
Abstract
Cardiovascular disease remains the leading cause of noncommunicable mortality globally, with aortic valve (AV) disorders, especially aortic stenosis (AS), representing a substantial burden. Transcatheter aortic valve implantation (TAVI) is an effective treatment for AS, where selecting the correct valve size is crucial and preimplantation mechanical assessment is desirable to predict possible complications that may occur post-TAVI. Finite-element analysis (FEA) is a powerful technique for predicting wall stresses, such as contact pressure and von Mises stresses. Predicting post-TAVI complications such as conduction abnormalities and paravalvular leakage is challenging. FEA is useful for that purpose, but it is technically demanding and time-consuming. This study introduces a deep learning (DL) approach to efficiently predict patient-specific aortic wall stresses for the TAVI procedure. We collaborated with Hamad Heart Hospital’s TAVI program, analyzing computed tomography (CT) data and implanted valve information from 55 patients. We conducted FEA for virtual implantation simulations to derive contact pressures and von Mises stresses. Using a graph neural network model that features SageConv and SplineConv layers within a Geometric PointNet architecture, we trained on data that included the actual implanted valve size and simulations with marginally smaller and larger sizes on the same patients to enhance training variability. Our model achieved a normalized mean squared error of 0.0020 for contact pressure and 0.0057 for von Mises stress predictions. Integrating the pre-TAVI aortic geometry with FEA results significantly improved prediction accuracy for contact pressure, though alignment of von Mises stress predictions was occasionally inconsistent.
This is a visual representation of the abstract.
Keywords
Key Points
Generated a 3D patient-specific dataset from CT scans and FEA for TAVI analysis. Developed a GNN-based method for predicting patient-specific TAVI outcomes. Compared three approaches to evaluate the effect of the geometric contact point. Qualitative results shown for different patients and stent size variations.
Introduction
Over the last two decades, cardiovascular disease (CVD) has become the major cause of global noncommunicable disease-related mortalities, accounting for more than half of all mortalities.1,2 Heart valve defects, particularly aortic valve (AV) abnormalities, are among the most common CVDs. AV, which regulates the flow of oxygenated blood from the left ventricle into the aorta, is subject to complex mechanical stresses and is vulnerable to various diseases, including congenital problems such as a bicuspid aortic valve and acquired disorders like valve calcification. The prevalence of AV abnormalities increases with age, affecting more than 3% of the population over 65.3,4 These abnormalities may cause aortic stenosis (AS), which is the narrowing of the AV during systole, increasing the pressure load of the heart and heart failure risk.
A nonfunctioning AV can be treated or replaced via surgery. Alternative to surgical aortic valve replacement (SAVR), transcatheter aortic valve implantation (TAVI) was introduced in the early 2000s, transforming the treatment for severe AS.5,6 TAVI involves guiding a crimped valve via a catheter through a major artery and its deployment within the native valve.7,8 Historically, SAVR has been the primary treatment for severe AS. However, SAVR requires invasive open-heart surgery, with considerable risks, especially for older or high-risk patients who may experience lengthy recovery times and secondary complications.9–11 Randomized controlled studies have indicated that TAVI improves survival rates and provides positive long-term results for patients with severe AS.12,13 Hence, several guidelines now recommend TAVI as a treatment option for selected high-risk AS patients.14,15 As a less invasive procedure, TAVI has significant benefits over open-heart surgery, including shorter hospital stays, faster recovery periods, and lower surgical risks. TAVI was formerly designated for patients with high surgical risk, but its benefits have led to its recommendation for lower-risk categories as well.16,17 This has resulted in a substantial increase in a global number of TAVI procedures, with an estimated 98 500 TAVI treatments conducted in the United States alone in 2022.18,19
Despite these advantages, TAVI still may be associated with complications for patients, such as paravalvular leakage between the implanted valve and native valve, valve migration, and conduction abnormalities.20,21 For a successful TAVI procedure, the implanted valve must achieve adequate anchoring to prevent migration and paravalvular leakage (associated with undersizing the valve) while avoiding excessive mechanical stress on the annulus that may lead to conduction abnormalities (associated with oversizing the valve). Hence a reliable patient-specific mechanical assessment for the interaction of the transcatheter aortic valve (TAV) with the aortic wall is needed, and it may be used to predict possible complications. Finite-element analysis (FEA) is a very useful approach for virtual TAVI surgery in a patient-specific manner at a preoperative stage. This technique can be used to assess different TAVs for a specific patient to identify the optimal valve with improved outcomes. 22 Several mechanical stress parameters such as contact pressure from TAV stent on the aortic wall and von Mises stresses on the aortic wall can be calculated with this analysis. 23 Contact pressure and von Mises stress are key biomechanical indicators of stent–tissue interaction during TAVI. Excessively low contact pressure may result in inadequate anchoring of the prosthetic valve, increasing the risk of paravalvular leakage or valve migration, whereas excessively high contact pressure may lead to conduction abnormalities due to compression of the conduction system or even annular or aortic root injury. Similarly, elevated von Mises stress concentrations in the aortic wall may indicate regions at higher risk of tissue damage or rupture. 22 These stresses should not be too low so that the TAV stent attaches appropriately on the wall, but also should not be too high not to induce conduction abnormalities.24,25 Although such an approach offers insightful analysis, FEA requires extensive efforts for model preparations and simulations making it impractical for clinical use.26,27
Recently, deep learning (DL) models have been applied to biomedical research, including FEA studies, to expedite such analysis. 28 Particularly graph neural networks (GNNs) are suitable for this use since these models can manage graph-structured data, such as complex three-dimensional (3D) blood vessels, aortic root in the case of TAVI. GNNs excel in simulating spatial linkages and dependencies inside intricate architectures making them ideal for capturing the particular wall stress patterns linked with patient-specific anatomies. 29 Therefore, GNNs can potentially improve preoperative planning for TAVI operations by enabling the accurate prediction of mechanical stresses otherwise needs to be obtained from cumbersome FEA. In this investigation, we collaborated with Hamad Heart Hospital TAVI program to access CT images and implanted TAV information for 55 patients. This program is an established program with excellent success rates. 30 These patients were implanted with a self-expandable Medtronic Evolut valve as the most common valve type in that program. FEA was adapted to virtually simulate complete TAVI including valve crimping and deployment steps according to our previous protocols. 31 For each patient case, we first run FEA for the actual implanted valve size. For each patient, we also simulated a smaller valve and a bigger valve scenario. From the simulations, we calculated aortic wall contact pressure and von Mises stress profiles, and these were used as the ground truth for the DL models as well as for training of these models. The simulated data went through a series of preprocessing steps to test different approaches for the training of GNN models. This step involved challenges because of the variabilities in aortic geometries among patients, resulting in different numbers of analysis nodes. In order to overcome these challenges, we proposed and assessed various modeling methodologies, and compared their predictions with the FEA results. We believe our work will contribute to the DL research area by expediting FEA for accurate mechanical assessment of stent–tissue interactions. The key contributions of this study are as follows:
Development of a patient-specific TAVI dataset using 3D aorta geometries and FEA simulations to generate aortic wall stress. Implementation of GNN models with SageConv and SplineConv layers to handle variable geometry complexities in TAVI aortic wall stress prediction. Qualitative evaluation demonstrating the model’s capacity to predict patient-specific aortic wall stress across different stent sizes.
