
Abstract
Objective
When used to secure prosthetic sutures in valve replacement procedures, titanium fasteners (TFs) have demonstrated benefits in both open and less invasive approaches. This study compares the outcomes from patients whose valve sutures were secured with conventional hand-tied (HT) knots to those whose valve sutures were secured with TFs.
Methods
A retrospective chart review was conducted to analyze the preoperative baseline characteristics and postoperative outcomes of 200 consecutive patients undergoing surgical valve replacement between January 2020 and May 2023. Patients were grouped according to whether their valve was secured using HT knots or TFs (COR-KNOT MINI® Device, LSI SOLUTIONS®, Victor, NY, USA).
Results
There were no significant differences in baseline preoperative characteristics between the groups. Patients in the TF group had significantly shorter aortic cross-clamp and cardiopulmonary bypass times than patients in the HT group (P < .05). The TF group also had shorter intensive care unit time and overall hospital length of stay (P < .05) compared to the HT group. Postoperative bleeding and paravalvular leak were less frequently observed in the TF group than the HT group (P < .05). Although not statistically significant, there was a trend toward fewer wound infections and lower mortality rates in the TF group.
Conclusions
In our single center's early experience, the use of TFs in surgical valve replacement was associated with shorter operative times, hospital length of stay, and lower overall complication rate compared to HT valve sutures. These results are consistent with the benefits of TFs that have been previously well established in surgical literature.
Key Learning Messages
Titanium fasteners reduce operative times Patients whose valve sutures were secured with titanium fasteners (TFs) experienced significantly shorter cardiopulmonary bypass time and aortic cross-clamp time compared to those with hand-tied knots. This benefit was observed across single, double, and triple valve replacement procedures. Improved postoperative outcomes with TFs The TF group had lower rates of postoperative complications, including significantly less postoperative bleeding, paravalvular leak, and wound infections. Although mortality differences were not statistically significant, no early or late-phase mortality was reported in the TF group. Shorter intensive care unit (ICU) and hospital length of stay Patients in the TF group had significantly shorter ICU length of stay (LOS) and total hospital LOS.
Introduction
Cardiovascular disease is the leading cause of death worldwide, responsible for 17.5 million deaths every year, 80% of which occur in low- and middle-income countries (LMIC). 1 One of the major causes of cardiovascular mortality is valvular heart disease, which has a greater prevalence in LMIC due to the burden of rheumatic heart disease (RHD). 1 In recent years, studies have been conducted to better understand the availability and reliability of cardiac surgery in LMIC. 1 Jordan is classified as an upper-middle income country, in which the etiology of valvular disease is mixed between RHD (as in LMIC) and degenerative and calcified valves, more characteristic of high-income countries. 2 Valvular heart disease, regardless of etiology, is a major source of morbidity and mortality and surgical intervention largely remains the gold standard for durable, long-term treatment. However, cardiac surgery presents a unique set of patient risks, including those associated with aortic cross-clamp time and cardiopulmonary bypass (CPB) time.
Innovative automated technology is available to support the management of valvular disease, potentially improving patient outcomes by reducing surgical times and increasing surgical efficiency. The use of titanium fasteners (TF) can expedite the process of securing valve sutures by automating the knot-tying process. The COR-KNOT® Device (LSI SOLUTIONS®, Victor, NY, USA) crimps a titanium “knot” on suture, providing instant security and eliminating the need for a traditional hand-tied (HT) knot. When used to secure prosthetic valves, TFs have been shown to reduce AXT and CPB time without increasing mortality or adverse outcomes.3-6 Though some sutureless valves have been demonstrated to similarly reduce AXT and CPB time, they have also been associated with increased rates of permanent pacemaker implantation and paravalvular leak. 7
COR-KNOT® TFs have been widely adopted in heart valve surgery over the past decade, with more than 15 million TFs implanted in more than 1 million patients across the world. Despite the widespread use of this technology, there is no consensus supporting its routine use in heart valve surgery.3,7-9 Herein, we present our single-center experience using TFs in single, double, and triple valve replacement surgery through a median sternotomy approach (Figure 1).
