
Abstract
Background:
Cardiovascular health is associated with various trajectories of holistic well-being. However, how various psychosocial factors may impact the associations between cardiovascular health and well-being across adulthood is still underexplored.
Methods:
We examined participants enrolled in waves 1–3 (1995–2015) of the Midlife in the United States (MIDUS) study (N = 2,536). We measured holistic well-being by a composite flourishing score that included emotional, psychological, and social well-being, and categorized cardiovascular health status based on the parameters of Life’s Essential-8 defined by the American Heart Association. We used a multiple linear regression model to examine whether ideal cardiovascular health is associated with better flourishing over 10 years and further examined whether long-term rural living or intermittent rural living moderates the cardiovascular health-flourishing association, compared to no rural living, while controlling baseline flourishing score and socio-demographic and health status.
Results:
Findings suggested that only 12.5% of participants had high cardiovascular health status. Ideal cardiovascular health at wave 2 was positively associated with flourishing at wave 3 (b = 0.332; SE = 0.150; p < .05). However, rural/urban living contexts do not moderate the above relationship.
Conclusions:
Future research should explore whether these associations vary in more vulnerable populations, such as long-term care residents, warranting new policy and practice recommendations.
What this paper adds
The current study revealed that, although only 12.5% of participants had high cardiovascular health status, individuals’ better cardiovascular health is associated with higher levels of holistic well-being over time.
Additionally, the findings suggest that higher age is associated with lower well-being.
While rural living was often considered a low socioeconomic condition in late adulthood, the association between cardiovascular health and well-being is independent of rurality.
Applications of study findings
The current findings have direct practical applications, highlighting that one macro-level factor, i.e., the rural or urban living context, has no directional impact on cardiovascular health and well-being association over time.
Future research should examine mechanisms for the impact of other socioeconomic and cultural factors on cardiovascular health and well-being association across adulthood.
Novel policy and practice recommendations are needed to validate the current findings on more vulnerable populations, such as long-term care residents.
Introduction
How we perceive health and well-being continues to be dominated by the biomedical approach; even the World Health Organization’s emphasis on “. . .the absence of disease,” while defining health, often limits the opportunity for individuals and populations to strive for greater well-being despite diseases (Schramme, 2023). Further, this disease-centric approach fails to acknowledge the remaining strengths of life beyond disability, loss, and medical treatment (Bhattacharyya, Craft Morgan, et al., 2022). Conversely, another objective approach to well-being argues that economic factors, such as income and wealth, predict well-being; while these material resources may contribute to well-being, they cannot guarantee the contextual sense of well-being (Diener & Seligman, 2004). The gap between these two approaches highlights the need for a more holistic approach to what constitutes well-being, one that enables individuals to strive for a comprehensive state of health and well-being in their lives, regardless of their medical or economic circumstances.
Earlier well-being constructs were largely scattered; for example, the Salutogenic health model focuses on health promoting factors rather than pathogenesis (Antonovsky, 1996). Chinese medicine (Unschuld, 1985) and Ayurveda (Lad, 2002) emphasize holistic harmony within the body and environment, while Hettler (1976) considered dimensions of quality of life in his Six-Dimensions of Wellness Model. Other measures include life satisfaction scores (Vittersø et al., 2005), self-acceptance or meaningfulness (Cordaro et al., 2024), and self-rated scores of psychological health or happiness grounded in a foundation of the absence of diseases or risk factors (Abdel-Khalek, 2006), which adopt a unidimensional approach. However, these constructs faced criticism for failing to capture an individual’s potential and sense of fulfillment (Lindert et al., 2015). Recognizing the need for more comprehensive and multidimensional metric tools to measure well-being, the concept of flourishing aims to provide a nuanced approach to understanding well-being. Several research efforts were conducted to understand and expand flourishing’s theoretical paradigm for definition and measurement (Lomas et al., 2025); however, flourishing’s use in a well-being study can help one understand the need to strive for well-being that is beyond the absence of diseases or metrics fulfillment of economic-focused outcomes per se income and longevity (Diener & Seligman, 2004; Shiba et al., 2022).
