
Abstract
Background:
Substance use is a global public health concern. However, how psychological stressors, such as job discrimination, mediate the association between substance use and holistic well-being is still unclear.
Methods:
Data were merged from the main and the biomarker projects of waves 2 to 3 of the Midlife in the United States (MIDUS) study. Using structural equation models, we examined whether participants’ (N = 1,729; Mage = 62 ± 10) substance use, assessed by the usage of 10 different non-prescription medications, predicts better holistic well-being, assessed by a composite flourishing score, including emotional, psychological, and social well-being, over time while controlling baseline flourishing and other covariates (sociodemographic, health, and functional status). We also examined whether individuals’ psychological stressors, assessed by a composite score of multiple aspects of discrimination, mediate the above association.
Results:
Findings revealed that individuals’ substance use has a negative and significant effect (b = −0.854; SE = 0.227; p < .001) on composite flourishing. Further, psychological stressors have a negative and significant association (b = −0.177; SE = 0.066; p = .008) with composite flourishing, and it also mediates the above association.
Conclusions:
The current study extends earlier research showing the impact of substance use on individuals’ well-being. Future research should examine biomedical mechanisms for potential aspects of substance use and psychological stressors on late-life holistic well-being.
Introduction
What constitutes well-being is a complex but essential concern to modern social sciences (J. J. Chen et al., 2022; Jarden & Roache, 2023). Well-being is considered a positive disposition of human beings influenced by social, economic, and environmental factors (World Health Organization, 2021). While a biomedical approach toward well-being cannot unfasten itself from disabilities and losses, another idea of well-being that argues for material resources, such as income and wealth, predict well-being also cannot affirm the contextual sense of well-being, indicating the need for a more holistic approach to well-being (Diener & Suh, 1997). Contextually, flourishing validates the individual’s well-being based on positive psychological growth; indeed, several positive psychology literatures acknowledge that it captures one’s emotional, psychological, and social feelings (Nguyen et al., 2020).
Flourishing is a psychosocial attribute that represents individuals’ overall well-being (Bhattacharyya et al., 2025). Huppert & So (2013) conceptualized flourishing as a combination of feeling good and operating effectively. This theoretical idea was constructed by combining two mental well-being concepts: hedonic, that is, feeling good, and eudemonic, that is, functioning well (Huppert & So, 2013; C. L. M. Keyes & Annas, 2009). Hedonic well-being emphasizes emotional well-being and is measured by life satisfaction and positive affect; in contrast, eudemonic well-being focuses on psychological and social well-being and is assessed by individuals’ subjective perception of life functionalities, such as autonomy, social integration, and personal growth (Huppert & So, 2013; C. L. M. Keyes, 1998).
Any deterioration from feeling and functioning well may force individuals to feel sad and consume substances. Substance use is a global public health issue. Substance use refers to substances such as alcohol, tobacco products, illicit drugs, and some other substances that are consumed by inhalation, injection, or pill (Centers for Disease Control and Prevention, 2024). In 2020, 49.9%, 24.7%, and 13.5% of the people in the US used at least one, three, and five prescription drugs in the past 30 days, respectively (Spencer et al., 2024). The excessive use of these substances deteriorates physical, mental, and emotional well-being and quality of life (Schulte & Hser, 2014), and later, individuals may develop substance use disorder. When substance use disorder creates a cyclic pattern, it hinders both recovery and the overall well-being of the individual (Office of the Surgeon General (US), 2016). Death rates attributed to substance misuse further undermine the importance of studying substance-related behaviors; in 2022, 107,941 deaths occurred due to drug overdose, and the age-adjusted rate was 32.6 deaths per 100,000 standard population in the United States (Spencer et al., 2024). The death due to drug overdose rate was found to be most common in the 35 to 44 years age group, and African American men were disproportionately affected (Spencer et al., 2024).
