AND” & “OR.”
Study Selection Process
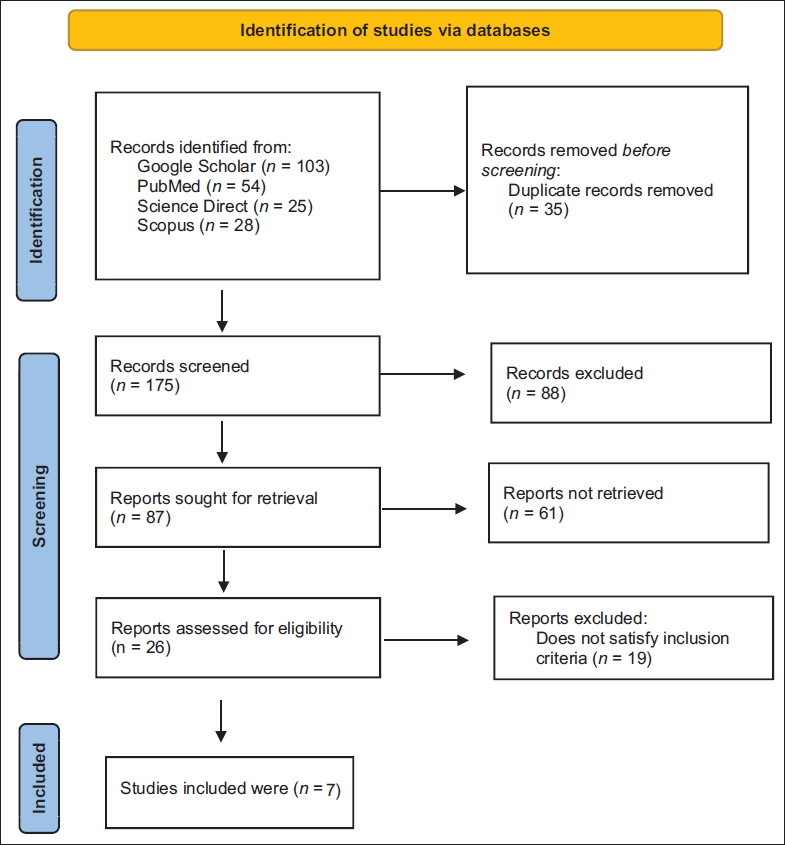
A total of 210 records were identified through database searches. After removing 35 duplicates, 175 titles and abstracts were screened. Of these, 88 records were excluded and 87 reports were sought for retrieval, and 61 reports were not retrieved. Following eligibility assessment, 26 reports were assessed for eligibility of theses 19 reports which do not satisfy inclusion criteria. At the end, seven reports met all criteria and were included in the final synthesis. The study selection process is illustrated in Figure 1 (PRISMA Flow Diagram).
PRISMA Flow Diagram for the Systematic Review Which Included Searches of Databases.
Selection Criteria
The inclusion criteria include:
Original research articles which were published in PubMed, Scopus, Science Direct, and Google Scholar. Studies published in English language showing “Mouthwash use and increase risk of pre-diabetes and hypertension both the over-the-counter and regular use.” Articles published within a period of 2011–2023. Studies with “pre-diabetes/ diabetes and pre- hypertension/ hypertension” as outcome.
The exclusion criteria were:
Systematic reviews, pilot studies, abstracts, letters to editor, case report, gray literature, narrative reviews, studies represented only in abstract format, and research not published in scholarly journals. Articles published in other languages were excluded.
Data Extraction
A meticulous description of the study characteristics (author, year, country, study design); sample size and age range, mouthwash intervention, and how it was carried out; biochemical variables included (oral nitrogen reducing capacity, salivary nitrate and nitrite, plasma nitrate and nitrite); other co-interventions if any and confounding variables; statistical tests; constraints; and conclusion were all extracted from the included articles. Owing to methodological and clinical heterogeneity across studies, a meta-analysis was inappropriate, and a narrative synthesis with supporting calculations was carried out. Quantitative findings were summarized in tabular form and described.
