
Abstract
This study explored the perspectives of family caregivers of older adults with hypertension and/or diabetes mellitus on the care provided to their kin when they visit the hospital. A qualitative research approach was used to conduct the study using family members providing informal care for older adults with hypertension and/or diabetes mellitus at a teaching hospital in Ghana. A total of 20 participants were purposively sampled, interviewed, and data was analyzed using reflexive thematic analysis. Family caregivers mainly had perceptions that their older adult kin had poor interactions with the healthcare system because of some healthcare workers’ negative attitudes, inadequate facilities at the clinics, and lack of geriatric care services at the facility. This notwithstanding, family caregivers also derived some benefits from accompanying their kin to the hospital. Practice and education in gerontological nursing must be employed to pragmatically meet the unique healthcare needs of older adults in Ghana with a focus on geriatrics units and standalone programs of study to prepare specialized healthcare professionals to provide comprehensive services to older adults. For a thorough understanding of issues of older adult care in the country, their perspectives on this subject should also be explored in future studies.
Introduction
Several obstacles hinder good healthcare provision to older adults (60-year-old-and-above) amid increasing complexities in their care globally. Key among them are perceived organizational barriers and lack of professional expertise (Agyemang-Duah & Rosenberg, 2023; Feng et al., 2020; van de Pol et al., 2015; Wilson et al., 2021). There are reported negative experiences with clinical follow-ups such as prolonged waiting times, ineffective consultations, and impatient healthcare providers in many studies (Agyemang-Duah & Rosenberg, 2023; English et al., 2022; Perry, 2020; Wong et al., 2011).
The presence of a chronic illness in the life of an individual has significant effects on both the individual and his or her family physically, psychologically, and socially because of their increased dependence on the healthcare system (Ayvat & Atli Ozbas, 2023; Jaarsma et al., 2017). Caregivers have been reported to help with activities such as handling challenges related to feeding, assisting with mobility, and keeping medical appointments (Faronbi et al., 2019). Family caregivers have been viewed as not having the required knowledge and time to provide care and, as a result, they are marginalized by formal health workers (Abigail Reid et al., 2023; National Academies of Sciences, Engineering and Medicine, 2016). Communication breakdowns, difficult-to-access healthcare facilities, and poorly trained healthcare personnel have also been reported as gaps in the care of older adults (Motsohi et al., 2020). Similar findings have been reported in Ghana to establish the burden for family caregivers of older adults (Agyapomah et al., 2023; Agyemang-Duah et al., 2020, 2024; Kyei-Arthur et al., 2022; Kyei-Arthur & Codjoe, 2021). However, none of these studies qualitatively focused on the perspectives of family caregivers on the care provided to older adults when they assist them in seeking healthcare in a hospital setting.
Ghana’s healthcare system comprises public, private, and traditional healthcare providers. Public hospitals and clinics are generally affordable but often face challenges like limited resources and equipment, and a shortage of medical staff and specialists leading to prolonged waiting times (Amoah et al., 2021)
To the best of our knowledge, this study is the first of its kind to qualitatively explore the perspectives of family caregivers of older adults with hypertension and/or diabetes mellitus on the care provided to their kin when they navigate the healthcare system in the country. The study backs the expansion of research that focuses on the care of older adults paving the way for future research, not only on the interactions of caregivers of older adults with the health system in Ghana, but also on different care activities undertaken by family caregivers and the burden of care in the country.
Methodology
Study Design
A qualitative research approach to explore how family caregivers of older adults living with hypertension and/or diabetes mellitus perceive the interactions between their kin and the healthcare system in Ghana was used (Amos, 2016; Ganapathy, 2016; LoBiondo-Wood & Haber, 2014).
Research Team and Reflexivity
EAB (Senior Lecturer) and RA (Principal Health Tutor) reviewed the literature and conceived the study. EAB, RA, IA (Senior Lecturer), VMD (Associate Professor), and LOP (Registered Nurse) were involved in protocol development, gaining ethical approval, recruitment and data analysis. No participant had prior knowledge of any of the authors. The assumptions of the researchers going into the study were that family caregivers of older adults play a significant role in ensuring the general well-being of the older adult.