In this context, chronic stress is a long-lasting, ongoing stressor threatening individuals’ personal, professional, and health status (Schetter & Dolbier, 2011). Chronic stress is a well-known factor that may contribute to substance addiction (Sinha, 2024). Other risk factors include economic instability, discrimination at work, and a history of trauma or abuse, existing mental health issues, or chronic health issues, and exposed environments (Sinha, 2008). Social isolation and discrimination are increasingly seen as critical components of allostatic load and are growing concerns for physical and mental well-being (Brandt et al., 2022; Gary et al., 2022). Increased allostatic load can lead to dysregulation of multiple physiologic systems and higher risks of illness. Multiple forms of discrimination have been found to negatively impact health, through inflammatory pathways or stress responses (Byrd & Allen, 2023). Discrimination in many ways can cause stress by stimulating feelings of anxiety, hopelessness, and poor self-esteem (Brandt et al., 2022; Singh & Bhattacharyya, 2024). In fiscal year 2022, 81,055 new discrimination charges were received, 233,704 field office inquiries, and 143 new lawsuits were filed (U.S. Equal Employment Opportunity Commission, 2024). Chronic stressors in the workplace, such as inequality and discrimination, may occur due to workload demand, high expectations, risk of burnout, and exposure to hazards in the industrial environment (Schetter & Dolbier, 2011). Likewise, living conditions, such as poverty, lack of resources for improvement, and protection of mental and physical health, exacerbate stressors. While appraisal evaluations may vary, several studies have used aggregated self-reported burdens of discrimination, without focusing on a specific encounter (Byrd & Allen, 2023; Lawrence et al., 2022).
Purpose of the Study
Substance use, chronic stress, and well-being interact with each other, impacting individuals’ lives across adulthood. While existing literature emphasizes the direct relationship between substance use and physical and mental health outcomes, less research has been conducted examining the impact of substance use on the broader aspects of holistic well-being. Using Keyes’ theoretical concept of flourishing that combines hedonic and eudaimonic dimensions of psychosocial well-being (Huppert & So, 2013), the current study uses a nationwide longitudinal sample of US adults to understand the association between substance use and overall well-being over time. We also examined whether individuals’ psychological stressors, assessed by a composite score of multiple aspects of discrimination, mediate the above association while controlling for well-documented correlates of behavioral attributes, including sociodemographic and health factors. We hypothesized that (i) substance use would negatively affect flourishing scores and (ii) psychological stressors would mediate the association between substance use and flourishing.
Methods
Study Design
The current study used data from the Midlife in the United States (MIDUS) survey, a national, longitudinal study conducted from 1995 to 2014 (Tighe et al., 2021). Waves 1, 2, and 3 of this large study were conducted in 1995 to 1996, 2004 to 2005, and 2013 to 2014, respectively, through the phone and mailed self-administered questionnaires across the United States (Bhattacharyya et al., 2022; Hughes et al., 2018). This study examined participants enrolled in waves 2 to 3 (2004–2014) of the MIDUS study and had no missing observations (N = 1,729); we merged data from the main and biomarker projects. IRB approval for this study is not applicable because we analyzed a publicly available dataset through the Inter-University Consortium for Political and Social Research (Bhattacharyya & Molinari, 2024).
Measures and Procedure
Dependent Variables
Flourishing
We used holistic well-being as the dependent variable to assess a composite flourishing score that includes emotional, psychological, and social well-being at wave 3, based on Keyes’ conception (C. L. M. Keyes, 2002).
Emotional Well-Being
MIDUS assessed emotional well-being by two components: life satisfaction and positive affect (C. L. Keyes & Simoes, 2012). The life satisfaction score was measured based on a five-item SAQ; for each item, participants were asked to rate their life based on overall, work, health, relationship with spouse/partner, and relationship with children (Prenda & Lachman, 2001). Responses were coded from 0 (the worst) to 10 (the best). MIDUS averaged the scores for the relationship with spouse/partner and children to create one item; this score was then added with the remaining three items (life overall, work, health) to compute an overall (average) mean score, with higher scores reflecting better overall life satisfaction. Then, MIDUS computed the score for cases with valid values for at least one item on the scale (score range 1–10). The life satisfaction score was not calculated for cases with no valid item and was identified as missing data. Initially, we considered the average (mean) score provided in MIDUS for the entire range of responses on life satisfaction. Next, a six-item validated positive affect scale was used to measure how much the participants felt cheerful, in good spirits, happy, calm and peaceful, satisfied, and full of life over the past 30 days (Mroczek & Kolarz, 1998). Responses were coded from 1 (all the time) to 5 (none of the time). Then, responses were reverse coded to reflect higher scores as greater positive feelings. An overall positive affect score (ranged 1–5) was derived from averaging responses across items. For the current analysis, because life satisfaction and positive affect were assessed on different scales, the scores were then standardized, respectively (mean = 0, standard deviation [SD] = 1), and then summed to create an overall score for emotional well-being (α = .71).
