
Abstract
Coping is defined as cognitive and behavioral effort to manage specific external and/or internal demands, such as managing one’s own fall risk. Little is known about the relationship between the risk of falling in older adults and their coping strategies. The purpose of this study is to examine the fall risk after hospitalization, the adequacy of self-perceived fall risk and coping strategies of older adults. In this mixed-methods study, the adequacy of perceived fall risk was determined using the de Morton Mobility Index and the ABC Scale in 98 geriatric patients recruited in a geriatric hospital. Semi-structured interviews were conducted with a subsample of 16 participants 6 months after discharge to identify coping strategies. The six interviewees who adequately assessed their fall risk reported active/positive coping. In contrast, participants who assessed their fall risk inadequately (10 out of 16) reported passive/negative coping. Older adults who inadequately assessed their fall risk need special accompaniment in geriatric wards to develop active/positive coping strategies.
What This Paper Adds
Older adults show active/positive or passive/negative coping strategies.
Older adults who adequately self-assess their own fall risk show only positive coping strategies.
Application of Study Findings
Coping strategies and the adequacy of the self-perceived fall risk should be observed in studies on older adults and/or geriatric patients in studies on fall risks and fear of falling
The results of this study enables scientists to plan and conduct future studies on fall risks in older people that include coping mechanisms and self-assessments of the risk of falling.
Introduction and Background
Older adults are exposed to an increased fall risk (FR) because of a variety of physiological and functional changes that occur with age, such as fading of muscle power, reduction in posture control and visual impairment (Ehrlich et al., 2019; Pua et al., 2017; Yeung et al., 2019). An increased FR, however, is not only associated with subsequent falls and fall-related injuries (Barbosa Pena et al., 2019; Gazibara et al., 2017), but also with reduced physical activities, social isolation (Barbosa Pena et al., 2019), psychological effects, fear of falling (Hughes et al., 2015). These factors results in the need for—and are subsequently modulated by—coping strategies that are developed in response to these risks by each individual (Young & Williams, 2015). The concept of coping was defined by Lazarus et al. as part of his appraisal theory and transactional model of stress and coping (Lazarus & Folkman, 1984). Lazarus (1993) postulated that the term coping is independent of attributes such as adaptive/non-adaptive, successful/unsuccessful, or stable/variable.
As stated by different authors, older adults do not always have an adequate perception of their own FR but instead a diverging perception of their FR from an objective FR assessment (Delbaere et al., 2010; Fortinsky et al., 2009; Kiselev et al., 2017). Using the Morse Fall Scale and Falls Efficacy Scale-International, Lim et al. (2018) described a ratio of one-third adequate self-assessing older adults to two-thirds inadequate self-assessing older adults.
There is a lack of studies investigating the underlying reasons in coping behavior or consequences of this inadequacy. In this study, we use the assumption of Lazarus as a basis. Among the first to examine a potential relationship between coping and older adults self-assessed risk of falling were Høst et al. In 2011, Høst et al. examined the relationship between adequate assessing FR and accompanied coping strategies of older adults. They identified active and passive coping strategies of older adults, with their aim of avoiding falls in the future.
The present study therefore aims to identify: (a) self-assessed fall risk by adults, (b) adequacy of self-assessed fall risk, and (c) coping of fall risk of older adults.
Methods
Study Design and Investigation Methods
This study was conducted with a subsample of participants out of a larger data set (N = 98) described by Brodowsky et al. (2022) (Supplemental Data 1) and applied as a sequential mixed-method design in two parts.
The study was assessed, positively evaluated, and approved by the responsible ethics committee (Ethics Committee of Charité—Universitätsmedizin Berlin, Number EA4/012/16) on March 16, 2016, prior to commencement. In this study, participants took part under the condition of written informed consent.
The two parts of our study were as follows:
(a) Mobility tests carried out immediately before participants were discharged from a geriatric hospital (t1) and 6 months after discharge (t2) (quantitative)
(b) Interviews were conducted 6 months after hospitalization (t2) (qualitative)
Setting and Participants
Participants were recruited consecutively in a geriatric hospital. In Germany, a geriatric hospital is a specialist inpatient facility for geriatric medicine, in which adults over the age of 65 receive nursing care, medical and therapeutic treatment after an acute deterioration in their health due to illness or accident, such as a falls. The standard treatment duration is 2 to 4 weeks.
All participants provided informed written consent.