Assessment of Risk of Bias
The quality of randomized trials was evaluated using the Cochrane Risk of Bias Tool 2 (ROB 2), which assesses potential bias across five domains: (a) randomization process, (b) deviations from intended interventions, (c) incomplete outcome data, (d) outcome measurement, and (e) selective reporting. Each study was subsequently rated as low risk (all domains low), high risk (at least one domain high), or some concerns (one or more domains unclear, but none high). For cohort studies, methodological quality was appraised using the Joanna Briggs Institute (JBI) Critical Appraisal Checklist which contains 11-item checklist and for non-randomized controlled trial (RCT) with nine-item checklist.
Studies were categorized as follows:
High quality: JBI score ≥70% Medium quality: JBI score 50%–69% Low quality: JBI score <50%
Results
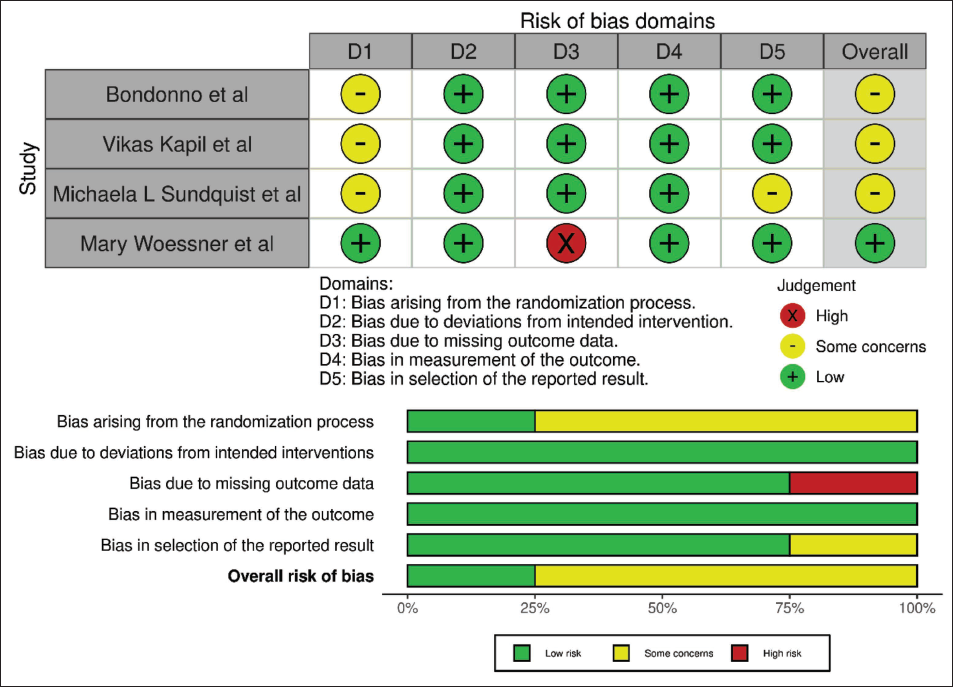
The Robvis tool was applied to appraise and visually present the risk-of-bias assessment for the included RCTs, which demonstrate variability in methodological rigor. Bondonno et al., 20 Kapil et al., 21 and Sundquist et al. 23 exhibited “some concerns” primarily related to the randomization process (Domain 1), which consequently influenced their overall bias judgment. In contrast, other domains were largely rated as low risk in these studies. Woessner et al. 24 demonstrated the most robust methodology, with low risk across nearly all domains; however, a high ROB was identified in relation to missing outcome data (D3). Despite this limitation, the overall assessment remained low risk, suggesting that the issue was not sufficient to substantially undermine study validity. Collectively, the analysis indicates that while the majority of studies are moderately reliable, caution should be exercised in interpreting findings due to recurring concerns regarding randomization and, in one instance, missing data. (Figure 2A and B) By using JBI critical evaluation tool, the two longitudinal studies showed medium quality of evidence and non-RCT showed high quality of evidence (Table 1).