Psychological Well-Being
Psychological well-being was measured based on Ryff’s Psychological Well-Being Scale (Ryff, 1989). The scale assessed six subdomains (three items per subdomain), consisting of autonomy (e.g., “I have confidence in my opinions, even if they are contrary to the general consensus”), environmental mastery (e.g., “I am quite good at managing the many responsibilities of my daily life”), personal growth (e.g., “I think it is important to have new experiences that challenge how you think about yourself and the world”), positive relations with others (e.g., “People would describe me as a giving person, willing to share my time with others”), purpose in life (e.g., “I sometimes feel as if I've done all there is to do in life”), and self-acceptance (e.g., “In many ways I feel disappointed about my achievements in life”). Responses were coded, ranging from 1 (strongly agree) to 7 (strongly disagree). Responses were reverse coded as necessary, indicating higher scores correspond with greater well-being. A score for each subdomain was created by adding responses for the respective three items under that subdomain. An overall psychological well-being score was created by summing responses of all six subdomains (α = .79).
Social Well-Being
We used C. L. M. Keyes and Shapiro’s (2004) 14-item scale to measure five subdomains of social well-being (three items per subdomain, except for two-item social coherence). The scale consisted of social coherence (e.g., “I cannot make sense of what’s going on in the world”), social integration (e.g., “I don’t feel I belong to anything I’d call a community”), acceptance of others (e.g., “People who do a favor expect nothing in return”), social contribution (e.g., “My daily activities do not create anything worthwhile for my community”), and social actualization (e.g., “Society isn’t improving for people like me”). Responses were coded, ranging from 1 (strongly agree) to 7 (strongly disagree), and reverse coded as necessary, reflecting higher scores for greater well-being. Each subdomain’s score was created by adding responses for items relevant to that subdomain. Because not all subdomains were measured on the same scale, each subdomain’s score was standardized separately and then summed to create an overall social well-being score (α = .74).
Because different scales in MIDUS assessed each domain’s scores, we standardized emotional, psychological, and social well-being scores and then summed them up to create a composite flourishing score (Y. Chen et al., 2018); finally, we used a continuous measure of flourishing to assess holistic well-being.
Key Independent Variable
The non-medical usage of substances was used as the key independent variable. Participants responded to the question, whether during the past 12 months they ever used any of the following substances on their own – (a) “Sedatives, including either barbiturates or sleeping pills (e.g., Seconal, Halcion, Methaqualone)?” (b) “Tranquilizers or nerve pills (e.g., Librium, Valium, Ativan, Xanax)?” (c) “Amphetamines or other stimulants (e.g., Methamphetamine, Preludin, Dexedrine, Ritalin, “Speed”)?” (d) “Analgesics or other prescription painkillers (Note: This does not include normal use of Aspirin, Tylenol without codeine, etc., but does include use of Tylenol with codeine and other prescribed painkillers like Demerol, Darvon, and Percodan)?” (e) “Prozac or other similar prescription medications to treat depression on your own)?” (f) “Inhalants that you sniff or breathe to get high or feel good (e.g., Amyl nitrate, Freon, Nitrous oxide (“Whippets”), Gasoline, Spray paint)?” (g) “Marijuana or Hashish?” (h) “Cocaine, Crack, or free base?” (i) “LSD or other Hallucinogens (e.g., PCP, Angel dust, Peyote, Ecstasy (MDMA), Mescaline)?” (j) “HEROIN?” MIDUS coded the responses as a binary variable (0 = no, 1 = yes). By “on their own,” MIDUS identified whether the use was either without a doctor’s prescription, in larger amounts than prescribed, or for a longer period than prescribed. In the current analysis, we constructed a composite categorical variable by summing up the above-mentioned 10 responses to assess potential dose-response effects of substances used. Additionally, we also categorized the reported drugs. Because very few respondents identified themselves as a user of sedatives or tranquilizers and because these terms often overlap, we combined them as “sedatives.” For those who use painkillers and marijuana and hashish, we created two categories, “painkillers” and “cannabis,” respectively. As only handful of respondents reported each of the remaining drugs, we combined them as “other drugs” category.
