
Abstract
Keywords
Introduction
Early on into the COVID-19 pandemic in the beginning of 2020, it was suggested that health inequalities may increase during and after this historical period. The reasons for this suggestion included reduced access to healthcare for non-COVID-19 concerns in overwhelmed healthcare systems (Bambra et al., 2020). This reduced access resulted, for example, in increased waiting times for elective surgeries in many OECD countries, even at times of fewer COVID-19 cases and hospitalizations (Organisation for Economic Co-operation and Development (OECD)/European Union, 2020). Within the United States, non-COVID-19 primary healthcare decreased in line with state closure policies (Ziedan e al., 2020). In particular, healthcare professionals viewed the management of chronic conditions as negatively affected, even if in-person visits could often be replaced by telehealthcare (Chudasama et al., 2020).
The pandemic control measures included stay-at-home orders, closures of restaurants, bars, fitness and other sports centers, social gatherings in- and outdoors, and restrictions to non-COVID-19 healthcare. This latter helped ensure healthcare systems’ responsiveness to people with severe COVID-19 illness, anticipating strained medical physical and human resources due to treatment of COVID-19 infected patients (Anderson et al., 2021; Lawson et al., 2021). Furthermore, there were concerns that COVID-19 infections could spread to both patients and staff within medical settings (Anderson et al., 2021; Metelmann & Busemann, 2020). Many persons thus had non-COVID-19 medical appointments or treatments forgone, postponed, or denied. These often included in-person primary care consultations and non-emergency medical appointments (e.g., fertility treatments and preventative dental care). However, to date, there has been limited comprehensive assessment of missed healthcare across Europe. Furthermore, we have little evidence on population groups and countries that were more affected by missed healthcare as an unintended consequence of the pandemic control measures. Accordingly, a detailed investigation of types of missed non-emergency healthcare, specifically forgone, postponed, and denied medical appointments and treatments, seems indicated.
During 2020, only a few European regions’ healthcare services were considered overwhelmed, most common of which were those within intensive-care units (e.g., Lombardy in spring 2020 and Portugal in winter 2020). Nonetheless, reduced access to medical services during the lockdown periods were observed in many countries (Nunez et al., 2021).
Users of primary healthcare services are predominantly of older age (Gerich et al., 2020; Rennemark et al., 2009). As older people more often need regular medical treatment due to aging-associated chronic conditions such as hypertension, chronic bronchitis/COPD, or coronary heart disease (OECD, 2019), they are likely more affected by reduced healthcare access. During the COVID-19 era, this compounds older adults’ health anxieties based on their greater vulnerability to the consequences of COVID-19 infection (Barber & Kim, 2021; Ribal et al., 2020). This is especially the case among older persons with chronic illnesses (Río-Lanza et al., 2021). Therefore, it is important that we understand missed healthcare through the COVID-19 pandemic among the more vulnerable older population.
In this paper, we estimate from a user perspective the extent to which medical appointments and treatments of older adults in Europe in 2020 were forgone, postponed, or denied. This provides insights into potential morbidity (and even mortality) burden due to missed healthcare. We investigated the demographic, social, and socioeconomic (individual-level) determinants of missed healthcare. Exploiting the harmonized design of a cross-national survey on aging, we additionally explored country-level predictors of missed healthcare, focusing on healthcare performance and old-age ageism.
Theoretical Perspectives
In analyses of older adults’ healthcare use during the pandemic for non-COVID-19 concerns, their amounts of various forms of capital are of importance (Abel, 2008; Malat, 2006; Paccoud et al., 2020). Paccoud et al. (2020) highlight the significance of Bourdieu’s (1986) concepts of economic, cultural, and social capital for older adults’ healthcare use. Economic capital includes wealth and income, which can purchase high-quality healthcare services. Cultural capital includes learned attitudes, behaviors, and ways of responding to the world, as well as credentials, such as university degrees.
The European context is dominated by universal health coverage systems (Immergut et al., 2021), in which fewer barriers exist to healthcare access compared to other countries. Within Europe, higher amounts of economic and cultural capitals, operationalized here through income and education, respectively, increase healthcare use, including for preventive care (Paccoud et al., 2020). Higher income and education may also go along with higher value placed on good health, and medical literacy (Paccoud et al., 2020). Increased healthcare use in pre-pandemic times and value placed therein may thus raise likelihoods of having had forgone, postponed, or denied medical healthcare through the pandemic. Furthermore, higher income and education might—in relation to medical literacy (see Paccoud et al., 2020)—increase awareness of risk of COVID-19 infection when leaving the home, raising likelihood of avoiding medical appointments and treatments. More generally, stronger sentiments of risk of COVID-19 infection and morbidity raised likelihood of avoiding healthcare (Lu et al., 2021).
Earlier Research on Predictors of Missed Healthcare during the COVID-19 Pandemic
Beyond analyses of the general extents and consequences of unmet healthcare needs during the pandemic (Anderson et al., 2021; Lawson et al., 2021; Metelmann & Busemann, 2020), some research has examined their predictors. Patients’ fragility and severity of conditions decreased likelihoods of medical professionals postponing treatments and the lengths of these postponements when they occurred (Metelmann & Busemann, 2020). Nonetheless, some persons with health concerns accepted or elected to have medical treatments canceled or postponed (Metelmann & Busemann, 2020). Psychological factors, such as tendencies to factually analyze circumstances, coping strategies based on cognitive restructuring (Lawson et al., 2021), and stronger emotional reactions to the COVID-19 pandemic (Hajek et al., 2021), influenced postponing medical care. One study found that women and those over 65 years of age were disinclined to proceed with a surgery with high risk of COVID-19 infection and mortality (Brown et al., 2021). Anderson et al. (2021) found in a U.S. sample increased rates of forgone medical services among Hispanics (compared to Whites) and younger persons, as well as those with lower household incomes, either unemployed or out of the workforce because of disability, in worse health, not taking a prescription medication, and with a mental health condition.
Furthermore, missed healthcare may differ by gender. At older ages in specific, and due to the longer life expectancy of women overall, women have on average higher morbidity burden, seek more medical care (Cameron et al., 2010), and live longer with activity limitations than men (Jagger et al., 2008). However, relative to their higher morbidity burden and functional limitations, older women still underuse healthcare services (Cameron et al., 2010). Additionally, women experienced greater feelings of risk concerning the COVID-19 pandemic and showed higher willingness to adhere to government recommendations (Dryhurst et al., 2020; Lu et al., 2021; Rana et al., 2021). This suggests that women might have been more likely to forgo medical appointments, or agree to their postponement, during the pandemic.
Importance of Country-Level Predictors
Going beyond individual-level predictors, we were also interested in comparative indicators of the functioning of (pre-pandemic) national healthcare systems. This concerns infrastructure, based on amounts of doctors and hospital beds, and generosity, indicated by healthcare expenditures per capita and population coverage for medical services. Because of the overburdening of medical systems during the COVID-19 pandemic (Metelmann & Busemann, 2020), these variables might have affected forgone, postponed, and denied medical appointments and treatments. For example, healthcare systems characterized by high population coverage may have imposed restrictions on “normal,” non-COVID-19 healthcare, anticipating higher than usual demands (including high COVID-19 hospitalization rates, i.e., Italy in spring 2020) potentially overburdening the system.
Furthermore, values and norms may define which healthcare needs of which population groups should be prioritized. Before the pandemic, these values and norms may have resulted in subtle differences in allocation of healthcare resources and in perceived barriers to healthcare access for certain population groups, such as women, older people, and people of lower socioeconomic status (Fitzpatrick et al., 2004). Values and norms may also influence which healthcare needs are seen as essential and are thus reimbursed by the state, and which may need co-payment or out-of-pocket (private) payment.
During a pandemic, as medical services and treatments are managed with scarce resources (numbers of nurses and doctors, hospital beds, equipment, etc.), these values and norms may become more important, affecting the prioritization of services. For example, during 2020, while emergency services and urgent medical treatments such as stroke units were maintained, and new COVID-19 units were installed, in many countries fertility treatments and elective (planned) surgeries were reduced or even temporarily stopped (Brown et al., 2021; Lawson et al., 2021). Equally, healthcare may prioritize more socially valued population groups, corresponding to the widely adopted categorization of “essential workers” (e.g., healthcare professionals and supermarket staff). The possible prioritization of younger groups to receive healthcare could be linked to old-age ageism (i.e., the attribution of characteristics to persons based on age) (Ayalon & Tesch-Römer, 2018).