Although an all-encompassing theory on holistic well-being has yet to be developed, a growing body of positive psychology literature emphasizes flourishing as a measure of holistic well-being (Keyes & Simoes, 2012). Flourishing is identified as a psychosocial attribute of an individual’s overall well-being. Although there is no universally accepted definition of flourishing, and the concept constantly evolves, currently, according to Huppert and So (2013, p. 838), “Flourishing refers to the experience of life going well. It is a combination of feeling good and operating effectively. Flourishing is synonymous with a high level of mental well-being, and it epitomizes mental health.” This concept was derived from combining two conceptual ideas of mental well-being: hedonic, i.e., feeling good, and eudemonic, i.e., functioning well (Huppert & So, 2013; Keyes & Simoes, 2012). While the former idea centered on emotional well-being through the self-reported measurement of satisfaction with life and positive effects, the latter idea centered on psychological and social well-being, assessing the subjective outlay on how individuals see themselves functioning in their life, such as autonomy, social integration, and personal growth (Huppert & So, 2013; Keyes, 1998).
Cardiovascular Health
Cardiovascular health (CVH) refers to the well-being of the heart and blood vessels, which are responsible for blood circulation (Teshale et al., 2023). Globally, cardiovascular diseases are the top cause of death; in 2021, nearly 20.5 million people died due to cardiovascular diseases (Di Cesare et al., 2024). Eighty percent of the deaths are linked to heart attacks and strokes, with one-third of deaths occurring prematurely before the age of 70 years (GBD 2019 Diseases and Injuries Collaborators, 2020). When CVH is in good working order, it helps other systems operate effectively and efficiently. However, the deterioration of CVH can cause severe financial and mental hardship and distress (Teshale et al., 2023) and functional limitations that lead to poor life satisfaction, quality of life, and reduced longevity (Lloyd-Jones et al., 2022; Parlati et al., 2024).
Recognizing the importance of establishing metrics to help prevent poorly functioning CVH and promote positive CVH, the American Heart Association (AHA) developed standardized metrics in 2010 based on clinical and population health studies. In 2022, the AHA updated and refined the metrics to address the prior limitations and incorporated sleep health as a key component, resulting in the development of Life’s Essential 8 (LE8; Lloyd-Jones et al., 2022). The LE8 encompasses eight components of CVH: healthy diet, adequate sleep, participation in physical activity, avoidance of nicotine, sleep health, a healthy body mass index, and healthy levels of blood lipids, blood glucose, and blood pressure (Lloyd-Jones et al., 2022). Numerous studies have utilized LE8 as a comprehensive metric to assess its association with both mental and physical health outcomes. Regarding mental health, research has been conducted to observe an association of LE8 with mental conditions, such as depression, anxiety, migraines, and cognitive decline, indicating that individuals with higher LE8 scores tend to have a lower risk of mental health disorders and better overall mental health outcomes (Lei et al., 2024; Zeng et al., 2024). For physical health, research has investigated its relationship with various risk factors (e.g., liver abnormalities, cardiometabolic risk, metabolic, and other biomarkers), and health outcomes (e.g., fertility, cancer, kidney diseases, psoriasis, and stroke); findings suggest that poorer LE8 increased the likelihood of risk factors, reduced survival rates, and increased complications (Hao et al., 2025; Wang et al., 2022).
Several past studies explored how macro contexts, such as race, ethnicity, and culture, impact different psychosocial attributes in adulthood (Bhattacharyya & Molinari, 2024; Gutchess & Rajaram, 2023; Menkin et al., 2017); however, research emphasizing the association between individuals’ living contexts, such as urban vs. rural, and mid/late-life well-being in the United States is limited. The rural population in the US accounts for around 15 percent of the total US population (Dobis et al., 2021) and has greater challenges in several social determinants of health, including availability of healthcare services (Gong et al., 2019), food security (Brinkley & Visser, 2022), transportation accessibility and insurance coverage (Nganje & Addey, 2019), and many others compared to their urban counterparts (Lewis-Thames et al., 2022). Additionally, evidence indicates that the infrastructure resource development over the last few decades has prioritized urban areas over rural ones (Thang et al., 2023). With population aging, structural inequities worsen access to and utilization of quality care resources; these disparities contribute to poorer morbidity and mortality outcomes in rural areas, warranting policies and financial reform (Lewis-Thames et al., 2022).