Study Population and Setting
The study was conducted in the hypertension and diabetes clinics of a large teaching hospital in Ghana and comprised family caregivers (aged 18 years and older) providing care for older people with hypertension and/or diabetes mellitus. The age of “60 years” has been adopted by the central government as the age of retirement, hence the benchmark for defining an older adult in Ghana (Braimah & Rosenberg, 2021).
Sampling
A purposive sampling method was used to select participants who could provide in-depth information about their experiences (Setia, 2017). It is described as the careful selection of a participant based on specific characteristics of the participant (McCrae & Purssell, 2016; Sharma, 2017; Taherdoost, 2016). This ensures focus on participants with specific features who will better assist with achieving the objectives of the research (Etikan et al., 2016). Older adults receiving care at the clinics were asked to identify their family caregivers who mostly accompany them to the health facility as is the common practice in many African countries (Given et al., 2012; Oyegbile & Brysiewicz, 2017). The sample size of 20 participants was informed by data saturation. Saturation is reached when the researcher is not getting any new theme arising from the data collected at a point in time (Saunders et al., 2018).
Family caregivers of older adults with either hypertension, diabetes mellitus or both who were 18 years old and above and were fluent in either English or Twi language were included. The older adult should have been diagnosed with and managed for either hypertension or diabetes mellitus for, at least, 1 year before the study. We excluded family caregivers who had provided care to the older adult for less than a year to ensure that they had assisted them in seeking care at the hospital on numerous occasions.
Data Collection
Data were collected in the offices assigned at the clinics. Semi-structured individual interviews were conducted using an interview guide and this allowed an in-depth exploration of family caregivers’ experiences (LoBiondo-Wood & Haber, 2017). Some of the questions that were on the interview guide include the following:
“What has your interaction with nurses and other healthcare providers been like, when taking care of older adults with hypertension and/or diabetes mellitus?”
“What services would make your role more efficient?”
Each interview session was audio-recorded with permission from participants and transcribed verbatim thereafter (Moser & Korstjens, 2018; Roulston & Choi, 2018). Eleven interviews were conducted in Twi while the remaining nine were conducted in the English language, based on the preference of each participant. EAB and RA who are both fluent in the Twi language listened to the recorded interviews in Twi and transcribed them in English. A certified English language teacher confirmed the accuracy of each translated transcript. Participants were compensated with a token of GHC 10.00 worth of airtime credit (about USD 0.75) of their preferred mobile phone network.
Data Analysis
Data collection and initial analysis took place simultaneously between June and July 2020, after which data analysis continued. Reflexive thematic analysis was used for the data analysis (Braun & Clarke, 2022; Byrne, 2022). This required first becoming familiar with the data through the transcribing process, and further reading each transcript and taking notes. Initial codes were then assigned to the data to describe the content. A search for patterns in the codes across the different interviews followed afterward. This was led by the principal investigator. All authors met regularly to review the themes that were generated. Lastly, a report using quotes from participants was written. We frequently revised and expanded our coding process during the data collection and analysis periods (Ganapathy, 2016; Moser & Korstjens, 2018). We managed the data with NVivo version 12.
Trustworthiness
The criteria of confirmability, credibility, dependability, and transferability as proposed by Lincoln and Guba (1986) were used to enhance the trustworthiness of the study (Nowell et al., 2017; Pyo et al., 2023). There were regular discussions among all authors to review themes that were generated from the data analysis to ensure credibility and confirmability (Birt et al., 2016; Candela, 2019; Gunawan, 2015). Thus, the study utilized the diverse experiences and perspectives of all authors to review decisions regarding sampling, data collection methods, and peer-reviewed data analysis (Nowell et al., 2017; Stahl & King, 2020). The systems put in place to safeguard credibility also warranted dependability (McInnes et al., 2017). To enhance transferability, an elaborate description of the study participants, setting, and processes has been given (Korstjens & Moser, 2018).