The remaining part of the manuscript is organized as follows: The Methodology section includes a comprehensive discussion of the methods and materials, detailing the dataset overview, data generation, data preparation for model training, DL algorithms and training approaches, and the evaluation metrics used for the performance evaluation. Experimental results section provides the experimental results, including the quantitative and qualitative results. The Discussion section provides an overall discussion and limitations of our work. Finally, in the conclusion section, we conclude with the discussion of our work and discuss the future research directions.
Methodology
In this section, we highlight the primary procedures associated with the development of datasets through the use of FEA, followed by data preparation procedures for DL. We subsequently explain the architecture, complexity, and methodological foundations of the DL algorithms employed to predict patient-specific aortic wall stress profiles. Furthermore, we detail the quantitative and qualitative metrics that are employed to assess the performance of the model. Lastly, Figure 1 illustrates the comprehensive overview of the methodology to ensure clarity.

Overall overview of the methodology. (a) Approach 1: the stresses are predicted from pre-TAVI geometries of aorta and stent, (b) Approach 2: the stresses are predicted from pre-TAVI geometries and their intersecting points, and (c) Approach 3: the stresses are predicted from post-TAVI geometries and their intersecting points. The post-TAVI contact pressure and von Mises stress contours shown are identical across all approaches, as they represent the FEA ground truth. TAVI = transcatheter aortic valve implantation.
Finite-Element Analysis
FEA involves the simulation of the complete TAVI procedure, including crimping the TAV and deployment inside the patient-specific 3D aortic annulus geometry with native valves. This procedure is explained in our previous paper in detail 31 and is briefly summarized here.
Computed tomography (CT) images from TAVI patients were collected from Hamad Medical Corporation Heart Hospital in Doha, Qatar. The aortic root regions were segmented and cropped from the original geometry using 3D Slicer (version 5.2.1, Slicer Community) and reconstructed using Mesh Mixer (version 3.5, Autodesk, Inc). The CT images used for reconstruction correspond to a single acquisition phase, and phase-specific variations across the cardiac cycle were not explicitly modeled in this study. In addition, calcific deposits were not explicitly segmented as separate structures, and their effects are implicitly represented within the reconstructed aortic geometry. Since CT images do not fully capture native valve leaflets, a parametric approach was used to model them within the aortic root. Native leaflets with 0.5 mm thickness were created in SolidWorks (Dassault Systèmes, 2024) and positioned based on the aortic root diameter for each case. 32 Medtronic Evolut-R TAV geometries (23, 26, 29, and 34 mm) were designed in SolidWorks, including the stent, skirt, and prosthetic leaflets, using manufacturer-provided dimensions. For mesh optimization, a mesh convergence analysis was performed: the aortic root was meshed with two-dimensional first-order tetrahedral elements (maximum size: 0.6 mm), while the TAV and native valve leaflets were meshed with 3D first-order tetrahedral elements (maximum size: 0.4 mm). Meshes were generated using Altair HyperMesh (Hyperworks, 2011). The FEA solver used in this study was Abaqus (Dassault Systèmes, 2023). A quasi-static solver in Abaqus was used to simulate large deformations.
Material properties were assigned based on previous studies. The TAV stent was modeled as a superelastic Ni–Ti alloy with a Young’s modulus of 51 700 MPa. The aortic root (2 MPa), native valve leaflets (8 MPa), and prosthetic valve leaflets (1.1 MPa) were treated as linear elastic materials. The leaflets, skirt, and stent were defined as homogeneous solids, while the aortic root was modeled as a homogeneous shell with a 2 mm thickness. Contact conditions were applied using surface-to-surface tie constraints connecting the aorta, skirt, and leaflets. The aortic root was modeled using a shell representation to reduce computational cost while preserving the geometric conformity of the thin-walled structure. Linear elastic material properties were adopted based on commonly reported values in prior TAVI simulations, providing a simplified yet stable approximation for large-scale parametric analyses. While nonlinear behavior may affect stress magnitudes, the adopted assumptions are sufficient to capture the relative distribution of stress and contact pressure for the purposes of this study.
The FEA simulation was carried out in multiple stages. First, the TAV was crimped to catheter size. Then, it was positioned inside the native aortic valve and expanded during deployment. The prosthetic and native leaflets were aligned, and the TAV base was positioned 4 mm below the annulus plane. The simulation process followed the clinical TAVI procedure by dividing it into native valve opening, crimping, and deployment stages. The native valve leaflets were radially expanded to the crimping diameter. The crimped TAV was then removed from the crimper and placed inside the native aortic valve. Finally, an opener expanded the native leaflets to a slightly larger diameter than the crimped state. Following the FEA simulations in Abaqus, FEA results such as contact pressure and von Mises stress were extracted. Contour plots were generated for use in further DL analysis.