Mediator Variable
Chronic Stressor
We used individuals’ chronic stressors in wave 2 as the mediator variable. Chronic stressors were assessed by a composite stressor score, including respondents’ perceived inequality in work/unfairness at work, chronic job discrimination, perceived lifetime discrimination, and perceived daily discrimination, based on Byrd and Allen’s (2023) conception, with an overall acceptable internal consistency (α = .75; Raharjanti et al., 2022).
For the last three measures, items were reverse-coded reflecting high scores as higher values in MIDUS dataset. For items with a missing value, the mean score of completed items was considered. Because each domain’s scores were measured on different scales, we standardized each component of chronic stressor scores (mean = 0, SD = 1), and then summed up to create a composite chronic stressor score (Byrd & Allen, 2023; Doyle & Molix, 2014).
Covariates
We included baseline sociodemographic, health, and functional factors as covariates. Sociodemographic variables included age, gender, race, marital status, education, and employment. While age (0 ≤ 65, 1 ≥ 65), and gender (0 = male, 1 = female) were measured as binary variables, race (1 = White, 2 = Black, 3 = other) was measured in three categories; in contrast, marital status (1 = married, 2 = separated/divorced, 3 = widowed, 4 = never married) and educational level (1 = no/some school, 2 = high school graduate/in college, 3 = graduated from college, 4 = having master’s/professional degree) were measured in four categories, and employment status in five categories (1 = working, 2 = self-employed, 3 = retired, 4 = unemployed, 5 = other; as Fearn & Bhattacharyya, 2024).
Regarding health and functional status variables, first, participants were asked to rate their current physical and mental health on a five-point scale ranging from 1 (excellent) to 5 (poor). We recoded the responses for self-reported physical and mental health as good (including responses “excellent,” “very good,” and “good”) and not good (including responses “fair” and “poor”). We also included additional variables related to health, including body mass index (BMI; 1 = underweight [<18.5], 2 = normal [18.5–24.9], 3 = overweight [>24.9–29.9], and 4 = obese [>29.9]) and tobacco and alcohol use (1 = regular tobacco/alcohol user, or 0 = not) and chronic condition/s (1 = yes, 0 = no). Chronic conditions included high blood pressure, stroke, heart problems, high cholesterol, diabetes, cancer, lung problems, ulcers, and aches/joint stiffness in the past 12 months. We also considered whether the participants were sad in the last 2 weeks. Finally, because early childhood trauma has been well documented as significant correlate of emotional, psychological, and social well-being across adulthood (Burns et al., 2024), we also considered this variable as a potential confounder in our analysis. We constructed early childhood trauma by summing up responses for emotional abuse, physical abuse, sexual abuse, emotional neglect, physical neglect, and minimization/denial (α = .81; Burns et al., 2024). We also adjusted baseline (wave 2) flourishing, as a covariate to reduce potential reverse causation.
Statistical Analysis
Preliminary analyses examined participants’ demographics, health, and functional status in the total sample and in the sample stratified by substance use status at wave 2. We then used structural equation models (SEM) to examine whether individuals’ substance use in wave 2 is associated with better flourishing over 10 years (assessed in wave 3) while controlling baseline flourishing and covariates (sociodemographic, health, and functional status). Additionally, we assessed if chronic psychological stressors, which were assessed as a composite measure of discrimination, mediate the above association. We chose SEM for its usefulness in dealing with both observed and latent variables, especially complex psychological or social constructs, and providing more accurate estimates of relationships between constructs; further, SEM fit indices evaluate how well the proposed model represents the data. Despite a traditional mediation analysis evaluates variables in successive waves while examining the causal effect on the outcome (Hayes, 2015), a half-longitudinal mediation analysis identifies mediators’ roles in two-wave studies evaluating the contemporaneous relations between either the predictor and the mediator or the mediator and the outcome (Bhattacharyya et al., 2024; Cole & Maxwell, 2003). We applied a half-longitudinal design in the current SEM analyses to evaluate whether respondents’ concurrent chronic stressors mediate the associations between substance use and flourishing. Statistical significance was evaluated at p < .05 (two-sided). Unstandardized regression coefficients (b) and standard errors (SE) are reported. All statistical analyses were conducted with Stata 18.5 SE (College Station, TX) software.