Earlier studies also identified compromised well-being in rural populations compared to their urban counterparts (Kanning et al., 2023). The underlying factors may include lower socioeconomic status, such as limited education, unemployment, rural-urban migration, or reduced access to healthcare resources (Saenz et al., 2018). Conversely, certain elements of urban living may negatively impact on the quality of life, including exposure to higher levels of air pollution, persistent psychosocial stressors, and unhealthy lifestyles (Saenz et al., 2018). Thus, the directionality of associations between rurality/urbanicity and well-being shows mixed findings (Prati, 2024). The impact of rurality on subjective well-being is a complex interplay of personal and contextual characteristics, and the inconsistencies may be due to unclear rural-urban definitions or related to the rural happiness paradox or the urban paradox (Prati, 2024). Furthermore, it was also found that while stress and subjective well-being were associated with diet, physical activity, and body mass index, these associations varied by individuals’ living contexts, specifically rural versus urban (Gold et al., 2023). Moreover, current research on rural-urban differences in longitudinal psychosocial well-being outcomes in relation to major chronic conditions, such as CVH, is limited in the United States.
Purpose of The Study
While much of the existing literature focuses on the direct relationship between CVH and physical and mental health risks and outcomes, less consideration has been given to broader aspects of holistic well-being. To fill this gap, using Keyes’ theoretical concepts of flourishing, a latent construct, that combines hedonic/emotional well-being with eudaimonic/functional dimensions of psychological and social well-being (Huppert & So, 2013), we used a large longitudinal sample of US adults to understand whether ideal (i.e., high) CVH, assessed by LE8, is linked with flourishing, a measure for holistic well-being, and whether better LE8 is associated to individuals’ sense of well-being across adulthood. To our knowledge, the current study is unique in its nature, examining whether ideal CVH is associated with better flourishing, assessed as a measure of holistic well-being over 10 years. We also examined whether long-term rural living across waves 1–2 or intermittent rural living moderates the CVH-flourishing association, compared to no rural living, while controlling for well-documented correlates of behavioral attributes, including sociodemographic and health factors. We hypothesized that i) ideal CVH would predict better flourishing scores and ii) long-term rurality would moderate the association between CVH and flourishing.
Methods
Study Design
We used data from the Midlife in the United States (MIDUS) survey, a nationwide longitudinal study spanning 20 years. MIDUS survey was initiated in 1995 to 1996 (wave 1), with 7,108 middle-aged and older adult English-speaking participants (Mean [M] age = 46±13) across the US (Bhattacharyya, Dobbs, et al., 2022; Yuan et al., 2024). MIDUS wave 2 survey was conducted in 2004-05, and wave 3 in 2013-14; all waves were conducted over the phone and mailed self-administered questionnaires (SAQ; Yuan et al., 2024). In this study, we examined participants enrolled in all three waves (1995–2015) with no missing observations (N = 2,536), which allowed us to control for unobserved individual effects, eliminate time-invariant factors, and achieve higher statistical efficiency. We merged data from the main SAQ and biomarker projects. We did not seek IRB approval for this study because our analyses are based on a publicly available dataset through the Inter-University Consortium for Political and Social Research (ICPSR; Bhattacharyya et al., 2024).
Measures and Procedure
Dependent Variables
Flourishing
As dependent variables, we used holistic well-being, which was measured by a composite flourishing score that included emotional, psychological, and social well-being, based on Keyes’ conception (Keyes, 2002; see Supplemental Table 1). We assessed flourishing at wave 3.
Emotional Well-Being
Two aspects of emotional well-being were assessed, including life satisfaction and positive affect (Keyes & Simoes, 2012). The life satisfaction score was measured using a 5-item SAQ; for each item, MIDUS asked participants to rate their life based on overall, work, health, relationship with spouse/partner, and relationship with children (Prenda & Lachman, 2001). Responses were coded on a scale from 0 (the worst possible) to 10 (the best possible). First, MIDUS averaged the scores for the relationship with spouse/partner and the relationship with children to create one item. Then, this score was used along with the remaining three items (life overall, work, health) to calculate an overall (average) mean score, with higher scores reflecting better overall life satisfaction. Next, MIDUS computed the score for cases that have valid values for at least one item on the scale (score range 1–10). The score for life satisfaction was not calculated for cases with no valid item and was identified as missing data. We considered the average (mean) score provided in MIDUS for the entire range of responses on life satisfaction. A 6-item validated positive affect scale (Mroczek & Kolarz, 1998) was used to measure the extent to which participants felt cheerful, in good spirits, happy, calm and peaceful, satisfied, and full of life over the past 30 days. Responses were coded from 1 (all the time) to 5 (none of the time). Responses were reverse coded so that a higher score indicated greater positive feelings. An overall score of positive affect (range: 1–5) was derived by averaging responses across the items. For the current analysis, because life satisfaction and positive affect were assessed on different scales, the scores were standardized separately (M = 0, standard deviation [SD] = 1) and then summed to create an overall score for emotional well-being (α = .71).
