
Abstract
Ageism may have harmful effects on the psychological well-being of older adults, leading to mental health issues, such as depression and anxiety. However, there are insufficient data to establish this hypothesis, and most work on the subject has appeared only in the form of conceptual or theoretical papers. This study reviewed quantitative studies of the relationship between ageism and psychological well-being of older adults. We conducted a comprehensive review using searches of academic databases, the grey literature, hand searches, and reference mining. A total of thirteen articles were selected using the inclusion criteria. All the reviewed studies showed a negative association between ageism and the psychological well-being of older adults. The study confirmed a negative association between ageism and older adults’ psychological well-being, finding that older adults with a high level of psychological well-being may be less negatively affected by ageism, especially those who were proud of their age group, experienced less negative emotions, were more optimistic about aging and their future, were more self-confident about their bodies, and were flexible in setting goals. The identified mediators of the association can inform intervention development to the effects of ageism and improve older adults’ psychological well-being.
Introduction
Growing older involves gaining maturity and becoming a more responsible and respectful adult. The process of aging can be viewed unfavorably by some people, who view it pessimistically, and this reduces the pleasure they may have gained from their own growth (Kang, 2020). Aging is often considered to be a challenging process, during which individuals lose their confidence and experience a loss of productivity (Schafer & Shippee, 2009). Significant declines in social and cultural status have been observed in older adults over the past century as a result of industrialization and modernization (Aboderin, 2004; Nelson, 2005). The industrial age and technological advancements have increased the need for people to work efficiently and quickly to remain competitive (Tuomi et al., 1997). These changes have had the effect of decreasing the need for and visibility of older adults’ activities (Solem, 2005).
A growing body of research has observed an increase in negative attitudes toward older individuals over the years (Nelson, 2005; Scharlach et al., 2000). Several studies have shown that members of the younger generations now exhibit more negative views and attitudes toward older adults than was previously the case (North & Fiske, 2012). Negative beliefs and attitudes towards older adults are increasingly prevalent, which may add to the barriers that older adults face when seeking employment (Skirbekk, 2004). Consequently, older adults are often considered to be merely passive recipients of welfare, and they may even be accused of being a burden to younger generations (Hudson, 2012). The belief that older adults are less valuable or of no interest to society may contribute to ageism.
Ageism is stereotyping, prejudice, and discriminatory actions or attitudes based on chronological age (Iversen et al., 2009). Ageism, therefore, can be operationalized as stereotypes, prejudices, and discrimination, and each of those components, individually, can be seen as cognitive, affective, and behavioral (Iversen et al., 2009). Consequently, age stereotypes are fixed beliefs that overgeneralize the characteristics, attributes, and behaviors held in common by a particular group (Whitley & Kite, 2006). Age stereotypes can contribute to assumptions about a person’s physical and mental capabilities, social skills, political and religious beliefs, and other traits based on their age (World Health Organization, 2021). A prejudice is a negative or positive emotional reaction to a person based on their perceived affiliation with a particular group (World Health Organization, 2021). Age prejudice is one of the most socially vocalized and institutionalized prejudices in many segments of society, and it is disregarded in numerous aspects of social life (Nelson, 2005). A discriminatory act is characterized primarily by distorted behavior that treats individuals in a non-constructive manner (Dovidio et al., 2011). Age discrimination is behavior directed at people based on their age, including actions, practices, and policies (World Health Organization, 2021).
Ageism is a very serious issue. While it can theoretically be directed toward any age group, the vast majority of studies focus on older adults or late adolescents (Nelson, 2005). Although ageism can be shown in terms of positive stereotypes or attitudes, it is most closely associated with negative stereotypes or attitudes (Palmore, 1999). Ageism can manifest in two main ways: implicitly, through unconscious thoughts, feelings, and behaviors, or explicitly, through intentional actions or verbal expressions triggered by conscious awareness (Iversen et al., 2009). Furthermore, ageism is not restricted to directed toward others but can also be self-directed (Ayalon & Tesch-römer, 2017). Exposure to ageism over time can result in the internalization of ageist attitudes and stereotypes, as described by Levy (2009) in stereotype embodiment theory. Many older adults tend to internalize the negative stereotypes of ageism that continue to be perpetuated throughout society today and tend to confine themselves to age-related stereotypes, becoming weak, unhealthy, and even less able to accept new learning opportunities (Streb et al., 2008).
Internalized age stereotypes may lead to low levels of self-esteem and self-confidence (Orth et al., 2010), and it may affect older adults’ health negatively (Emile et al., 2014), especially with regard to their mental health and well-being (Bryant et al., 2012). An individual who believes that they are too old may be more susceptible to the negative consequences of ageism, which may include decreased self-efficacy and increased negative emotions (Eibach et al., 2010). The converse may also be true, as positive perceptions and attitudes on aging may have beneficial effects on psychological well-being (Bryant et al., 2012). Older adults who have experienced discrimination based upon their chronological age may be more exposed to stressors (Snape & Redman, 2003) and depression (Tougas et al., 2004), which are detrimental to their mental health (Pascoe & Richman, 2009).
Ageism is increasingly recognized as a risk factor associated with increased stress, anxiety, depression, and lowered life satisfaction (Ayalon et al., 2019). However, articles on ageism generally take the form of conceptual or theoretical papers, and they tend to center on identifying the causes and consequences of ageism (Iversen et al., 2009). More empirical studies are needed to investigate the harm that ageism can cause to the psychological well-being of older adults. Our review examined this relationship by synthesizing the results of several studies identified in a thorough systematic search.
Purpose of the Review
This systematic review examines how the experience of ageism experience among older adults influences their psychological well-being. This study also seeks insight into successful aging by identifying factors that mediate or moderate the relationship of ageism to psychological well-being. Our overarching goal is to mitigate or eliminate the adverse effects of ageism, especially on the psychological well-being of older adults. Using a systematic review method allows the researcher to comprehensively identify relevant literature through transparent and rigorous processes (Littell et al., 2008). Several systematic reviews have examined ageism and its effects on older adults: these include assessments of how stereotypes of aging affect memory and cognitive performance (Lamont et al., 2015), ageism’s broad effects, and theories that explain ageism (North & Fiske, 2012). However, no research has hitherto examined the direct effects of ageism on older adults’ psychological well-being.
A new paradigm for understanding the aging society is necessary in the face of a rapidly expanding population of older adults to assess these developments in a long-term perspective. The study of ageism can be a key foundational resource for older adults. Unbiased summaries of quantitative outcome studies from our systematic review may help to develop an understanding of the potential risks of ageism on psychological well-being. Furthermore, the mediators and moderators identified between ageism and the psychological well-being of older adults will support future policy and practices.