Inclusion Criteria
Inclusion criteria were defined as follows: an age of 65 years and older, an expected ability to walk (with or without assistive device and without the assistance of another person), and climb stairs with full weight bearing during the hospital stay, sufficient vision to complete a questionnaire and ability to consent. Exclusion criteria were defined as severe cognitive impairment (Mini Mental State Examination <24), severe heart failure or peripheral artery disease. The latter two criteria were defined participants with such ailments were not expected to be able to complete the functional assessment battery.
Data Collection
Data Collection: Quantitative Data
Participants were recruited face-to-face within the first 5 days after admittance to hospital. An extensive test battery was applied, including the use of walking aids, fall history and their physiological and psychological consequences, muscle strength, functional mobility assessments and questionnaires on fear of falling.
Two assessments from this test battery were relevant for the current research question: the Activities-specific Balance Confidence Scale (ABC Scale) (Powell & Myers, 1995) and the de Morton Mobility Index (DEMMI) (de Morton et al., 2011). Both measurements were applied twice: Within 3 days before discharge (t1)—to insure that participants required a high functional level after their hospital and rehabilitation stay—and 6 months after discharge (t2).
The ABC Scale captures the subjective confidence to maintain balance without staggering during 16 everyday defined activities (Friedman et al., 2002). The question for the stair climbing example is “How confident are you that you can maintain your balance or not falter when you walk up and down stairs?” The validated german version of the ABC Scale was used (Schott, 2008). While the original scale evaluates the individual items on a scale between 0 and 100 points, the present study used a Likert-scale version with each item being answered on a scale between 0 and 3 points and an overall score between 0 and 48 points. The ABC Scale shows a high test reliability (Myers et al., 1998) and good discriminant and convergent validity (Powell & Myers, 1995). A cutoff value of less than 67% of the maximum score identifies subjects with an increased FR (Lajoie & Gallagher, 2004).
The DEMMI was developed as a measurement tool of general mobility of institutionalized older adults (de Morton et al., 2008). The addition of all 15 item ratings gives a raw score with a range of 0 to 18, which is transformed into a score with a range of 0 to 100. Zero indicates the lowest and 100 the highest general mobility. The DEMMI has shown high criterion validity and reliability in comparison with other instruments that measure mobility in inpatient geriatric settings and in patients who are making the transition from hospital to the community (de Morton et al., 2011; de Morton & Lane, 2010). In the current study, the Median of the DEMMI was used as cutoff to assign the participants into a group with lower and a group with higher fall risk.
Data Collection: Qualitative Data
The qualitative approach was conducted according to the consolidated criteria for reporting qualitative research (COREQ) checklist (Tong et al., 2007). An interview guide was pretested by the author and two older adults staying at geriatric hospitals. After pretests subsidiary questions were modified (e.g., “What paths do you take in your home?” to “What are typical appointments and activities?”). The semi-structured interview guide was used to provide insights in older adults’ coping strategies. Interviews were conducted 6 months after discharge at the older adults’ homes/residencies with the second ABC and DEMMI at the same appointment (t2). The content of the interviews were topics of current mobility, changes since fall events and coping with fall risk and mobility limitations. All interviews were conducted face-to-face by the same researcher.
All participants were asked consecutively by phone to take part in the qualitative part by being interviewed. The participants who consented to the interviews comprise the study population considered here.
Analysis
Data Analysis: Quantitative Data
SPSS Version 25 (Armonk, NY: IBM Corp.) was used for analyzing all data.
First, scores of mobility abilities (DEMMI) (t1 and t2) were compared. Second, results from the self-perceived FR via ABC Scale and the objective FR via DEMMI were inserted into a 4 × 4 contingency table to display the frequency distribution. The self-assessment was deemed “adequate” if both objective and subjective FR were either positive or negative. Divergences from the concurrent results of the two assessments were deemed “inadequate.”
Data Analysis: Qualitative Data
All 16 audio recorded interviews were transcribed literally by trained personnel and transcription guideline. The qualitative analysis and research software Atlas.ti 8.0 (Berlin, Germany: ATLAS.ti Scientific Software Development GmbH) was used to analyze data. Qualitative content analysis was performed according to Mayring (2010) by two researchers experienced in analyzing qualitative data. A coding manual that included definition of categories, anchor examples, and coding rules was applied. The number of interviewed participants was based on the principle of theoretical saturation (Glaser & Strauss, 1967/1998).