Psychological Well-Being
We measured psychological well-being using Ryff’s Psychological Well-Being Scale (Ryff, 1989), which assesses six subdomains (each with three items). These consisted of autonomy (e.g., “I tend to be influenced by people with strong opinions”), environmental mastery (e.g., “The demands of everyday life often get me down”), personal growth (e.g., “I gave up trying to make big improvements or changes in my life a long time ago”), positive relations with others (e.g., “I have not experienced many warm and trusting relationships with others”), purpose in life (e.g., “Some people wander aimlessly through life, but I am not one of them,” R), and self-acceptance (e.g., “When I look at the story of my life, I am pleased with how things have turned out,” R). Responses were coded, ranging from 1 (strongly agree) to 7 (strongly disagree). Responses were reverse coded as necessary (items marked with “R”), reflecting a higher score for greater well-being. A score for each subdomain was calculated by summing the responses for the respective three items under that subdomain. An overall score for psychological well-being was created by summing the responses across all six subdomains (α = .79).
Social Well-Being
We used a 14-item scale, as suggested by Keyes and Shapiro (2004), to measure 5 subdomains of social well-being (3 items for each subdomain except for the 2-item social coherence). The scale consisted of social coherence (e.g., “I cannot make sense of what’s going on in the world”), social integration (e.g., “My community is a source of comfort,” R), acceptance of others (e.g., “I believe that people are kind,” R), social contribution (e.g., “I have nothing important to contribute to society”), and social actualization (e.g., “Society has stopped making progress”). Responses were coded, ranging from 1 (strongly agree) to 7 (strongly disagree). Responses were reverse coded as necessary (items marked with “R”), reflecting higher scores for greater well-being. Each subdomain’s score was created by adding responses for items relevant to that subdomain. Because not all subdomains were measured on the same scale (for example, social coherence was assessed with 2 items instead of 3 items for the others), each subdomain’s score was standardized separately and then summed to create an overall score of social well-being (α = .74).
Because each domain’s scores were measured on different scales, we standardized emotional, psychological, and social well-being scores and then summed them to create a composite flourishing score (Chen et al., 2019). We used the continuous measure of flourishing to assess holistic well-being.
Key Independent Variable
We used individuals’ CVH status in wave 2 as the key independent variable. Participants’ CVH status was categorized based on the parameters of LE8, as defined by the American Heart Association (AHA; Lloyd-Jones et al., 2022), which include diet, physical activity, nicotine exposure, sleep health, body mass index, blood lipids, blood glucose, and blood pressure. For each indicator, scores were either coded as 1 (if participants met the ideal AHA criterion) or 0 (otherwise). A composite CVH score was created by summing the parameters assessed that ranged from 0 (i.e., meeting no ideal CVH metric) to 8 (i.e., meeting all ideal cardiovascular health metrics); further, CVH was categorized as low (0–4 metrics at ideal levels) and high (5–8) to stratify the sample by CVH status. In the current regression analyses, we used the continuous composite CVH score.
Briefly, regarding the percentile score for diet, the 2015 Healthy Eating Index score was assessed from self-reported food frequency questionnaires from the National Health and Nutrition Examination Survey. Physical activity and sleep health were assessed through self-reported minutes of moderate or vigorous activity per week and the average number of hours of sleep per night, respectively. Blood pressure and body mass index were measured during clinic visits. Given the constraints of the WHI data, nicotine exposure scoring was calculated from the original AHA scoring. Nicotine exposure was measured based on self-report questionnaires and categorized as never, previous, or current smoker in a prior study. Blood lipids (non-HDL cholesterol) and blood glucose were measured from WHI data samples. For participants who self-reported taking lipid-lowering medications on the questionnaire data, the blood lipid score was reduced by 20 points. Finally, as glycosylated hemoglobin was unavailable in many participants’ WHI data, the blood glucose score was measured using data on fasting blood glucose and treatment for diabetes. LE8 measures are described in Supplemental Table 2.