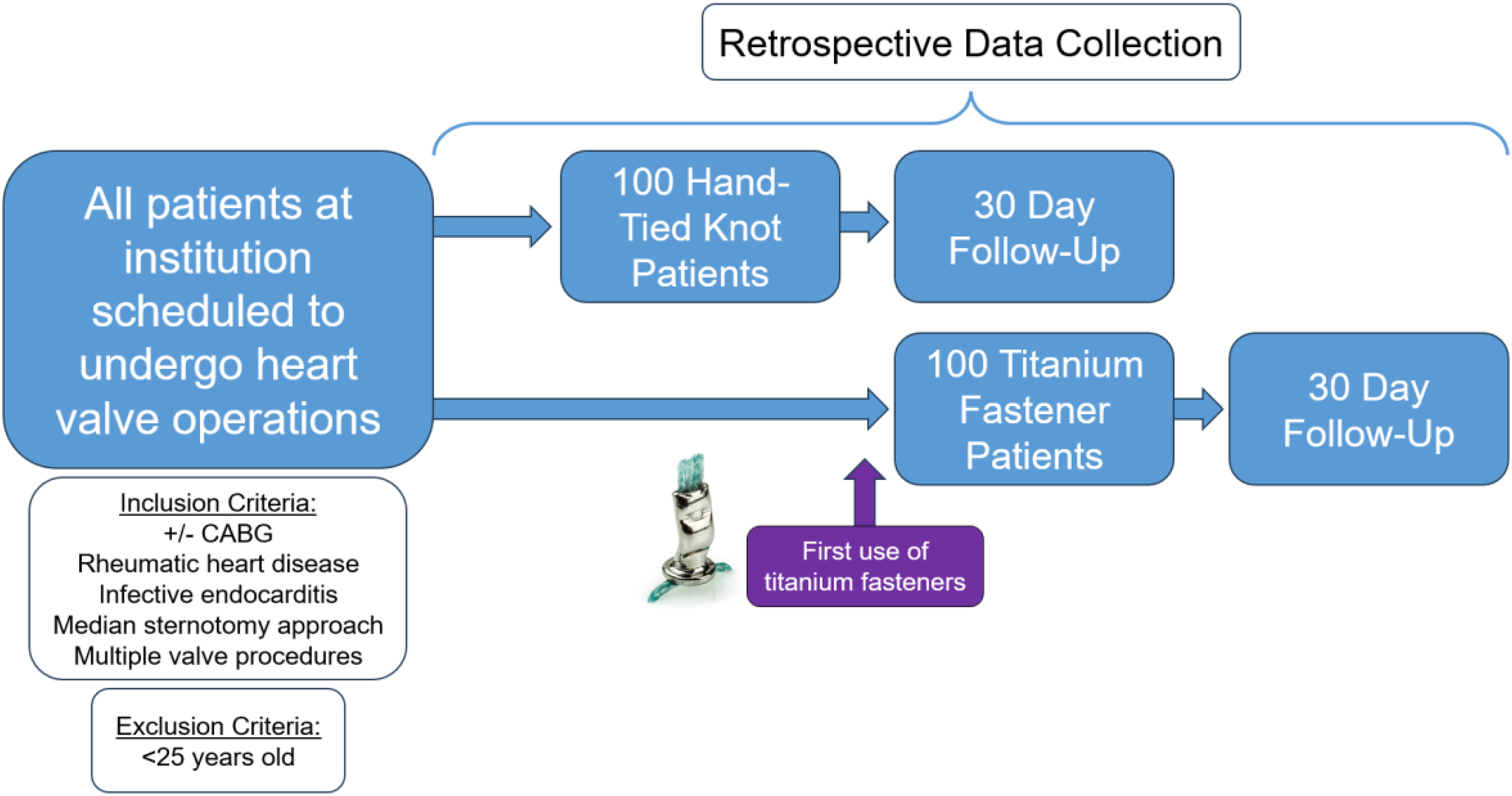
Visual representation of study methods.
Methods
We conducted a retrospective chart review of patients ≥25 years old who underwent elective heart valve replacement surgery at Albasheer Hospital for Specialized Surgery and at private hospitals in Amman, Jordan, between January 1, 2020, and May 3, 2023. All procedures were consecutively performed by a single surgeon via a median sternotomy approach. Patients were grouped according to the method by which their valve sutures were secured: TFs (n = 100) or HT knots (n = 100) (Figure 2). For this study, the primary outcomes were CPB and AXT times. Secondary outcomes included length of stay (LOS) in the intensive care unit (ICU), total hospital length of stay, major morbidity, early phase mortality (defined as mortality within 30 days) and late-phase mortality (mortality after 30 days).