Methods
We aimed to locate all empirical evidence that examined the relationship between ageism and older adults’ psychological well-being through a comprehensive and unbiased search. The systematic review methodology was guided by two sources: Systematic Reviews from the Centre for Reviews and Dissemination (2009) and Systematic Reviews and Meta-Analysis from Littell et al. (2008). We also followed the guidelines from a review protocol, the PRISMA 2020 statement (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) developed by Page et al. (2021), to verify the validity of the steps involved in the systematic review. PRISMA is a set of standards that includes a 27-item checklist and a four-phase flow diagram describing how systematic reviews should be reported (Page et al., 2021). The completed PRISMA checklist was included in Appendix B. A critical appraisal checklist for analytical cross-sectional studies developed by the Joanna Briggs Institute (JBI) was used to assess the methodological quality of the reviewed studies (Moola et al., 2020). Additionally, we reported our results using Pleasant et al.'s (2020) study as a guide (Pleasant et al., 2020). Our first step was to develop a search strategy to guide a thorough but rigorous systematic search by refining our research question. We also articulated and tested our complete set of search terms to decrease our chances of missing relevant literature. A number of inclusion and exclusion criteria were set to prevent bias in the selection process. We used a wide range of sources for our review, including several electronic databases, grey literature, hand searches, and reference mining.
Criteria for Considering Studies for the Review
PICOS Framework for Systematic Review.

The review included studies that measured ageism or attitudes towards older adults. Ageism can be direct or indirect, and it tends to be reproduced and unconsciously reflected in social or cultural spheres (Iversen et al., 2009). While ageism toward older adults might also be demonstrated in a positive stereotype or attitudes toward them (Palmore, 1999), ageism in this study was confined to only negative attitudes and feelings. Furthermore, we included studies on self-directed ageism, which refers to ageism directed at oneself, in order to examine how internalized age stereotypes affect older adults’ psychological well-being. The large number of words associated with ageism prompted us to choose broad and general search terms in order to avoid the omission of relevant articles and to identify all potentially relevant studies.
In this study, the psychological well-being of older adults was the outcome of interest. Psychological well-being is a multi-dimensional concept determined by multiple components and factors (Kim et al., 2017). We adopted a broader definition of psychological well-being as suggested by Diener et al. (2017). They conceptualized psychological well-being as an all-inclusive term that includes desirable psychological characteristics as well as subjective well-being; that is, the subjective perception of life that an individual experiences in their environment (Baker et al., 2005). Psychological well-being is a key indicator for measuring the subjective aspects of quality of life (Baker et al., 2005). Further, it is an integrative construct that includes diverse affective and cognitive dimensions, such as life satisfaction, positive/negative affect, mental health, self-actualization, optimal functioning, happiness, and mood (Levin & Chatters, 1998; Ryff, 1989). Depression, life satisfaction, stress, and other mental health behaviors were also considered in measuring psychological well-being. Study designs were limited to empirical quantitative studies that used statistical, rather than descriptive, analysis to present findings. Studies that met this population, predictor, outcome, and type of study criteria were eligible for review consideration.
To summarize, ageism literature was systematically reviewed using the following criteria: (a) focused solely on ageism without any other forms of discrimination; (b) measured ageism against older adults (60 years old and above); (c) examined the relationship between ageism and psychological well-being; (d) was written in English; and (e) used a quantitative design. Studies were excluded that (a) identified other sources of discrimination such as disability, race, sexuality, HIV, LGBTQ (lesbian, gay, bisexual, transgender, and questioning), and mental illness; (b) examined the relationship between ageism and physical health without psychological well-being; (c) used ageism as an outcome variable; and (d) used a literature review and qualitative design as the research method.
Search Strategy
To identify and determine all published research studies on ageism focusing on the influence on older adults’ psychological well-being, we conducted a comprehensive search to identify all potentially relevant literature from the inception of each index to August 31, 2019, both published and unpublished. We searched relevant resources regardless of the country of origin but only included resources written in English. In order to find all potential studies, we established four search strategies: database searches, grey literature searches, hand searches of selected journals, and reference mining. We used three bibliographic databases: ProQuest Research Library, Web of Science, and Academic Search Complete for our literature search. The search included all literature from the earliest years that the databases cover to August 31, 2019. The set of search terms included Ageism (or ageist), older adults (or aged or the elderly), and psychological (or emotional) well-being (or health or satisfaction). Various combinations of terms were tested to identify all potentially relevant studies, and our final search terms used for each database were provided in Appendix A.
To find possible unpublished literature on our topic, we visited websites of state/national government agencies, research centers, and both profit/nonprofit organizations that were most relevant to our topic and selection criteria. The grey literature sites included Cochrane Library, ProQuest Dissertations & Theses, American Psychological Association (APA), American Society on Aging (ASA), National Center on Elder Abuse (NCEA), National Committee for the Prevention of Elder Abuse (NCPEA), and The Fiske Lab. A general web search located additional studies through google and google scholar.
Four journals that were highly relevant to the search criteria were selected for a hand search to supplement unidentified literature that might have been missed through an electronic search: Ageing and Society (1981–present), Aging and Mental Health (1997–present), Gerontologist (1961–present), and Psychology and Aging (1986–present). We searched the entire contents of the four journals to find potentially eligible studies. Backward reviews through a reverse bibliographic search were also included for the hand search. Furthermore, we scanned the relevant references from articles identified through previous search methods to identify additional literature that met the search criteria.
Data Collection and Analysis Methods
We used EndNote X9, a reference managing computer program, for data collection processes, including downloading results of electronic searches, organizing downloaded references, checking duplication, and locating full texts. The data collection process started by first retrieving abstracts or titles for all resources through the search process. The second screening process involved reviewing full texts of the initially screened resources to determine if the sources were relevant by applying exclusion and inclusion criteria. For reliability of quality assessment and data extraction, all screening processes were undertaken by both the first author and the second author. Disagreements about screening and full-text retrieval decisions were discussed until reaching a consensus.
