
Abstract
This study is the first to investigate ageism and its determinants in Lebanese healthcare settings. We diffused an online survey including the Fraboni Scale for Ageism (FSA) and other variables to healthcare workers and trainees at an urban university hospital in Lebanon. We recruited 233 participants (47.2% medical students, 21.5% nurses, 20.6% physicians, and 10.7% nursing students). The FSA mean total score was 58.9 (SD: 10.2), considered to be “low levels” of ageism. There was a positive correlation between age and FSA total score (p = .041). Regression analyses showed that only living or having lived with an older person remained associated with significantly lower ageism scores. Workers in the field of nursing had significantly higher ageist attitudes compared to those in medicine. Promoting intergenerational contact in addition to modifying nursing curricula and providing educational workshops on healthy ageing in the workplace are needed to mitigate ageism among healthcare workers and trainees.
Introduction
Ageism, defined as stereotyping, prejudice, or discrimination towards individuals based on age, has become an emerging international and public health concern (Chang et al., 2020; Lenchik et al., 2023). With the rapid increase in life expectancy and population ageing, the term “ageism” has been used interchangeably with ageism against older adults. Data from the World Values Survey, including 57 countries, revealed that 60% of respondents have reported that older people do not receive the respect they deserve (Inglehart et al., 2014). In addition, one in two people have demonstrated an ageist attitude, according to the latest 2021 report by the World Health Organization (WHO). There are three levels of expression of ageism: self-directed ageism, for example when older adults believe they are unable to learn new things; interpersonal or social ageism, for example when an individual avoids contact with an older adult or belittles an older adult, and institutional ageism. Examples of the latter include imposing a retirement age, age dictating certain medical procedures, exclusion of subjects from clinical research based on age, or adopting laws and policies that are discriminatory based on age (Marques et al., 2020). Ageism against older adults is associated with poor physical health (increased unhealthy habits, obesity, poor adherence to treatment), poor recovery from illness and increased mortality risk. It is also associated with increased loneliness and isolation due to social exclusion from meaningful relationships and roles, poor mental health, including increased risk for depression and cognitive impairment and increased financial burden (Burnes et al., 2019; B. R. Levy et al., 2020). Unfortunately, ageist attitudes against older adults are widespread among physicians, nurses, nursing, and medical students/trainees and other healthcare workers (Nemiroff, 2022). Dangerous assumptions related to old age have been shown to be associated with detrimental consequences in older adults. Examples include withholding medical information from patients, withholding certain treatment options based on age, and excluding older adults from clinical trials. These examples and many others have been associated with decreased quality of care, and negative physical, mental, and functional consequences in older adults (Chrisler et al., 2016; Herrera et al., 2010; Higashi et al., 2012; São José & Amado, 2017). The COVID-19 pandemic further exposed ageism towards older individuals, notably in healthcare settings (Silva et al., 2021). Combating ageism is one of the four action areas of the Decade of Healthy Ageing (2021–2030) launched by the WHO, the Office of the UN High Commissioner for Human Rights, the UN Department of Economic and Social Affairs, and the UN Population Fund in 2021 (Mikton et al., 2021). Individuals residing in low- and lower-middle-income countries (LMIC) are five times more likely to have higher ageist attitudes compared to higher-income countries (Officer et al., 2020). This finding could be explained by higher exposure of the population living in LMIC to older adults with poor health, and precarious healthcare systems, leading to negative attitudes and assumptions about age related functional decline. This is concerning as two-thirds of the world’s population aged 60 years and over will reside in LMIC by 2050. Many LMIC are experiencing rapid population ageing at a faster rate than in Western Europe and North America, but may not have the resources to respond to the WHO call to action (Tan, 2022).
Lebanon is a small low-income country located in Western Asia surrounded by the Mediterranean Sea to the west, Syria to the north and east, and Israel/Palestine to the south. Its surface area measures 10,452 km2, and its population is estimated to be 5,268,229, as of February 2024. The life expectancy at birth is around 76 years ( https://www.worldometers.info/world-population/lebanon-population/ ). Lebanon has been experiencing an extremely fast-growing population confronted with limited resources to meet its basic requirements. Despite the few data available, this small country reports that more than 10% of its population is above 65, ranking first in the Arab region with this proportion (Abdulrahim et al., 2015). The well-being of Lebanese older adults has been threatened by the longstanding political instability, lack of governmental support, social and health related policies, and lack of publicly funded healthcare centres/institutions (Abdulrahim et al., 2015).
