
Abstract
The increasing global geriatric population, including Pakistan’s, poses significant challenges to nurses due to the limited resources, knowledge, and frailty of older patients. Addressing these challenges is not only crucial but also of utmost importance for delivering high-quality care to geriatric populations. This study investigates nurses’ perceptions and challenges in geriatric inpatient tertiary care hospitals. The study used a qualitative exploratory design, conducting semi-structured interviews with 13 nurses at a tertiary teaching hospital in Karachi. The study highlights nurses’ perceptions of geriatric care as a complex yet emotionally rewarding field. Comorbidities, dependency, non-compliance, communication gaps, and a lack of specialized education were identified as challenges for nurses. It recommends improved infrastructure, separate wards, staffing ratios, and enabling factors such as kindness and compassion to enhance care. The study examines nurses’ perceptions of geriatric care, including enabling factors and challenges, highlighting crucial considerations for healthcare professionals and management to provide effective care for older adult patients.
What This Paper Adds
This study has explored nurses’ perceptions of geriatric care as complex and emotionally rewarding. The multifaceted health issues, holistic care, and therapeutic relationships that geriatric care entails contribute to professional satisfaction and a sense of fulfilment among nurses. This emotional reward is a significant aspect of the profession that can attract more nurses to this field.
This paper emphasizes the addition of geriatrics as a specialty in the curriculum and highlights its utmost importance in clinical care settings from the nurse’s perspective.
The study highlights the challenges faced by nurses in geriatric care, including comorbidities, communication gaps, dependency, non-compliance, and a lack of specialized education, all of which are necessary due to the complex healthcare needs of older adults. These challenges are exacerbated by communication barriers and insufficient training in geriatrics, underscoring the need for continuous professional education.
Applications of Study Findings
The primary finding highlights the importance of recognizing geriatric care as a specialized field and incorporating it into nursing curricula for healthcare leaders and educators.
Hospital management’s identification of challenges can lead to interventions regarding nurse training and education, the establishment of geriatric wards, and curriculum integrations by incorporating geriatric nursing at undergraduate and graduate levels to prepare future nurses with the necessary skills and knowledge for older adult care.
Background
Geriatrics is the field of medicine that deals with managing diseases and caring for older adults” (Türkbeyler et al., 2019). Older adult care encompasses the emotional, physical, social, and spiritual aspects, including living assistance, hospice care, nursing, and home-based care, to meet the unique needs of older adults (Efiong, 2015). The aging population has an impact on health resources. Additionally, older adults are perceived as requiring more quality nursing care and medical resources (DeFrances et al., 2010). Moreover, the number of hospitalization cases among older adult patients is more than double that of other adult patients (Centers for Disease Control and Prevention, 2021). The UN predicts that by 2050, 8 out of 10 individuals over 60 will reside in lower and middle-income countries due to the global aging issue (United Nations, 2017). The increasing demand for healthcare services is exacerbated by inadequate healthcare structures and a shortage of trained staff in providing care to older adults in low- and middle-income countries (Abudu-Birresborn et al., 2019).
Pakistan, the sixth-most populous country globally, is experiencing a rising life expectancy, with an estimated 72-year life expectancy by 2023. However, the country’s geriatric population, expected to reach 27 million by 2050, is disproportionately affected by a weak pension system, economic recession, and lack of health insurance (Cassum et al., 2020). Pakistan’s health system is considered fragile compared to those of developed countries (Tariq, 2021). Older adult patients require specialized healthcare professionals with high qualifications and geriatric training to provide comprehensive care and address their unique health needs (Kotsani et al., 2021). Overwork in acute care often results in missed care for fragile older adult patients due to their complexity, communication challenges, and high dependency (Rezaei-Shahsavarloo et al., 2021).
Advanced age is associated with multiple morbidities and a high mortality rate (Heydari et al., 2019). Ageism negatively impacts healthcare professionals’ perceptions and attitudes toward older adults, often leading to stereotypes of poverty, impaired mental health, loneliness, and unhappiness (Musaiger & D'Souza, 2009). In addition, geriatric patients are highly dependent and need more care and time. As a result, nurses see this care negatively (Liu et al., 2013). In contrast, some studies have concluded that nurses have a positive attitude toward caring for older adult patients (Mahmud et al., 2020). A study in Nigeria found that nurses reported feeling positive while caring for geriatric patients (Oyetunde et al., 2013).