Moderator Variable
We used waves 1 and 2 living contexts (rural vs. urban) as the moderator variable to assess its long-term effect on flourishing. We applied the Beale Rural-Urban Continuum Codes (RUCC), as described by the United States Office of Management and Budget (OMB), to define rurality. The Beale RUCC categorizes counties or county-equivalent units (e.g., parishes, boroughs) as rural/urban based on a) population count and b) whether the location is adjacent to a metropolitan area (United States Department of Agriculture [USDA] Economic Research Service, 2019). The RUCC classification is used to denote participants’ living contexts, whether they reside in rural or urban areas, by identifying the location in the respective county as urban, suburban, or rural based on its population and adjacency to a metro area. The categorization scored from 0–9 in 1993 and 1–9 in 2003, representing “0 or 1 = county in metro area of 1 million population or more” to “9 = nonmetro county completely rural or less than 2500 urban population, not adjacent to metro area” (Atherton et al., 2024). Next, the addresses were merged with a time-varying RUCC dataset to harmonize MIDUS waves 1–3 data with RUCC codes in 1993, 2003, and 2013, respectively. In the current study, we recoded the 0/1–9 RUCC categories into two groups, denoting ‘0’=RUCCs 0/1–6 (urban/suburban) and ‘1’=RUCCs 7–9 (rural). Finally, we measured long-term rurality, by further constructing the outcome as a four-level living context variable using rural living status across waves 1 and 2: no rural living either at wave 1 or 2 (reference) coded with a [0], rural living at wave 1 only [=1], rural living at wave 2 only [=2], and long-term rural living at waves 1 and 2 [=3].
Covariates
We used sociodemographic factors, health, and functional status (at wave 1) as covariates. Sociodemographic variables included age, gender, race, marital status, education, and employment. Age (0 = <65, 1 = ≥65) and gender (0 = male, 1 = female) were measured as binary variables, and race (1 = White, 2 = Black, 3 = other) was measured in three categories; in contrast, marital status (1 = married, 2 = separated/divorced, 3 = widowed, 4 = never married) and educational level (1 = no/some school, 2 = high school graduate/in college, 3 = graduated from college, 4 = having master’s/professional degree) were measured in four categories. Employment status was measured in two categories (1 = currently working, 2 = currently not working).
Several variables indicated health and functional status. First, participants were asked, using a functional status questionnaire, whether they had difficulty (i.e., functional limitations) in activities of daily living (ADLs) and instrumental activities of daily living (IADLs). We computed the sum using responses in MIDUS on functional limitations (range: from “a lot” to “no difficulty”) with higher values indicating greater difficulties. We also included additional variables related to health, including tobacco and alcohol use (1 = regular tobacco/alcohol user, or 0 = not) and chronic condition/s (1 = yes, 0 = no). Chronic conditions included high blood pressure, stroke, heart problems, high cholesterol, diabetes, cancer, lung problems, ulcers, and aches/joint stiffness in the past 12 months. Further, we considered the past 12 months’ medication usage (sum of five indicators: tranquilizers, sedatives, stimulants, painkillers, and anti-depression medications). Finally, because personality traits have been well-documented as significant correlates of well-being across adulthood (Abdullahi et al., 2020), we also considered these variables as potential confounders in our analysis. We included the big five personality traits, including agreeableness, conscientiousness, extraversion, openness, and neuroticism (Zimprich et al., 2012), as MIDUS measured participants’ responses on a 4-point Likert scale (1 = “a lot” to 4 = “not at all”) and averaged for each trait. This study adjusted for the prior level of flourishing assessed in wave 1 as a covariate to reduce potential reverse causation.
Statistical Analysis
Statistical analyses were conducted with Stata 18.5 SE (College Station, TX) software. Preliminary analyses examined participants’ demographics, health, and functional status in the total sample and in the sample stratified by having an ideal versus lower CVH at baseline (wave 2); we used multiple imputations to address missing data. We then conducted multiple linear regression analyses to examine whether ideal CVH (wave 2) predicts flourishing (assessed in wave 3) over 10 years, using the composite scores of flourishing and its three domains (emotional, psychological, and social well-being) in separate models. Further, we examined whether participants’ long-term rural living (at waves 1 and 2) or rural living at only one time point (either at wave 1 or 2) moderate the CVH-flourishing association, compared to no rural living while controlling for prior flourishing score and covariates (socio-demographics, health, and functional status) assessed at wave 1; we used wave 1 variables as control as a robust approach for establishing causality. Statistical significance was evaluated at p < .05 (two-sided). Unstandardized regression coefficients (b) and standard errors (SE) are reported. We also adjusted the standard errors for repeated observations over time with non-parametric bootstrapping.