Enlarged view of a titanium fastener in place to secure annular sutures.
Statistical Analysis
Study data were manually extracted from the subjects’ medical records and analyzed using SPSS Version 23 Software (IBM Corp, Armonk, NY, USA). Nonparametric data were compared using Fisher's exact test. Categorical data were compared using χ2 tests, with Fisher's exact test used as an alternative when cell counts in a 2 × 2 table were less than 5. Normality of data was assessed using the Kolmogorov–Smirnov test. Normally distributed continuous variables were reported as means ± standard deviation (SD) and compared using Student's t-test. Statistical significance was considered for P < .05.
Results
Patient Characteristics
A total of 200 patients were included in the study: 100 in the TF group and 100 HT knots group. Patient demographic characteristics and baseline clinical characteristics were similar between the 2 groups, with no significant difference in age or gender distribution, or the presence of rheumatic disease and preoperative endocarditis (Table 1). Additionally, the distribution of surgical procedures (single valve, double valve, triple valve) and concomitant coronary artery bypass grafting were comparable between TF and HT knots groups (Table 1).
Subject Demographics and Clinical Characteristics by Group.

TF, titanium fastener; HT, hand-tied; CABG, coronary artery bypass grafting; RHD, rheumatic heart disease.
Operative Outcomes
The TF group experienced significantly shorter CPB time (55.47 vs 64.78 min, P < .002) and AXT (41.32 vs 47.67 min, P = .002) compared to the HT knots group (Table 2). Similarly, ICU LOS (1.05 vs 1.39 days, P < .001) and total hospital length of stay (4.86 vs 6.13 days, P < .001) were also significantly lower in the TF group (Table 2).
Surgical Metrics Between Groups.

TF, titanium fastener; HT, hand-tied; ICU, intensive care unit.
When patients were stratified by number of concomitant valve procedures (ie, single valve, double valve, or triple valve), similar results were observed. Patients in the TF group had significantly shorter CPB time in single (49.07 vs 55.51 min, P < .001), double (65.36 vs 82.77 min, P < .001) and triple (95.00 vs 110.00 min, P = .015) valve surgery compared to the HT knots group (Table 4). Similarly, TF patients had significantly shorter AXT compared to the HT knots group in single (36.50 vs 39.57 min, P = .040), double (48.57 vs 65.68 min, P < .001), and triple (72.50 vs 78.83 min, P = .022) valve replacements (Table 4). Across patients undergoing single, double, and triple valve surgery, the TF group also experienced significantly shorter total hospital and ICU LOS (Table 4).
Overall, postoperative complications were more frequently observed in the HT knots group (18 vs 0, P = .029). Specifically, the occurrence of postoperative bleeding (6 vs 0, P = .029), paravalvular leak (6 vs 0, P = .029), and wound infection (6 vs 0, P = .029) was significantly higher in the HT knots group compared to the TF group. Mortality rates also trended lower in the TF group, with no early or late phase mortality—compared to 1 early mortality and 2 late mortalities in the HT knots group—although the difference was not statistically significant (P = .246). Overall, the TF group experienced fewer postoperative complications, highlighting the potential for enhanced patient safety and improved surgical outcomes (Table 3).
Surgical Metrics Between Groups.

TF, titanium fastener; HT, hand-tied.
Surgical Metrics Between Groups Stratified by Single, Double, or Triple Valve Operation.

TF,#titanium fastener; HT, hand-tied; ICU, intensive care unit.