Furthermore, multiple studies reveal challenges affecting nurses’ care of older patients, highlighting their insufficient capabilities to manage the needs of hospitalized older adult patients effectively (Rejeh et al., 2010). A Nigerian study found that a lack of special education, social support, and specialized wards influences geriatric care. In contrast, a Turkish study found that policies and disregard toward geriatric patients also impact older adult care (Adibelli & Kılıç, 2013). The increasing number of older adult patients has significantly impacted nurses, leading to a higher demand for their services in elder care (Carlson & Idvall, 2015). Moreover, studies worldwide suggest that nurses have poor knowledge of geriatric care (Amsalu et al., 2021). Quality care for geriatric patients requires adequate expertise and trained nurses with specialized skills in geriatric care to improve outcomes, reduce hospital stays and readmissions, and enhance overall patient care (Amsalu et al., 2021).
Unfortunately, Geriatric nursing is a neglected field in Pakistan, with undergraduate and graduate nursing programs not focusing on this specialty (Khokhar, 2012). Limited research exists on geriatric care in the country (Ejaz & Sughra, 2019). Different perceptions and challenges exist among nurses toward older adult care in Pakistan. Therefore, this study aims to rule out nurses’ perceptions and challenges in caring for older adult patients. It helps nurses share challenges and provides insights for government and healthcare stakeholders. The findings can guide healthcare providers in focusing on specialized care and providing education-level training, with support from healthcare and government stakeholders, to address the growing number of older adult patients effectively.
Methodology
Study Design
This study employed a qualitative exploratory design using a content analysis approach with an interpretive stance to investigate factors, allowing for direct exploration of the phenomenon through participants’ experiences and a comprehensive understanding of their perceptions. This design is helpful when exploring a particular phenomenon directly from the participants’ experience. It is considered feasible for exploring and understanding the phenomenon, along with the associated perceptions of the participants (Creswell & Poth, 2016). To ensure methodological rigor, Consolidated criteria for reporting qualitative research (COREQ) were followed (Additional File 1).
Study Setting
This study was conducted at a tertiary teaching hospital in Karachi, Pakistan, aiming to investigate the perceptions of experienced nurses from diverse specialties, including emergency medicine, internal medicine, critical care, musculoskeletal care, cardiology, neurology, and surgical wards.
Sampling Strategy
This study employed purposeful sampling to focus on nurses with valuable insights into the care of admitted geriatric patients. Participants included experienced registered nurses holding bachelor’s degrees in nursing who had two or more years of experience in inpatient care in their respective wards. Both male and female nurses were included, while those with less than 2 years of experience in the specified wards and lacking the necessary educational qualifications were excluded.
A total of 13 nurses were interviewed till data saturation was achieved, as no new codes and data emerged further. It is often referred to as “data” or “thematic” saturation, and it has evolved beyond its roots in grounded theory to encompass several qualitative research communities. Saturation has evolved as the “gold standard” in qualitative research, along with its definition being expanded to include “no new data,” “no new theme,” and “no new codes ”(Vasileiou et al., 2018). A sample size of 13 was considered sufficient, as it falls within the empirical recommendations for achieving thematic saturation (Hennink & Kaiser, 2022). Moreover, it also aligned with the principle of informational redundancy (Lincoln, 1985), which ensured that unnecessary oversampling was avoided once no new theme emerged.
Data Collection
Data were gathered after obtaining approval from the Ethical Review Committee (ERC) through semi-structured interviews (Appendix 1). The most popular method for gathering qualitative data in health services research is semi-structured in-depth interviews. This approach typically involves a conversation between the participant and the researcher, guided by an adaptable interview protocol that includes questions, probes, and comments. It enables researchers to gather open-ended data and investigate participants’ opinions, sentiments, and beliefs regarding a particular phenomenon (DeJonckheere & Vaughn, 2019). During data collection, open-ended questions were used to elicit meaningful responses regarding geriatric patients and their care. Interviews were conducted in a comfortable room. The time and place were chosen according to participants’ wishes, ensuring their privacy. It lasted for 40 to 50 min, supported by a questionnaire with guiding questions and probes. Permission was obtained from participants to record and transcribe the interviews. The interview explored the challenges of caring for geriatric patients and participants’ perceptions of geriatric care. Interviews were recorded to capture the data more effectively (Jamshed, 2014). Identity protection was ensured through coding, and transcripts were securely stored in password-protected files.
Data Analysis
Demographic details were tabulated, and data were analyzed using an interpretive approach to content analysis following Graneheim and Lundman’s (2004) process. The process involved five steps: transcription, repeated reading for comprehension, identification of primary codes, grouping similar codes into major categories, and identifying major themes within these categories (Graneheim & Lundman, 2004). Categories and themes were validated with subject matter experts, healthcare professionals, and researchers to ensure alignment with participants’ responses. The researcher meticulously listened, identifying the connections between the data and the participants’ emotions, which led to the identification of codes, categories, and themes. Categories and themes were validated with the research team to ensure alignment with participants’ responses.