Study Cohort and Baseline Characteristic
We carried out this investigation under IRB ethical approval obtained from Hamad Medical Corporation, Heart Hospital (MRC-02-20-134). CT images of 55 patients who have received TAVI treatment at Hamad Heart Hospital were included in the study. The study population comprises 35 male patients and 20 female patients. The average ages are 73.9 and 72.7 years for male and female patients, respectively. The youngest and oldest patients in the male group are 51 and 93 years old, respectively. On the other hand, the youngest and oldest female patients are 61 and 89 years old respectively. Among the included cases, 25 were implemented with a 26 mm valve size, 23 with a 29 mm valve size, and 7 with a 34 mm valve size. Additional clinical characteristics such as valve morphology (eg, bicuspid or tricuspid), calcium severity, and comorbidities were not consistently available for all patients and were therefore not included in this study. The current dataset focuses primarily on patient-specific anatomical geometries and procedural configurations for biomechanical simulation.
FEA Dataset Description
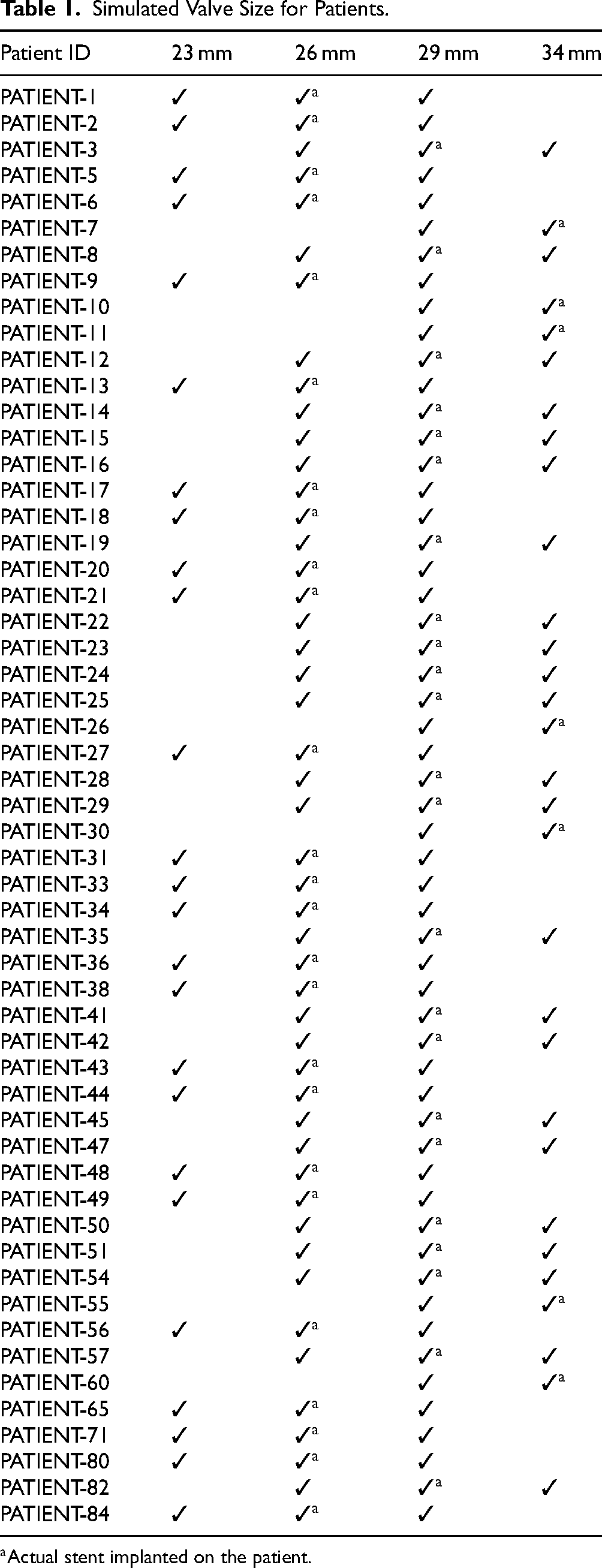
For each patient, we performed FEA for three conditions: a real implanted, a smaller, and a bigger Medtronic Evolut-R TAV. Therefore, three different virtual TAV implantation analyses were carried out for each patient-specific case except for patients with 34 mm TAV deployment since no bigger size was available than the 34 mm. As a result, for patients implanted with the largest available valve size (34 mm), only two simulation scenarios (smaller and actual size) were considered instead of three. This leads to a total of 157 samples rather than the theoretical maximum of 165. Table 1 summarizes each patient FEA case. With FEA, we generated post-TAVI 3D aortic annulus contact pressure and von Mises stress profiles for virtual implantations.
Simulated Valve Size for Patients.
Preparation of the DL Training Data
Analysis of Pre-TAVI and Post-TAVI Stent and Aorta Geometries
Using DL, we aim to predict post-TAVI 3D aortic wall contact pressure and von Mises stress profiles. Here, FEA stress profiles are used to train the DL model for accurate prediction. After the training, we would expect this model to predict the stress profiles with pre-TAVI information such as patient aorta geometries and selected TAV to be implanted. The major challenge in this approach is the deformation of the stent geometry and the aortic root geometry during FEA; therefore, pre-TAVI and post-TAVI geometries do not match exactly. Another challenge is the differences in node numbers in 3D aorta geometries from patient to patient. Each of these geometries contains tens of thousands of nodes, with a maximum of 32 000 nodes. However, once FEA contact pressure and von Mises stress profiles are carefully examined, we realize that only a few thousand nodes were producing significant results, particularly in the vicinity of the TAVI stent contact points on the aorta. Therefore, it seemed that it was possible to establish a direct correlation between post-TAVI FEA stress profiles and pre-TAVI initial aorta geometries by incorporating TAV stent geometries into the training, as this connection is crucial for the effective training of the DL models. To investigate these correlations further, a data preparation procedure was implemented, which comprised aligning the initial geometries of the aorta and the TAVI stents for each studied case, followed by identifying the prospective contact points. Upon examining prospective contact points, FEA contact points, and FEA stress profiles, we noted significant similarities in the patterns between the FEA profiles and the prospective contact points as well as the FEA contact points. This observation suggested that the performance of the DL models could be substantially improved by incorporating prospective contact point information in the training.