Old-age ageism may negatively impact healthcare allocation and use. First, old-age ageist views may implicitly or explicitly affect political leaders’ prioritization of healthcare resources to younger people, particularly in times of scarce resources, such as during the COVID-19 pandemic. Earlier research has shown that the demographic structure of the population itself potently contributes to attitudes and behaviors (Hill et al., 2021). For example, the population-level share of older adults itself is a determinant of protective behaviors during COVID-19, such as sheltering in place (Hill et al., 2021). While globally a higher share of older adults is associated with lower general (young- and old-age) ageism (Officer et al., 2020), in the European context, perceptions of age discrimination are quite high, with 44% of respondents in the European Social Survey countries reporting that age discrimination is “quite” or “very” serious (Abrams et al., 2011). Earlier research has confirmed direct associations between state-level negative views on old age, or old-age ageism, and poorer state-level health (Giasson & Chopik, 2020). Second, country-level old-age ageist views may be internalized by older adults (Weiss & Kornadt, 2018). This may change their behavior, for example, they may not insist on receiving healthcare even when it is needed. Wyman et al. (2018) discuss the general ageism within healthcare settings that reduces the quantity and quality of the healthcare older adults receive. While ageism becomes increasingly salient in times of almost universal dramatic population aging, the importance of ageism has not yet been reflected in empirical research (Ayalon et al., 2019; Wilson et al., 2019).
While higher levels of old-age ageism may not become manifest as explicit discrimination, we hypothesize that in times of scarce resources, subtle barriers to healthcare access may develop, and particular needs might thus be neglected. For example, reductions might occur within public transport especially utilized by older people to access healthcare services.
Associations between country-level old-age ageism and older people’s healthcare use have not been systematically explored to date. However, old-age ageist statements in the media, in public discourse, and even by some countries’ political leaders were quite common during the COVID-19 pandemic (Ayalon et al., 2021; Fletcher, 2021; Graf & Carney, 2021). Earlier research has shown that societal-level negative attitudes toward aging are quite stable through time (Abrams et al., 2015; Azulai, 2014). Negative attitudes toward aging may have become more explicit during the COVID-19 pandemic and may have had substantial impact on political decisions to prioritize healthcare services for different population groups. Accordingly, we explored country-level old-age ageism as a predictor of older adults’ unmet healthcare needs (or barriers to healthcare access), indicated by forgone, postponed, or denied medical appointments and treatments.
Methods
Dataset and Sample
This study focused on the COVID-19 module of the Survey of Health, Ageing and Retirement in Europe (SHARE), conducted from June to August 2020 in 27 European countries and Israel (see Börsch-Supan, 2022). This module is complemented by data from waves eight (2019–2020) (see Börsch-Supan, 2021), seven (2017), and six (2015) (see Börsch-Supan, 2020a; 2020b), and the easySHARE dataset (see Börsch-Supan & Gruber, 2020). The SHARE studies the economic, social, and health situations of European respondents of 50 years of age and older. It is based on biennial waves since 2004, includes regular refreshment samples, and has grown from initially eleven to now 27 European countries and Israel. The COVID-19 module of the SHARE further includes assessments of respondents’ lives through the COVID-19 pandemic. Further details concerning the SHARE are available within Börsch-Supan et al. (2013). This study’s sample took part in the COVID-19 module and was then at least 50 years of age (analytical sample of 57,025 respondents).
Some variables were obtained from waves eight, seven, and six of the SHARE, and the easySHARE dataset, because they were required and were not included in the COVID-19 module. The easySHARE is a streamlined generated dataset that combines variables for all respondents within all waves into one file (see Gruber et al., 2014). The variables obtained from these additional datasets are discussed below.
Variables
Dependent Variables
This study’s three dependent variables denote different types (forgone, postponed, and denied) of missed healthcare through the COVID-19 pandemic. Respondents answered “yes” or “no” to each of these questions within the COVID-19 module: “Since the outbreak of Corona, did you forgo medical treatment because you were afraid to become infected by the corona virus?” “Did you have a medical appointment scheduled, which the doctor or medical facility decided to postpone due to Corona?” “Did you ask for an appointment for a medical treatment since the outbreak of Corona and did not get one?”
Answers of “yes” were accorded scores of “one” while answers of “no” were accorded scores of “zero.”
Independent Variables
This study assessed both individual- (respondent-) and country-level determinants of the three types of missed healthcare. At the respondent level, we explored if types and extents of missed healthcare differed by gender (reference (ref.) = men) and by age group (50–59, 60–69, 70–79, and 80 years and older (ref.)). Our focus also included years of education and respondent-reported total household income as measures of socioeconomic status (see the above discussion of various forms of capital). Only 14.39% of respondents reported their years of education (a relatively time-constant variable) at wave eight. For the remainder, years of education were obtained from wave seven within the easySHARE, which includes years of education reported in all waves up to and including wave seven. Total household income was based on the SHARE’s COVID-19 module question, “How much was the overall monthly income, after taxes and contributions that your entire household had in a typical month before Corona broke out?” Among respondents with missing data (23.65%), household income information from the SHARE’s wave eight (if available and non-missing) was substituted, based on the question, “How much was the overall income, after taxes and contributions, that your entire household had in an average month in [the previous year]?” All answers were recorded in Euros. Respondents were categorized into household income quintiles, specific to their particular countries. This assuaged concerns with country-level differences in purchasing power parity (PPP) and household income distributions.
We studied six country-level variables relevant to the allocation and use of healthcare services by middle-aged and older adults. The first two were based on healthcare systems’ infrastructure in terms of medical staff and resources: 1) number of practicing doctors per 1000 population (2018, or nearest year) and 2) number of hospital beds per 1000 population (2018, or nearest year). These variables are available within OECD (2020).
Two additional country-level predictors were based on policies related to healthcare systems’ generosity: 1) health expenditures per capita (2019, or nearest year) (adjusted for unequal PPPs) and 2) combined total public and primary private coverage for a core set of medical services (2018, or nearest year) (in percentages). Both variables are also available within OECD (2020). To produce more substantial odds ratios (ORs), the former was divided by 1000.
The final two country-level predictors were measures of old-age ageism. They were developed through the 2008 module of the European Social Survey (ESS Round 4, 2008), which is the latest module to include measures of old-age ageist views. In answer to, “And overall, how negative or positive do you feel toward people over 70?,” respondents responded zero (extremely negative) to ten (extremely positive). In answer to, “Please tell me whether or not you think people over 70 are a burden on [country]’s health service these days?,” respondents reported zero (no burden) to ten (a great burden). Both variables were averaged within each country, producing two country-level measures of ageism. The average country had 1924 respondents answering the former question and 1894 respondents answering the latter question. Respondents’ ages ranged from 15 to 105 years.
The timing of these two measures is supported by scholarship emphasizing stability through time in society-wide ageist viewpoints (see Abrams et al., 2015; Azulai, 2014). In addressing ageist trends through time, it is important to distinguish between individual-level ageism, based on older adults’ internalization of negative perceptions of advancing age diffuse throughout a culture, and structural-level ageism, enacted through the biased policies and practices of societal institutions that disadvantage older adults (Chang et al., 2020). The above studies’ claims of general temporal stability in ageist attitudes were focused on individual-level ageism, in concordance with the present study’s analyses of ageism. While there is some evidence of changing extents of ageism due to the Great Recession of 2007–2009, it is based primarily on structural ageism, especially within the labor market (Neumark & Button, 2014; Pruchno et al., 2017). One systematic review of how ageism affects older adults’ health based on studies from 1970 to 2017 crossing 45 countries (including many European nations) found that increasing effects of ageism through time were largely due to structural ageism, including among medical professionals (Chang et al., 2020). This scholarship on changing patterns of ageism through time thus reinforces the stability of prevalent individual-level ageism since 2008, thus supporting the timing of the present study’s ageism variables.