Findings
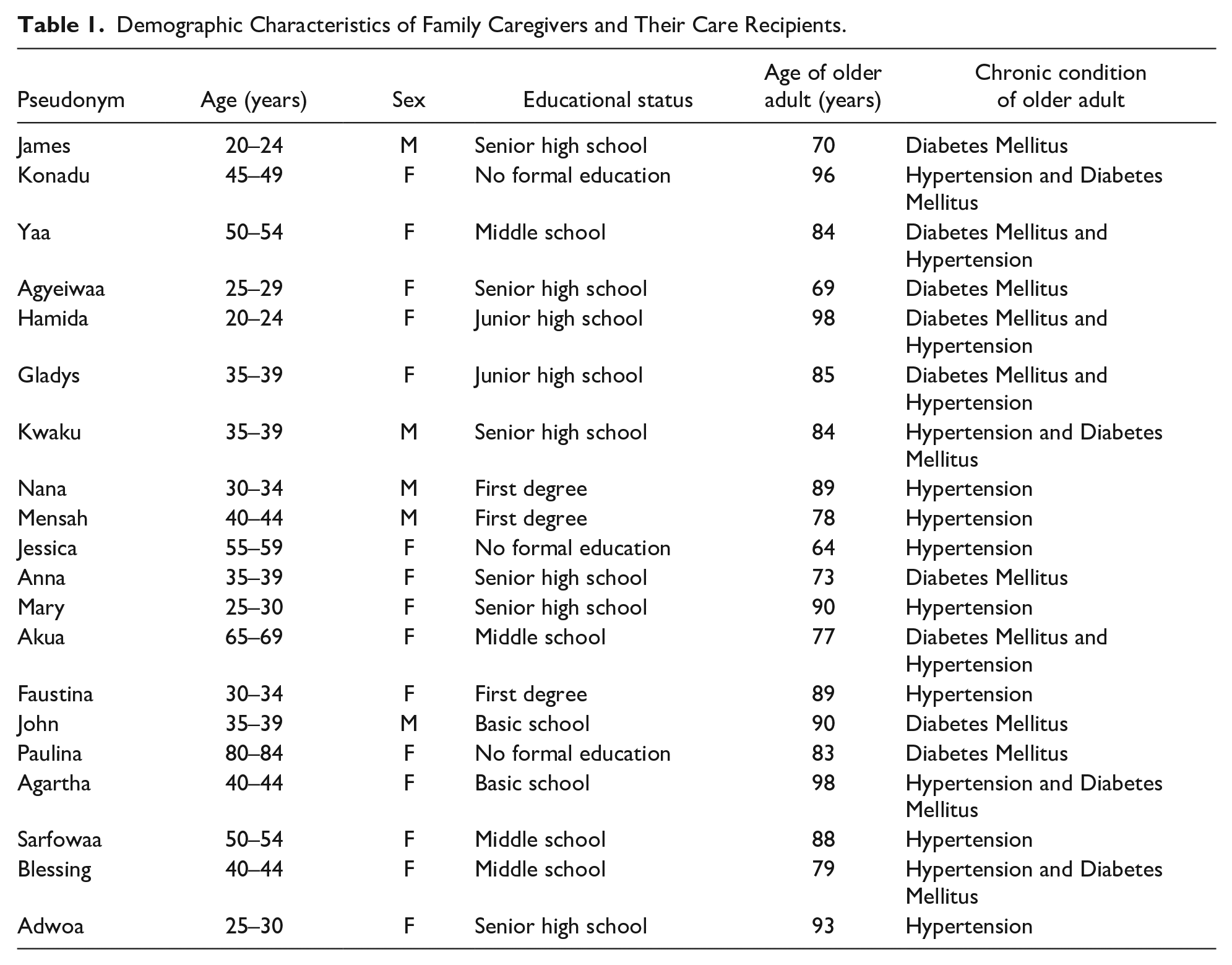
There were 20 participants involved in this study, of whom 15 were women while the remaining five were men. For the older adults receiving care, seven were living with hypertension only, five with diabetes mellitus only, and eight with both hypertension and diabetes mellitus. A summary of these has been provided in Table 1.