After the full-text review, final resources were selected for data extraction. The first author collected data from the final resources, and the second author checked and revised the data extraction by the first author and supplemented insufficient data, if needed. Disagreements among the two authors were again resolved by consensus to establish inter-rater reliability in the data extraction process. The data collection included (a) Study design: overarching goal, study site and control variables, (b) Methodology: type of data, data collection methods and statistical techniques, (c) Sample: random sampling, sample size, and sample characteristics (age, education level, race/ethnicity, (d) Predictor (ageism): data source, measures, tools used, information regarding the validity of tools, (e) Outcome (psychological well-being): data source, list of outcomes assessed, measures, tools used, information regarding the validity of tools, (f) Findings: the relationship between ageism and psychological well-being (statistically significant associated or not associated), and (g) Intervention: interventions between ageism and psychological well-being (statistically significant associated or not associated). Finally, to establish the study quality standards, information regarding (a) Internal validity (missing data and reliability and/or validity of variables) and (b) External validity (representative of the population) were extracted
Results
Figure 1 illustrates the search process. The database search identified 6103 records, while additional 314 records were identified from other sources. 673 duplicates were removed from the initial sample (n = 6417). A screening of the remaining records’ titles and abstracts (n = 5744) was conducted to ascertain eligibility criteria, which led to the exclusion of (n = 5447) records. All of the remaining articles (n = 297) were evaluated by full-text review, and 284 articles were excluded for the reasons outlined in Figure 1. Thirteen articles were ultimately selected for data extraction. Systematic review flow diagram.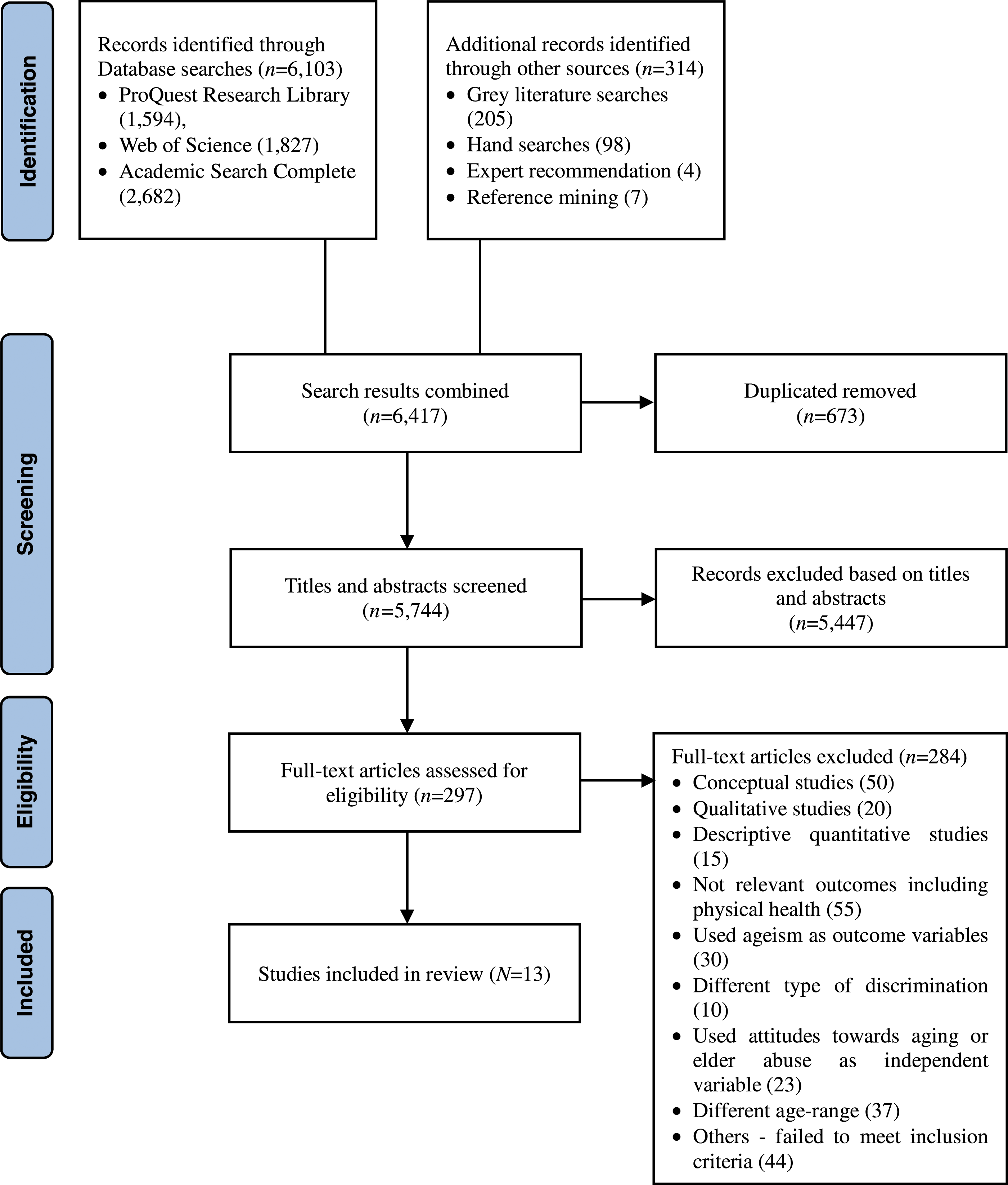
Studies’ Design and Setting
Study Design and Setting.
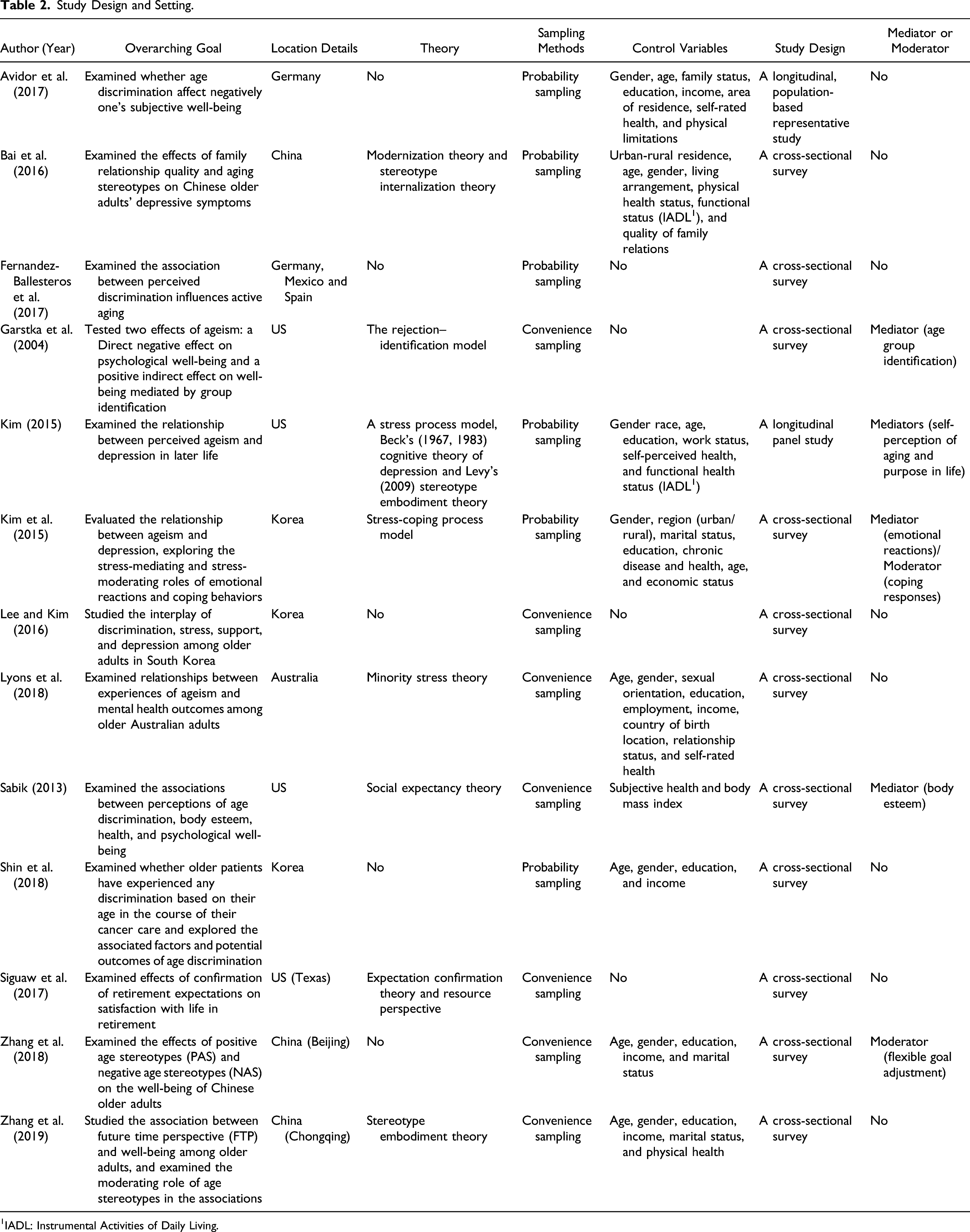
1IADL: Instrumental Activities of Daily Living.