Control Variables
We employed family-based control variables plausibly associated with personal medical decisions and needs, thus potentially confounding the central relationships here studied. One was marital or relationship status (married and living together with spouse (ref.), registered partnership, married-living separated from spouse, never married, divorced, and widowed) at wave eight of the SHARE. Because the majority of respondents did not change their marital status between waves seven and eight, only 17.25% of respondents reported their marital status at wave eight. For the remainder, whose marital status stayed constant between waves seven and eight, marital status was obtained from wave seven within the easySHARE. Parental status at wave eight was further controlled (no children, one or two children, and three or more children (ref.)). For the 51.42% of respondents missing data in this relatively time-constant variable at wave eight, amounts from wave seven (if available and non-missing) were substituted. For respondents still missing data in this relatively time-constant variable, amounts from wave six (if available and non-missing) were then substituted. These procedures permitted the assessments of the marital and parental statuses of the complete sample.
Further control variables denoted respondent characteristics that affected their perceived or actual need for medical care, specifically self-perceived health, extent of neuroticism, and general trust. Self-perceived health relates closely to morbidity and indicates need for regular medical care. Neuroticism has been associated with increased medical appointments and visits (Hajek et al., 2017, 2020). Beyond perceived need for medical care, neuroticism might affect sentiments of risk of COVID-19 infection during medical appointments and treatments. General trust may be related to more specific trust that medical personnel’s treatments improve and protect health. It is further an individual-level determinant of compliance with government COVID-19 policies (Bargain & Aminjonov, 2020), thus affecting rates of forgone healthcare (to relieve the burdening of healthcare systems). In fact, social (general) trust and political trust have been shown in several studies to be robustly interrelated (for a review, see Newton et al., 2018).
Self-perceived health was based on the SHARE’s COVID-19 module question, “Before the outbreak of Corona, would you say your health was excellent, very good, good, fair, or poor?” When missing (0.09%), answers within the same range to “Would you say your health is…” in wave eight were substituted. “Poor” was the reference category. Extent of neuroticism, one of the big five dimensions of personality (see McAdams & Pals, 2006), was assessed in the SHARE through amalgamating two separate items, one based on being relaxed, the other based on being nervous. Scores ranged from one to five, with intervals of 0.5. For the 85.74% of the sample missing data in this variable at wave eight, scores at wave seven (if available and non-missing) were substituted. In the SHARE’s wave eight, in response to, “I see myself as someone who is generally trusting,” respondents answered “disagree strongly,” “disagree a little,” neither agree nor disagree,” “agree a little,” and “agree strongly” (ref.). For the 85.65% of the sample missing data in this variable at wave eight, amounts from wave seven (if available and non-missing) were substituted.
Analysis
The central analyses were based on three sets of multilevel logistic regression analyses, one for each dependent variable. Each set included seven models. In each case, the first model regressed the dependent variable upon all the individual-level variables. The second through seventh models sequentially and individually added to the first model each of the six country-level predictors in the following order: number of practicing doctors per 1000 population, number of hospital beds per 1000 population, health expenditures per capita (divided by 1000), extent of population coverage for a core set of medical services, positive feelings toward people over 70, and extent to which people over 70 are viewed as a health services burden.
Missing data were dealt with through multiple imputation using chained equations (ten imputed datasets). While the three dependent variables (see Von Hippel, 2007) and the six country-level predictors were included in the multiple imputation process, all logistic regressions excluded those respondents originally missing data in their respective dependent and country-level variables.
To address unequal probabilities of selection into the sample, all models were weighted with the SHARE’s COVID-19 module design weight. Standard errors were adjusted for clustering at the level of country of residence within the SHARE’s COVID-19 module. Analyses were conducted with the Stata 17 statistical software package.
Supplementary Analyses
The supplementary analyses included descriptive statistics displaying the percentages of the three types of missed healthcare within each country (see Table S1).
They further included assessments of the bivariate relationships between each of the individual- and country-level independent variables and each of the three dependent variables (see Table S2). As with the central analyses, these logistic regressions were conducted with inclusion of the design weights and standard errors clustered by country of residence.
Furthermore, Stata’s “margins” command was employed to assess the magnitudes of the associations of each independent variable with each dependent variable (see Table S3). The predictive margins thus developed revealed the percentile probabilities of forgone, postponed, and denied healthcare. For the individual-level independent variables, these predictive margins were based on the first model of each set of analyses. Concerning the country-level independent variables, these predictive margins were based on the respective model within each set of analyses. For the continuous independent variables, the resultant percentages pertained to their 10th percentiles, their medians, and their 90th percentiles. The only exception is for “population coverage for medical services,” the spread of which suggested that analyses of the 10th percentile, 25th percentile, and median and above (100% coverage) are more appropriate. Throughout these computations, all covariates were held at their means.
As a robustness check, all analyses were repeated with further controls for whether or not a respondent had tested positive for COVID-19, and whether or not someone close to a respondent had tested positive for COVID-19.
It is plausible that the two measures of country-level ageism and the two measures of medical resources here studied might moderate how age is associated with forgone, postponed, and denied healthcare. By its very nature, ageism likely affects older persons differently based on their specific ages. Additionally, because advancing age affects both general health and risk of severe morbidity due to COVID-19 infection, it might affect how burdened medical systems apportion their physical and human resources. Accordingly, further analyses replicated the corresponding models with the addition of interactions between respondents’ ages and these country-level variables (see Table S4). Each interaction was tested individually, within a separate model. To increase the interpretability of the main effects for age within these supplementary analyses, the continuous country-level predictors were mean-centered (see Jaccard et al., 1990).
A robustness check repeated these analyses with the exclusion of Israel because it is not a European nation.
Beyond analyses of variables spanning all countries here included, it is of further interest whether broader European regions showed different patterns of missed healthcare among their older populations. Accordingly, broader European regions were studied as predictors of the three types of missed healthcare (see Table S5).
Northern Europe: Denmark, Finland, and Sweden; Western Europe: Austria, Belgium, Germany, Luxembourg, the Netherlands, and Switzerland; Southern Europe: Cyprus, France, Greece, Israel, Italy, Malta, Portugal, and Spain; and Eastern Europe: Bulgaria, Czech Republic, Croatia, Estonia, Hungary, Latvia, Lithuania, Poland, Romania, Slovakia, and Slovenia.
All individual-level variables were included in all three models. These three logistic regressions also included the design weights and standard errors clustered by country of residence.
Results
Descriptive Results
Descriptive statistics. a
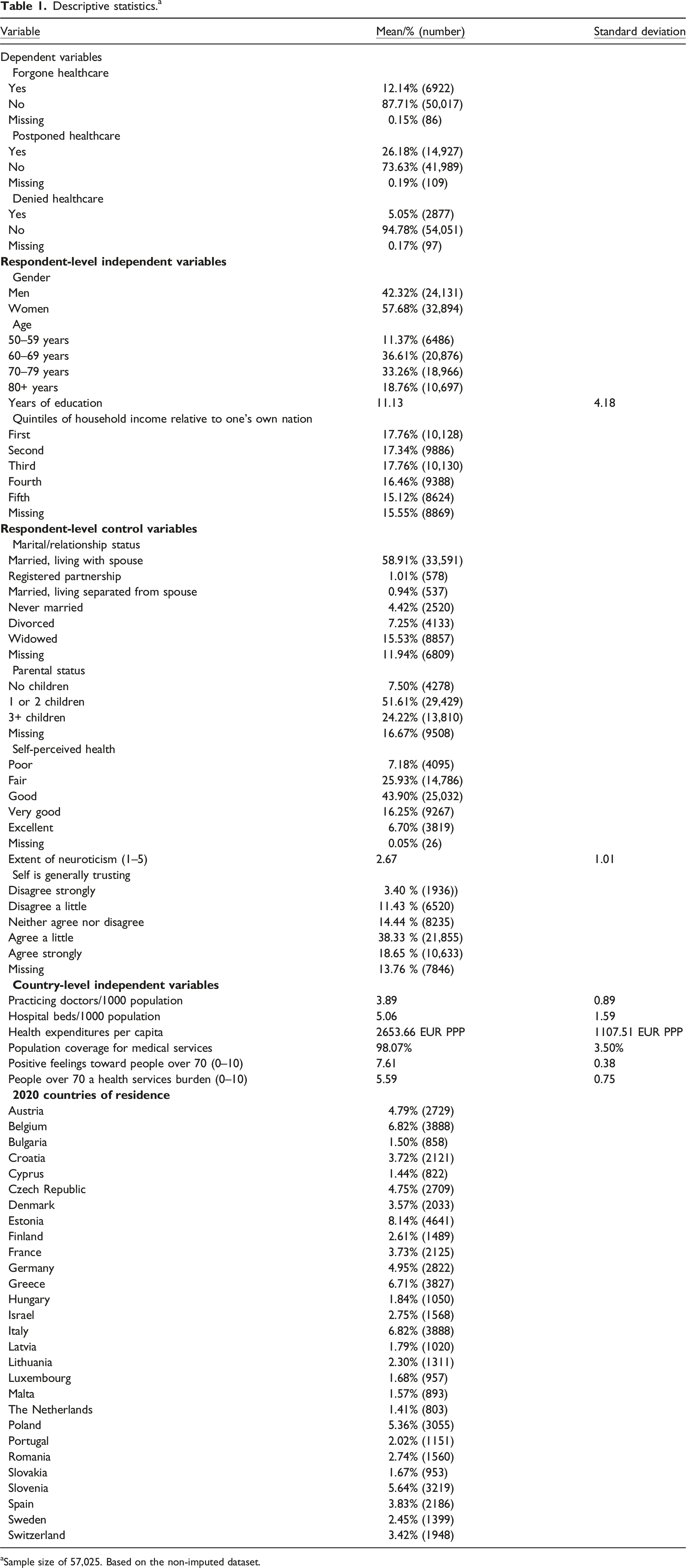
aSample size of 57,025. Based on the non-imputed dataset.