Demographic Characteristics of Family Caregivers and Their Care Recipients.
Themes and Sub-themes
Three main themes and six sub-themes were generated from the analysis of data for this study. A summary of these has been provided in Table 2 with relevant participant quotes to support the interpretations.
List of Themes and Sub-themes.

Theme 1: Interactions With the Healthcare System
This theme described the day-to-day experiences of participants when they visited the healthcare facility with their care recipient and comprised two sub-themes—attitude of healthcare workers and available resources.
Subtheme 1: Attitude of Health Workers
The attitude of healthcare workers described how healthcare workers responded to the needs of caregivers. It was considered good or bad depending on the kind of interactions that participants and their care recipients had with healthcare workers. Some participants described the attitude of healthcare workers as very professional, explaining that they were very polite and patient with them.
“Some of the nurses are very supportive and considerate. They will move their machines to where my mother is sitting because she has a challenge moving easily” (Sarfowaa)
However, some participants described the attitude of some healthcare workers as poor and cited incidents that suggested inattentiveness, and disregard from the healthcare workers.
“Instead of paying attention to the work they are doing, all they do is to sit there and talk.” (Akua)
“You will always feel sorry for the kind of reply you will receive from them when you need clarification about one thing or the other.” (Anna)
Subtheme 2: Available Resources
Most of the participants described the available resources at the clinic such as space, chairs, and equipment used by the healthcare workers as inadequate, creating avoidable congestion at the clinic.
“When we come here, we don’t even get a place to sit.” (Jessica)
“When you come, you would have to stand because there are not enough chairs.” (Nana)
Participants reported that making plans to adjust to the challenges posed by inadequate resources at the clinic had concomitant issues and was deemed highly distressing. For instance, those who are scheduled to attend the clinics on a particular day are not given time for an appointment—they are seen on a first-come-first-served basis. Participants and their care recipients, therefore, had to leave their homes very early to arrive at the clinic early even though the clinic runs in the afternoon. There was also the possibility that prescribed medications would not be served at the pharmacy before leaving the clinic as they would have to join another long queue for that.
“If you do not come early, you are sure to leave after 6:00 pm. In addition to leaving very late, you might would have to go home and come another day for the drugs to be served to you.” (Mensah)
Some of the participants reported few consulting rooms, with few consultants attending to a larger patient population per visit which significantly contributed to the long queues and waiting times experienced with each visit. They, thus, avoided scheduling any other activity on the day of their clinic attendance.
“They don’t have enough space and the doctors are not many. I have never seen more than 3 consulting rooms working at a time.” (John)
Theme 2: Expectations of Caregivers
This theme described the various expectations that caregivers had while using the health facility, for themselves and their care recipients. Two sub-themes generated from the data concerning this theme were financial support from the government and geriatric care services as discuss below.
Subtheme 1: Financial Support From the Government
Some of the participants expressed the desire to be supported by the government financially, Alternatively, they would appreciate having the cost of some services provided at the clinic borne by the government as a way of providing further relief.
“Financially if the government could relieve us of the burden of paying for certain services. They are not working and are not able to afford some things.” (Akua)
Subtheme 2: Geriatric Care Services
Some of the participants expressed their desire for home care services, nursing homes, special days for health education and preferential treatment for older adults with hypertension and/or diabetes mellitus to lighten some of the burden of caregiving on them.
“I remember having beneficial home care services for my mother when she experienced a mild stroke some time ago.” (Agartha)
Some of the participants also felt that having a separate clinic day for older adults and not mixing them up with the general population could be instrumental in ensuring that the older adult population received appropriate care.
“If older adults were treated separately from those who were below 60 years old, I feel it would be very helpful for such older adults and even those who come with their caregivers.” (Gladys)
Some of the participants explained the need for education on how to manage the disease conditions of older adults. They felt that the short health education sessions by the nurses and, sometimes, the dieticians were not enough for them to provide the needed care to older adults with hypertension and/or diabetes mellitus to prevent the development of complications.