DL Model Training Dataset Generation
We analyzed three different approaches using three different datasets:
Approach 1: The first approach is based on generating a dataset with initial pre-TAVI aorta and TAV stent geometries and post-TAVI FEA contact pressure and von Mises stress profiles.
Approach 2: In the second approach, a dataset is generated as follows: in addition to initial pre-TAVI aorta geometries and post-TAVI FEA contact pressure and von Mises stress profiles, prospective contact points between the TAVI stent and the aorta geometries are added.
Approach 3: In the third approach, the dataset is generated with post-TAVI FEA contact pressure and von Mises stress profiles and post-TAVI FEA contact points between the TAVI stent and the aorta geometries.
It should be noted that Approach 3 utilizes post-TAVI information derived from FEA simulations and is therefore intended as an upper-bound performance reference rather than a clinically deployable solution. Experimental results present a comprehensive comparison of these datasets using a variety of evaluation metrics.
The data preparation procedures and the visual patterns of contact points, contact pressure, and von Mises stress are depicted in Figure 2. The procedure of measuring contact points from the initial geometries of the aorta and stent is illustrated in Figure 2(a). This entails the alignment of the two geometries, and the calculation of the corresponding contact point on the aorta for every point of the stent that is located outside the aorta. This information is used in Approach 2. In Figure 2(b), we demonstrate the measurement of contact points based on the final geometries of the aorta and stent. In this part, we align the final geometries and take each point on the aorta that is in contact with the stent as a contact point. We incorporated the measured contact points into the initial aorta geometry, as both the initial and final geometries have the same number of nodes and each node has a unique identifier. Lastly, Figure 2(c) illustrates the contact points from both the initial and final geometries, as well as the FEA outcomes of contact pressure and von Mises stress, which illustrate their similar patterns. This information is used in Approach 3.

Overall overview of data preparation. (a) Calculation of intersecting points from pre-TAVI aorta and stent geometries, (b) calculation of intersecting points from post-TAVI geometries, and (c) comparison of the intersecting points from the two approaches and FEA stress outcomes. TAVI = transcatheter aortic valve implantation.
Upon finalizing the data preparation, we extract the coordinates
Methodology and DL Algorithms
This study uses a methodological framework employing DL models to predict patient-specific outcomes, including von Mises stress and contact pressure, for TAVI operations. The procedure starts with building three separate datasets obtained from FEA simulations of 55 patient-specific aorta geometries and stent sizes (23, 26, 29, and 34 mm). These datasets comprise FEA results and pre-TAVI aortic geometry, each tailored to assess the model’s prediction capabilities under different configurations. In data preparation, the three datasets for the three approaches are described. To address the variability in the number of points or nodes across patient geometries, the study employs GNN models built with SageConv 33 and SplineConv 34 layers. The processing of nonuniform graph structures is particularly well-suited to these layers, which are integrated within a PointNet-inspired architecture. 35 By sampling neighbors and aggregating their features using methods such as mean, max, or long short-term memory-based aggregation, the SageConv layer from the GraphSAGE framework efficiently learns node embeddings. This layer is optimal for large and dynamic graphs due to its generalization capacity to invisible nodes or subgraphs. In contrast, the SplineConv layer employs B-spline basis functions to generate continuous convolutional kernels, which facilitates the extraction of features in a dynamic and adaptive manner across irregular geometries, such as 3D point clouds or meshes. By combining these layers, the GNN models are able to efficiently manage the intricate and variable geometries that are inherent in the TAVI dataset.
Traditional DL methods are modified by the Geometric PointNet 36 architecture to accommodate non-Euclidean data, including 3D polygonal structures. Geometric PointNet processes polygonal meshes directly, in contrast to conventional methods such as UV mapping and voxelization, which introduce distortions. It employs pseudo-coordinates based on Cartesian distances to capture spatial relationships between nodes and uses SplineConv to manage mesh data without requiring explicit correspondences. To learn local features, the architecture integrates sequential layers and aggregates them into global features through max-pooling. The model’s representation of mesh structures is enhanced by the inclusion of supplementary vertex features, including surface normals and curvature. The model is developed using PyTorch Geometric (PyG), a library for geometric deep learning. PyG converts the mesh data into graph representations, with vertices and edges serving as nodes and mesh faces, respectively. The architecture uses Adam optimizer with an optimized learning rate of 0.0001 and is tuned using dropout layers to avoid over-fitting. Different hidden channels (32, 64, and 128) were employed in experiments to optimize the efficacy of the SageConv and SplineConv layers. The Geometric PointNet architecture’s robustness and flexibility are assured by the combination of these layers and configurations, which enable the precise prediction of patient-specific outcomes, even in the presence of highly variable aortic geometries. This research emphasizes the benefits of integrating sophisticated GNN layers into predictive modeling for TAVI procedures. The proposed framework has the potential to significantly reduce computational time and resources compared to traditional FEA methods by refining the relationship between initial aortic geometries and FEA outcomes. The experimental results, which will be discussed in the subsequent sections, demonstrate the model’s performance and its ability to adapt to the complexities of patient-specific geometries and stress distributions.
Evaluation Metrics
We are training GNN models on various subsets of the TAVI dataset to predict patient-specific mechanical stress outcomes, which are von Mises stress and contact pressure. To thoroughly evaluate the models’ performance, we implement both quantitative and qualitative methodologies. For quantitative evaluation, we employ three important metrics: mean squared error (MSE), mean absolute error (MAE), and normalized mean squared error (NMSE). These metrics are essential for analyzing the predicted and actual outcomes, allowing us to identify the most effective model based on prediction precision. These evaluation metrics are mathematically expressed in equations (1) to (3)37,38:


In addition to these quantitative measures, qualitative evaluations are implemented to collect additional information about the model’s performance. The predicted contact pressure and von Mises stress are visualized using the PyVista plotter for each patient and stent size. This visualization enables us to directly compare the model’s predictions with the FEA results, providing a visual knowledge of the predicted mechanical outcomes’ alignment with the ground truth for different patient geometries and stent sizes. Additionally, we perform thorough comparisons between the GNN model’s predictions and the FEA-derived outcomes for each patient in the test set, utilizing a variety of stent diameters. Additionally, we offer the training curves for the GNN models, which serve to illustrate the learning behavior and convergence characteristics during the training process. These curves provide valuable insights into the model’s learning dynamics and the training process’s efficacy.