38% (n = 5/13) were conducted in the US and 46% (n = 6/13) in Asia. There was one study conducted in Europe, and the other in Germany, Mexico, and Spain. 38% (n = 5/13) conducted a secondary analysis of existing data, and the samples in these studies were selected through a probability sample design. 15% (n = 2/13) were longitudinal panel research, whereas all the other studies were cross-sectional design. Except for one PhD dissertation (Kim, 2015), all other studies (92%) were published in peer-reviewed journals and were published between 2004 and 2019.
Studies’ Participants
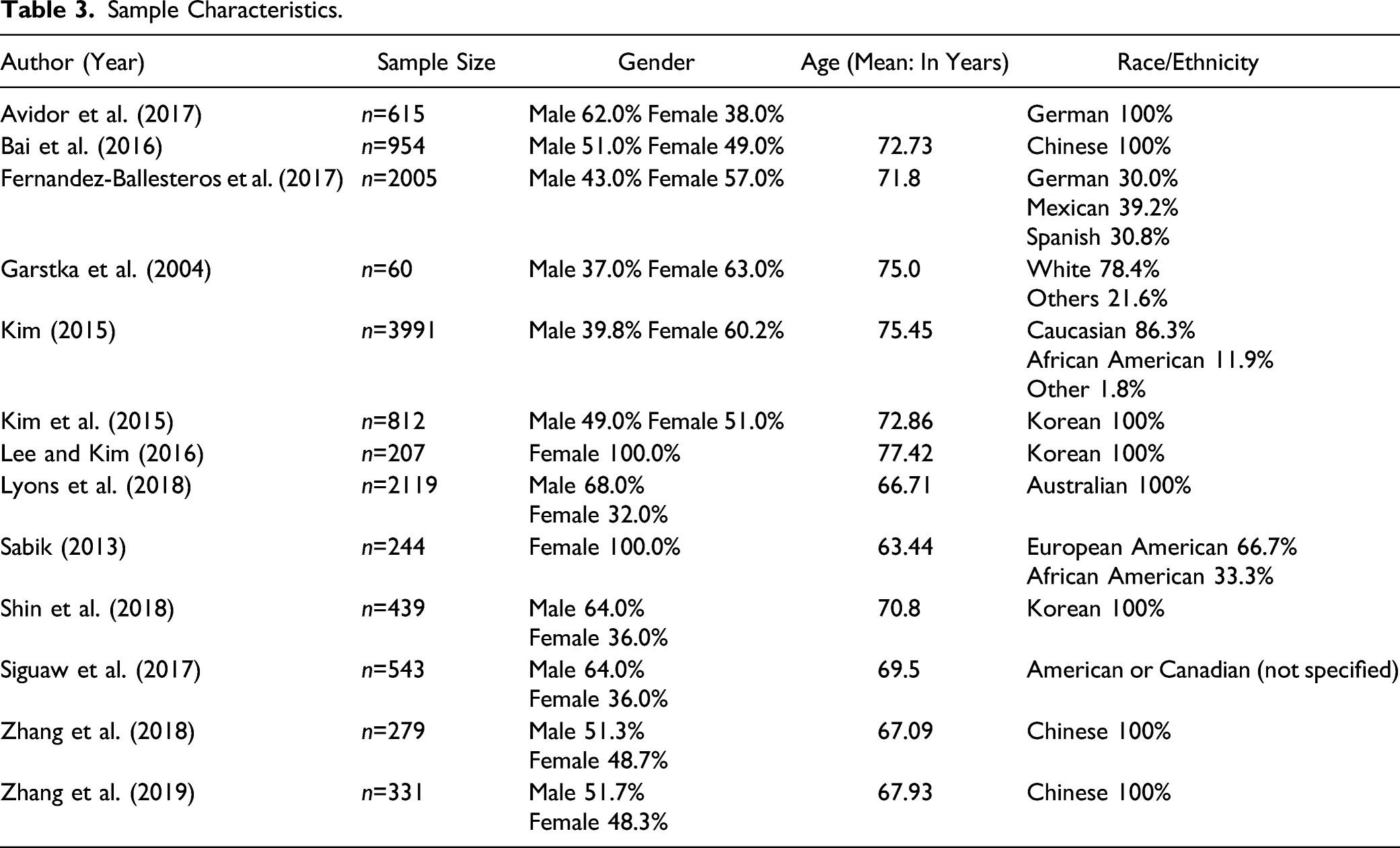
Sample Characteristics.
Measurement
Ageism
38% (n = 5/13) used established scales that have been used and evaluated. Three studies used Palmore’s (1999, 2001) ageism scale (Kim et al., 2015; Lee & Kim, 2016; Lyons et al., 2018). Zhang et al. (2018) and Zhang et al. (2018) used the Image of Aging Scale developed by Levy et al.(2004). 62% (n = 8/13) used non-validated measures or developed their scales to measure ageism. Avidor et al. (2017), Kim (2015), and Shin et al. (2018) used a dichotomous variable to measure age-based discriminations. Bai et al. (2016) used a measure of perceptions of aging as a burden to examine the self-directed ageism of older adults. Fernandez-Ballesteros et al. (2017) used three questions with a 4-point Likert-type scale to measure negatively perceived age discrimination. Garstka et al. (2004) measured ageism through four different items: victims of age discrimination as an individual, age group victimized by society according to age, deprivation of opportunities, and discrimination due to old age. Siguaw et al. (2017) used four items that were developed by Garstka et al. (2004). Sabik (2013) used five questions to assess ageism: individual/age group deprivation of opportunities, exclusion from many sectors of public life, considered to be worthless after retirement, achievements not properly appreciated because of chronological old age. All measures of ageism in the included studies provided Cronbach’s alpha, and 85% (n = 11/13) were above .75.