Women represented the majority of the sample (57.68%). The 60- to 69-year-old (36.61%) and 70- to 79-year-old (33.26%) age groups included the most respondents. The average respondent had 11.13 years of education. Across all countries, the third household income quintile had the most respondents (17.76%) and the fifth household income quintile (highest) had the least (15.12%).
Just under 60% of respondents were married and living with their spouse (58.91%). While just over half of respondents had one or two children (51.61%), only 7.50% of the sample had no children.
Self-perceived health had an approximately normal distribution within which “good” health was the modal category (43.90%). Concerning extent of neuroticism, the average respondents had a score of 2.67 within the range of 1–5. Regarding seeing oneself as generally trusting, the modal category was “agree a little” (38.33%).
On average, there were 3.89 practicing doctors and 5.06 hospital beds per 1000 population. Adjusted for differences in PPP, the average health expenditures per capita was 2654 Euros. The average population coverage for a core set of medical services was high (98.07%) but had substantial variability (standard deviation = 3.50%). Views of individuals over 70 years of age were generally positive across the countries (M = 7.61 out of 10). However, views of persons aged over 70 years being burdens on healthcare systems were relatively common (M = 5.59 out of 10).
Respondents were broadly distributed across this study’s 28 countries, listed in Table 1.
Multilevel Logistic Regressions of Respondent- and Country-Level Variables
Logistic regression analyses of forgone healthcare, odds ratios.
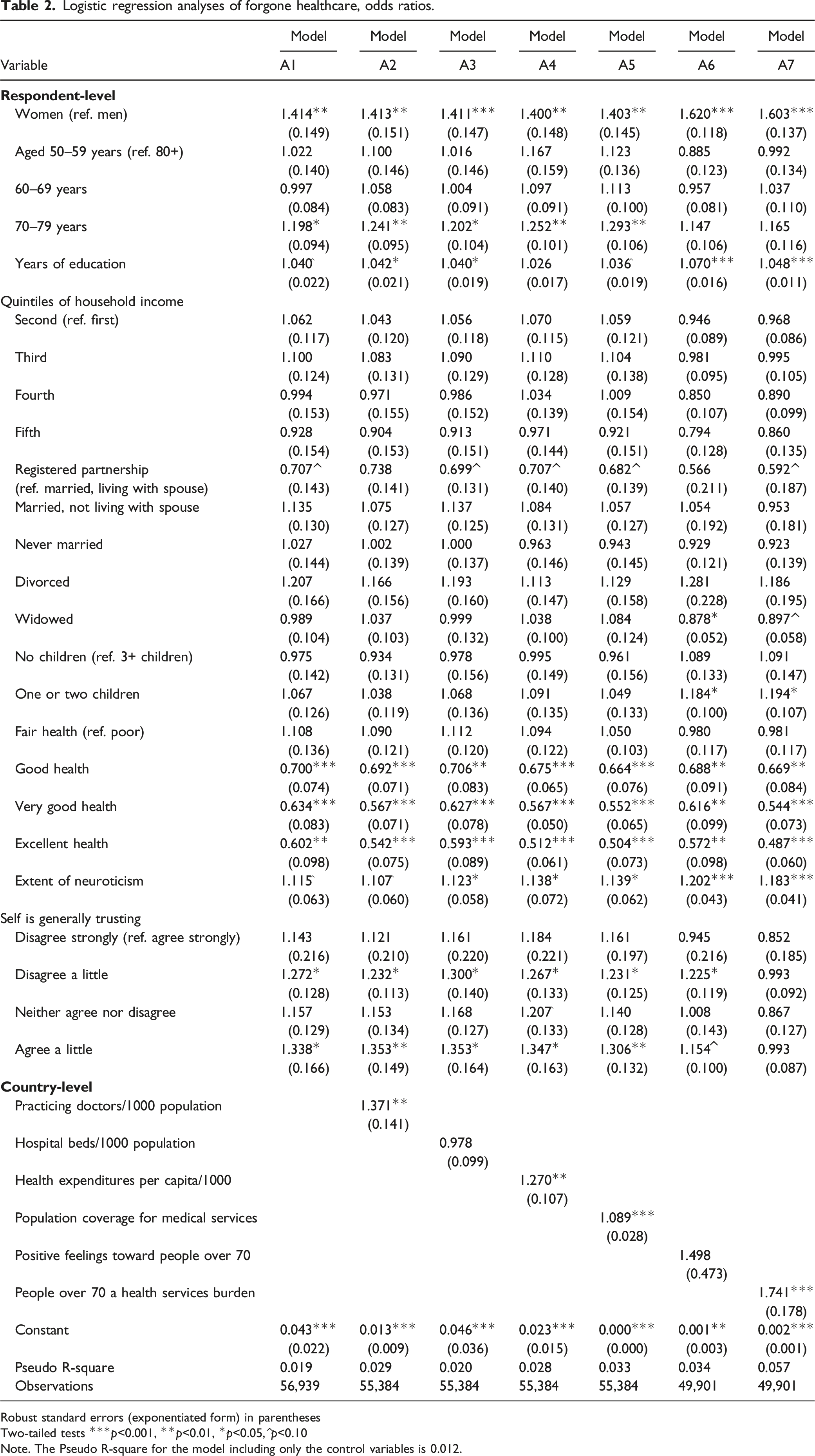
Robust standard errors (exponentiated form) in parentheses
Two-tailed tests ***p<0.001, **p<0.01, *p<0.05, ^p<0.10
Note. The Pseudo R-square for the model including only the control variables is 0.012.
Logistic regression analyses of postponed healthcare, odds ratios.