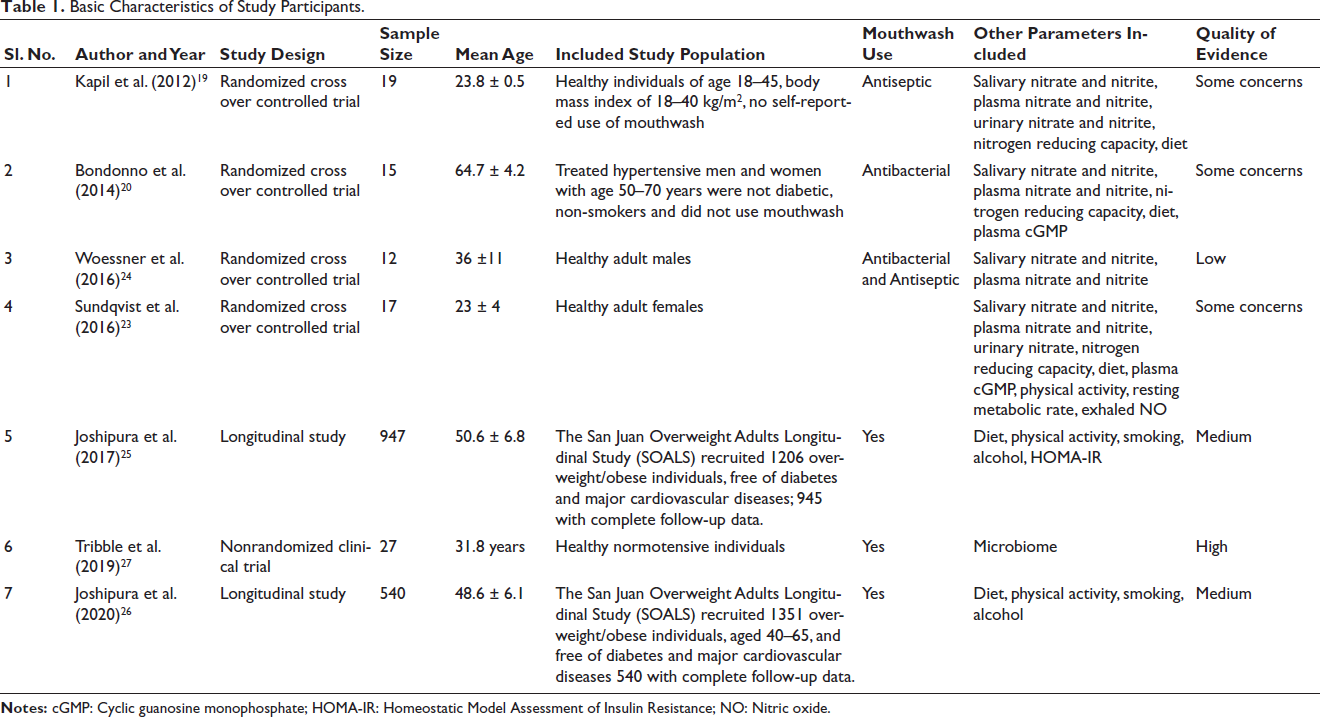
Basic Characteristics of Study Participants.
(A) Risk of Bias According to the Robvis Tool. (B) Summary of Risk of Bias According to Robvis Tool.
The studies published around three different countries during the time period of 2011–2023 were included. One-thousand five-hundred seventy-seven (1,577) subjects aged between 18 and 70 years in the randomized trials, longitudinal study, and non-RCT with follow-up period ranging from few days to 3 years were included. All of the 6 studies were focused on effect of mouthwash and nitrate–nitrite nitric oxide pathway on levels of blood pressure and one study focused on levels of diabetes in common. The basic characteristics such as study design, mean age, study population, type of mouthwash used, other parameters assessed, quality of evidence of each included research are shown in Table 1.
Table 2 summarizes findings from different studies assessing the effects of mouthwash or oral interventions on the nitrate–nitrite–NO pathway and related health outcomes. Overall, most studies consistently report a reduction in salivary nitrite and oral nitrate-reducing capacity (ONRC) following mouthwash use, indicating disruption of the enterosalivary nitrate–nitrite pathway. Salivary and plasma nitrate levels showed variable or nonsignificant changes across studies. Notably, multiple studies reported elevations in both systolic and diastolic blood pressure, supporting the biological plausibility that inhibition of oral bacteria-mediated nitrate reduction adversely affects vascular health. Additionally, Joshipura et al. 25 uniquely linked mouthwash uses with an increased risk of DM, highlighting potential systemic metabolic implications. Collectively, these findings suggest that frequent mouthwash use can impair oral microbial function, reduce NO bioavailability, and potentially elevate cardiometabolic risk.