Results
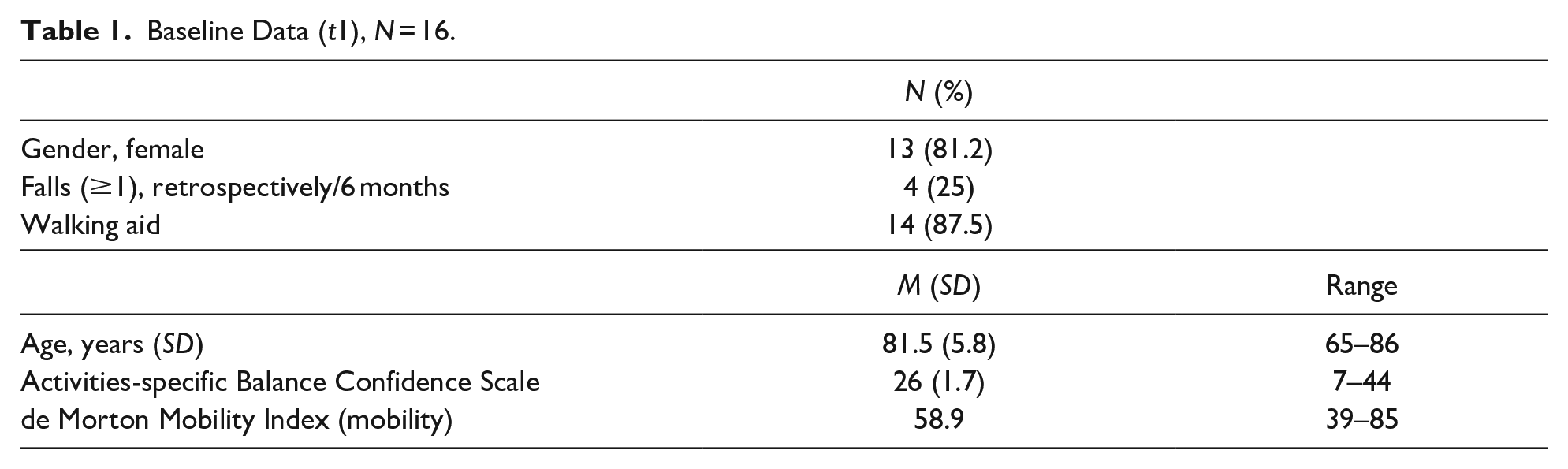
At t1, quantitative data from 98 participants (cohort study) were collected. Of these participants with baseline data, 16 older adults were interviewed (Table 1). The interviewees (female n = 13, 81.2%) demonstrated comparable characteristics to the cohort of 98 participants (female n = 67, 68%) in terms of gender ratio, age, median of DEMMI, and median of the ABC scale (Supplement 1: Results of total cohort).
Baseline Data (t1), N = 16.
Identified Self-Assessed Adequacy of Fall Risk
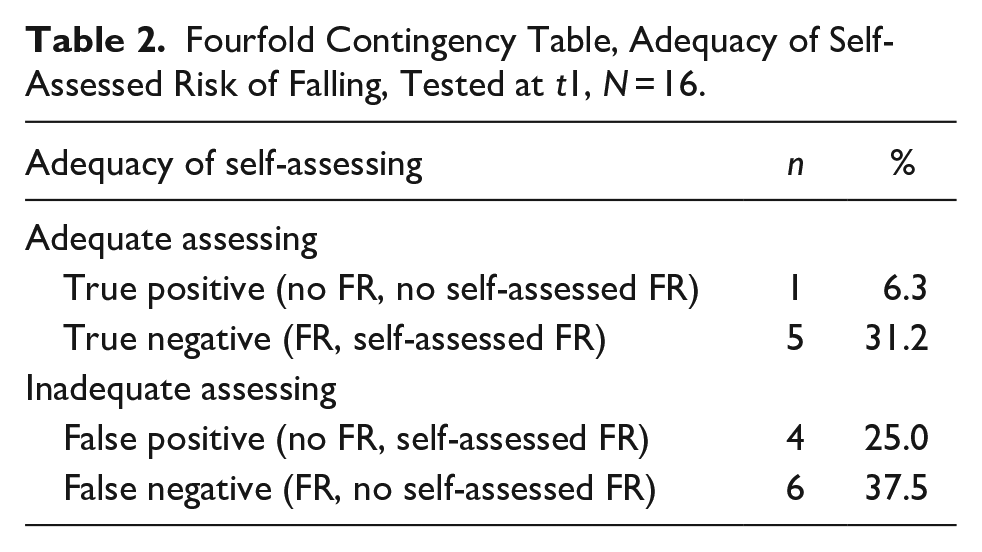
Based on the cutoff categorization (DEMMI, M = 58.9) the results of FR and self-assessed FR were analyzed in a fourfold contingency table. Out of 16 interviewed older adults, six (37.5%) adequately assessed their own FR at t1, either having no FR and no self-assessed FR (n = 1) or showing FR and self-assessed FR (n = 5). Of those inadequately assessing their FR (62.5%), six participants with FR reported no self-assessed FR, while others (n = 4) demonstrated no FR but self-assessed FR (Table 2). Of the 10 participants who inadequately assessed (62.5%) their own FR, six considered a risk of falling without objective mobility impairment, whereas four participants perceived their FR to be lower than objectively assessed.