“It would have been best if you could set aside a day other than the review date so that we can come only to be educated about the condition.” (James)
Theme 3: Benefits of Accompanying Care Recipient
Some participants reported that they had learned a lot about hypertension and diabetes mellitus. Their familiarity with these conditions made some of them more conscious of their lifestyle choices and also learned that punctuality at the clinic yielded positive prognoses.
Subtheme 1: Caregiver Becoming Conscious of Personal Lifestyle
Except for one who did not have a history of hypertension or diabetes mellitus in their family, all other participants had a history of either hypertension, diabetes mellitus, or both in their family. Most of the participants reported that they had become more conscious of their lifestyle choices as a result of their caregiving experiences. These included adhering to some of the food restrictions that had been prescribed for their care recipients at the clinic.
“Because of my father’s condition, my eating habits have changed. . .I eat less sugar and starchy foods.” (Anna)
Subtheme 2: Adherence to Treatment Yields Positive Results
Some participants reported that they were happy to ensure punctuality at hospital appointments and adherence to the treatment regimen as these had led to significant improvements in the condition of their care recipients.
“We are very punctual at the clinic. The food restrictions too, we follow strictly. Taking the drugs accordingly and so now we can see a massive improvement in his condition.” (Anna).
A participant reported that his father was almost always on hospital admission previously because he missed a lot of his clinic appointments. However, since he started attending the clinic with him, ensuring all clinic appointments were honored, there has been a significant improvement in his father’s condition.
“I don’t remember the last time he came on [hospital] admission.” (Mensah)
Discussion
Both formal and family caregivers are beneficial to each other in the care of older adults living with various chronic diseases (Kemp et al., 2013; Pristavec & Luth, 2020). To prevent caregiver burden, family caregivers need support from healthcare workers, especially regarding information sharing (Lilleheie et al., 2020; Rodger et al., 2015; Willemse et al., 2016). This is the first study to report on the perspectives of family caregivers on healthcare services provided to older adults with hypertension and/or diabetes mellitus in Ghana. While some of the findings have been reported in other places, it is noteworthy that this study adds to the existing literature on the need to provide specialist services to older adults in Africa. In this study, participants’ descriptions of their experiences while navigating the healthcare system with their care recipients were mostly worrying. Participants were frustrated by the negative attitudes of some healthcare workers as well as inadequate chairs to sit on during their interactions.
It is believed that some healthcare workers have compromised the health of some older adults due to their lack of expertise in dealing with their complex healthcare needs resulting from one or more chronic diseases (Brémault-Phillips et al., 2016; van de Pol et al., 2015). Our participants believed that some healthcare workers were unprofessional in their interactions with them. Deliberate efforts to train healthcare workers on issues related to aging could positively influence the care of older adults in Ghana ensuring improved attitudes toward their care.
Prolonged waiting times and crowded clinic days were reported by our participants as worrisome anytime they came for follow-up visits and treatment. Wong et al. (2011) reported on older adults with diabetes mellitus, also highlighting prolonged waiting times for consultations and medication dispensing at the clinic as worrisome. The implementation of WHO execution of systems for long-term care is highly necessary. With an improved infrastructure, family caregivers and older adults could feel comfortable attending the clinic. Emphasis on building age-friendly environments as well as improving frameworks for delivering long-term care is one of WHO’s five priority areas for action toward safe aging (World Health Organization, 2017). These initiatives could be implemented in the country to improve the care older adults and their family caregivers receive.
There is a limited scope of the nation’s retirement income security system for older adults, and this presents an actual financial hardship for their family caregivers (Agyemang-Duah et al., 2019, 2020, 2024; Kpessa-Whyte, 2018). It is, therefore, not surprising that there were genuine calls for financial support from the government by some of our participants.