Only one previous Lebanese study investigated self-discrimination against older adults aged 60 and above: Lebanese living in urban areas like Beirut or rural areas like Ras-Baalbeck were shown to have higher age discrimination and lower self-esteem than those who immigrated to Dakar (El Bcheraoui et al., 2015). Our study is the first to investigate the prevalence of ageism among Lebanese healthcare professionals (doctors and nurses) and trainees (nursing and medical students) and explore the correlates of ageist perceptions and attitudes to inform future anti-ageist interventions in our country. We postulated that low levels of ageism would be found among all Lebanese healthcare workers, irrespective of their age or healthcare work category, given that collectivism and religion are considered fundamental values in the Lebanese culture (Ayyash-Abdo, 2001) which could mitigate ageism.
Methods
Study Design
This is a single-centre, cross-sectional study aiming to examine ageism and its correlates among Lebanese healthcare professionals (physicians and nurses) and trainees (medical and nursing students). The data were collected between January 28 till February 28, 2022.
Study Population
We enrolled physicians, nurses, nursing, and medical students working or rotating at Saint Georges Hospital University Medical Centre, at the time of the study.
Ethical Approval
The study received approval from the Institutional Review Board (IRB) of Saint Georges Hospital University Medical Centre (IRB-REC/O/066-21/3321).
Survey Dissemination and Data Collection
After receiving IRB approval, we sent electronic mail invitations to the Deans of both schools of nursing and medicine, affiliated with Saint Georges Hospital University Medical Centre to disseminate an electronic survey to their students. Similarly, the head nurse administrator at Saint Georges Hospital, as well as the head of medical and surgical departments were contacted to send a similar electronic mail invitation to physicians, residents, and nurses in each department. The electronic google form survey was made accessible for 1 month (January 28–February 28, 2022). Electronic reminders to fill out the survey were sent to elicit participation.
Instruments
Filling the online survey required obtaining electronic consent prior to participation by ticking a box. We gathered the following sociodemographic information: age, gender, location of origin, and region of current residence (capital city/suburbs vs. rural areas/villages), contact with older adults by asking the following question: “do you currently live or have lived with an adult aged ≥ 60 years?.”
All participants had a university level of education, given that they are working or training in this academic setting. The level of education was thus not assessed, but participants were rather divided depending on the healthcare category they belonged to (nurse, physician, nursing student, medical student). The main tool used to measure ageism was the Fraboni Scale for Ageism (FSA) which is a thorough assessment of three components: antilocution (making negative verbal comments against older adults), discrimination, and avoidance (Ayalon et al., 2019). It comprises 29 items, with a total score ranging between 29 and 116. The higher the score, the more ageist attitude the participant has (Fraboni et al., 1990). This scale has been previously used in the Arab culture (Ibrahim & Bayen, 2019). One validation study using the Turkish version of the FSA in healthcare workers determined a cutoff score of 78 and above to demonstrate the presence of discrimination in this population (Ozel Bilim & Kutlu, 2021).
The entire survey was in English, which is the official language taught and spoken in nursing and medical schools at University of Balamand, in Lebanon.
Statistical Analysis
The data collected through google forms was extracted to Excel then SPSS (Statistical Package for the Social Sciences, version 21.0, Armonk, NY: IBM Corp) to conduct statistical analysis. First, we performed a descriptive analysis to explore the demographics of participants, as well as their ageist perceptions towards older people as reflected by the total FSA score, as well as the three subscales (antilocution, discrimination, and avoidance subscores). Then, we performed bivariate and multivariate analyses to examine the relationship between the FSA total score and subscores and the different variables of interest gathered. We used chi-square tests to assess the association between two categorical variables, and t-tests for continuous variables with a significance level set at .05.
Results
Descriptive Analysis
In total, 233 participants completed the online survey. The studied population consisted of 110 medical students (47.2%), 50 nurses (21.5%), 48 physicians (20.6%), and 25 nursing students (10.7%). The mean age was 29.2 (Standard Deviation—SD = 12) years; with an age range of 19 to 75 years, and a median age of 24 years. Almost two-thirds were female (68.7%). Half the sample came from rural areas. Almost 60% currently lived or have lived with an adult aged ≥ 60 years (results shown in Table 1). The FSA total score ranged between 33 and 87 (mean 58.9; SD 10.2). The mean/SD scores were 22.6 (4.5), 17.2 (3.2), and 19.1 (4.3) for the antilocution, discrimination and avoidance subscales of the FSA respectively, as shown in Figure 1.
Descriptive Analysis of Variables of Interest in Study Population.