Experimental Setup
This study employed the DL algorithms and GNN models to train on the TAVI dataset, using the PyTorch and PyTorch Geometric framework. The training of these GNN models was conducted on a local server with a NVIDIA RTX 4090 graphics card with 24 GB GPU memory, an Intel Core i9 14th gen processor with 128 GB system memory. All investigations were done using Python 3.11.7 and PyTorch 2.5.0.
Experimental Results
This section presents the experimental findings of our DL models, emphasizing performance comparisons among several GNN architectures and their combinations. We assess these models in predicting patient-specific outcomes, including contact pressure and von Mises stress. Furthermore, we evaluate the three distinct ways previously described, assessing their impact on model performance and emphasizing the enhancements realized through each technique. The findings comprise both quantitative and qualitative assessments. We offer quantitative performance measures for every model and methodology, including MSE, MAE, and NMSE. We qualitatively assess the predictions of the top-performing model, demonstrating its efficacy in accurately predicting patient-specific outcomes. To maintain transparency, we provide essential performance measures with the relevant training curves for each model, facilitating a clear understanding of model convergence and generalization behavior.
Quantitative Results
We implemented DL-based GNN models to predict patient-specific FEA outcomes: von Mises stress and contact pressure across different stent sizes. The TAVI dataset contains FEA results for 55 patients and a total of 157 samples, including different stent sizes. To ensure proper evaluation of the model, the dataset is split into 80% for the training set and 10% each for the validation and test sets. The dataset split was performed at the patient level rather than the sample level, ensuring that all samples corresponding to a single patient (including different stent sizes) were included exclusively within a single subset (training, validation, or testing). This approach prevents data leakage and ensures a more reliable evaluation of the model’s generalization performance. To address the complexity given by different patient geometries and unique FEA outputs, we constructed GNN models with SageConv and SplineConv layers within a PointNet-inspired architecture, which is also known as Geometric PointNet. This method enabled us to handle nonuniform graph structures while effectively capturing spatial connections inside patient-specific geometries. We conducted experiments with various configurations, adjusting the number of layers and hidden channels to enhance the model’s performance. Table 2 shows the comparison findings for the contact pressure predictions across different setups.
To assess our models’ performance, we used quantitative metrics such as MSE, MAE, and NMSE. We trained models with 32, 64, and 128 hidden layers in both SageConv and SplineConv architectures to see how layer depth affected performance. The results show that adding more hidden layers increased model performance across both architectures. As demonstrated in Table 2, SplineConv with 128 hidden units produced the best results in predicting patient-specific outcomes. Table 2 reports the quantitative evaluation results for the best-performing configuration (Approach 3), which incorporates contact point information. The other approaches (Approaches 1 and 2) were evaluated comparatively and showed consistently lower performance. For contact pressure, the model has an MSE of 0.0321, MAE of 0.0671, and NMSE of 0.0020. In the case of von Mises stress, we found comparable high accuracy, with an MSE of 0.0512, MAE of 0.1488, and NMSE of 0.0057. These results highlight the model’s ability to capture complicated patient geometries and FEA outcomes. Despite the inherent obstacles posed by unique geometries and changing stent sizes, the models demonstrated good predictive power, with low error rates demonstrating the usefulness of the chosen GNN architectures for this patient-specific task.
Performance of GNN Models on Predicting Contact Pressure and von Mises Stress (MAE in MPa, MSE in MPa
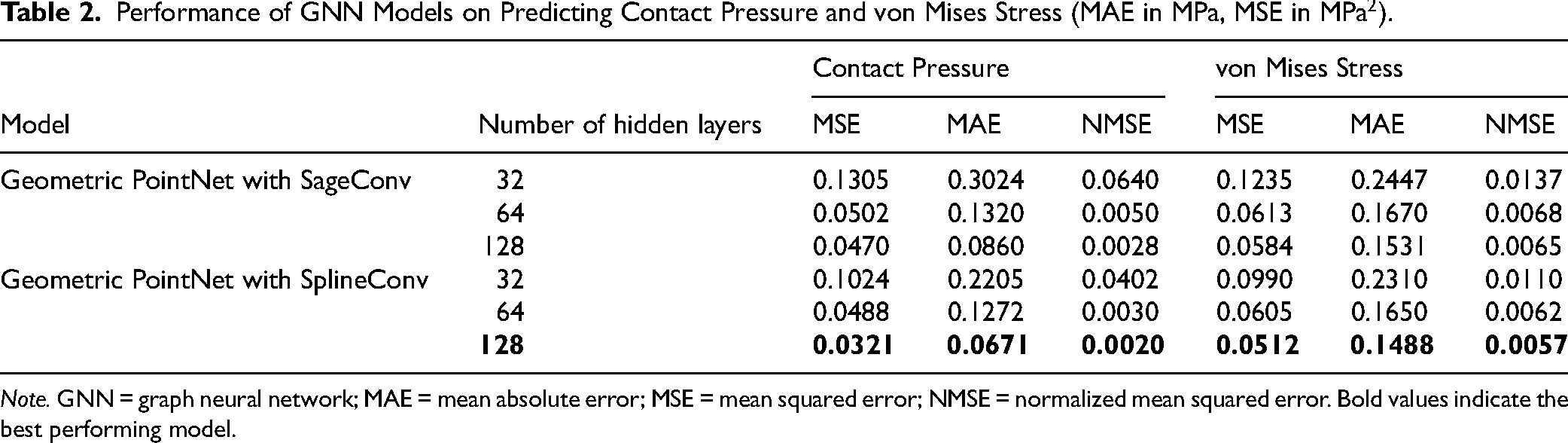
Note. GNN = graph neural network; MAE = mean absolute error; MSE = mean squared error; NMSE = normalized mean squared error. Bold values indicate the best performing model.