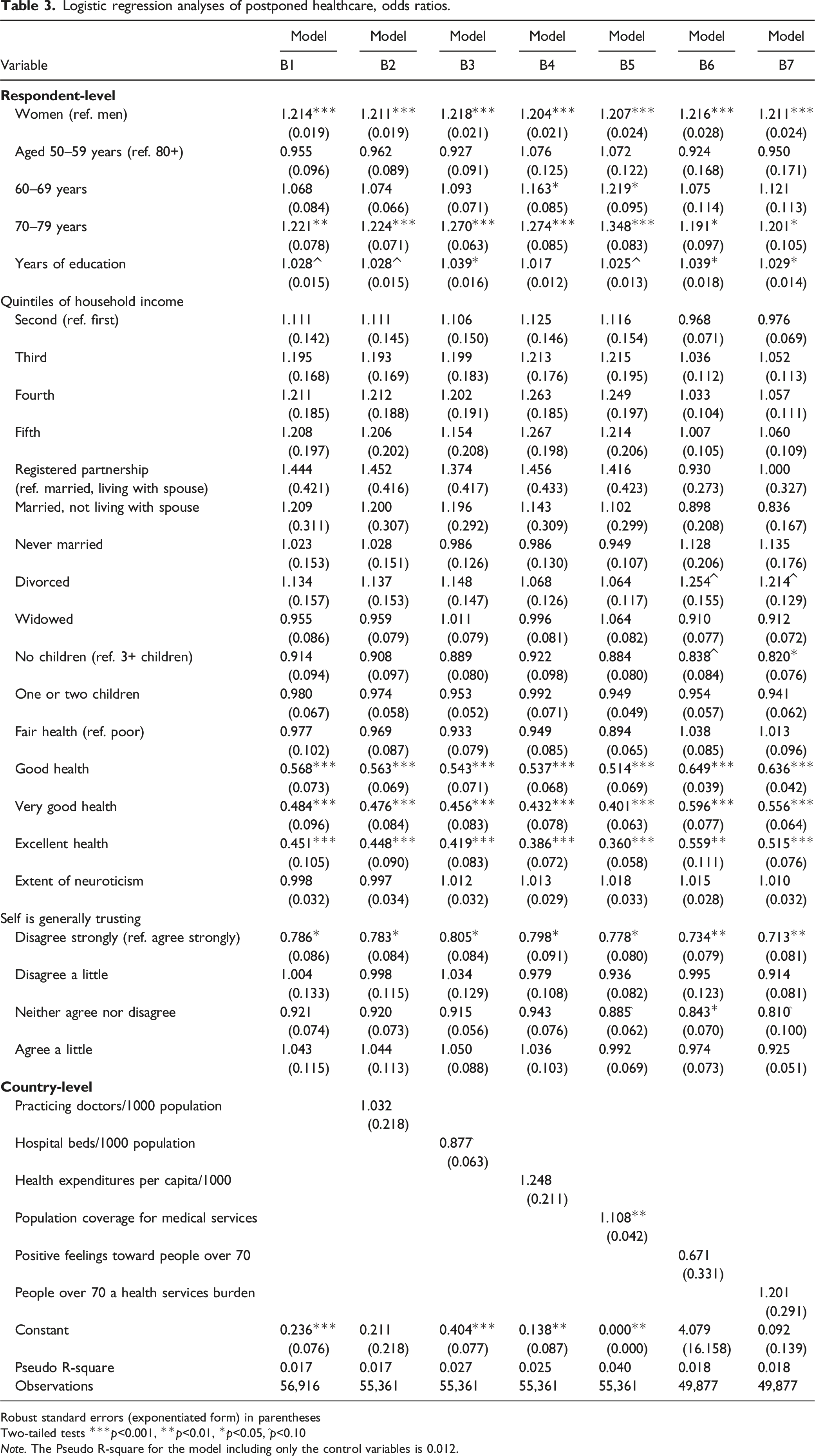
Robust standard errors (exponentiated form) in parentheses
Two-tailed tests ***p<0.001, **p<0.01, *p<0.05, ^p<0.10
Note. The Pseudo R-square for the model including only the control variables is 0.012.
Logistic regression analyses of denied healthcare, odds ratios.
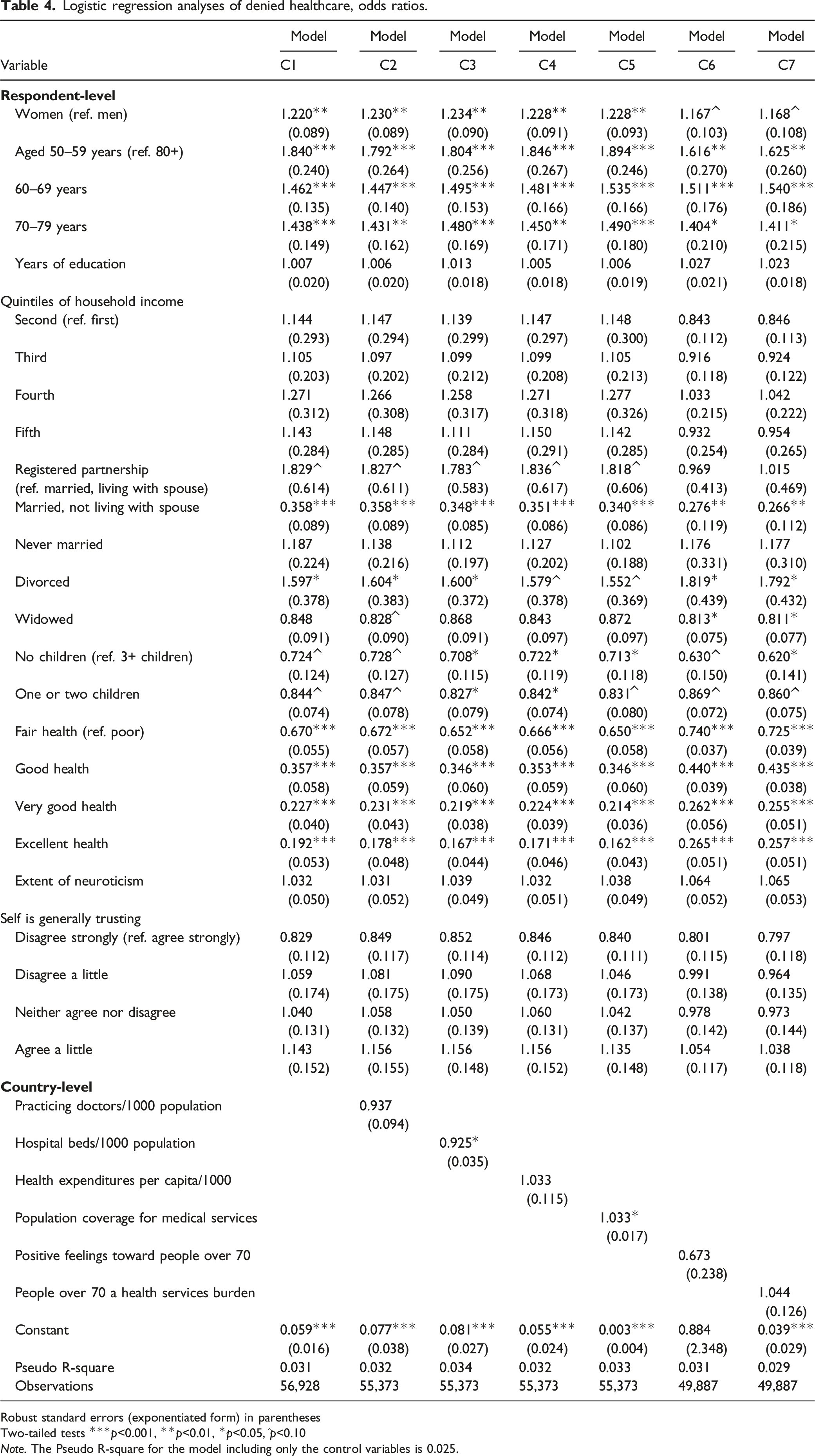
Robust standard errors (exponentiated form) in parentheses
Two-tailed tests ***p<0.001, **p<0.01, *p<0.05, ^p<0.10
Note. The Pseudo R-square for the model including only the control variables is 0.025.
Across all seven models of Table 2 (forgone healthcare), women were more likely than men were (Model A1 OR: 1.41, SE: 0.15) to report forgone healthcare. In Models A1 through A5, those of 70–79 years of age were more likely than those of 80 years of age and older were (Model A1 OR: 1.20, SE: 0.09) to report having had forgone a medical appointment or treatment. More years of education increased the likelihood of forgone healthcare in Models A2, A3, A6, and A7 (Model A2 OR: 1.04, SE: 0.02). It is plausible that the country-level variables within these four models differentially affected respondents of differing levels of education, masking the effects of education within the other models. Household income quintiles were insignificantly associated with likelihood of forgone healthcare. In Models A3 through A7, extent of neuroticism was significantly associated with higher probability of forgone healthcare (Model A3 OR: 1.12, SE: 0.06).