Effect of a Mouth Rinse Intervention on Biochemical and Clinical Parameters in Various Studies.
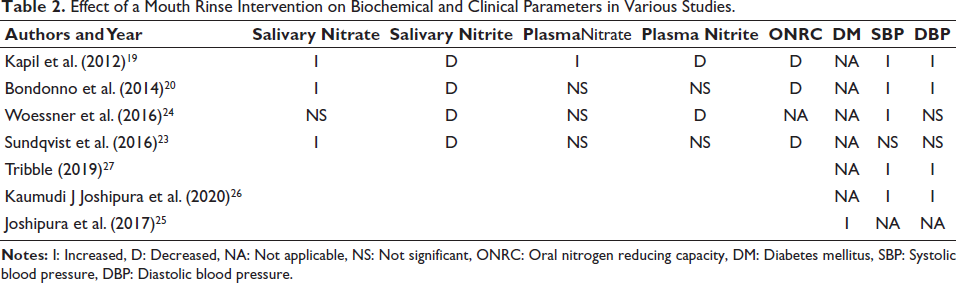
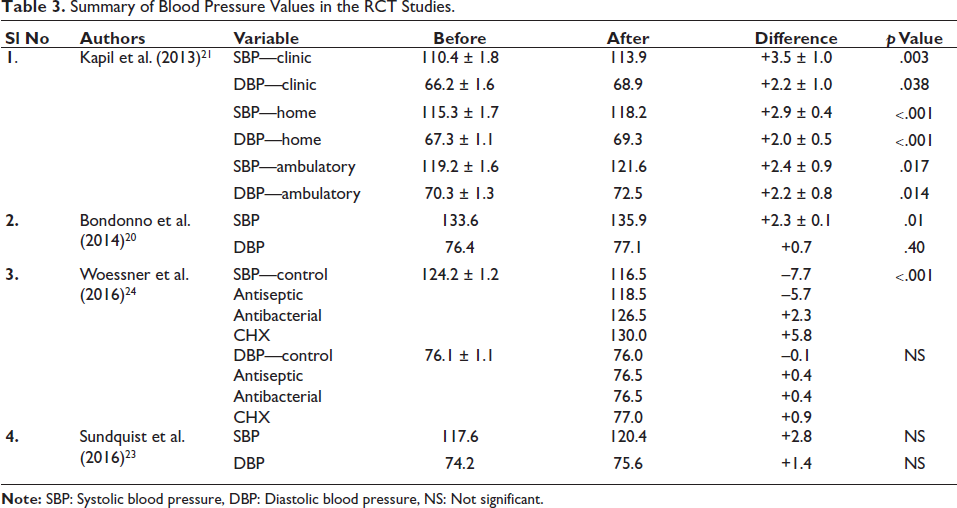
The reviewed RCT studies indicate that mouthwash use generally leads to a decrease in salivary nitrite and ONRC, with inconsistent effects on salivary and plasma nitrate levels. Plasma nitrite was largely reduced or not significantly altered. While a number of studies demonstrated rises in systolic and diastolic blood pressure, one study demonstrated an association with increased risk of DM. These findings support the disruption of the nitrate–nitrite–NO pathway with potential adverse effects on cardiometabolic outcomes (Table 3).
Summary of Blood Pressure Values in the RCT Studies.
Discussion
This systematic review presents compelling epidemiological evidence for an association between the mouthwash use and relative risk of hypertension and diabetes through NO pathway. Across the seven included studies, statistical findings of majority of the studies consistently highlight the use of mouthwash as a potential risk factor for increase in levels of hypertension and diabetes. The exact mechanism of action of mouthwash in NO pathway needs to be explored deeply, but one of the mechanisms explored and proposed to explain exactly how this impacts on general health is summarized as follows:
Use of antiseptic/antibacterial mouthwash disrupts the bacterial conversion of nitrate to nitrite in the oral cavity. This interruption of the enterosalivary circulation leads to reduced plasma nitrite levels, which have been associated with elevated blood pressure and diabetes. These findings highlight the critical role of oral nitrate-reducing bacteria in the regulation of blood pressure.