Results
Table 1 shows the descriptive statistics of the analyzed variables, including respondents’ sociodemographic and health status at wave 2 for the total sample and sample stratified by substance use status. A total of 1,729 individuals (who participated in all 1–3 waves of MIDUS) aged 30 to 81 years (Mage = 52 ± 10) in wave 2 (i.e., Mage = 62 ± 10 in wave 3) were included in the analysis. Women comprised 52% of the sample, 75% were employed, and 93% were White. Substantial proportions of participants were alcohol users (63%); 33% of the sample had normal BMI. The findings revealed that only 11.5% of participants were substance users. The mean score of participants’ composite flourishing was 1.0 ± 8.3 at wave 2, which is significantly lower among substance users.
Comparison of Participant Characteristics of US Adults in MIDUS Wave 2 (n = 1,729).
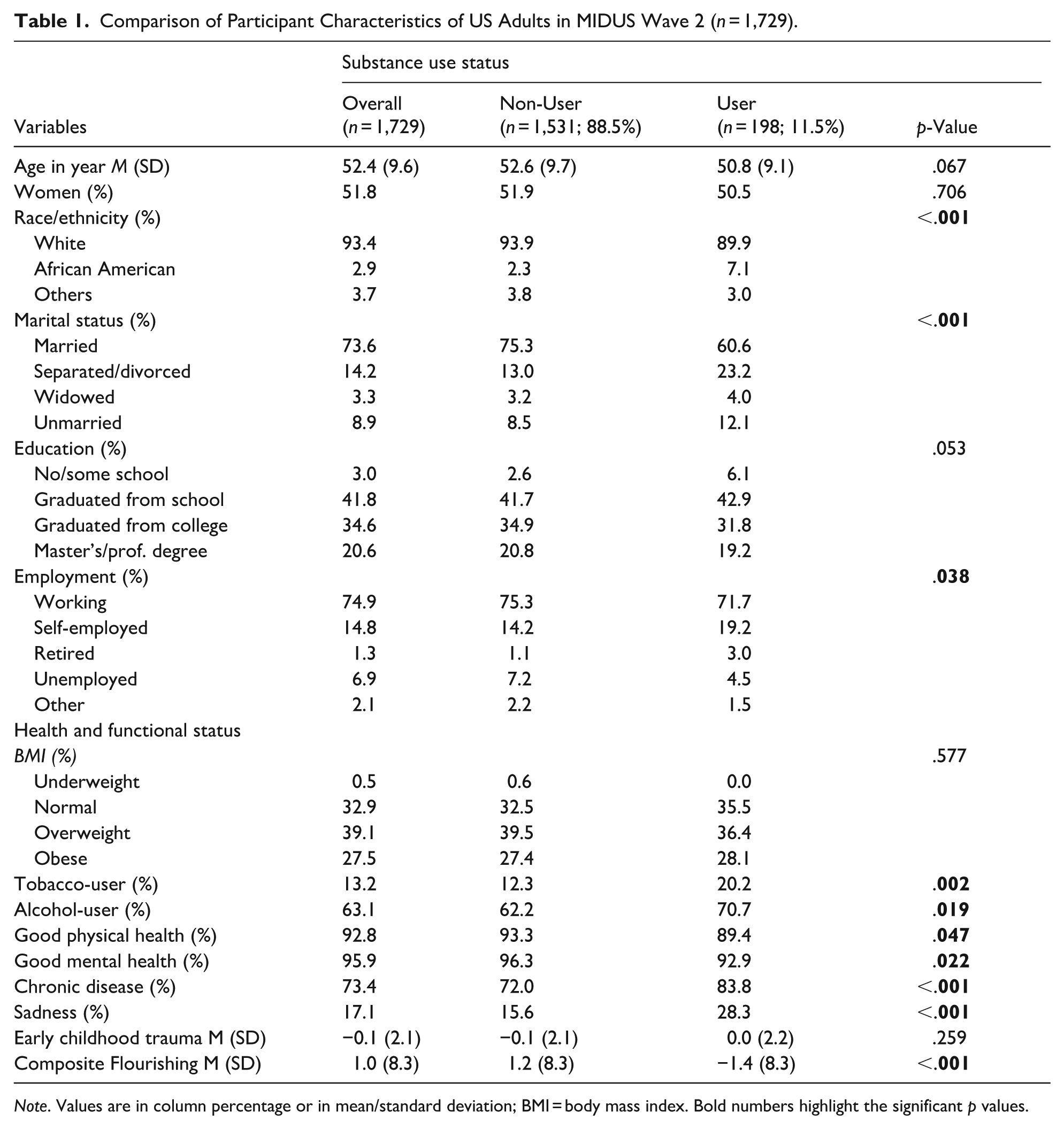
Note. Values are in column percentage or in mean/standard deviation; BMI = body mass index. Bold numbers highlight the significant p values.