Model A2 shows that more practicing doctors per 1000 population increased the probability of forgone healthcare (OR: 1.37, SE: 0.14). However, Model A3 reveals that number of hospital beds per 1000 population had no significant relationship with this probability. Higher health expenditures per capita (divided by 1000) (Model A4 OR: 1.27, SE: 0.11) and population coverage for a core set of medical services (Model A5 OR: 1.09, SE: 0.03) were both positively associated with forgone healthcare. Model A6 shows no significant relationship between country-level extent of positive feelings toward people over 70 years of age and likelihood of forgone healthcare. However, Model A7 reveals that higher country-level extent of viewing persons over 70 years of age as burdens on health services increased this likelihood (OR: 1.74, SE: 0.18).
Table 3 displays ORs of predictors of postponed healthcare. Across all seven models, women were more likely than men were (Model B1 OR: 1.21, SE: 0.02) and those from 70 to 79 years of age showed higher probabilities than those of at least 80 years of age (Model B1 OR: 1.22, SE: 0.08) to have had postponed healthcare. In Models B3, B6, and B7, more years of education significantly increased the likelihood that one has had a postponed medical appointment or treatment (Model B3 OR: 1.04, SE: 0.02). As with forgone healthcare, characteristics of countries might have had contrasting effects upon respondents with differing extents of education, masking the impact of education within the remaining models. The seven models show quintiles of household income to have been insignificantly associated with postponed healthcare.
Among the country-level predictors, the only significant effect was population coverage for a core set of medical services increasing the likelihood of postponed healthcare (Model B5 OR: 1.11, SE: 0.04).
Table 4 displays the associations of the predictors with denied healthcare. In Models C1 through C5, women were significantly more likely to have had denied healthcare (Model C1 OR: 1.22, SE: 0.09). Across all seven models, younger age implied higher probabilities of denied healthcare (Model C1: 50–59 years OR: 1.84, SE: 0.24; 60–69 years OR: 1.46, SE: 0.14; 70–79 years OR: 1.44, SE: 0.15). All seven models show that neither years of education nor household income quintiles were significantly associated with denied healthcare.
Model C3 reveals that more hospital beds per 1000 population significantly reduced the likelihood of having had denied healthcare (OR: 0.93, SE: 0.04); likelihood of postponed healthcare was only marginally significantly (p<0.10) reduced by more hospital beds per 1000 population (see Model B3 in Table 3: OR: 0.88, SE: 0.06). Model C5 shows that higher population coverage for a core set of medical services increased the probability of having had denied healthcare (OR: 1.03, SE: 0.02).
Tables 2–4 all show worse self-perceived health increasing the probability of missed healthcare. Additionally, Table 2 reveals that higher extents of neuroticism raise the likelihood of foregone healthcare.
These three tables further include the pseudo R-square scores for each model. Rather than denoting the proportion of the variance that is explained, pseudo R-square scores indicate the extent to which one model more effectively predicts a dependent variable than a comparison model (Hemmert et al., 2018). The pseudo R-square scores within all three tables reveal that this study’s independent variables extend substantially beyond the control variables in predicting the three dependent variables.
Supplementary Analyses
Table S1 presents descriptive statistics showing percentages of all three types of missed healthcare by country. Prevalence of missed healthcare by country differed by type. The highest prevalences of forgone healthcare were found in Czech Republic, Greece, Israel, and Luxembourg (all prevalences between 17.2% and 21.4%). Prevalences of postponed healthcare were much higher and most extensive in Belgium, Czech Republic, Luxembourg, Malta, the Netherlands, and Portugal (prevalences between 35.2% and 50.7%). Prevalences of denied healthcare were lowest across the countries (most prevalences below 5%) and only higher than 5% in Belgium (7.1%), Estonia (6.9%), France (10.0%), Italy (6.1%), Latvia (7.6%), Lithuania (12.0%), Luxembourg (7.0%), Poland (6.9%), Portugal (7.1%), and Slovakia (5.5%).
Table S2 presents the bivariate associations between the individual- and country-level independent variables and the three outcomes. Women were significantly more likely to have reported all three types of missed healthcare (forgone: OR: 1.42, SE: 0.15; postponed: OR: 1.16, SE: 0.02; denied: OR: 1.20, SE: 0.09). Those who were 70–79 years of age showed significantly higher likelihoods of postponed healthcare than those of at least 80 years of age (OR: 1.17, SE: 0.06). Within this older sample, younger age was significantly associated with more denied healthcare (50–59 years of age: OR: 1.37, SE: 0.14; 60–69 years of age: OR: 1.16, SE: 0.19; 70–79 years of age: OR: 1.28, SE: 0.15). More practicing doctors per 1000 population (OR: 1.34, SE: 0.14), higher health expenditures per capita (OR: 1.24, SE: 0.12), higher population coverage for medical services (OR: 1.08, SE: 0.03), and stronger views of people over 70 as a health services burden (OR: 1.79, SE: 0.19) were all significantly associated with higher likelihood of having had forgone healthcare. Higher population coverage for medical services was also significantly associated with a higher probability of having had postponed healthcare (OR: 1.10, SE: 0.04).
The predicted percentages of the three types of missed healthcare (developed through Stata’s “margins” command) revealed in Table S3 show that the above discussed significant effects are of substantial magnitude. Prevalence of missed healthcare differed most prominently between men and women, and mainly for forgone and postponed healthcare (differences of 3 percentage points to the disadvantage of women), but less for denied healthcare (difference of less than one percentage point, also to the disadvantage of women). Respondents aged 70–79 years had more healthcare forgone and postponed than respondents of other age groups; concerning postponed healthcare, the biggest difference was in comparison with respondents aged 50–59 years (4.1 percentage points). Rates of denied healthcare were higher at younger ages (50–59 years of age: 5.7%, 80+ years of age: 3.2%). Higher-educated respondents reported substantially higher frequencies of forgone and postponed healthcare (4 and 5 percentage points differences between the 10th and 90th percentiles, respectively), while frequencies for denied healthcare were more equal across educational levels.
Concerning numbers of practicing doctors per 1000 population, the difference between the 10th and 90th percentiles is most striking for forgone healthcare, with the former being 6.7 percentage points lower than the latter. While the corresponding difference for postponed healthcare is 1.2 percentage points, that for denied healthcare is in the opposite direction and less than 1 percentage point. Regarding numbers of hospital beds per 1000 population, while for forgone healthcare the difference between the 10th and 90th percentiles is less than one percentage point higher in the former, the corresponding difference for postponed healthcare is 9.2 percentage points, and that for denied healthcare is 1.4 percentage points.
Higher health expenditures per capita increased rates of all three types of missed healthcare (somewhat less of an increase for denied healthcare), with the differences between the 10th and 90th percentiles being 5.7 percentage points for forgone healthcare, 9.7 percentage points for postponed healthcare, and 0.4 percentage points for denied healthcare. Higher population coverage for a core set of medical services also increased all three types of missed healthcare. Differences between the 10th percentile and the median and above were 5.0 percentage points for forgone healthcare, 11.1 percentage points for postponed healthcare, and 1.0 percentage points for denied healthcare.
While increasing all three types of missed healthcare, views of people over 70 as a health services burden most affected forgone healthcare, with the difference between the 10th and 90th percentiles being 8.8 percentage points. The corresponding difference for postponed healthcare was 5.7 percentage points, and that for denied healthcare was less than half of a percentage point.
Robustness checks further controlled for whether or not a respondent (0.48% of the sample) and whether or not someone close to a respondent (7.11% of the sample) had ever tested positive for COVID-19 infection. The result patterns were substantively the same with these additional controls.
Table S4 displays only those interactions between age and country-level ageism, as well as country-level medical resources, that significantly contributed to model fit (according to F-tests, at least at p < 0.05) within their separate models. The results show that respondents of at least 80 years of age are significantly more likely to have had forgone healthcare when general society-wide positive feelings toward older persons are higher. When society-wide views of older persons as a health services burden are stronger, the younger segments of the older population show increased likelihoods of postponed healthcare. More hospital beds per 1000 population most reduces postponed healthcare among those of at least 80 years of age. The age group of 70–79 years stands out as least affected by societal views of older persons as a health services burden in increasing rates of denied healthcare.