Following Lincoln’s (1985) criteria, Rigor included dependability, credibility, transferability, and confirmability. An audit was conducted by the research supervisor and a committee member to ensure the dependability of the study. Confirmability was achieved through the maintenance of the audit trail and the rechecking of documentation. Furthermore, codes, categories, and themes were finalized under the supervision of committee members and research experts. The truthfulness of the study was established through data validations. This was ensured by returning to the participants for the confirmation and validation of the data. Details regarding the sample, study setting, and results were included, aiming for rich data and transferability of results to similar settings. Moreover, reflexivity was maintained throughout the study by the research team, which included one male master’s student and three female nurse educators, two of whom hold PhD in nursing and are experienced qualitative researchers, and one who holds a master’s degree in nursing. They actively engaged in reflexivity. The team regularly assessed and recorded their own biases and potential impact on data interpretation, considering the mostly female participant group.
Results
The demographic data are tabulated below: Out of the 13 participants, the majority were females, with an age range of 25 to 31 years. Participants included nurses with undergraduate and graduate education. The participants had an average of 5 years of experience. Moreover, to ensure variability, nurses from different departments and years of experience were selected (Refer to Table 1).
Socio-demographics.
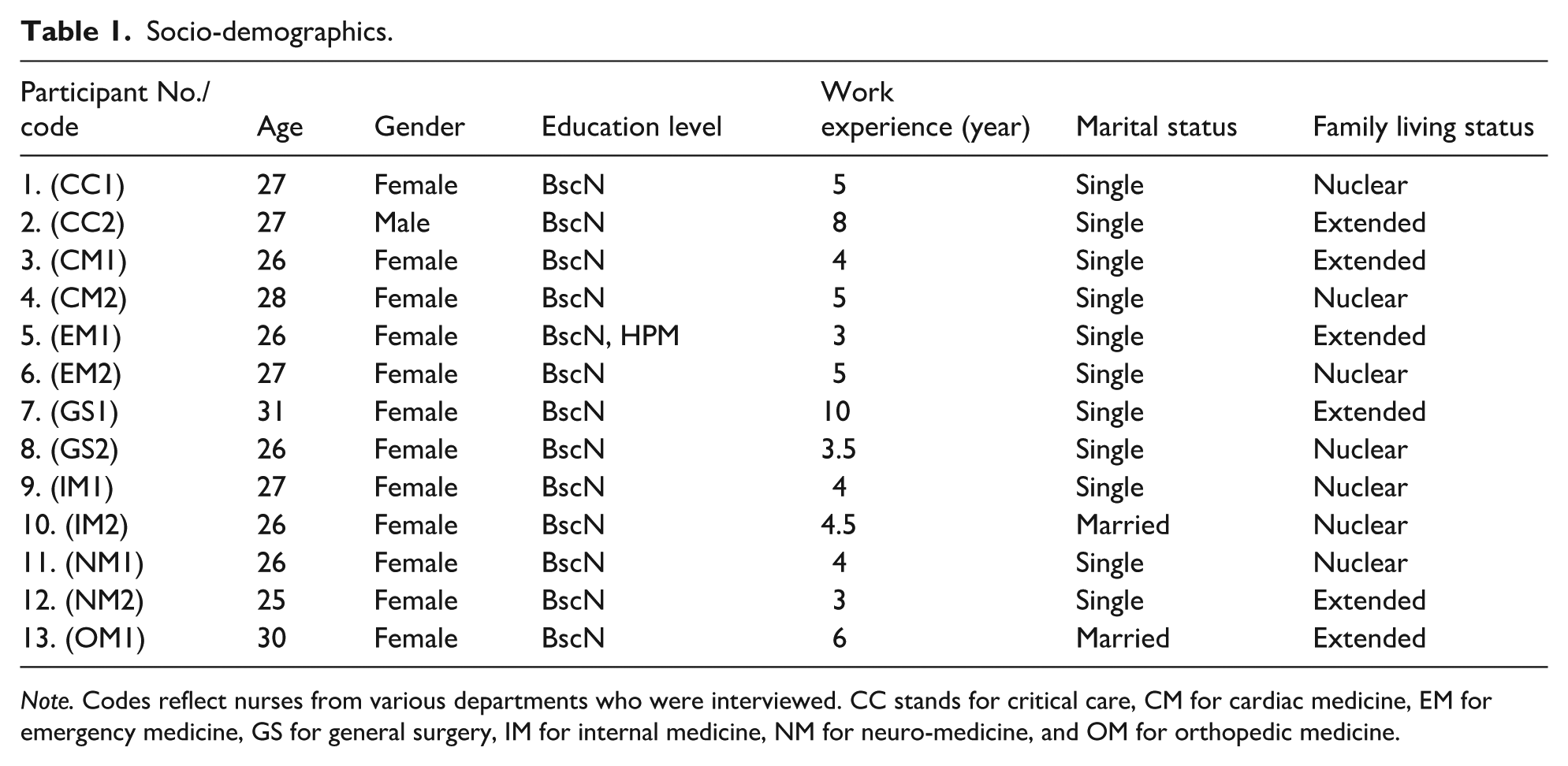
Note. Codes reflect nurses from various departments who were interviewed. CC stands for critical care, CM for cardiac medicine, EM for emergency medicine, GS for general surgery, IM for internal medicine, NM for neuro-medicine, and OM for orthopedic medicine.