Mean and standard deviation (SD) were used for continuous variables whereas percentages and absolute numbers were shown for categorical variables.
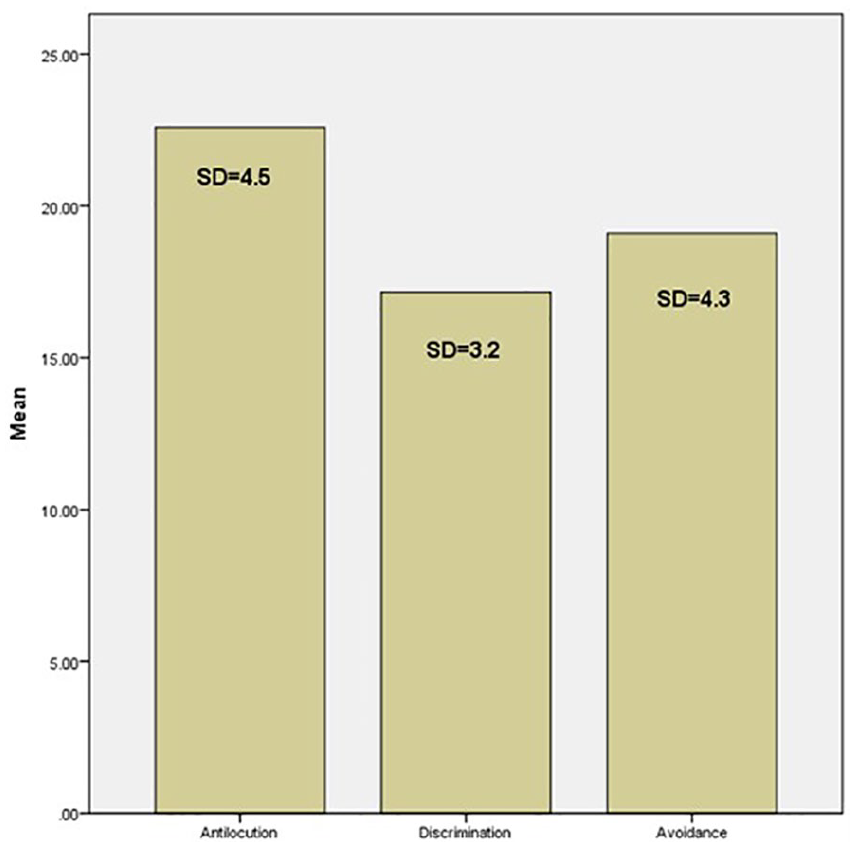
Mean scores and standard deviations (SD) of FSA subscales.
To note, the Cronbach’s alpha for the total FSA scale was found to be .88. The Cronbach’s alpha values for the antilocution, discrimination and avoidance subscales were .76, .67, and .79 respectively.
Inferential Statistics
We found a positive correlation between mean age and the FSA total score (p = .041), as well as discrimination and avoidance subscores (p = .0001). The results of the bivariate analysis are detailed in Table 2. There was no statistically significant effect of gender on ageist attitudes of healthcare professionals in our study. Originating from rural areas/villages was associated with significantly lower discrimination scores (p = .029). Living or having lived with an older individual was associated with significantly lower discrimination scores (p = .002). In addition, students (nursing and medical) were found to have significantly lower avoidance scores on the FSA compared to physicians and nurses (18.53 vs. 19.9; p = .017). However, when the nursing workers (students and nurses) were compared to medical students and physicians grouped together, the first group showed significantly higher ageist attitudes and perceptions on the total FSA, antilocution, as well as discrimination subscales (p < .0001), compared to the second group, as shown in Table 2. Regression analysis showed that living or having lived with an older person, in addition to belonging to the medical healthcare work category compared to the nursing category remained significantly associated with lower ageism scores on the total FSA (p = .036 and p < .0001, respectively), as shown in Table 3. To note, the Variance Inflation Factor (VIF) to assess multicollinearity ranged between 1.05 and 1.3 for the independent variables, indicating absence of collinearity. The adjusted R2 was .09.
Bivariate Analyses of FSA Total Score and Subscores on Covariates of Interest.

Regression Analysis of FSA Total Score with Other Covariates.