Psychological Well-being
92% (n = 11/13) used validated outcome measures to evaluate older adults’ psychological well-being. Reviewed studies measured psychological well-being with different measurement instruments such as depression, subjective well-being through life satisfaction, and mental health. The outcome variable for 54% of the studies (n = 7/13) was depression. 38% (n = 5/13) used the concept of subject well-being by measuring life satisfaction. Ballesteros et al.’ s (2017) study included a life satisfaction measure as a component of measuring active aging. Garstka et al. (2004) assessed self-esteem in addition to life satisfaction as outcome measures. Sabik (2013) used the 5-item Mental Health subscale from the MOS 36-Item Short-Form Health Survey, which assesses general mental health and well-being. Cronbach’s alphas of all the measures of psychological well-being in the included studies were all above. Seventy-seven except the life satisfaction measure (Cronbach’s α: 0.57) of Garstka et al. (2004).
Relationship between Ageism and Psychological Well-being
All of the studies indicated that an increase in experiences of ageism was a statistically significant predictor of decreased psychological well-being in older adults (Table 4). 62% (n = 8/13) examined ageism as a predictor that influences the psychological well-being of older adults through the regression analysis. All regressions include many control variables such as sociodemographic, socioeconomic, and physical health status. 38% (n = 5/13) conducted structural equation modeling tests to look at direct or indirect effects of ageism.
Depression was an outcome assessed in 54% (n = 7/13). An increase in experiences or perceptions of ageism (or age discrimination) was associated with an increase in depressive symptoms as well as stress and anxiety. The study by Lyons et al. (2017) showed that ageism experience is significantly related to the prevalence of stress and anxiety disorders, as well as depression. In Lee and Kim’s (2016) study, ageism was found to affect stress directly and had an indirect effect on depression through stress. Zhang et al. (2019) indicated that negative age stereotypes were associated with higher levels of depression and loneliness and lower morale.
Summary of Results (Relationship between Ageism and Psychological Well-being).
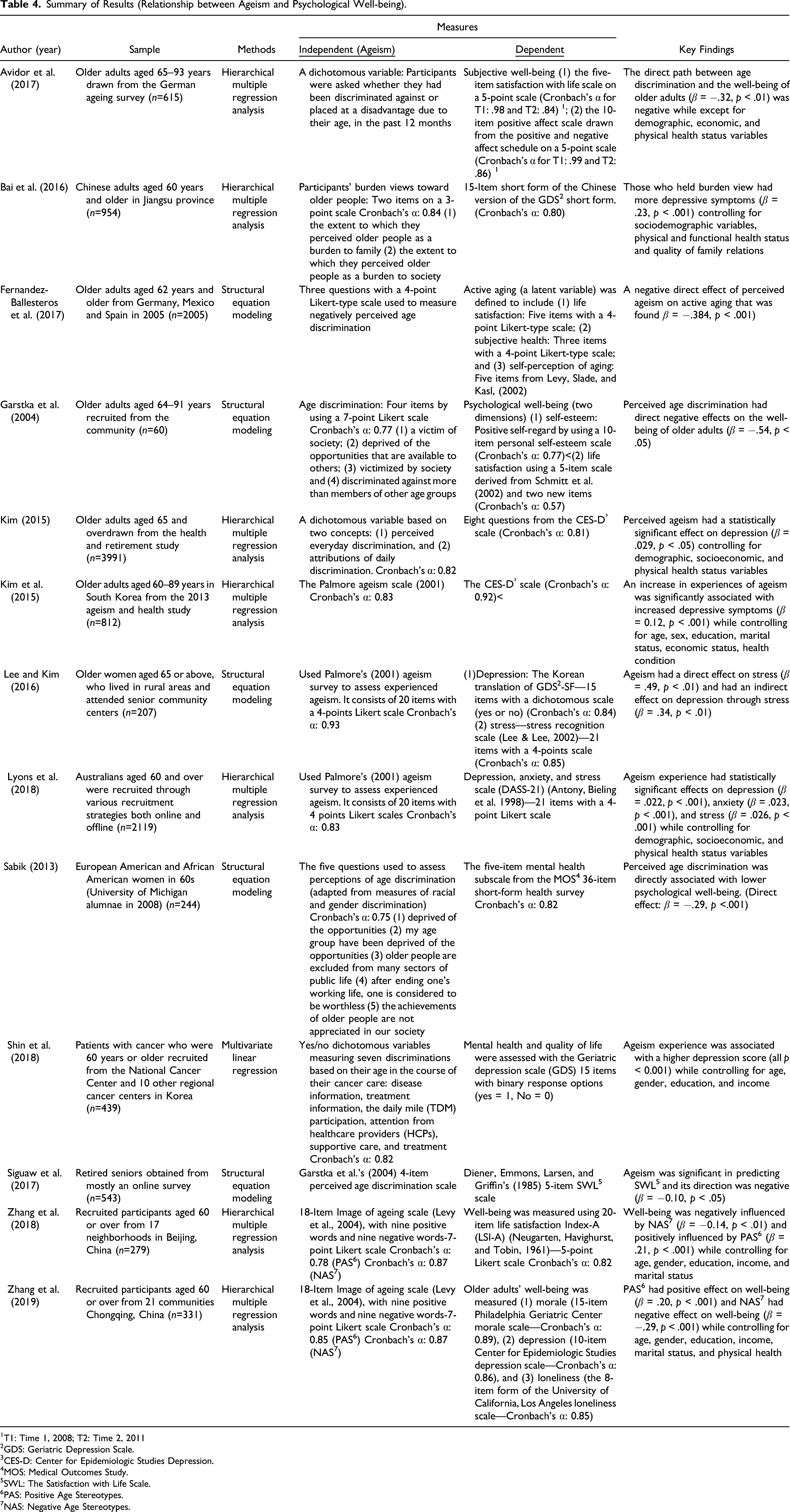
1T1: Time 1, 2008; T2: Time 2, 2011
2GDS: Geriatric Depression Scale.
3CES-D: Center for Epidemiologic Studies Depression.
4MOS: Medical Outcomes Study.
5SWL: The Satisfaction with Life Scale.
6PAS: Positive Age Stereotypes.
7NAS: Negative Age Stereotypes.