Qualitative Evaluation
Predicting patient-specific results such as contact pressure and von Mises stress is difficult due to the significant variation in aorta geometries between individuals. Furthermore, the exact points at which these outcomes appear are significantly fewer than the total number of points within each aorta. These factors challenge the prediction task, requiring a comprehensive qualitative assessment in addition to quantitative evaluation to gain a detailed understanding of the model’s performance. Here we provide a comparison of the three techniques for predicting patient-specific outcomes. For each example, model predictions are visually compared to FEA-derived ground truth, revealing the models’ accuracy and dependability across a wide range of patient geometries.
Figure 3 illustrates a qualitative comparison of the three prediction methodologies with the simulated results of FEA as ground truth. The initial method, which only uses the initial geometry of the aorta, shows limited performance in predicting contact pressure, particularly when the stent size changes. This method is unable to accurately capture the complexity of pressure changes caused by varying stent diameters in the absence of extra contextual data, resulting in substantial deviations from the FEA baseline. The predictive accuracy is significantly enhanced by the second approach, which incorporates contact points calculated from the initial geometries of the aorta and stent. In accordance with the FEA results, the model begins to respond more closely to stent size variations, as demonstrated in Figure 3. With the addition of contact points, the model is able to more effectively capture contact pressure variations by establishing critical spatial relationships. The third approach achieves the most accurate alignment with FEA-derived results, which includes contact points from the final geometries after FEA simulation. This method allows the model to precisely predict critical contact pressure changes, even in high-pressure regions, as stent sizes change. This enhanced predictive accuracy is the result of the significant relationship between the contact points extracted from the final geometry and the contact pressure nodes, as is explained in the data preparation section. The inclusion of these final contact sites provides the model with supplementary structural information, enabling it to more accurately approximate the patient-specific mechanical responses. This results in predictions that closely resemble the complex structures observed in the FEA simulation. Although Approach 3 demonstrates the highest accuracy, its reliance on post-TAVI information limits its direct clinical applicability, whereas Approach 2 provides a more practical trade-off between performance and usability.

Comparison of different approaches with FEA simulated ground truth of contact pressure. FEA = finite-element analysis.
For von Mises stress predictions, the FEA-simulated results vary significantly between patients and respond strongly to stent size variations. While the model may approach overall stress distribution patterns in some cases, it overstates stress levels in most cases when compared to the FEA-simulated ground truth. This disparity emphasizes the difficulty of accurately capturing biomechanical responses that are unique to each patient due to variations in anatomy and stent interactions. Among the three techniques used, using contact points generated from final geometries gave the best prediction for von Mises stress too. By utilizing the extra structural information given by the final geometry, our method brought the model closer to the actual stress distributions shown by the FEA findings. Figure 4 shows a thorough comparison of model predictions with FEA ground truth. This is not surprising as in the third approach, we are utilizing FEA-generated data to train the model. This approach is not directly clinically practical, as it requires FEA simulations; however, it provides important insight into the role of contact topology, which can guide the development of clinically feasible approximations based on preoperative data.

Comparison of different approaches with FEA simulated ground truth of von Mises stress. FEA = finite-element analysis.
Discussion
Findings from this study illustrate the performance of GNN models in predicting patient-specific mechanical stress outcomes for TAVI procedures, such as von Mises stress and contact pressure. By conducting FEA simulations with patient specific aortic root geometries, we have created a comprehensive TAVI dataset that represents various stent diameters and aortic geometries. With this dataset, we were able to investigate the predictive capabilities of various GNN models in managing the natural variation in patient-specific anatomy. Our results indicate that the model’s performance is considerably enhanced when contact points from the final geometries are taken into account, instead of solely relying on the initial geometries. This method improves the predictive accuracy of patient-specific stress distribution by capturing more detailed structural interactions between the stent and the aorta. While Approach 3, which incorporates contact points derived from post-TAVI FEA simulations, achieves the highest predictive accuracy, this approach is not directly applicable in clinical settings due to the requirement of performing FEA simulations. In contrast, Approaches 1 and 2 rely only on pre-TAVI geometries and geometrically derived contact point approximations, making them more suitable for preoperative use. These findings highlight an important distinction between scientific insight and clinical applicability. Specifically, the results demonstrate that contact topology plays a critical role in accurately predicting stress distributions, while clinically feasible models must rely solely on information available prior to intervention.
From a clinical perspective, the predicted contact pressure and von Mises stress distributions can provide meaningful insight into potential procedural risks. Regions with insufficient contact pressure may indicate a higher likelihood of paravalvular leakage or inadequate valve anchoring, whereas excessive contact pressure may be associated with conduction abnormalities due to compression of adjacent cardiac structures or increased risk of annular injury. Similarly, elevated von Mises stress concentrations may highlight regions susceptible to tissue damage or aortic root complications. Although universal threshold values remain patient-specific and dependent on anatomical variability, these predicted biomechanical patterns can be used comparatively to identify high-risk cases and support decision-making in valve sizing and positioning. Regarding the prediction error, although the MAE for von Mises stress appears relatively high compared to the maximum reported values, it should be noted that stress distributions are highly localized and vary significantly across patient-specific anatomies. Therefore, even with moderate absolute errors, the model is able to capture the overall spatial distribution and key high-stress regions, which are of primary clinical interest. From a clinical perspective, the relative distribution patterns and identification of critical regions are more relevant for risk assessment than exact point-wise agreement. In addition, predicted contact pressure distributions can support personalization of TAVI procedures by providing insight into optimal valve sizing and positioning to minimize risks such as paravalvular leakage and conduction abnormalities.