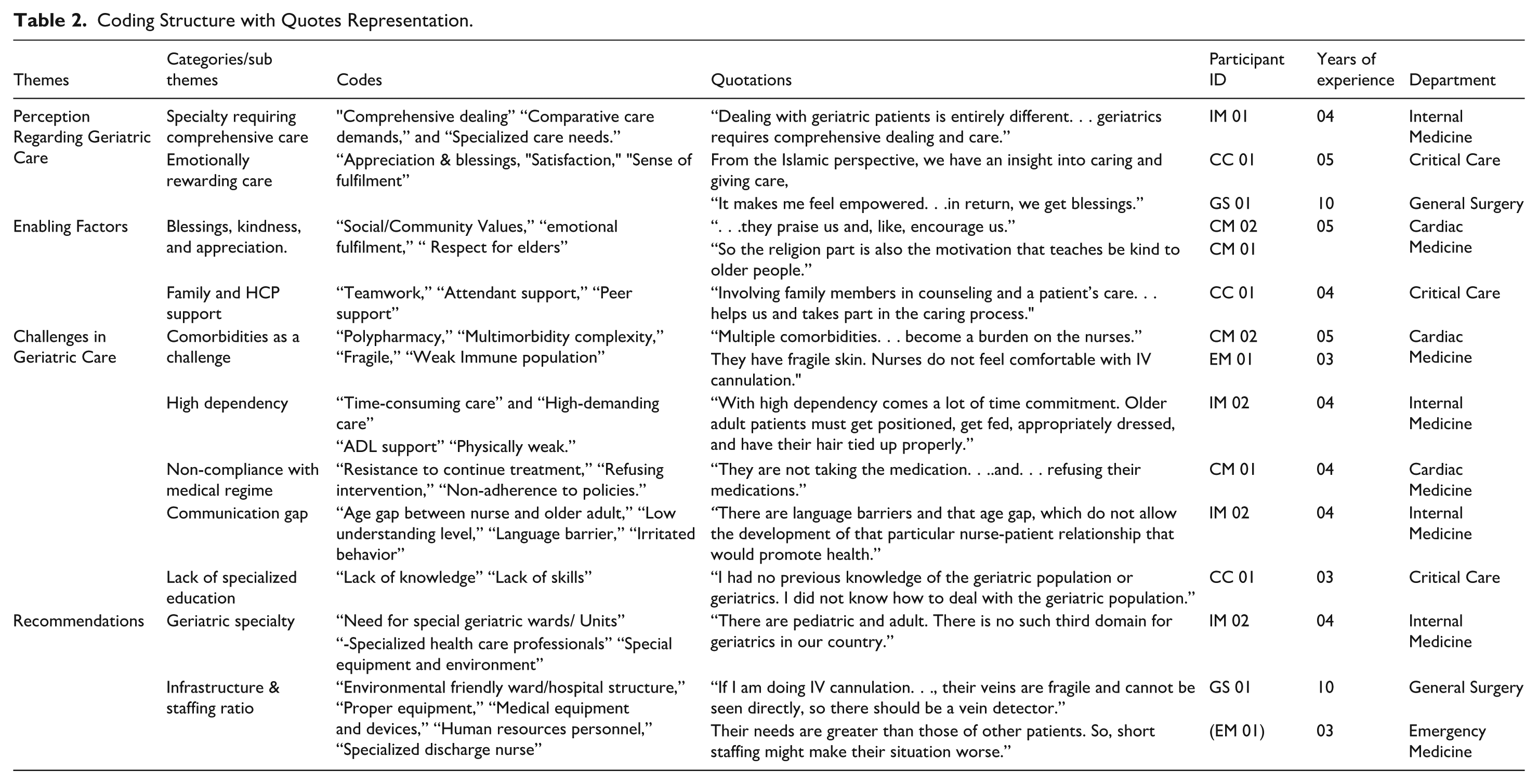
Data obtained from nurses through semi-structured interviews were manually analyzed, resulting in the identification of codes and the clustering of similar codes to derive categories and themes. The coding structure and representative quotes, along with the metadata of the participants, are presented in Table 2 to ensure transparency.