Interventions Between Ageism and Psychological Well-being
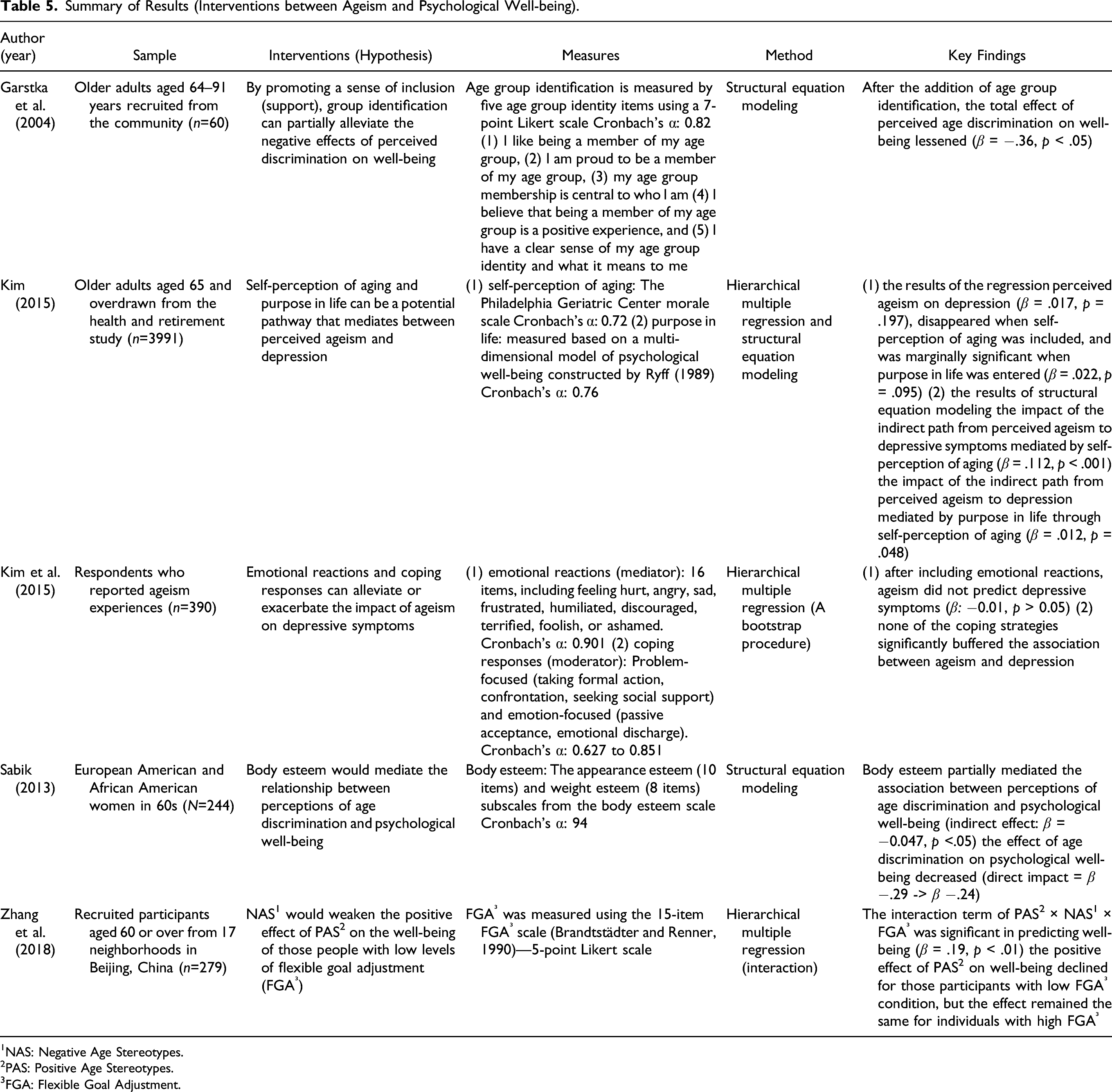
Summary of Results (Interventions between Ageism and Psychological Well-being).
1NAS: Negative Age Stereotypes.
2PAS: Positive Age Stereotypes.
3FGA: Flexible Goal Adjustment.
Kim (2015) tested the mediating effects of self-perception of aging and purpose in life on the relationship between ageism and depression. The overall indirect effect of ageism on depression mediated by self-perception of aging and purpose in life was statistically significant (β = .124, p < .001). The mediating effect of self-perception of aging (β = .112, p < .001) was larger than that of purpose in life (β = .012, p = .048).
Kim et al. (2015) examined the mediating effect of emotional reactions and the moderating effect of coping responses. The duration of many negative emotional reactions was examined, including being hurt, angry, frustrated, humiliated, discouraged, terrified, foolish, or ashamed. Coping responses included problem-focused responses such as formal action, confrontation, and seeking support, and emotion-focused such as passive acceptance and emotional discharge. Although the results did not confirm the moderating effect of coping responses, the effect of ageism on depression (β = −.01, p > 0.05) was no more statistically significant after adding emotional reactions.
Sabik (2013) tested the mediating effect of body esteem on the relationship between ageism and the psychological well-being of older adults. Sabik assumed that a high level of body esteem might mediate the association between ageism and psychological well-being. The results suggested that body esteem partially mediated the association (indirect effect: β = −0.047, p < .05); that is, the effect of ageism on psychological well-being was decreased from −.29 (β, p < .001) to −.24 (β, p < .001).
Lastly, Zhang et al. (2018) examined a moderating role of flexible goal adjustment (FGA) between age stereotypes and the well-being of older adults. FGA implies that individuals pursue their own personal goals, disengaging from goals that are incompatible with their preferences and altering their goals in response to unique conditions. Zhang et al. (2018) found that the interaction term, including FGA, was significant in predicting well-being (β = .19, p < .01). Negative age stereotypes decreased the positive effect of positive age stereotypes on well-being for older adults with low FGA conditions, but the effect remained the same for individuals with high FGA.
Methodological Quality
Review of Methodological Quality.

a Were the criteria for inclusion in the sample clearly defined?
b Were the study subjects and the setting described in detail?
c Was the exposure measured in a valid and reliable way?
d Were objective, standard criteria used for measurement of the condition?
e Were confounding factors identified?
f Were strategies to deal with confounding factors stated?
g Were the outcomes measured in a valid and reliable way?
h Was appropriate statistical analysis used?
*Y: Yes; N: No; U: Unclear; N/A: Not applicable.
Discussion
The first goal of this study was to locate studies that examined the relationship between ageism and older adults’ psychological well-being. A total of 13 studies were identified through a comprehensive search, and all of them empirically showed the negative effects of ageism on the psychological well-being of older adults. That is, older adults who perceived or experienced ageism were more likely to show lower levels of psychological well-being than those who did not perceive or experience ageism. Moreover, the psychological well-being of older people was adversely affected if they held internalized ageist thoughts.
The second goal of the study was to identify mediating or moderating factors between ageism and the psychological well-being of older adults. Five of the reviewed studies tested mediating or moderating effects of interventions between ageism and psychological well-being. Except for the coping responses, all mediating variables buffered the negative effects of ageism on psychological well-being in older adults. Age group identification (Garstka et al., 2004), emotional reactions (Kim et al., 2015), self-perception of aging and purpose in life (Kim, 2015), body esteem (Sabik, 2015), and flexible goal adjustment (Zhang et al., 2018) were all identified as effective mediators to mitigate the negative effects of ageism on the psychological well-being.
To briefly synthesize the interventions, the psychological well-being of older adults (1) who were proud to be a member of their age group, (2) who experienced less negative emotions (i.e., feeling hurt, angry, sad, frustrated, humiliated, discouraged, terrified, foolish, or ashamed), (3) who considered aging process positively and held a positive view of their future, (4) who had greater body esteem, and (5) who had high levels of flexible goal adjustment were less negatively influenced by ageism. These mediators can inform intervention developments that will lessen the effects of ageism and improve older adults’ psychological well-being.