The models that used the SplineConv layer with more hidden units consistently outperformed the other architectures in terms of prediction performance. The SplineConv layer’s capacity to manage variable input size was crucial in precisely capturing mechanical stress outcomes across a range of stent sizes. We have achieved an impressive root mean square error (RMSE) of 0.0020 for contact pressure and RMSE of 0.0057 for von Mises stress prediction. In addition to predictive performance, the computational efficiency of the proposed framework offers a significant advantage over conventional FEA simulations. A typical patient-specific FEA workflow for TAVI, including geometry reconstruction, meshing, and simulation, may require several days to weeks depending on model complexity and computational resources. In contrast, once trained, the proposed GNN model can generate predictions within a few seconds for a new patient case. The data preparation stage, including geometry alignment and graph construction, is performed offline during model development, and subsequent inference remains computationally lightweight. Training the GNN model incurs a one-time computational cost on a high-performance GPU system; however, this cost is amortized across all future predictions. Among the three approaches, Approach 3 involves the highest initial cost due to reliance on post-FEA data, whereas Approach 2 provides a more practical balance between computational efficiency and clinical applicability.
From a broader perspective, the proposed GNN-based surrogate model can be viewed as a data-driven alternative to conventional simulation acceleration techniques used in TAVI planning. Unlike full-order FEA, which aims to capture detailed physics at high computational cost, the proposed model learns a direct mapping from patient-specific geometry to mechanical outcomes, enabling rapid prediction. In this context, the framework can serve as a fast screening tool to identify potentially high-risk cases, which may then be further analyzed using full FEA if required. Compared to physics-based reduced order models (ROMs), which preserve governing equations through dimensionality reduction, 39 the GNN approach does not explicitly enforce physical laws but instead leverages data to learn complex nonlinear relationships. This allows greater flexibility in handling highly variable patient-specific geometries, although it may require sufficient training data for generalization. Future work may explore hybrid approaches that integrate data-driven models with physics-based constraints, combining the efficiency of GNNs with the interpretability and robustness of ROM-based methods.
A Comparison with the Literature with GNN Applications
Recent studies have begun to explore the application of deep learning techniques in TAVI, particularly in areas such as outcome prediction, valve calcification quantification, and anatomical segmentation.40–42 However, the integration of advanced graph-based approaches, such as GNNs, remains largely unexplored, highlighting a significant gap in leveraging relational and structural information in TAVI-related modeling. Despite this, the potential of GNNs to enhance predictive modeling across various aspects of cardiovascular health is evident, as detailed in Table 3. Morales et al 36 and Gao et al 43 use GNNs for predicting thrombotic risks in the left atrial appendage, with Morales achieving an MAE of 0.521 using a Geometric PointNet, while Gao extends the model’s capability to predict multiple indices such as endothelial cell activation potential and time-averaged wall shear stress, illustrating GNNs’ versatility in handling complex biological data. Suk et al 44 apply the gauge-equivariant mesh graph convolutional network model to estimate Wall Shear Stress on coronary artery walls, achieving a median NMAE of 0.4%, which underscores the precision of GNNs in crucial flow dynamics predictions. Yao et al 45 demonstrate an integrated approach with the Image2Flow model, which not only segments pulmonary arteries but also calculates computational fluid dynamics (CFD) flow fields, achieving a Dice Score of 91% and an NMAE under 12% for CFD fields. In our contribution to this emerging field, we explore the application of the Geometric PointNet model for stress prediction in TAVI procedures, achieving exceptionally low NMAEs, thus emphasizing the significant potential for GNNs to support precise and effective intervention strategies. This broad array of applications showcases GNNs’ ability to revolutionize predictive modeling in biomedical engineering, enhancing diagnostic and prognostic accuracies within a clinical setting.
Comparison of GNN Models’ Performance on Different Fields.
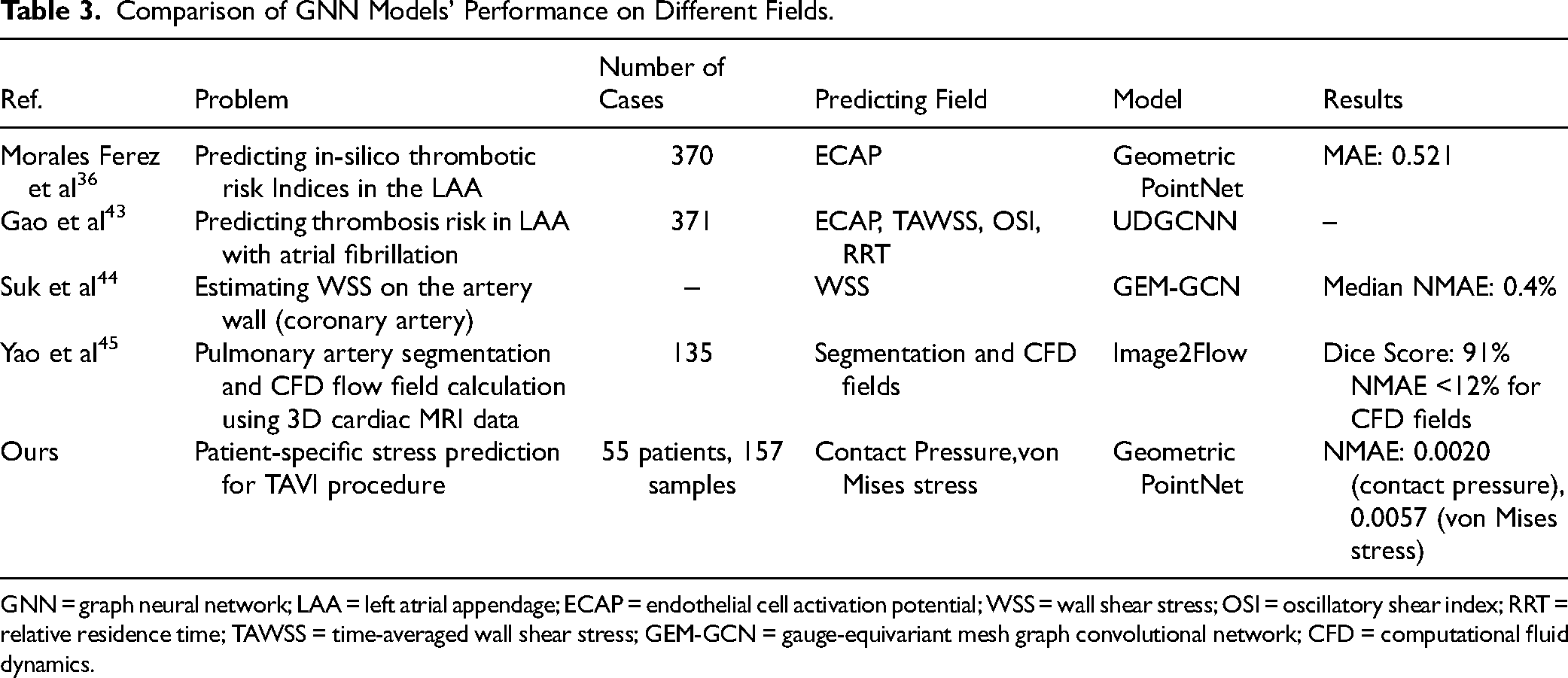
GNN = graph neural network; LAA = left atrial appendage; ECAP = endothelial cell activation potential; WSS = wall shear stress; OSI = oscillatory shear index; RRT = relative residence time; TAWSS = time-averaged wall shear stress; GEM-GCN = gauge-equivariant mesh graph convolutional network; CFD = computational fluid dynamics.