Coding Structure with Quotes Representation.
Finally, four themes were derived through analysis (Refer to Figure 1). Then, the sub-themes and categories were interpreted using quotes from the participants. The relationship among themes and categories/sub-themes is shown in Figure 2.

Themes and categories.

Framework of interconnected themes.
Perception Regarding Geriatric Care
This theme describes how nurses perceive and define geriatric care and nursing from their perspective. According to the participants’ responses, two categories emerge that align with their perception of geriatric care. These are composed of specialties requiring comprehensive care and emotionally rewarding experiences, as discussed below.
Specialty Requiring Comprehensive Care
Nurses emphasized that older adult care is a specialized field that requires an individualized and comprehensive approach to cater to the complex physical, emotional, and cognitive healthcare needs of geriatric patients. “Dealing with geriatric patients is entirely different. . . geriatrics requires comprehensive dealing and care” (IM 01).
Unlike general nursing, it requires expert nurses, knowledge, and understanding that clinical integrates the variation in care and psychosocial support of ageing patients. “There must be an expert nurse who knows the needs, processes, and everything regarding geriatric populations” (IM 02). This signifies that geriatric care as a specialty requires a comprehensive approach.
Emotionally Rewarding Care
The participants identified that giving care to older adult patients gives a sense of fulfilment, satisfaction, and empowered care, as the quotes revealed that older adult care aligned with spiritual and cultural values “. . .As per the Islamic perspective, we have an insight of caring and giving care, and we have the concept of helping others as well” (CC 01). Nurses’ perceptions highlighted that older adult care provided emotional sustenance and a sense of reward, including blessings and prayers in return for the care provided. “Also, it makes me feel empowered because when caring for the elderly. . .in return, we get so many blessings” (GS 01).
Enabling Factors in Geriatric Care
Based on the analysis, two categories explained the participants’ responses, which facilitated and motivated them to care for geriatric patients. These categories include blessings, kindness, appreciation, and support from family and healthcare professionals.
Blessings, Kindness, and Appreciation
Participants reported that appreciation and kindness in geriatric care bring them a sense of fulfilment. Even small actions are met with greater blessings. “While caring. . .patient gets attached to us, or they praise us and, like, encourage us” (CM 02). Moreover, cultural and religious values provide them with ongoing support, helping to sustain the continuity of care. “So the religion part is also the motivation that teaches be kind to older people” (CM 01).
Family and HCP Support
Family and team member support during geriatric care is crucial in bridging the gap between personalized understanding and the treatment process. Nurses gained valuable insights into understanding the needs and behaviors of older adults. This facilitation not only eases the work burden but also creates a therapeutic alliance for nurses in the care environment. “Involving family members in counselling and a patient's care. . . helps us and takes part in the caring process” (CC 01).
Some participants also reported that team members supported and helped motivate us in the care process. One of them said, “If I cannot deal with an older adult patient, I have a good colleague who can help us” (CM 01).
Challenges in Geriatric Care
Nurses reported a unique set of challenges in caring for older adults. These challenges were Comorbidities, high dependency demand, non-compliance with the medical regime, communication gaps, and lack of specialized education.
Comorbidities as a Challenge
Nurses identified that older adult patients often have multiple chronic diseases and use multiple medications, making it challenging for them due to polypharmacy and disease burden, as treating one condition may lead to another. “Multiple comorbidities lead to a prolonged hospital stay for older adult patients, which becomes a burden on the nurses” (CM 02). Also, the fragility of older patients makes skincare and invasive procedures difficult due to their delicate and fragile skin. This fragility required a high level of skill and training. “They have very fragile skin and veins. Nurses do not feel comfortable doing many procedures like nasogastric tube insertion, IV cannulation, and catheterization” (EM 01).
High Dependency
The data analysis revealed that geriatric care is time-consuming and highly labor-intensive, causing discomfort to nurses due to physical demands and time constraints. One of the participants stated, “Older adult patients must get positioned, get fed, appropriately dressed, and get their hair tied up properly (IM 02), as this demands a significant time investment. Also, the independence of care gets compromised as these patients are dependent on nurses for their ADLs, which creates an extra burden on nurses. “They are mostly dependent on nurses for every little thing.” (CM 02).