Discussion
This study is the first to examine ageist attitudes among nursing and medical healthcare workers (including trainees) in Lebanon, using a comprehensive tool assessing for cognitive, emotional, and behavioural components of ageism. Our findings indicated no (or low) levels of discrimination, as shown by the FSA mean total score of less than 78 in the entire sample (58.9 ± 10.2), as well as in the subgroup of nursing (62.81 ± 8.91) and medical doctors (56.98 ± 10.3). These positive attitudes are reassuring and can be explained by the fact that the Arab culture holds positive views, great respect and importance towards older individuals (Ibrahim & Bayen, 2019). Our study revealed a trend for higher ageist attitudes with increasing age of the healthcare worker. Although some researchers have found a negative correlation between age and ageism (Kalavar, 2001; Rupp et al., 2005), our findings are more concordant with the conclusions of Hellbusch et al. (1995). The latter demonstrated that older adults are often more prejudiced against their own age group, relative to younger age groups, due to high levels of anxiety about ageing as well as self-directed or internalized ageism (Ungar et al., 2024), which are expressed differently across age groups and in different cultures. Our study also showed a lower discrimination attitude among the student category compared to practicing healthcare workers. This could also be explained by higher rates of anxiety about ageing in the older population compared to the students’ subgroup or younger age generation. Moreover, the students have mostly theoretical knowledge about ageing, but have not been in recurrent contact with older adults with multimorbidity and disability to be able to develop yet any negative stereotypes about older individuals such as viewing them as vulnerable, frail and with terminal illnesses (López-Hernández et al., 2021).
Our sample provides an ideal opportunity to examine the contrast between individuals from urban and rural backgrounds, as it consists of 50.2% participants hailing from the capital city and its suburbs, and 49.8% coming from rural areas or villages. Our bivariate analysis showed that originating from rural areas was associated with significantly lower discrimination scores than originating from urban settings. This difference disappeared however in multivariate analysis, possibly due to the small sample size. Various studies in the literature investigated the urban–rural difference in expression of ageism against the older population, with mixed findings. A 2023 Turkish study involving nursing students showed that residing in or originating from a rural background significantly diminished negative ageist attitudes (Ozaydin et al., 2023). Zhou et al. discussed that there is an increasing prevalence of an ageing population in rural areas which can be attributed to the migration of young individuals to urban areas for education, employment, social activities, and lifestyle. This demographic trend is hypothesized to increase interaction with older individuals in rural settings, thereby fostering a sense of prevention against discrimination and stigmatization towards them (Zhou et al., 2019). On the other hand, an Egyptian study conducted among 320 nursing students revealed lack of knowledge regarding older adult care, and significant correlation with negative attitudes towards them, measured using the Anxiety about Ageing Scale (AAS). However, urban nursing students were shown to have higher knowledge and significantly lower ageism compared to rural students (Mohammed & Abdel Aziz, 2019). Similarly, high levels of ageism, abuse, neglect, and exploitation were found in rural Ethiopia, probably fed by lack of healthcare resources and financial insecurity in the underserved rural regions (Zelalem et al., 2023).
In addition, our results showed that living or having lived with an older individual was associated with significantly lower overall ageism and discrimination scores, which is in concordance with the available literature. Toygar and Karadakovan (2020) demonstrated that ageism assessed using the AAS was significantly lower in nursing students who had cared for older individuals throughout their education and those who had lived with older relatives throughout their lives. Another study assessing ageism in 377 nursing students using the Kogan’s Attitude Towards Old People Scale showed that having a previous experience with community older adults or with older relatives favoured a more positive attitude, while working for institutionalized older patients worsened their attitudes (López-Hernández et al., 2021). These findings highlight the importance of intergenerational contact offering opportunities for prolonged contact between younger and older individuals, fostering positive relationships and acting as a buffer against stereotypical negative self-views (Nelson, 2019). More recent research has shown that intergenerational programmes implemented from early childhood (school years through college) yielded significant effective results on building a positive attitude towards the older generation (Burnes et al., 2019; S. R. Levy & Lytle, 2019). More importantly, contact with healthy older individuals shapes how young and older adults view ageing, in a rather positive lens, leading to a reduction of ageist stereotypes across the lifespan (Cohn-Schwartz et al., 2023). In Lebanon, Ajrouch et al. reported that only 12% of adults aged 65 and above live alone (Abdulrahim et al., 2015). Mehio-Sibai et al. (2009) also reported that among older individuals who live with others, the majority are the heads of their own household where the rest of the family resides. Less than 10% of older Lebanese are institutionalized (El-Hayeck et al., 2016). The reasons behind this high percentage of older Lebanese living with their respective relatives are the strong belief Lebanese hold regarding keeping nursing homes as a last resort for their older parents, in addition to the lack of a retirement plan or health coverage supported by the government. It is thus very common for children to be brought up by their grandparents who may be living very close by or within the same household. Older Lebanese rely on their own children to support them financially (Chemali et al., 2008). This multigenerational living situation possibly underlies low ageism scores among the Lebanese population.