Table 2 presents parameter estimates from the SEM showing direct effects of substance use (as a composite construct) on flourishing over the 10-year study period, without involving covariates, that is, zero-order model. Findings revealed that individuals’ substance use has a negative and significant effect (b = −0.785; SE = 0.226; p < .001) on the composite score of flourishing. While substance use has a significant positive association with chronic psychological stressors (b = 0.405; SE = 0.095; p < .001), which also have a negative and significant association (b = −0.190; SE = 0.065; p = .004) with composite flourishing, indicating that chronic psychological stressors mediate the relationship between substance use and flourishing over time.
Zero-order Structural Equation Model Examining Associations of Substance Use, Chronic Stressors, and Flourishing in Mid and Later Life, n = 1,729.

Note. W2 = wave 2; W3 = wave 3. Bold numbers highlight the significant p values.
Table 3 presents parameter estimates from the SEM showing direct effects of substance use (as a composite construct) on flourishing over the 10-year study period (full model). After controlling baseline (wave 2) sociodemographic and health factors and flourishing, findings revealed that individuals’ substance use has a negative and significant effect (b = −0.854; SE = 0.227; p < .001) on the composite score of flourishing. Further, substance use has a significant positive association with chronic psychological stressors (b = 0.179; SE = 0.090; p = .046) which also have a negative and significant association (b = −0.177; SE = 0.066; p = .008) with composite flourishing, indicating its mediating role in the association between substance use and flourishing over time. For a visual representation of the main findings from Table 3, Figure 1 illustrates the schematic path diagram showing the pathways linking the key independent variable (substance use), mediator (chronic stressors), and outcome (composite flourishing) for the SEM analysis (effects of covariates not shown in the diagram). The model fit was good for the analyzed model (comparative fit index [CFI] = 0.90, root means square error of approximation [RMSEA] = 0.05, and standardized root means squared residual [SRMR] = 0.02).
Structural Equation Model (Full Model) Examining Associations of Substance Use, Chronic Stressors, and Flourishing in Mid and Later Life, n = 1,729.

Note. BMI = body mass index; W2 = wave 2; W3 = wave 3. Bold numbers highlight the significant p values.

Path diagram showing the pathways linking the key independent variable (substance use), mediator (chronic stressors), and outcome (flourishing) for the structural equation model (full model), n = 1,729.
We also analyzed the associations between substance use, chronic stressors, and each component of flourishing separately. SEM analyses in Table 4 (full models) show that individuals’ substance use has a negative and significant effect on both emotional (b = −0.217; SE = 0.054; p < .001) and psychological (b = −0.637; SE = 0.133; p < .001) well-being but this effect was not found with social well-being. However, chronic stressors mediate the association between substance use and each component of flourishing over time. Figure 2 illustrates the schematic path diagram showing the pathways linking the key independent variable (substance use), mediator (chronic stressors), and outcome (each component of flourishing) for the SEM analysis (effects of covariates not shown in the diagram).