Non-compliance with Medical Regime
Participants revealed that due to polypharmacy and long-term chronic disease, older adults get tired of continuing the medical regimen. As a result, they become reluctant to the treatment and medications. This poses a greater challenge for us to convince them of their continuity of care. “They are not taking the medication. . ..and. . . refusing their medications” (CM 01).
Communication Gap
Participants reported communication and behavioral issues with older adult patients due to generational gaps and hearing loss. This gap hinders the formation of therapeutic communication. As the participant reported, “There are language barriers and that age gap, which does not allow the development of that particular nurse-patient relationship that would promote health” (IM 02).
Lack of Specialized Education
Nurses identified their concerns regarding the lack of geriatric education and training in Pakistan, which hindered older adult care. Nurses often feel unprepared due to limited skills and training in geriatric care. This gap and lack of training result in compromised care. “I had no previous knowledge of the geriatric population or geriatrics. I did not know how to deal with the geriatric population" (CC 01). Similarly, another participant also endorsed that “Everyone is unwilling to take care of them for multiple reasons, as geriatric nursing in Pakistan is not that developed” (EM 01).
Recommendations for Better Care
The content’s findings proposed some recommendations to overcome the challenges, including improvements in the categories of geriatric specialty, infrastructure, and a better staffing ratio.
Geriatric Specialty
Participants identified the lack of a geriatric specialty in the Pakistani healthcare system. They highlighted that only two categories, pediatrics and adults, are prominent and proposed that the unique needs of the geriatric specialty be addressed to ensure nurses can provide individualized care. Due to the unavailability of this specialty, geriatric patients are treated in general wards alongside younger adults, resulting in their care being compromised due to the lack of specialized nurses. “There are pediatric and adult. There is no such third domain for geriatrics in our country” (IM 02). Specific wards are crucial for receiving specialized and individualized care. Additionally, it provides an environment for nurses to receive training and refine their skills. “There were no specific wards and courses where we got trained or got our skills polished for performing care for geriatric patients” (CM 02).
Infrastructure & Staffing Ratio
Participants identified specialized medical equipment, wards, and proper human resources as the key factors in improving geriatric care. Proper wards and equipment enhance patients’ safety. “If I am doing IV cannulations. . ., their veins are fragile and cannot be seen directly, so there should be a vein detector” (GS 01). Similarly, a nurse shortage can increase the risk of compromised care. Therefore, a proper staffing ratio is crucial to minimize the risk. “Their needs are greater than the other patients. So, short staffing might make their situation worse” (EM 01).
Discussion
Nurses view geriatric care as a specialty requiring comprehensive care due to the complex physical, cognitive, and emotional needs of older adults. Factors such as diseases and a weak physical status compromise their health, requiring high levels of assistance and understanding. Effective care can be achieved through therapeutic communication, the expertise of skilled healthcare professionals, and individualized care plans tailored to each patient’s needs. This perception is supported by a qualitative study in China, which emphasizes the importance of comprehensive assessment and personalized care for older adults (Li et al., 2021).
Nurses also found geriatric care emotionally rewarding, highlighting the emotional approach they take in caring for older adults. This satisfaction stems from the positive outcomes of their care. In Pakistan, the concept of “khidmat” (service), which involves serving the needs of older adults, highlights the emotional satisfaction nurses derive from their patients. (Qureshi, 2014). In Pakistani culture, older adults often express gratitude through blessings and prayers more frequently than other adults, highlighting the significance they attach to the care provided. Therefore, nurses view geriatric care as emotionally rewarding and emphasize the importance of comprehensive care. These perceptions were further supported by enabling factors that facilitate nurses in caring for older adults.
These factors include spirituality, family involvement, and support from the healthcare team. Spiritual satisfaction is a key factor in sustaining the motivation of nurses in caring for older adults. Literature also suggests that spirituality enhances motivation and effectiveness in healthcare settings (Khalaaf et al., 2022). Another study in Pakistan also supported this, stating that spirituality leads to better care performance and increased quality of care (Aron, 2015; Mumtaz, 2017).
Another factor is family member involvement in care, which facilitates nurses by reducing their workload and alleviating the burden on them. Family members assist older patients with daily activities, medication management, self-care, and personal care, thereby reducing the workload of nurses. A study in Pakistan found that family involvement in the care of older adults is a facilitating factor for the continuity of patient care (Khalil & Gul, 2021). Nurses perceive family members as facilitators, as they are involved in their patients’ physical care and play a role in preventing missed nursing care for older patients. This approach reduces the burden of care on nurses and improves patient outcomes.