Fourfold Contingency Table, Adequacy of Self-Assessed Risk of Falling, Tested at t1, N = 16.
Identified Coping Strategies
Based on the 16 interviews, the identified coping strategies could be divided into subcategories that were either active and positively connoted, or passive and negatively (Table 3).
Identified Categories and Subcategories, Tested at t2, N = 16.

Twelve out of the 16 interviewees reported active/positive coping. Statements such as “well, every morning before I get up, i.e., still in bed, I raise my legs 100 times. . .” (123) and “could have been worse, I think. That I was ending up in a wheelchair or something like that. I should be happy” (042) demonstrated a positive attitude to the challenge of their own FR or reduced state of health after hospitalization. This positive attitude was also reflected in a reported physical activity in daily life. This was shown by statements like “after all, I’m still on the move because I go out every day” (042).
Four older adults demonstrated passive/negative coping. An example of passive coping was the statement “well, I’m not even thinking about falling down right now” (026). An example of passive/negative coping was “but I don’t know how it is going to be. You can only pray every day that you will feel better” (079). From these interviews, we extracted subcategories such as the lack of prospects or low self-efficacy.
After completing and analyzing the 16th interview, due to theoretical saturation according to Glaser and Strauss was reached (Glaser & Strauss, 1967/1998). Therefore, no further interviews were performed.
Coping Strategies and Identified Self-Assessed Adequacy of Fall Risk
Merging qualitative and quantitative data none of the adequate self-assessing participants showed passive coping strategies (Figure 1).
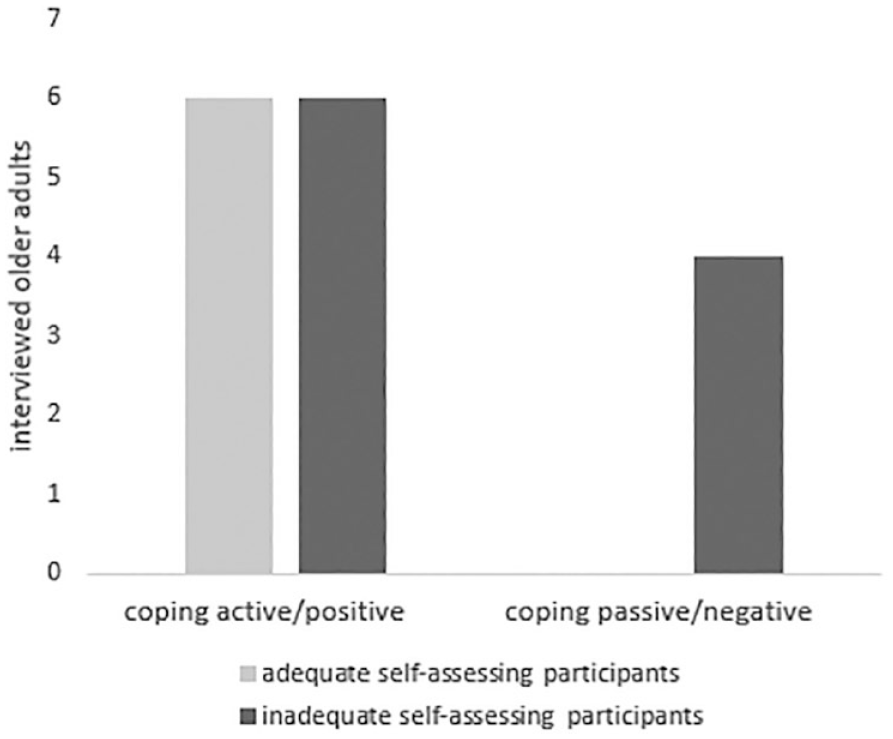
Adequacy of self-assessed risk of falling and characteristics of coping strategies, N = 16.