Structural Equation Model (Full Model) Examining Associations of Substance Use, Chronic Stressors, and Components of Flourishing in Mid and Later Life, n = 1,729.

Note. W2 = wave 2; W3 = wave 3. Bold numbers highlight the significant p values.

Path diagram showing the pathways linking the key independent variable (substance use), mediator (chronic stressors), and outcome (components of flourishing) for the structural equation model (full model), n = 1,729.
Additionally, we also analyzed the associations between each category of substance use, chronic stressors, and flourishing over the 10-year study period (full model; see Table 5). Findings revealed that sedatives (b = −1.263; SE = 0.559; p = .024), cannabis (b = −1.930; SE = 0.636; p = .002), and other drugs (b = −1.285; SE = 0.498; p = .010) have negative and significant effects on flourishing. Although chronic stressor has significant negative effects on flourishing, it does not mediate the associations of flourishing with sedatives, cannabis, and other drugs. However, the same effect was not found for painkillers; although painkillers do not have significant effect on flourishing, chronic stressor mediates their association.
Structural Equation Model (Full Model) Examining Associations of Various Categories of Substance Use, Chronic Stressors, and Flourishing in Mid and Later Life, n = 1,729.

Note. Effects of covariates not shown in the models. W2 = wave 2; W3 = wave 3. Bold numbers highlight the significant p values.
Discussion
Our study makes a unique contribution to the existing literature by providing longitudinal evidence showing a direct and negative impact of individuals’ substance use on late-life flourishing. Supporting our first hypothesis, the findings suggest that people with higher substance use are more likely to have poorer holistic well-being. Regarding our second hypothesis, chronic stress, in addition to negatively impacting flourishing, also influences the relationship between substance abuse and flourishing in both zero-order model and full model. However, its non-identical association with each component of flourishing indicates that chronic psychological stress factors associated with substance abuse may not fully account for the well-being outcomes. Instead, other psychosocial, cultural, or health-related factors may play roles in shaping these associations.
Despite a growing concern on late-life holistic well-being, studies exploring relationships between substance use, psychological stressors, and flourishing are limited. Relatedly, existing prior studies consistently demonstrated substance abuse to be associated with reduced quality of life (Armoon et al., 2023; Rand et al., 2020). For instance, a systematic review revealed that people with substance use experience a 40% to 60% reduction in overall quality of life compared across physical, mental, and environmental domains in comparison to the general population (Bratu et al., 2023). While quality of life is a more subjective evaluation of individuals’ position in life within the context of their culture and values (H. W. J. Chen et al., 2023; Marzo et al., 2023), flourishing is a broader multidimensional sense of thriving that are not captured in quality-of-life assessments (Y. Chen et al., 2018). Moreover, although flourishing provides a comprehensive picture of health, well-being, and wholeness in later life (Y. Chen et al., 2018), only a few earlier studies investigated the relationship of substance abuse with various components of holistic well-being, such as psychological, social, and emotional well-being, in different demographics.
A consistent and negative association was observed in the relationship between substance abuse and psychological well-being (Aiyappan et al., 2018). For example, a survey conducted on South African adolescents reported that use of illicit drugs had significantly lower levels of psychological well-being and life satisfaction compared to their non-using peers (Visser & Routledge, 2007), indicating that substance abuse may lead to a possible increase in poor psychological well-being among other age-group individuals. Our findings corroborate with earlier research. Moreover, substantial evidence shows that substance use increases the risk of mental health problems, such as depression, anxiety, and self-harm. These conditions are often present as comorbidities among individuals with substance abuse disorders, further deteriorating their psychological well-being (National Institute on Drug Abuse, 2020). These results explain how illicit drug substances are in various ways. On the one hand, lowering self-esteem and self-worth cause depression and anxiety, and on the other hand, leading to negative behavioral changes result in reduced cognitive performance, impaired decision making, and emotional detachment, impacting individual behaviors (Fish, 2012). These findings warrant the need for more psychological well-being interventions to support individuals with substance use issues in their treatment and recovery, addressing co-occurring mental health conditions and implementing interventions that aim to enhance overall psychological well-being.