Discussion
This study represents an expansion on the well-established benefits of using TFs as an alternative to HT knots to secure valve sutures. In this single-center study in Jordan, we observed that, on average, using TFs translated to a nearly 9-min reduction in CPB time and a 6-min reduction in AXT. The shorter operative times observed in the TF group are consistent with prior studies that reported the benefit automated fasteners in reducing surgical durations.3–6,10 While the benefits of TFs are frequently reported in minimally invasive cardiac procedures, in which securing sutures at deep surgical sites presents increased technical challenges, their benefits in a median sternotomy approach have not been as well discussed.3,5–7 Some reports have concluded that using TFs in sternotomy cases had no overall effect on operative times, while others, including this study, have demonstrated that there are significant advantages to using automated technology.4,10 In a 2021 propensity-matched retrospective cohort of patients undergoing heart valve surgery via a median sternotomy, Ler et al observed a 49 min reduction in CPB time and 32 min reduction in AXT in the TF group. 11
A 2021 meta-analysis investigated the use of TFs in open and minimally invasive heart surgery, revealing that patients whose valve sutures were secured with TFs experienced a lower rate of postoperative valvular regurgitation than those whose valve sutures were secured with HT knots. 3 Though valvular regurgitation was not incorporated as an outcome variable in our analysis, we similarly observed a lower rate of paravalvular leak in the TF group relative to the HT group (0 vs 6 occurrences, P = .029). A 2010 benchtop study demonstrated that the COR-KNOT® Device provided more consistent pressure between the valve sewing cuff and the underlying tissue, resulting in better seating of the valve prosthesis. 12 This study also showed that the prosthetic sewing cuff attachment pressures in the areas contained within the individual sutures (intrasuture) was double the intrasuture pressure of HT knots. 12 This study noted that greater intrasuture and extrasuture pressure around the valve annulus complex could potentially decrease the risk for paravalvular leak. 12 Our results appear to provide additional real-world evidence supporting these reported potential benefits. While there have been case reports of leaflet perforation associated with TF use, proper use of the device—including placing TFs on the outer ring of the sewing cuff, holding the device perpendicular to the annulus, and applying sufficient suture tension—helps prevent this potential complication.13–15
Though the cost of care using TF technology was not evaluated as part of our study, we expect that the significant decrease in operative times, ICU LOS, and overall hospital length of stay in the TF group ultimately leads to a lower total cost of care. The observed reduction in operative times may indirectly contribute to improved outcomes, as patients benefit from reduced exposure to the well-established risks associated with prolonged AXT and CPB time. Importantly, the lower rates of postoperative bleeding, paravalvular leak, and wound infections experienced by patients in the TF group also suggest a potential for both reduced overall costs and enhanced patient outcomes. It is paramount that, regardless of cost of care metrics, the incorporation of TF technology is ultimately viewed in the context of its potential to enhance patient safety.
In addition to corroborating the benefits of TFs already published in the literature, this study draws attention to the unique clinical environment in LMICs, generally, and in Jordan, specifically. In a previous update of the American Society of Thoracic Surgeons Database, it was reported that 11% of patients underwent double valve procedures, while triple valve surgery was performed in only 1% of cases. 16 However, these statistics are representative of patient populations in high-income countries. In our studied cohort, which is more reflective of an LMIC patient population, 30% of patients required multiple valve surgery, with nearly 5% undergoing a triple valve procedure. Multiple valve disease has an increased prevalence in LMIC, as rheumatic heart disease contributes significantly to the overall disease burden. 17 Our stratified analysis of single, double, and triple valve procedures showed consistently lower operative times and shorter hospital stays for patients in the TF group (Table 4). Jordan is facing a severe shortage of surgical providers, with just 1.7 adult cardiac surgeons per 1 million people (contrasted with 11.12 cardiac surgeons per 1 million people in North America). 2 Accordingly, it is difficult for even very sick patients to get OR time. Efforts to improve access to surgical care in LMICs should be accompanied by investment in improving the quality, efficiency, and safety of care. Our results suggest that TF technology has the potential to provide this improved surgical efficiency for health care systems in Jordan and other LMICs, expanding the availability of critical care for patients with multiple valve disease while also providing enhanced outcomes.
Conclusion
Patients whose valve sutures were secured with TFs experienced significantly less CPB and AXT time, had fewer postoperative complications, and spent less time in the ICU and in the hospital overall. These results from a single center are consistent with those reported in other single- and multicenter studies, while also highlighting the benefits of automated TF technology to Jordan and similar LMICs. A larger, multicenter prospective study including centers from various LMICs is necessary to strengthen the evidence for these already compelling results.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Kyle Purrman is a full-time employee of LSI Solutions and serves as the manager of the Surgical Science Department; Dr Shaelyn Cavanaugh is a research fellow at the University of Rochester which receives unrestricted research grant funding from LSI Solutions; Dr Ariana Goodman is a research fellow at the University of Rochester which receives unrestricted research grant funding from LSI Solutions; and Mark Lutz is participating in a research fellowship funded by LSI Solutions.