Results
Table 1 shows the descriptive statistics of different variables, including participants’ sociodemographic characteristics and health status at wave 2 for the total sample and the sample stratified by CVH status, i.e., ideal versus lower. A total of 2,536 individuals (who participated in all three waves of MIDUS) aged 33 to 83 years (Mage = 55±11) in wave 2 (i.e., aged 42–92 years in wave 3) were included in the analysis. Women made up 55% of the sample, 55% were employed, and 93% were White. Substantial proportions of participants were alcohol users (62%); 16% of the sample had difficulty in performing activities of daily living. The findings revealed that only 12.5% of participants had high CVH status. Table 1 also reports participants’ rural living status and flourishing scores. Ninety-one percent of participants consistently (in waves 1 and 2) lived in urban/suburban areas, while 6% persistently lived in rural areas. The mean score of participants’ composite flourishing was 0.03±8.7 at wave 2.
Comparison of participant characteristics of US adults in MIDUS wave 2 (n = 2,536).
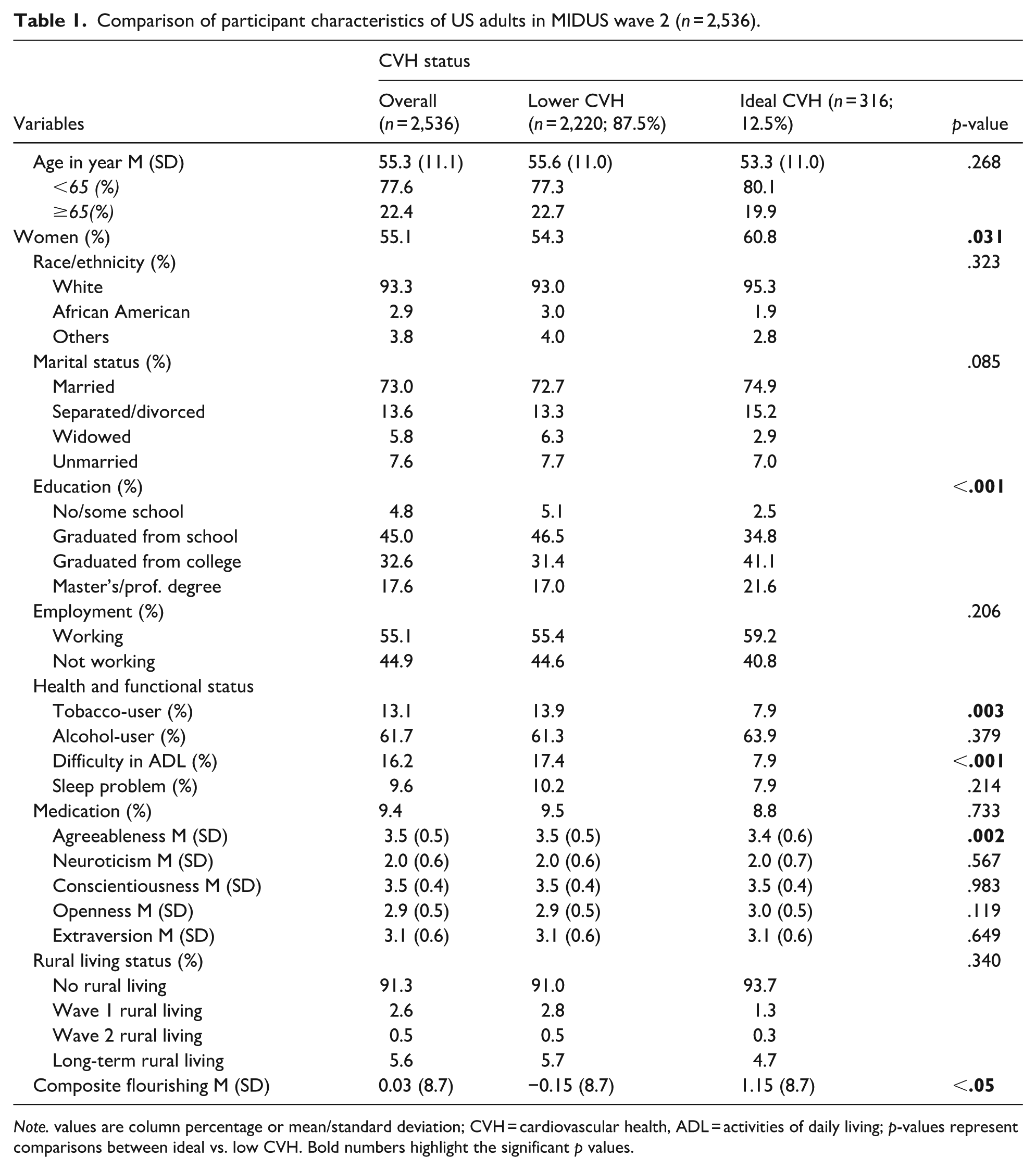
Note. values are column percentage or mean/standard deviation; CVH = cardiovascular health, ADL = activities of daily living; p-values represent comparisons between ideal vs. low CVH. Bold numbers highlight the significant p values.