The last facilitating factor was assistance from their team members and healthcare professionals, as it helped them understand complex geriatric patients with multiple comorbidities, risk of polypharmacy, and cognitive decline, and provided them with the necessary support and understanding through the sharing of evidence-based knowledge and problem-solving skills. Teamwork enhances nursing care and patient outcomes in acute medical settings, as supported by literature, which found that supervisor assistance reduced missed nursing care in geriatric patients (Rezaei-Shahsavarloo et al., 2021). Additionally, another study found that senior colleagues can enhance the learning and clinical training of assigned nurses in older adult care, as they can provide support and assistance due to a lack of clinical competency and knowledge (Markey et al., 2020). Pakistan’s geriatric care is hindered by underdeveloped skills and a lack of specialized education among nurses, necessitating the need for experienced support from the healthcare team.
Despite the enabling factors, nurses face physical and emotional challenges in caring for geriatric patients, including comorbidities, high dependency, communication barriers, non-compliance with medical regimens, and lack of specialized education. Geriatric patients have complex health conditions, often suffering from multiple diseases and comorbidities, and are inclined towards cognitive decline. These comorbidities pose a greater challenge to nurses during the care process. A study revealed that frail older patients with multimorbidity face challenges in physical health, leading to missed nursing care. Another study highlighted that the growing number of elderly patients with multimorbidity poses a significant challenge (Meschi et al., 2016; Rezaei-Shahsavarloo et al., 2021). A Pakistani study found that most geriatric patients are in critical condition due to severe comorbidities and frailty (Mushtaq et al., 2022). Therefore, nurses need to be trained and qualified in geriatrics to provide comprehensive care.
This study also revealed high dependency among geriatric patients, who are primarily dependent on nurses due to their physical status and are dependent on their ADLs, increasing the work burden on the primary nurse. This makes it difficult for nurses to provide timely and adequate care. This finding is consistent with a study that found that high dependency on older patients makes it challenging for nurses to choose this age group for their careers, as geriatric patients are highly care-dependent. This makes geriatric care time-consuming and necessitates a separate specialty and proper staffing ratio to reduce the care burden.
Furthermore, older adult patients are often reluctant with their medical regimen, refusing to take their medications and insisting on taking them at their own pace due to long-term usage of certain medications. They also exert pressure on nurses to allow their family members to visit them, but due to infection control measures, they are not allowed in critical areas. A study reveals that older adult patients often struggle with medication adherence due to inadequate patient education, lower income, and high medication costs (Algameel, 2020). Pakistani literature also revealed low adherence to medication among older adult hypotensive patients, attributed to a lack of health literacy among the geriatric population (Saqlain et al., 2019). Research indicates that medication compliance in the treatment of geriatric patients is a significant challenge, yet this issue is often underrecognized (Smaje et al., 2018). Thus, non-compliance is a big concern for nurses in sustaining the long-term treatment of such patients.
Along with this, therapeutic communication was hindered due to the age gap and cognitive impairments. The communication gap between nurses and patients is a significant challenge, resulting in a lack of understanding and preventing healthcare providers from effectively addressing patients’ concerns. Factors contributing to this gap include issues related to older adult patients’ health, such as hearing problems, irritable behaviors, aging, and dementia, and a low level of understanding, which contribute to the difficulty in communication between nurses and patients (Adibelli & Kılıç, 2013; Park & Song, 2005).
Moreover, due to a lack of specialized education and training, nurses often face difficulties in providing high-quality care for these fragile patients. This finding is supported by nurses who reported that a lack of education and skills hinders their ability to provide care to older adults in critical care units (Heydari et al., 2019). Similarly, another study found that nurses struggle with caring for older patients due to a lack of sufficient knowledge and skills (Adibelli & Kılıç, 2013). In Ethiopia, most nurses have inadequate knowledge and gaps in practice related to geriatric care (Mitike et al., 2023). Similarly, in Pakistan, geriatric nursing is not well-developed, leading to nurses feeling inadequate knowledge.
In contrast, the study found that the physical structure of the ward, including extended distances between patient rooms and nurse stations, significantly impacted the care of older adult patients, leading to missed nurse care and a lack of efficient nursing services (Rezaei-Shahsavarloo et al., 2021). Another study found that a lack of time, patient choice, routine, and resistance to change hinder the quality of care for older adult patients (Murphy, 2007). Nurses in Ghana also perceive the lack of special wards as a challenge to older adult care, as they primarily focus on geriatric care (Salia et al., 2022). In Turkey, administrative problems and a lack of technical equipment were also identified as challenges. The absence of a geriatric care policy, inadequate attention to older adults, insufficient resource allocation, and a lack of equipment such as hearing aids made nursing care for older adult patients complex and challenging (Adibelli & Kılıç, 2013). These factors depend on a country’s economic situation and sociocultural aspects.