Discussion
Within our study, more than half of the participants interviewed did not adequately self-assess their individual FR. This high number corresponds with findings reported in other publications (Delbaere et al., 2004; Fortinsky et al., 2009; Kiselev et al., 2017; Lim et al., 2018). Fortinsky et al. reported an overconfidence between 26% and 42% of sample members. Overconfidence was defined as a high (balance) confidence and high fall risk. Similar to our study, 37.5% of older adults assessed their fall risk inadequately (existing fall risk and no self-perceived fall risk). Inadequate self-assessment of fall risk potentially leads to an insufficient coping behavior. Underestimating one’s own fall risk could lead to a higher risk exposition and, consequently, to higher fall incidence while overestimating his/her own fall risk could lead to activity restrictions and less social interaction. One result of our interviews was that an adequate coping strategy regarding their fall risk resulted in a more active lifestyle. While these results cannot be generalized due to the qualitative nature of our data, they still point to the importance of an adequate self-assessment of the risk of falling (or lack thereof) in order to draw adequate conclusions (in the form of a coping strategy) that enables older people to stay active. If our findings are confirmed in larger studies, it would highlight the importance of assessing the adequacy of subjective fall risk as a prerequisite to offer interventions to develop positive coping strategies that keep older adults active and safe.
The identified coping strategies in this study corresponded with the findings of Høst et al. (2011), suggesting there are active and passive coping strategies to counter FR. Some literature addresses coping strategies for risk of falling like WHO Europe (Health Evidence Network, 2004). Nevertheless, little is known about the characteristics of coping strategies. In our analysis, we found that an adequate self-assessment of FR, irrespective of whether it’s low or high fall risk, is exclusively accompanied by active/positive coping strategies. This finding, if confirmed by larger studies with a robust study design, should help health professionals to expand their therapy strategies by including the actual coping strategies of their patients. One possible hypothesis is that, by including a focus on the self-assessed FR and fear of falling with the aim of patients assessing themselves adequately would, in turn, lead to active coping. Another hypothesis is that by helping patients to manage the demands of their daily life, providing social support, and to offer instrumental support, patients can be supported in changing their perspective on their situation regarding their risk of falling and, consequently, raises their level of physical activity (positive reframing). For testing this second hypothesis, clinicians should assist patients to find their individual active/positive coping strategies as well as implementing these strategies into their daily routines. In turn, this will lead to adequate self-assessment of FR. We are aware that have an element of a “chicken-egg-debate,” (what comes first and which aspect affects the other). However, we prefer, on the basis of the construct of proactive coping (Schwarzer & Taubert, 2002) to test the second hypothesis, which should be implemented in future longitudinal studies.
Limitations
As this study was conducted with an explorative character on quantitative data and small sample size due to qualitative data, our results cannot be generalized. Additionally, while we used the ABC-Scale with the emphasis of evaluating the adequacy/non-adequacy of the self-perceived FR of older people in comparison to an objective FR-assessment. However, the ABC-Scale and, by extension, no other assessment for measuring Fear of falling or balance confidence have been validated for that purpose. While the face validity for its use in this context is high, the need for a thorough validation of the ABC-Scale for the use in this context is obvious. Therefore, more research is needed in order to gain (a) a better understanding on how active/positive coping strategies are developed by older adults with FR; (b) how this development can be facilitated in any kind of intervention to lower FR in older adults; and (c) to validate existing scales or developing new ones to measure the adequacy of a patients’ self-perceived fall risk.
Conclusion
We conclude that older adults who inadequately self-assess their fall risk need to be identified as well as accompanied in geriatric wards to develop active/positive coping strategies. Long-term studies are needed, as further consequences for inadequately assessing older adults are still unknown.
Morbidity and long-term consequences for activities and participation of inadequate self-assessment of FR should be investigated further.
Supplemental Material
sj-docx-1-ggm-10.1177_23337214231152700 – Supplemental material for Fall Risk and Coping of Older Adults After Hospitalization: A Mixed Methods Study
Supplemental material, sj-docx-1-ggm-10.1177_23337214231152700 for Fall Risk and Coping of Older Adults After Hospitalization: A Mixed Methods Study by Nicole Strutz, Hanna Brodowski, Sandra Angelika Mümken, Ursula Müller-Werdan and Joern Kiselev in Gerontology and Geriatric Medicine
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The study was assessed, positively evaluated and approved by the responsible ethics committee (Ethics Committee of Charité—Universitätsmedizin Berlin, Number EA4/012/16) on March 16, 2016, prior to commencement. In this study human participants were included, who took part under the condition of written informed consent.
Trial Registration
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.