Scholars who investigate the extent of the detrimental impacts of ageism on older adults have focused on developing effective interventions in recent years (Bujang, Sa’at, & Bakar, 2017). For instance, Burnes et al.’s (2019) systematic review of interventions to reduce ageism against older adults found that aging education toward young people and intergenerational contact were effective approaches for adolescents and young adults. However, it remains a question whether education and intergenerational contact can fully reduce the effects of ageism on older adults. In addition, during the COVID-19 pandemic, maintaining contact between generations has been an increasingly challenging endeavor. Thus, it is important to discuss how the negative effects of ageism among older adults during the pandemic. We believe that the intervention results of our study can be used as a basis for implementing innovative strategies to reduce ageism’s pernicious effects among older adults during periods of social distancing. These effects may result in a necessity for effective interventions in older adults, such as education for positive aging, emotional management, boosting body confidence, and flexible goal setting that may serve as downstream factors to mitigate or perhaps reverse negative effects of ageism on their psychological well-being. Our review also provides theoretical frameworks that enable a deeper understanding of the role of ageism in psychological well-being. One of these is the stress process model (Kim, 2015). Recurrent experiences of ageism can be a stressor, and exposure to these stressful events could lead to depressive symptoms (Kim, 2015). Unlike other stressors, ageism cannot be resolved only at the individual level. All age groups should be involved in addressing issues regarding ageism because it is one of the most socially condoned and institutionalized forms of prejudice that is reflected in many areas of society (Nelson, 2005). The stereotype embodiment framework also helps us understand how ageism inhibits the psychological well-being of older adults. Stereotype embodiment refers to a person’s internalization of age stereotypes through life-long exposure (Levy, 2009). This tends to adversely affect older adults psychologically, behaviorally, and physiologically. That is, when older adults endorse negative stereotypes, they are more likely to experience a broader range of adverse health outcomes.
Through the review process, we found that the research on the relationship between ageism and the psychological well-being of older adults is at an early stage with ample room for development. The number of identified quantitative studies was small, and most studies identified were conceptual. Considering that ageism is an immediate societal issue, more quantitative studies that provide generalizable empirical evidence are needed. Additionally, very few interventions regarding mediating or moderating factors between ageism and psychological well-being have been identified. That is, no definitive answer has been given for an effective method to deal with the negative effects of ageism. The need to develop an effective intervention as a buffer against the negative effects of ageism has increased due to the pervasive ageism in current society. Finding a way to mitigate or end the negative effects of ageism, especially on the psychological well-being of older adults, would provide additional insight into successful aging.
We also found the measurement of ageism to be insufficient. Among our identified studies, Kim et al. (2015), Lee and Kim (2016), and Lyons et al. (2018) used Palmore (2001)’s ageism measure, and Zhang et al. (2018) and Zhang et al. (2019) used the Levy’s et al. (2004) Image of Aging Scale. Palmore’s (2001) measure and Levy’s et al. (2004) measure assess ageism from different perspectives. While Palmer examined discrimination experienced by older adults, the Images of Aging Scale by Levy et al. (2004) could be completed by respondents of any age and asked to rate the degree to which the words or phrases are representative of older adults. That is, Zhang et al. (2018) and Zhang et al. (2019) adopted and revised ageism scales that were specifically designed to measure the attitudes of younger people toward older people. Similarly, Bai et al. (2016) employed a measure of “perceptions of aging as a burden” to examine internalized ageism of older adults. Palmore’s (2001) scale was the only one to examine how older adults felt and responded to being perceived as a stereotype. However, Palmor’s (2001) scale is inadequate since it does not account for all aspects of ageism, and because of the ambiguous terminology, it is difficult to determine how the original meaning of the items was meant to be understood (Kang, 2020). Except for the five studies, other studies in this review used not established scales such as uni-dimensional or simple measures. Ageism is a subjective concept, which requires considerable effort to measure accurately. Considering that ageism can be assessed using cognitive, behavioral, and informative components, a comprehensive set of constructs is necessary, as these constructs contain reliable and valid indicators.
Several limitations were identified in this systematic review. In our search, we identified a limited number of studies; whereas a comprehensive search was conducted, we found only thirteen studies that met the criteria for inclusion. Although we aimed to include all potentially relevant studies through a comprehensive search using a wide range of search strategies, some literature could not be included. For example, we were not able to include studies in languages other than English. Further, we found several articles that discussed the ageism of older adults aged 50+ or 55+. Our review also found many qualitative studies on ageism. Therefore, we suggest that future researchers might consider setting an age cutoff of 50 for the review, which would provide a larger number of studies to consider. In addition, research will be conducted to review more diverse forms of evidence, both quantitatively and qualitatively. Using qualitative research methods can also help to deepen the understanding of ageism, which is an extremely subjective concept.
Conclusion
From our review, we found that ageism can be a significant threat to the well-being of older adults. Ageism is negatively associated with older adults’ psychological health, causing mental health issues such as depression and anxiety and well-being in a negative way. Considering the growing mental health needs of older adults, future research needs to focus on establishing an effective preventive intervention against ageism. The importance of reducing or preventing ageism is often noted (Nelson, 2005; Raposo & Carstensen, 2015), but few specific methods or variables have been presented that might help to reduce ageism, especially from the perspective of older adults. The results from the systematic review contribute to building a literature base that can be used to guide future research on developing interventions for older adults.
In light of the rapid growth of aging people, research on ageism should receive greater attention. While ageism, unlike sexism or racism, is a problem that all individuals may potentially face (Nemmers, 2005), its importance has been neglected, and there is much less research on ageism than on sexism and racism (Kim, 2009). Significant scholarly attention should be given to ageism, considering its importance and universality, as it encompasses every generation and the growth of the population of older adults. At this important moment, this systematic review lays the foundation for future work on ageism against older adults.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Appendix A
Search Strategy
ProQuest Research Library—August 31, 2019
1. All (“prejudice” or “stigma” or “labelling” or “stereotyp*“) in anywhere except full text-ALL
2. All (“age*” or “age-related”) in anywhere except full text-ALL
3. All (“ageism” or “ageist” or “age discrimination”) in anywhere except full text-ALL
4. All (“older*” or “elder*” or “senior*” or “aged” or “old age”) in anywhere except full text-ALL
5. All (“psycholo*” or “emotion*” or “mental” or “stress” or “isolation” or “satisfaction”) in anywhere except full text-ALL
6. All (“well-being” or “outcome” or “impact*” or “result*” or “health”) in anywhere except full text-ALL
7. All (“quality of life” or “life satisfaction”) in anywhere except full text-ALL
8. 1 and 2
9. 3 or 8
10.4 and 9
11.5 and 6
12.7 or 11
13.10 and 12
Web of Science—August 31, 2019
1. Topic: (“prejudice” or “stigma” or “labelling” or “stereotyp*”)
2. Topic: (“age*” or “age-related”)
3. Topic: (“ageism” or “ageist” or “age discrimination”)
4. Topic: (“older*” or “elder*” or “senior*” or “aged” or “old age”)
5. Topic: (“psycholo*" OR “emotion*" OR “mental” OR “stress” OR “isolation” OR “satisfaction")
6. Topic: (“well-being” OR “outcome” OR “impact*" OR “result*" OR “health")
7. Topic: (“quality of life” or “life satisfaction”)
8. 1 and 2
9. 3 or 8
10.4 and 9
11.5 and 6
12.7 or 11
13.10 and 12
Academic Search Complete—August 31, 2019
1. All (“prejudice” or “stigma” or “labelling” or “stereotyp*“) in anywhere except full text-ALL
2. All (“age*” or “age-related”) in anywhere except full text-ALL
3. All (“ageism” or “ageist” or “age discrimination”) in anywhere except full text-ALL
4. All (“older*” or “elder*” or “senior*” or “aged” or “old age”) in anywhere except full text-ALL
5. All (“psycholo*” or “emotion*” or “mental” or “stress” or “isolation” or “satisfaction”) in anywhere except full text-ALL
6. All (“well-being” or “outcome” or “impact*” or “result*” or “health”) in anywhere except full text-ALL
7. All (“quality of life” or “life satisfaction”) in anywhere except full text-ALL
8. 1 and 2
9. 3 or 8
10.4 and 9
11.5 and 6
12.7 or 11
13.10 and 12
Appendix B
PRISMA 2020 Item Checklist Note. The PRISMA 2020 item checklist is from Page et al. (2021).