Finally, the nursing healthcare workers (nurses and nursing students) were shown to have significantly higher ageist attitudes compared to medical doctors and students. These results are similar to the findings of a Jordanian study (Shoqeirat & Al-Nawaiseh, 2002) which assessed for ageism among 911 healthcare workers using the Attitude Towards Elderly scale, and found significantly higher ageism among female nurses. This finding is also concordant with the Western literature showing that nurses may have less accurate knowledge about healthy ageing, higher anxiety about ageing, and lower expectations for treatments and rehabilitation for their older patients (Ben-Harush et al., 2017). Additionally, nurses carry a high burden of care compared to physicians, given that they are more in contact with sick and frail older patients. Although contact or exposure theory encourages increased contact with older individuals, being exposed on a daily or weekly basis to older individuals who are frail, malnourished, or with dementia was found to promote negative stereotypes of “getting older” (Rababa & Hammouri, 2023).
In another study involving nursing healthcare workers, the authors emphasized the importance of applying several concurrent anti-ageist interventions, the most important being increasing knowledge about ageing, decreasing levels of anxiety about ageing and adjustment of expectations (Donizzetti, 2019; Palsgaard et al., 2022). Based on these findings, we recommend revising university curricula in Lebanese nursing schools to include education material related to healthy ageing. A second recommendation includes providing continuous education in healthcare work settings such as conducting workshops covering topics such as the beauty of ageing, polypharmacy, autonomy, and healthy ageing (Wong et al., 2022). Finally, we recommend alleviating nursing caregiver burden (Burnes et al., 2019) to allow nurses to happily work with older patients.
Our study is not without limitations. First, our sample stems from one urban tertiary care centre and groups only physicians and nurses (practitioners and trainees). It is an exploratory study based on convenience sampling, as data collection was limited to 1 month only due to COVID-19. Thus, our study is not representative of the entire Lebanese healthcare worker population which should ideally include social workers, medical and non-medical technicians, nurse aids, and administrative hospital personnel, from different healthcare fields and settings. Second, our study was conducted during the COVID-19 pandemic, when misinformation and negative stereotypes against older individuals were at their peak, which might have affected the participants answers. Indeed, ageism is a subjective variable reflective of a person’s opinion, and subject to certain circumstances and stressors. Third, although the FSA is a comprehensive tool, we used an English version with cutoffs adopted in a Turkish study, as there are no validated Arabic version, nor cut-offs adopted by the originators of the FSA. Future studies should thus focus on translating, validating, and determining normative values for ageism assessment tools in Arab-speaking populations. Additional variables such as anxiety about ageing, and psychological distress of healthcare workers need to be incorporated in future studies on ageism.
Conclusion
Our study provides valuable insights into ageism in the healthcare setting in the Middle East, showing an overall positive attitude towards older patients among Lebanese nursing and medical students and professionals, during very challenging times experienced throughout the COVID-19 pandemic. Being exposed to older adults emerged as a consistent protective factor against ageism towards older adults. Hence, our findings highlight the importance of intergenerational exposure in developing positive and healthy ageing concepts to combat ageism. Compared to medical students and physicians, the nursing body was found to have significantly higher ageist attitudes and perceptions, emphasizing the need to modify nursing curricula to incorporate lectures and regular workshops on this topic, and to implement interventions to decrease the burden of care on nurses working with the geriatric population. Larger and more generalizable studies are needed to provide a better understanding of the healthcare practitioners’ perceptions and stereotypes throughout their healthcare career, in different settings.
Footnotes
Acknowledgements
None reported.
Ethical Considerations
The study received approval from the Institutional Review Board (IRB) of Saint Georges Hospital University Medical Centre (IRB-REC/O/066-21/3321)
Consent to Participate
Informed consent was obtained electronically prior to starting the survey (by ticking a box).
Consent for Publication
Not applicable.
Author Contributions
S.A. contributed to study conceptualization and design, data collection and writing the different drafts of the manuscript. A.B., and S.M. contributed to study design, data collection, and writing the different drafts of the manuscript. R.K. assumed a leading role and was involved in supervising all aspects of the study. R.K. contributed to study conceptualization and design, data analysis and interpretation and editing and revising the manuscript.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All data generated or analysed during this study are included in this published article. Any further data needed can be made available upon request made to the corresponding author.