The four included RCTs were assessed for ROB using the Robvis tool, a web-based application developed to visualize ROB assessments in systematic reviews. The tool generates:
(1) “traffic light” plots displaying domain-level judgments for individual studies, and
(2) Weighted bar plots illustrating the distribution of ROB judgments across domains. Of the four RCTs, three were rated as having some concerns, while one was judged to have a low ROB. Other studies by using JBI critical evaluation tool, the two longitudinal studies showed medium quality of evidence and non-RCT showed high quality of evidence.
Mouthwash Use and Diabetes
Joshipura et al. were the first to investigate whether routine mouthrinse use may represent a risk factor for DM. Their findings showed that individuals who used mouthwash twice daily or more had higher levels indicative of risk and an increased likelihood of developing pre-diabetes or diabetes compared to less frequent users. These subjects used mouthwash mostly for teeth cleaning and breath refreshing. Along with numerous additional confounders that were evaluated, these associations held true regardless of physical activity, baseline age, waist size, sex, alcohol use, smoking, and hypertension. The observed associations remained consistent across multiple subgroups, indicating robustness and minimal confounding from lifestyle factors such as smoking and physical activity. As the cohort excluded individuals with baseline cardiovascular disease and diabetes, the observed associations likely operate independently of traditional diabetes risk factors. The findings suggest that routine antibacterial mouthwash use may adversely influence NO bioavailability, blood pressure, and diabetes risk, independent of major confounders, and could further impair glycemic control through shared NO-mediated pathways. 24
Mouthwash Use and Hypertension
Recent evidence indicates that oral nitrate-reducing bacteria play a critical role in the nitrate–nitrite–NO pathway. Nitrite is produced as a by-product when facultative anaerobic bacteria use salivary nitrate as an alternative electron acceptor instead of oxygen. 28 Salivary nitrate, actively concentrated from plasma, 29 is mainly obtained from dietary sources such as green leafy vegetables 30 and also generated via the l-arginine–NOS pathway. 31 Studies investigating dietary or supplemental nitrate have shown that antibacterial mouthwash abolishes the associated increases in salivary and plasma nitrite, as well as related vascular effects. 11
In view of this, a study conducted by Joshipura et al. concluded that participants who used over-the-counter mouthwash twice a day at beginning of the study had more risk of hypertension as diagnosed by a healthcare professional than those who uses less frequently and non-users. 26 When people with hypertension and normotension rinsed their mouths twice a day with chlorhexidine, the effects of exogenous nitrate-dependent increases in plasma and salivary nitrate and nitrite were eliminated, and their blood pressure improved.11, 21, 22, 32, 33
According to Bondonno et al. when treated hypertensive men and women used an antimicrobial mouthrinse twice a day for three days, their systolic blood pressure improved and their oral nitrate and plasma nitrite levels decreased, 22 and these results are equivalent to the results by Kapil et al., 21 oral nitrate to nitrite transition was almost completely eliminated after one week of twice-daily application of an antimicrobial mouthwash. Along this, there was an increase in blood pressure and a 25% drop in plasma nitrite content. Their claim that using antiseptic mouthwash prevents nitrate from being converted to nitrite results in an increase in blood pressure is supported by the link found between changes in plasma nitrite levels and changes in blood pressure.
A study by Tribble et al. 27 showed there is a change of at least 5 mm Hg in resting systolic blood pressure after CHX treatment. Overall, there is a substantial change in diastolic and systolic blood pressure when mouthwash is used frequently but according to Sundqvist et al. 23 there is no major shift in 24-hour ambulatory blood pressure neither during night nor day time and salivary nitrate levels were grown while salivary nitrite levels were decreased. There was no statistical difference in plasma nitrate and nitrite levels when mouthwash was handed-down for three days. A key difference between the Sundqvist et al. study and those by Kapil et al. 21 and Bondonno et al. 22 lies in the control of dietary nitrate intake. This study implemented stricter restrictions, allowing only four types of low-nitrate vegetables, whereas Kapil et al. 21 excluded high-nitrate vegetables and Bondonno et al. 22 permitted usual diets with only a low-nitrate breakfast before assessments. Given evidence that mouthwash interferes with dietary nitrate effects, it is possible that outcomes in these studies partly reflect blockade of exogenous nitrate, even at low levels. Dietary intake places a crucial role in regulating blood pressure and diabetes levels and is considered as the one of the confounding factors. Interestingly, all included studies reported that the use of antibacterial mouthwash led to a marked reduction in salivary and plasma nitrite when participants were maintained on a low-nitrate diet for 24 hours. Nitrate intake is generally linked to concomitant effects on blood pressure, with clinical trials demonstrating reductions following both acute and chronic supplementation.34–37 While certain studies noted declines in both systolic and diastolic blood pressure, others found reductions limited to either systolic or diastolic pressure.