The results were substantively the same when analyses were repeated with the exclusion of Israel.
Analyses of how regions of Europe predicted rates of missed healthcare (Table S5) reveal no significant differences regarding postponed healthcare. However, Western Europe stands out as having higher rates of forgone healthcare and Southern Europe is distinct in its higher rates of denied healthcare.
Discussion
Quantity and quality of healthcare are important determinants of health, especially in later life. Our study aimed at thoroughly investigating individual- and country-level predictors of various types of missed healthcare during the COVID-19 pandemic. We find that prevalence of denied healthcare was quite small. This indicates that in Europe up to late summer 2020, in few countries or regions healthcare services were effectively overburdened and denied to those who actively sought them. However, prevalences of forgone and postponed healthcare appointments across Europe were substantial.
Individual-Level Predictors
In accordance with earlier studies on sex differences in later life healthcare needs and use, and risk perception (Cameron et al., 2010; Dryhurst et al., 2020; Lu et al., 2021; Rana et al., 2021), we found that women respondents were more likely to report forgone, postponed, or denied healthcare. The fact that the bivariate and multivariate results reveal these significant relationships emphasizes their robustness. These findings across all three types of missed healthcare are especially worrying given evidence that many older women underuse medical services when compared with their actual needs (Cameron et al., 2010).
Respondents from 70 to 79 years of age were the most likely to have had forgone and postponed medical appointments and treatments. Those from 70 to 79 years of age might have been at a nexus of anxiety concerning COVID-19 infection and perceived severity of health concerns that made them most likely to forgo or agree with the postponement of healthcare services.
In contrast, more advanced age was negatively associated with denied medical appointments and treatments. While this could be due to confounding between age and the severity of the health problem for which medical care was sought (more severe medical problems are less likely to be denied treatment), one should note that the SHARE is not necessarily representative of very old adults (only 8.34% of this study’s sample were 85 years of age and older) and those living in institutions. One year into the pandemic, many countries had seen large numbers of older adults dying from COVID-19 disease, particularly nursing home residents and people living with dementia (Suárez-González et al., 2020). Our findings are thus representative of middle-aged and older community-dwelling adults who have not yet reached oldest-old age (≥85 years of age, see Lee et al., 2018).
There was evidence that more educated respondents had higher likelihoods of forgone and postponed healthcare, possibly because they more regularly sought medical care in pre-pandemic times (Paccoud et al., 2020). This is associated with the fact that higher-educated persons may place higher value on high-quality medical care and personal health practices, and have higher medical literacy (Abel, 2008; Malat, 2006; Paccoud et al., 2020). During periods of restricted healthcare access, these characteristics may lead to higher rates of missed healthcare. Additionally, higher-educated persons might possess the cultural, social, and informational resources to acquire needed care through means other than formal medical institutions (Abel, 2008; Malat, 2006; Paccoud et al., 2020). Finally, they might be more aware of COVID-19-related pressures on healthcare systems, inclining them to agree with their medical appointments and treatments being postponed.
A potential explanation for the statistical insignificance of years of education within the bivariate analyses is based on the association of higher extents of education with better health (Mirowsky & Ross, 2005). This study has shown that the latter reduces likelihood of missed healthcare, and thus might constitute a suppressor effect. Controlling for health within the multivariate analyses thus reveals the effect that education has upon missed healthcare net of the effects of health.
Positive associations between worse self-perceived health and all three types of missed healthcare are likely because of greater medical needs, increasing the numbers of potential medical appointments and treatments that might be missed. This finding suggests, worryingly, that those individuals with the highest healthcare needs were also the most likely to suffer from missed healthcare. There is also evidence that higher neuroticism increases rates of forgone healthcare. This finding concords with research suggesting that individuals higher in neuroticism tend to seek out more medical appointments and visits (Hajek et al., 2017, 2020), raising the amounts of potential medical services that might be forgone. Furthermore, higher neuroticism might accentuate feelings of risk regarding potential COVID-19 infection, raising the probability that a medical service is forgone to avoid possible infection.
Country-Level Predictors
Investigating the role of healthcare systems’ availability and generosity, we find that in countries with higher numbers of practicing doctors per 1000 population and healthcare expenditures, rates of forgone healthcare were higher. We suggest that in these countries, larger rates of healthcare services use may have been for prevention (e.g., regular checkups). Respondents from these countries may have voluntarily refrained from using non-COVID-19 healthcare services for prevention, in line with public health messages. Higher population coverage for a core set of medical services was positively associated with all three types of missed healthcare. From a service provider perspective, this is possibly related to the necessity to limit medical services for non-COVID-19 healthcare. From a user perspective, this might be linked with individuals voluntarily refraining from medical services due to public health messages. Further, in countries with higher health coverage, stronger containment policies may have led to higher rates of postponed healthcare, as revealed within the countries that were EU members since before 2004 (Smolić et al., 2021). Higher numbers of hospital beds per 1000 population predicted less denied healthcare. This suggests that higher hospital capacity buffered increased demands due to COVID-19 patients and expanded sanitary measures for a broad range of healthcare services, even if there is evidence that waiting times for surgeries increased during the pandemic (OECD/European Union, 2020).
Investigating the role of country-level old-age ageism, we find that more negative general old-age ageism on a population level did not increase rates of any of the three types of missed healthcare, neither within the entire sample nor within any specific age group. This provides reassurance that societal negative views toward older people were likely not reducing their receipt of healthcare. However, stronger views of older people as a burden for health services on a population level were positively associated with forgone healthcare. This suggests that in countries with negative views of older people consuming healthcare resources, older individuals may have internalized these negative views (Weiss & Kornadt, 2018), increasing their likelihood of forgoing healthcare in the pandemic setting with perceived scarce healthcare resources. While some significant interactions were found between population-level views of older people as a burden for health services and age (discussed below), neither within the entire sample nor within any specific age group were there any significant links between these views and postponed or denied healthcare. This suggests that service providers did not (systematically) increase barriers to healthcare use for older people during the pandemic in Europe, which is reassuring considering the very unequal policy responses in other countries (Ribeiro & Leist, 2020).
These are the country-level findings after numerous individual-level variables were controlled. As such, they display the effects of these country-level characteristics net of these individual-level variables. It is notable that the bivariate statistics reveal no country-level variables significantly affecting denied healthcare. It is possible that in contexts of higher population coverage for medical services, health tends to be higher (Witthayapipopsakul et al., 2019). Better health decreases likelihood of denied healthcare, thus potentially constituting a suppressor effect. Therefore, controlling for health in the multivariate analyses reveals a significant impact of population coverage for medical services upon denied healthcare. It is further possible that in contexts well-endowed with medical resources, including hospital beds, the typical respondent has higher levels of education, which increase likelihood of denied healthcare. Once again, a suppressor effect might explain why controlling for years of education in the multivariate analyses reveals amounts of hospital beds to significantly decrease likelihoods of denied healthcare.
Beyond statistical significance, the percentages presented in Table S3 reveal that these effects are of considerable magnitude.
Cross-Level Interactions
This study further tested moderation of the effects of age upon all three dependent variables by the country-level ageism and medical resources variables. Some significant interactions were revealed that add further nuance to our understandings of older persons’ missed healthcare during the COVID-19 pandemic.
Society-wide positive feelings toward people over 70 did the most to increase rates of forgone healthcare within the oldest age group (80+ years). It is plausible that within environments characterized by high amounts of these positive feelings, the oldest persons are more optimistic about their health, and thus see their own health problems as less severe. In combination with their greater vulnerability to severe COVID-19 morbidity, this might further incline them to forego healthcare to avoid possible infection.
Our results further show that the younger segments of the older population show the strongest increases in postponed healthcare when views of older persons as a burden on health services are more prevalent. For the oldest age group (80+ years), generally increased health concerns might imply that decisions to postpone medical appointments and treatments are less affected by these societal biases. For the younger segments of older adults, with somewhat lesser health concerns, these postponement decisions might be more affected by these societal biases.
Additionally, more hospital beds per 1000 population had the strongest impact upon reducing postponed healthcare among respondents of 80 years of age and older. Treatment of older age groups might be more resource-intensive. As such, more hospital beds per 1000 population might do the most for preventing postponed healthcare within the oldest age group.