Table 2 shows the results of multiple linear regression models estimating the effect of CVH at wave 2 on wave 3 composite flourishing score and each flourishing domain after controlling for covariates. Ideal cardiovascular health at wave 2 was positively associated with composite flourishing at wave 3 (b = 0.332; SE = 0.150; p < .05). Regarding each of the flourishing domains, although ideal CVH was not found to be associated with emotional well-being (b = 0.020; SE = 0.021; p = .325), it was positively associated with psychological well-being (b = 0.194; SE = 0.087; p < .05) and social well-being (b = 0.129; SE = 0.066; p < .05) over time. However, rural/urban living status does not moderate the association between CVH (wave 2) and flourishing (composite and each domain in wave 3) in mid and later life. Among covariates, individuals who were once married and those with the highest level of education showed a significant positive effect on composite flourishing, whereas older age had a significant negative effect on composite flourishing. Furthermore, conscientiousness and extraversion exhibited significant positive effects on flourishing, whereas neuroticism showed the opposite.
Multiple linear regression models examining moderating roles of rural living status (waves 1 and 2) in the association between cardiovascular health (wave 2) and flourishing (wave 3) in mid and later life over 20 years, controlling for covariates (n = 2,536).

Note. ICVH = Ideal cardiovascular health; W1 = wave 1; W2 = wave 2; W3 = wave 3. Bold numbers highlight the significant p values.
Discussion
The current study makes a unique contribution to the existing literature with population-based, longitudinal evidence that individuals’ CVH status is positively associated with their later life flourishing. This suggests that individuals with better CVH tend to experience higher levels of holistic well-being, supporting our first hypothesis. The multidimensional perspective of individuals’ CVH, as assessed by LE8, addresses various aspects of well-being as guided by Keyes’ theoretical concepts of flourishing. However, despite rural-living US adults having lower socioeconomic status compared to their urban-living counterparts, and possible underlying causes are the availability of lower educational and healthcare resources (Saenz et al., 2018), differences in rural-urban living status do not affect the direction of the relationship between CVH and well-being and, thus, disprove our second hypothesis. Individuals’ well-being cannot be explained solely by sociodemographic and health factors that often coexist in rural contexts; instead, certain psychological factors may also play a role in these associations (Nganje & Addey, 2019; Saenz et al., 2018). Moreover, due to similar underlying biobehavioral and psychosocial factors, rural-urban disparities impact levels of CVH and well-being status but not their association (Cohen et al., 2023).
Earlier research addresses the relationship between psychological well-being and CVH (Kubzansky et al., 2018). It is generally accepted that psychological well-being and CVH have bidirectional associations (Boehm et al., 2017). In this study, we tested the directionality of the association, specifically whether CVH acts as a prospective predictor of well-being, to emphasize that a positive attitude toward CVH highlights the importance of overall well-being. To our knowledge, while no prior studies have explored the longitudinal relationship between CVH, assessed by LE8, and flourishing, the findings have generally been consistent with previous related research on quality of life. Studies have demonstrated a strong and positive relationship between LE8 metrics and mental, cognitive, and physical quality of life (Liang & Zhang, 2024). Similarly, many studies exploring the relationship between LE8 and chronic disease outcomes have consistently found higher LE8 scores to increase the likelihood of alleviating the risk factors contributing to chronic diseases (Hao et al., 2025; Ren et al., 2023), leading to higher well-being because chronic diseases disrupt individuals’ lives that may be interpreted to affect their well-being (Megari, 2013).