The study by Woessner et al. was the only investigation to examine the differential effects of various commercially available mouthwash solutions on plasma and salivary nitrite concentrations, as well as resting blood pressure. Their findings indicate that “stronger” antibacterial rinses, such as Cepacol and chlorhexidine, which suppress the rise in both plasma and salivary NO₂, are associated with higher systolic blood pressure. Furthermore, systolic blood pressure was significantly lower under control (water) and antiseptic conditions compared to the antibacterial and chlorhexidine conditions. These results were obtained after controlling for potential confounding factors. 24
The findings of this review have important implications for both clinical practice and public health. While mouthwash is widely promoted for oral hygiene, the evidence suggests that its frequent antibacterial use may disrupt the nitrate–nitrite–NO pathway, potentially leading to adverse systemic effects such as elevated blood pressure and increased risk of diabetes. These results highlight the need for cautious recommendations regarding routine mouthwash use, particularly in individuals with existing cardiometabolic risk factors. Regarding applicability, the findings are relevant given the widespread global use of mouthwash. However, the variability in formulations, dosing, and population characteristics across studies constrains generalizability. While suggestive of a potential risk, current evidence is insufficient to establish causality.
Limitations include heterogenicity of the studies, differences in study designs, populations, interventions, and outcome measures which can make it difficult to compare results and draw meaningful conclusions. Differences in how studies report outcomes can make data synthesis challenging, and missing data can lead to biased conclusions. Future studies should employ larger, multicenter RCTs to enhance the reliability and generalizability of findings. Also, intervention studies can assess the enterosalivary route, mouthwash components with different concentrations and compositions and use dose-duration studies. Also, the included RCTs were limited by small sample sizes, short follow-up, heterogeneity in mouthwash type and dosage, and reliance on surrogate markers rather than clinical outcomes. Observational studies faced issues of self-reported exposure, recall bias, residual confounding, and limited causal inference due to cross-sectional designs. These limitations highlight the need for larger, long-term, and well-controlled studies.
Conclusion
The systematic review explores whether routine use of antibacterial mouthwash contributes to the risk of hypertension and diabetes. Evidence indicates that mouthwash may interfere with oral bacterial nitrate reduction, thereby reducing NO bioavailability, a key factor in vascular and metabolic health. This disruption could adversely affect blood pressure regulation and glucose control. Although the findings point to a potential link, further clinical research is necessary to confirm these associations and determine their clinical significance, to establish causality and clarify the long-term health implications of regular mouthwash use.
Footnotes
Acknowledgment
We would like to thank all those who were involved in this systematic review for their contribution, support, guidance, and reviewing the manuscript.
Authors’ Contribution
Sindhusha designed the systematic review. Sindhusha and Ravoori Srinivas conducted the literature search. Sindhusha collected and organized the data, performed data analysis, and prepared tables and figures. Sindhusha and Ravoori Srinivas were involved in manuscript writing. Srinivas Pachava edited and revised the final draft of the article. All authors have approved the final draft of the manuscript.
Data Availability
This study is based exclusively on data from previously published sources. No new data were created or analyzed in this work. Therefore, data sharing is not applicable to this article.
Declaration of Conflict of Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval: registered with PROSPERO (Prospective Register of Systematic Reviews) with registration number CRD42023485664 as it is a systematic review.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Not applicable. This systematic review did not involve collection of primary data or participation of human subjects; it is based entirely on analysis of already published studies.