Contextually, prior research revealed a negative association between substance abuse and social well-being (McDonald et al., 2011; Preller et al., 2014). The relationship may be shown to have effects through various pathways; evidence has shown that people with substance abuse struggle to maintain good relationships with their families and communities due to frequent conflict, financial strain, loss of friendship, and low cohesion (de Espíndola et al., 2020; Ebiai et al., 2023). These challenges deteriorate their social network and social support, which are often found to be beneficial attributes for substance abuse recovery, lowering their social well-being and reducing the support system needed for proper treatment and recovery (Birkeland et al., 2021). Likewise, another pathway is through stigma and shame against substance use disorder patients. Research has shown that individuals with substance abuse problems experience social stigma, discrimination, and exclusion (Kennedy-Hendricks et al., 2017). For example, one study conducted among opioid overdose patients found that 40.5% of patients self-reported experiencing drug-related discrimination in emergency departments. Similarly, a national survey found that 18.5% reported biased treatment from police, and 16.2% reported being unable to get a job (Nolen et al., 2023). This social stigma often leads to internalized stigma and perceived shame, ultimately affecting help-seeking behavior, treatment outcomes, and delivery (Benz et al., 2021; L. Chen et al., 2022), further leading to marginalization, social exclusion, and poorer social wellbeing (Wesselmann & Parris, 2021). These results highlight the consideration of rebuilding social networks and social support systems for sustainable and meaningful recovery from substance use. However, the current findings are not in line with the above research. Contextually, research revealed a varied effect of social support status on substance use; while higher quality seemed beneficial, higher quantity was yielded as a risk factor (Spohr et al., 2019). Further, substance use has been found to help some individuals maintaining stable social lives despite addiction (Spohr et al., 2019). Future research may help us show more directions on this issue.
Although research examining the relationship between substance abuse and emotional well-being is limited, existing evidence suggests that substance abuse disorders impair individuals’ ability to regulate their emotions. This impairment leads to higher negative emotionality compared with individuals without substance use (Garke et al., 2021). A systematic review found that substance users scored significantly higher on the Difficulties in Emotion Regulation Scale, with a mean difference of 21.33 (95% CI), indicating greater challenges in emotional regulation (Stellern et al., 2023). Our findings echo the above results.
In addition, our findings on sociodemographic covariates indicate that females are positively associated with flourishing, corroborating earlier research that females exhibit better flourishing compared to males (Schotanus-Dijkstra et al., 2016). There is evidence of positive associations between African Americans and flourishing; African Americans are also more associated with substance use compared to “other” racial pattern; the above findings corroborate with earlier research (Broman et al., 2008; Mahlobo et al., 2025; Spencer et al., 2024). Further, in line with earlier research (Y. Chen et al., 2018; VanderWeele et al., 2025), married (compared to their non-married counterparts) and higher educated individuals have been found to be positively associated with better flourishing.
Limitations
Our study has some limitations. Most importantly, participants’ baseline cognitive status was not screened in the MIDUS survey, making it hard to comment on participants’ neurocognitive status. A retrospective collection of responses was also a concern for recall bias. Further, despite our inclusion of several sociodemographic and health factors as control variables, other factors, such as informal caregiving, early childhood adversity, and cultural status, could affect the outcomes. Finally, a White predominance in the study population may also raise a generalizability concern.
Conclusion
Despite the above limitations, the current findings provide important contributions to research on well-being. Chronic stress is an established risk factor for substance abuse as a means of coping mechanism. Conversely, people with substance use disorders have increased susceptibility and vulnerability to chronic stress, creating a vicious cycle. Similarly, other studies have shown that chronic stress greatly reduces well-being and quality of life (Schotanus-Dijkstra et al., 2016). While our research has shown that multiple forms of discrimination as chronic stress reduce the flourishing score, they do not act as mediator between substance abuse and flourishing. These findings suggest that other factors may influence the link between substance abuse and flourishing, highlighting the need for further research in these areas. Health policies should prioritize lowering the prevalence and severity of substance use, particularly in later life, through sustained education, more community participation, workforce development, increased screening programs, integrative management, and early intervention.
Footnotes
Acknowledgements
None.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.