Title
1
Identify the report as a systematic review
1
Abstract
2
Provide a structured summary including, as applicable: Background: Main objectives methods: Data sources; study eligibility criteria, participants, and interventions; study appraisal; and synthesis methods, such as network meta-analysis. Results: Number of studies and participants identified; summary estimates with corresponding confidence/credible intervals; treatment rankings may also be discussed. Authors may choose to summarize pairwise comparisons against a chosen treatment included in their analyses for brevity. Discussion/Conclusions: Limitations; conclusions and implications of findings. Other: Primary source of funding; systematic review registration number with registry name
1
Rationale
3
Describe the rationale for the review in the context of existing knowledge
2–3
Objectives
4
Provide an explicit statement of the objective(s) or question(s) the review addresses
4–5
Eligibility criteria
5
Specify the inclusion and exclusion criteria for the review and how studies were grouped for the syntheses
6–8
Information sources
6
Specify all databases, registers, websites, organizations, reference lists and other sources searched or consulted to identify studies. Specify the date when each source was last searched or consulted
8–9
Search strategy
7
Present the full search strategies for all databases, registers and websites, including any filters and limits used
8–9, AppendixA
Selection process
8
Specify the methods used to decide whether a study met the inclusion criteria of the review, including how many reviewers screened each record and each report retrieved, whether they worked independently, and if applicable, details of automation tools used in the process
9–10
Data collection process
9
Specify the methods used to collect data from reports, including how many reviewers collected data from each report, whether they worked independently, any processes for obtaining or confirming data from study investigators, and if applicable, details of automation tools used in the process
9–10
Data items
10a
List and define all outcomes for which data were sought. Specify whether all results that were compatible with each outcome domain in each study were sought (e.g., for all measures, time points, analyses), and if not, the methods used to decide which results to collect
7
10b
List and define all other variables for which data were sought (e.g., participant and intervention characteristics, funding sources). Describe any assumptions made about any missing or unclear information
6–7
Study risk of bias assessment
11
Specify the methods used to assess risk of bias in the included studies, including details of the tool(s) used, how many reviewers assessed each study and whether they worked independently, and if applicable, details of automation tools used in the process
10
Effect measures
12
Specify for each outcome the effect measure(s) (e.g., risk ratio, mean difference) used in the synthesis or presentation of results
10
Synthesis methods
13a
Describe the processes used to decide which studies were eligible for each synthesis (e.g., tabulating the study intervention characteristics and comparing against the planned groups for each synthesis (item #5))
10
13b
Describe any methods required to prepare the data for presentation or synthesis, such as handling of missing summary statistics, or data conversions
N/A
13c
Describe any methods used to tabulate or visually display results of individual studies and syntheses
N/A
13d
Describe any methods used to synthesize results and provide a rationale for the choice(s). If meta-analysis was performed, describe the model(s), method(s) to identify the presence and extent of statistical heterogeneity, and software package(s) used
N/A
13e
Describe any methods used to explore possible causes of heterogeneity among study results (e.g., subgroup analysis, meta-regression)
N/A
13f
Describe any sensitivity analyses conducted to assess robustness of the synthesized results
N/A
Reporting bias assessment
14
Describe any methods used to assess risk of bias due to missing results in a synthesis (arising from reporting biases)
Table 5
Certainty assessment
15
Describe any methods used to assess certainty (or confidence) in the body of evidence for an outcome
N/A
Study selection
16a
Describe the results of the search and selection process, from the number of records identified in the search to the number of studies included in the review, ideally using a flow diagram
10–11, Figure 1
16b
Cite studies that might appear to meet the inclusion criteria, but which were excluded, and explain why they were excluded
10–11
Study characteristics
17
Cite each included study and present its characteristics
11–12 Table 1 and 2
Risk of bias in studies
18
Present assessments of risk of bias for each included study
19–20 Table 5
Results of individual studies
19
For all outcomes, present, for each study: (a) Summary statistics for each group (where appropriate) and (b) an effect estimate and its precision (e.g., confidence/credible interval), ideally using structured tables or plots
Table 3 and 4
Results of syntheses
20a
For each synthesis, briefly summarize the characteristics and risk of bias among contributing studies
11–12
20b
Present results of all statistical syntheses conducted. If meta-analysis was done, present for each the summary estimate and its precision (e.g., confidence/credible interval) and measures of statistical heterogeneity. If comparing groups, describe the direction of the effect
15–18
20c
Present results of all investigations of possible causes of heterogeneity among study results
N/A
20d
Present results of all sensitivity analyses conducted to assess the robustness of the synthesized results
19–20 Table 5
Reporting biases
21
Present assessments of risk of bias due to missing results (arising from reporting biases) for each synthesis assessed
19–20 Table 5
Certainty of evidence
22
Present assessments of certainty (or confidence) in the body of evidence for each outcome assessed
N/A
Discussion
23a
Provide a general interpretation of the results in the context of other evidence
20–21
23b
Discuss any limitations of the evidence included in the review
19–20 Table 5
23c
Discuss any limitations of the review processes used
24
23d
Discuss implications of the results for practice, policy, and future research
21–23
Registration and protocol
24a
Provide registration information for the review, including register name and registration number, or state that the review was not registered
N/A
24b
Indicate where the review protocol can be accessed, or state that a protocol was not prepared
N/A
24c
Describe and explain any amendments to information provided at registration or in the protocol
N/A
Support
25
Describe sources of financial or non-financial support for the review, and the role of the funders or sponsors in the review
N/A
Competing interests
26
Declare any competing interests of review authors
N/A
Availability of data, code and other materials
27
Report which of the following are publicly available and where they can be found: Template data collection forms; data extracted from included studies; data used for all analyses; analytic code; any other materials used in the review
N/A