The final significant interaction showed that among those from 70 to 79 years of age, denied healthcare was least increased by society-wide views of older persons as a burden on health services. It is possible that for those from 50 to 59 years of age, health problems are seen as less severe, and so these societal biases might substantially increase their rates of denied healthcare. Plausibly, for those of at least 80 years of age, visits to the same doctors might be more frequent and for more minor concerns, raising likelihoods that these societal biases increase their rates of denied healthcare. Alternatively, for those of at least 80 years of age, health concerns might require more medical resources, accentuating how these societal biases increase their rates of denied healthcare. Those from 70 to 79 years of age might be at a nexus of severity of health problems, likelihood of visiting doctors for relatively minor concerns, tendencies to frequently visit the same doctors, and resources required for medical treatment that might make them least affected by these societal biases.
Policy Implications
To ensure greater medical system capacity that will reduce denied healthcare, future responses to large-scale medical crises will require greater investments in medical personnel and infrastructure to increase pandemic preparedness (Kuhlmann et al., 2021). These resources should be especially dedicated to segments of the population, such as older women and those in worse health, who are more likely to miss needed healthcare during an epidemic. In countries with more negative societal views of older people as burdens on health services, public health messages should convey the importance of healthcare visits for older adults. This will help ensure that (short-term) forgone healthcare during pandemic control measures does not raise older adults’ longer-term morbidity burden. As availability and generosity of healthcare services increased likelihoods of (voluntarily) forgoing healthcare, it seems important to offer health education to increase individual capacities to plan healthcare visits according to medical needs.
While our findings are relevant for all observed countries, our descriptive results within Table S1 and our analyses of regions of Europe within Table S5 suggest some geographical locations within which policymakers should be the most concerned about their older residents’ missed healthcare during the COVID-19 pandemic. Policymakers in the Czech Republic, Greece, Israel, and Luxembourg should be the most concerned about forgone healthcare. Those in Belgium, the Czech Republic, Luxembourg, Malta, the Netherlands, and Portugal should focus most on preventing postponed healthcare. Finally, policymakers in Belgium, Estonia, France, Italy, Latvia, Lithuania, Luxembourg, Poland, Portugal, and Slovakia should consider policies that will reduce rates of denied medical appointments and treatments.
There were no statistically significant differences among regions of Europe in postponed healthcare. However, there is reason to be concerned about denied healthcare in Southern Europe. Furthermore, policymakers in Western Europe should be aware of high rates of forgone healthcare as this may lead to accumulation of medical issues and possibly more severe disease stages when presenting to the doctor for the first time.
Strengths, Limitations, and Paths for Future Research
The harmonized SHARE design allowed us to investigate country-level predictors of missed healthcare in a large sample of diverse European countries. Our findings held after controlling for individual-level self-perceived health, extent of neuroticism, and general trust (among other variables), three variables that influence actual and perceived need for healthcare.
Data limitations prevent us from knowing the full circumstances of and reasons for missed healthcare, that is, if general lockdown measures or healthcare systems’ prioritization rules prevented healthcare access. These limitations also make it difficult to compare missed healthcare to the pre-pandemic levels of healthcare services use. For example, in a case where curative care was sought, no information is provided on the nature and severity of the medical problem.
Both individual-level and structural ageism have so far not received the empirical research attention they deserve (Wilson et al., 2019). Scholarship has emphasized the general stability of society-wide ageist views through time (see Abrams et al., 2015; Azulai, 2014). Specifically, a systematic review of how ageism affects older adults’ health based on studies from 1970 to 2017 crossing 45 countries (including many European nations) found that increasing effects of ageism through time were largely due to structural ageism, including among medical professionals (Chang et al., 2020). While this evidence supports our use of the only available European ageism data from 2008, which are at the more stable individual level, more up-to-date country-level ageism data would be preferred. This lack of more recent European ageism data is a limitation of our study. Indeed, we second the call for more systematic, harmonized, comparative assessments of ageism (Ayalon et al., 2019; Wilson et al., 2019).
Future research should investigate how COVID-19 (and future epidemics) affected older adults living within institutional settings (beyond the community-dwelling population). These individuals form an important population that was especially vulnerable to COVID-19 infection and subsequent health complications (Leontowitsch et al., 2021; Numbers & Brodaty, 2021). Additionally, future research should study the specific health consequences of these various types of missed healthcare.
Conclusion
During a medical crisis, such as the COVID-19 pandemic, it is not only those directly affected, such as those infected, who suffer negative consequences. Indirect effects, such as medical appointments and treatments missed for various reasons, are also consequential. Indirect effects such as these should receive further research and policy attention.
Supplemental Material
Supplemental Material - The Role of Country-Level Availability and Generosity of Healthcare Services, and Old-Age Ageism for Missed Healthcare during the COVID-19 Pandemic Control Measures in Europe
Supplemental Material for “The Role of Country-Level Availability and Generosity of Healthcare Services, and Old-Age Ageism for Missed Healthcare during the COVID-19 Pandemic Control Measures in Europe by Jason Settels, and Anja K. Leist in Journal of Aging and Health
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Faculty of Humanities, Education and Social Sciences, University of Luxembourg (2020 Research Block Grant Allocation Scheme–Merit Based Funding Scheme: Incentive B) to [J.S.]. This funding source had no involvement in study design; in the collection, analysis and interpretation of data; in the writing of the article; and in the decision to submit it for publication.
Data Availability
This paper uses data from SHARE Waves 6, 7, and 8 (DOIs: 10.6103/SHARE.w6.800, 10.6103/SHARE.w7.800, 10.6103/SHARE.w8.800), see Börsch-Supan et al. (2013) for methodological details. The SHARE data collection has been funded by the European Commission, DG RTD through FP5 (QLK6-CT-2001–00360), FP6 (SHARE-I3: RII-CT-2006–062193, COMPARE: CIT5-CT-2005–028857, SHARELIFE: CIT4-CT-2006–028812), FP7 (SHARE-PREP: GA N°211909, SHARE-LEAP: GA N°227822, SHARE M4: GA N°261982, DASISH: GA N°283646) and Horizon 2020 (SHARE-DEV3: GA N°676536, SHARE-COHESION: GA N°870628, SERISS: GA N°654221, SSHOC: GA N°823782, SHARE-COVID19: GA N°101015924) and by DG Employment, Social Affairs & Inclusion through VS 2015/0195, VS 2016/0135, VS 2018/0285, VS 2019/0332, and VS 2020/0313. Additional funding from the German Ministry of Education and Research, the Max Planck Society for the Advancement of Science, the U.S. National Institute on Aging (U01_AG09740-13S2, P01_AG005842, P01_AG08291, P30_AG12815, R21_AG025169, Y1-AG-4553–01, IAG_BSR06-11, OGHA_04-064, HHSN271201300071C, RAG052527A) and from various national funding sources is gratefully acknowledged (see ![]() ). This paper uses data from the generated easySHARE data set (DOI: 10.6103/SHARE.easy.800), see Gruber et al. (2014) for methodological details. The easySHARE release 8.0.0 is based on SHARE Waves 1, 2, 3, 4, 5, 6, 7 and 8 (DOIs: 10.6103/SHARE.w1.800, 10.6103/SHARE.w2.800, 10.6103/SHARE.w3.800, 10.6103/SHARE.w4.800, 10.6103/SHARE.w5.800, 10.6103/SHARE.w6.800, 10.6103/SHARE.w7.800, 10.6103/SHARE.w8.800).
). This paper uses data from the generated easySHARE data set (DOI: 10.6103/SHARE.easy.800), see Gruber et al. (2014) for methodological details. The easySHARE release 8.0.0 is based on SHARE Waves 1, 2, 3, 4, 5, 6, 7 and 8 (DOIs: 10.6103/SHARE.w1.800, 10.6103/SHARE.w2.800, 10.6103/SHARE.w3.800, 10.6103/SHARE.w4.800, 10.6103/SHARE.w5.800, 10.6103/SHARE.w6.800, 10.6103/SHARE.w7.800, 10.6103/SHARE.w8.800).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.