Participants preferred the isolation of older adults from the general adult populations at the hospital to allow for preferential treatment. As opposed to treating older patients in conventional general units, dedicated geriatrics units have better-quality results (Flood & Allen, 2013; Magalhães et al., 2023). Declined hospital readmissions, improved functional capacity of older adults and minimum general cost of healthcare has been reported (Fox et al., 2012; Tun et al., 2021). Specialized geriatric units have a lot to add to the care of older adults, but these specialized services for them in Africa are limited (Akoria, 2016). It must also be noted that setting up geriatric units requires geriatric professionals which, at the moment in the country’s healthcare system, are lacking (Essuman et al., 2019; Magalhães et al., 2023). There is no evidence of standalone programs in gerontological nursing in the health training institutions in the country. It is concerning that Ghana is advancing in other specialty areas yet, seemingly neglecting gerontology given that there is an urgency to meet the unique needs of older adults and their family caregivers in the country.
Our study is the first to report on the benefits that family caregivers reportedly derive from accompanying their older adult kin to the hospital for the management of hypertension and/or diabetes mellitus. Indeed, these experiences reinforce their awareness of the relevance of lifestyle choices in protecting them from hypertension and/or diabetes mellitus in the future while having first-hand experience of the benefits of following prescribed regimens for long-term conditions.
Implications for Policy, Practice, and Future Research
Home visits should be part of the plan of care for older adults to have adequate time for the family to know their problems and offer solutions appropriate to their needs. Establishing geriatrics units will provide exclusive services to older adults and their family caregivers and avoid prolonged waiting times. This will be successful when more healthcare professionals receive specialist training in gerontology. Studies that focus on the perspectives of older adults with hypertension and/or diabetes mellitus on this subject will ensure a thorough understanding of issues of older adult care in the country. Quantitative approaches could also be utilized to add to the perspectives from a larger sample.
Strengths and Limitation of the Study
This study has provided a comprehensive account of the perspectives of family caregivers through the adoption of a qualitative approach. The use of reflexive thematic analysis also ensured that concepts were adequately explored in the analysis process and further data generation. While comprehensive accounts of the family caregivers have been provided, exploring perspectives of the older adults themselves and the healthcare providers would have potentially provided more insightful accounts. Studies involving these two groups will be highly instrumental in developing geriatrics services in the country.
Conclusion
Most of our participants’ interactions with the healthcare system were deemed worrying and they desired better services as they depended on it to give the required assistance to older adults with hypertension and/or diabetes mellitus. Negative attitudes of some healthcare workers and inadequate infrastructure, according to caregivers, frustrated them in the process of their interactions. They desired home care services, and preferential treatment for older adults. With these, they would be supported in providing the needed care to older adults and their burden for caregiving will be reduced.
Footnotes
Acknowledgements
The researchers acknowledge the co-operation of family caregivers of older adults with Hypertension and/or Diabetes Mellitus who participated in the study. We are equally grateful to Dr. Sarfo Kantanka and Dr. Osei Nyantakyi for their collaboration.
Author Contributions
Edward Appiah Boateng and Rosemary Agyapomah researched literature and conceived the study. Edward Appiah Boateng, Rosemary Agyapomah, Isaac Amankwaa, Veronica Millicent Dzomeku, and Lawrencia Oppong Peprah were involved in protocol development, gaining ethical approval, patient recruitment and data analysis. Rosemary Agyapomah wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.
Ethical Considerations
Ethical clearance was obtained from the Committee on Human Research Publication and Ethics (CHRPE) with reference number CHRPE/AP/100/20 and the Komfo Anokye Teaching Hospital Institutional Review Board (KATH-IRB) with reference number KATH-IRB/CA/016/20. Researchers explained the purpose of the study to potential participants and allowed them to decide whether to participate on a voluntary basis. Those who chose to be part of the study signed or put a thumbprint on the informed consent form (Connelly, 2014; Pietila et al., 2020). Participants were assured of confidentiality and we used pseudonyms in presenting the results of the study to guard participants identities. Soft copies of files were kept on a password-protected computer while hard copies were kept under lock-and-key, only accessible to the research team.