To address the above challenges faced by nurses, the following actionable steps are recommended: incorporating a geriatric module into nursing curricula that focuses on comorbidities, such as multimorbidity, polypharmacy, and the high risk of falls, as well as developing communication strategies to improve the quality of care. Secondly, the development and implementation of Frailty Care Bundles (FCBs) for geriatric patients are recommended to address high dependency and frailty, thereby improving the physical status of older adult patients (Naughton et al., 2022). In Pakistan, geriatric nursing and gerontology are underdeveloped; however, research suggests that scaling these fields and establishing special aged care facilities can improve the quality of care (Salia et al., 2022). A separate speciality will enhance nurses’ knowledge in geriatrics, focus on geriatric-centered care, and enhance overall care.
The study suggests that improving geriatric care requires infrastructure improvements and staffing ratios. It recommends separate units with medical devices and equipment for nurses, as well as improved staff ratios. In Iran, inappropriate care environments and high workloads exacerbate missed nursing care (Rezaei-Shahsavarloo et al., 2021).
In the US, nurses struggle to provide comprehensive care due to inadequate structures and low staffing ratios (Lake et al., 2020). Specialized care units, trained healthcare staff, and medical aid devices help overcome these challenges (Hwang & Morrison, 2007).
Limitations and Future Directions
This study has several limitations. First, the study was limited to a single tertiary institution, which restricts the transferability of the findings to other secondary and primary-level institutions. Secondly, the study involved only one male participant, thereby limiting the variability in gender. Lastly, the sample size was 13, although it was supported by thematic saturation; however, this may limit the generalizability of the study to a larger population.
Research on patients’ perspectives and healthcare challenges is limited, prompting nurses and healthcare professionals to conduct further studies on the perspectives of older adults. Patient-centred care policies should be designed to reduce barriers and improve care.
Conclusion
This study examines nurses’ perceptions of geriatric care in Pakistan, revealing that it constitutes a distinct specialty that necessitates a comprehensive approach. It also highlights the emotionally rewarding experience of caring for the elderly. Spirituality, family, and support from the healthcare team motivate nurses in caring for older adults. However, challenges such as comorbidities, high dependency, communication gaps, non-compliance with medical regimes, and lack of specialized education hinder the care of older adult patients. To overcome these issues, nurses propose the establishment of separate specialties and improved infrastructure to enhance the quality of care for older adult patients in Pakistan.
Supplemental Material
sj-docx-1-ggm-10.1177_30495334251382413 – Supplemental material for Unveiling the Perception of Nurses and Challenges to Admitted Geriatric Patients in Pakistan: A Qualitative Explorative Study
Supplemental material, sj-docx-1-ggm-10.1177_30495334251382413 for Unveiling the Perception of Nurses and Challenges to Admitted Geriatric Patients in Pakistan: A Qualitative Explorative Study by Muhammad Shoaib, Khairulnissa Ajani, Amina Huda and Zohra Jetha in Sage Open Aging
Footnotes
Appendix
Interview Question

| What is your opinion/perception regarding geriatric patients? |
| How do you perceive geriatric nursing? |
| Share your experiences in caring for geriatric patients. |
| What are the obstacles and challenges in caring for geriatric patients? |
| What are the facilitating factors in caring for geriatric patients? |
| What type of resources and facilities could help you in this situation? |
| Would you like to provide any additional information regarding older adult patients? |
Ethical Considerations
IRB protocol/Human Subjects Approval Numbers: 2023-8391-24147.
Author Contributions
Muhammad Shoaib conceptualized the study, conducted the data analysis, and wrote the paper. Dr. Khairulnissa Ajani directed and supervised the data analysis and reviewed and revised the manuscript. Amina Huda and Zohra Jetha co-supervised data and reviewed the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors received only financial support for the research from the School of Nursing and Midwifery Graduate Office at Aga Khan University.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The authors confirm that the data supporting this study’s findings are available within the articles with DOI (https://doi.org/10.3889/oamjms.2019.846) and (![]() ). However, the nurses’ perceptions regarding geriatric care findings are newly generated, and no exact study findings support this.
). However, the nurses’ perceptions regarding geriatric care findings are newly generated, and no exact study findings support this.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.