Limitations and Future Directions
Despite the promising outcomes of this investigation, numerous challenges remain. A major challenge is the limited number of contact points and the variability of aortic geometries, which complicate predictions, particularly in cases with extreme geometric differences. The model succeeds in capturing the patterns and extreme values of contact pressure in most cases, but von Mises stress predictions are more challenging since they do not always have similar stress patterns in the FEA findings for different patients. This disparity might be due to differences in stress distribution patterns across diverse patient anatomies, which the model has difficulty in capturing consistently. Dealing with these difficulties may benefit from more extensive datasets covering a broader range of anatomical characteristics as well as further research on the exact connections between patient-specific geometries and FEA results. Future research should focus on creating a large dataset encompassing a wider variety of patient anatomies. By expanding the dataset with more comprehensive patient information, models can potentially learn more delicate representations of physiological and anatomical variations, enhancing their accuracy and reliability. Furthermore, exploring adaptive learning algorithms that can adjust to new data or rare conditions without extensive retraining could significantly improve model robustness. Collaboration with clinical and research institutions for data collection, along with adherence to privacy and ethical standards, will be crucial in this endeavor. Additionally, integrating enhanced machine learning techniques such as physics-informed neural networks or unsupervised learning algorithms may help in deriving deeper insights from the expanded dataset without the need for extensive labeling. Moreover, investigating hybrid models that combine traditional computational fluid dynamics with GNNs could provide a more robust framework for understanding complex biomechanical interactions in TAVI procedures. A limitation of this study is that the segmentation was based on a single-phase CT reconstruction, without explicitly accounting for dynamic changes in aortic root geometry throughout the cardiac cycle. In addition, calcific nodules were not separately modeled, which may influence local stent expansion behavior and the resulting stress and contact pressure distributions. Future work will incorporate multiphase imaging and improved modeling of calcification to better capture patient-specific biomechanical responses. Another limitation of this study is the lack of direct clinical validation of the FEA simulations against post-TAVR imaging data. While the FEA framework follows established protocols, differences between simulated and actual stent expansion may affect the accuracy of predicted contact pressure and stress distributions. Future work will focus on validating the simulation outcomes using post-TAVR CT images to better assess the accuracy of device deformation and improve the reliability of the predictive model. Another limitation of the current framework is that implantation depth is not explicitly modeled as an independent variable. The predicted outcomes are based on fixed deployment configurations derived from FEA simulations and therefore do not allow systematic exploration of different implantation depths. Future work will focus on incorporating implantation depth as a controllable parameter to enable preoperative optimization of valve positioning and reduce the risk of conduction disturbances. All things considered, this work offers a fundamental structure for applying GNNs in mechanical stress predictions, particularly in TAVI. The suggested method has great potential for personalized modeling in cardiovascular therapies and helps to enable customized treatment plans for aortic valve replacement. By using GNNs, this approach also provides a computationally effective substitute for conventional FEA, hence lowering the significant processing time and computational capability usually needed. To bridge this gap, future work will focus on estimating contact regions directly from pre-TAVI data. This can be achieved through geometry-based proximity analysis between the aortic wall and the virtual stent, or by training auxiliary learning models to predict likely contact regions based on anatomical features. Such approaches would enable the surrogate model to approximate the benefits of contact-informed predictions without requiring full FEA simulations, thereby improving clinical usability.
Conclusion
In this investigation, we implemented GNN models for predicting patient-specific stress outcomes, specifically contact pressure and von Mises stress, for TAVI procedures. We conducted FEA simulations using 3D aorta geometries and a variety of stent diameters to produce patient-specific stress data, which was then processed and prepared for the training of the GNN model. For contact pressure, the GNN model accurately predicted contact pressure with the change of stent diameters, with an MSE of 0.0321, MAE of 0.0671, and NMSE of 0.0020, showing high quantitative performance. The qualitative study found that combining initial aortic geometry with contact points from final geometries resulted in the most accurate predictions. For von Mises stress, the model achieved positive quantitative metrics, with an MSE of 0.0512, MAE of 0.1488, and NMSE of 0.0057. However, qualitative results showed inconsistencies between GNN predictions and FEA outcomes. These challenges may be caused by stent size variances and greater stress variability among patients in the case of von Mises stress. The predicted accuracy in this case could be enhanced by increasing the dataset and taking into account more complex correlations between aortic geometry and von Mises stress. Despite these limitations, this study offers a computationally efficient alternative to traditional FEA or CFD methodologies by developing a core framework for forecasting patient-specific stress predictions using GNNs. Future studies should focus on creating a larger dataset with additional patient-specific aortic root geometries to introduce more anatomical variations in the dataset. Also, establishing a more intricate relationship between the initial aorta geometry and FEA outcomes may significantly boost the performance of GNN models.
Footnotes
Acknowledgments
This research was supported by Qatar National Research Fund, National Research Priorities Program NPRP13S-0108-200024. The Open Access funding is provided by the Qatar National Library. We thank Ms Ruba Suleiman and Mr Mahmoud Khatib A. A. Al-Ruweidi for the TAVI registry data preparation for this work.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and publication of this article.