Previous studies exploring the relationship between CVH and psychological well-being have found that positive psychological well-being (e.g., a sense of purpose, optimism, and life satisfaction) is independently associated with a healthier profile of CVH and a reduced risk of cardiovascular disease (Kubzansky et al., 2018). Further, many studies were found to have an inverse relationship between CVH and mental health outcomes, such as depression and anxiety. For example, using the Health and Nutrition Examination Surveys (NHANES) data, one study showed that people with low CVH status were 5.5 times more likely to have depression compared to people with high CVH; this study strongly suggested the dose-response relationship between the CVH and depression (Chen et al., 2023). Contextually, several studies have shown a strong relationship between each component of CVH, like physical activity, sleep, and a healthy diet. For example, in a longitudinal observational twin study survey examining genetic variability, twins who exercised regularly reported fewer anxious and depressive symptoms compared to those who did not exercise (De Moor et al., 2008). Exercise also has effects like antidepressants in reducing depression symptoms (Blumenthal et al., 2007). Moreover, depression can be caused by inadequate sleep, which can further be influenced by depression (Yasugaki et al., 2025). Further, old age is a predictor of inadequate sleep, which may aggravate depressive symptoms. Our finding that higher age is associated with lower well-being is relevant in this context.
These results align with the growing body of evidence suggesting that CVH or lifestyle measures play a significant role in mental health. Contextually, Sabia et al. (2019) found a negative correlation between cardiovascular scores (assessed using Life’s Simple 7, i.e., all LE8 components excluding sleep) and the likelihood of developing dementia, with higher CVH scores associated with a lower risk of dementia. More recently, another study using NHANES data found a positive association between LE8 and cognitive function in older adults (Liang & Zhang, 2024). Our finding adds to the existing literature.
Our findings corroborate earlier research showing that people with compromised CVH face severe financial and mental hardship (Teshale et al., 2023), leading to poor life satisfaction and quality of life (Lloyd-Jones et al., 2022). The findings of this study indicate that only 12.5% of individuals in Wave 2 (2003–2004) achieved the highest CVH status, as measured by LE8. This highlights the rarity of optimal CVH in older adults, possibly due to a lack of awareness. Furthermore, individuals with higher socioeconomic status living in urban environments may experience less stress and greater well-being; they also tend to exhibit a more positive attitude towards achieving things in their favor (Bhattacharyya & Molinari, 2024). In this context, the negative effects of stress on well-being are well-documented (Purchase et al., 2024). Although we did not measure any factors related to the stress process, the findings suggest that further insight into the mechanism by which this association occurs may be important.
Limitations
A large sample size and national representativeness are the main strengths of the current study; however, multiple limitations are also noted. First, MIDUS did not screen participants for baseline cognitive status, which makes it hard to comment on the neurocognitive status of the included participants. Further, the analytic sample comprises only participants who completed all three waves of MIDUS, which introduces potential bias due to non-random attrition. Socioeconomic status and health, including cardiovascular-related mortality, are likely to influence study retention. Although we control for sociodemographic and health factors in the analysis, other factors, such as cultural background and immigration status, may also influence the outcomes. White predominancy in the study population may also raise a generalizability concern. Further, collapsing RUCC codes into a binary rural versus urban geographical variation could weaken the impact. Future research with a finer classification may provide different outcomes. Next, individuals categorized as having ideal CVH appear to include tobacco users. Since nicotine exposure is one of the key components used to define CVH, this inconsistency may be due to the amount of nicotine exposure or a compound effect of other CVH parameters. Additionally, although HbA1c data were available for many participants, they are missing in many others, and MIDUS substituted fasting glucose, which raises concerns about generalizability. Finally, the data are rather old, and the difference in socioeconomic status, especially from the rural/urban context, between the survey time and today may lead to a generalizability bias.
Conclusion
Despite the above limitations, the current findings have important theoretical implications, as they explore the positive impact of good CVH on well-being. However, our findings suggest that one macro-level factor, namely the rural or urban living context, has no directional impact on the association between CVH and well-being over time. While rural living is often considered a low socioeconomic condition in late adulthood, our findings are not consistent with those in mid and later life over 10 years, providing a unique contribution to the existing literature. Future research should examine the mechanisms by which other socioeconomic and cultural factors influence the association between CVH and well-being across adulthood.
Supplemental Material
sj-docx-1-ggm-10.1177_30495334251389181 – Supplemental material for Does Cardiovascular Health Influence the Well-Being of People Living in Rural Areas: Findings From a 20-Year Study in US Adults
Supplemental material, sj-docx-1-ggm-10.1177_30495334251389181 for Does Cardiovascular Health Influence the Well-Being of People Living in Rural Areas: Findings From a 20-Year Study in US Adults by Kallol Kumar Bhattacharyya, Sharmila Acharya and Mark Hendricks in Sage Open Aging
Footnotes
Acknowledgements
None.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.