
Abstract
Background
Extracorporeal membrane oxygenation (ECMO) is a life support technique used in patients with respiratory or cardiac failure. Despite the increased use of ECMO, the incidence and risk factors for healthcare-associated infections (HAIs) are highly variable and dependent on healthcare systems.
Objectives
To describe the incidence of HAIs in patients on ECMO secondary to respiratory or cardiac failure, the microorganisms involved, and antibiotic resistance, and to identify risk factors associated with the incidence of HAIs.
Design
Single-center retrospective cohort study.
Methods
We included adult patients (15 years or older) on venovenous ECMO (VV-ECMO) or venoarterial ECMO (VA-ECMO) secondary to respiratory or cardiac failure and who were admitted to the Instituto Nacional del Tórax (Santiago, Chile) between 2022 and 2024. We included confirmed HAIs related to the ECMO procedure between 24 h after ECMO initiation and 48 h after its withdrawal. Microbiological confirmation was obtained through positive cultures, positive pneumonia FilmArray results, or elevated bronchoalveolar lavage galactomannan levels (> 1 mg/L). The data were collected by two researchers and verified by a third party. We conducted multivariable logistic regression to identify risk factors for HAI.
Results
Seventy-two patients were included in our study, with a median age of 46 years (IQR 29.75-59) and 55.56% male. Thirty-eight (52.78%) patients had confirmed HAI. We identified 70 microorganisms, with gram-negative bacilli being the most prevalent. Among these, the majority were Pseudomonas spp. (32.65%), Klebsiella spp. (20.41%), and Enterobacter spp. (16.33%). Among the gram-positive cocci, Staphylococcus aureus was the most frequently detected microorganism (57.9%). Antibiotic resistance patterns included methicillin-susceptible Staphylococcus aureus (n = 9), non-carbapenemase-producing carbapenem-resistant isolates (n = 11), and carbapenemase-producing isolates (n = 10). Multivariable analysis demonstrated that each additional day on ECMO increased HAI risk by 7% (95% CI 1.0-13.4), after adjusting for left ventricular ejection fraction, organ failure type, and ECMO indication.
Conclusion
Half of the patients on ECMO secondary to respiratory or cardiac failure developed HAI. The most frequent microorganisms were gram-negative bacteria, and the primary antibiotic resistance detected was for carbapenems. The only independent risk factor for developing HAI was the length of stay on ECMO.
Keywords
Introduction
Extracorporeal membrane oxygenation (ECMO) is a life support technique used in patients with respiratory or cardiac failure.1–3 Its use has increased significantly in the last decade, coinciding with landmark studies such as CESAR 4 and EOLIA 5 and experience gained during the H1N16,7 and COVID-19 pandemics.8–10 The effectiveness of ECMO support is variable, with heterogeneous impacts on clinical outcomes such as mortality.11,12 Observational and experimental studies report a mortality rate of patients who are on ECMO ranging from 22% to 63%, 11 with a national registry showing a lower mortality rate in patients on venovenous ECMO (VV-ECMO) than in those on venoarterial ECMO (VA-ECMO). 12 This outcome may occur more frequently in people with acute respiratory distress syndrome. 12
ECMO circuits, whether VA- or VV-ECMO or other less common system configurations, present a high risk of healthcare-associated infections (HAIs).13,14 The incidence and risk factors for HAIs in patients on ECMO are highly variable and likely vary across different clinical settings and healthcare institutions. These infections are common due to factors such as pre-existing comorbidities and immunocompromised states associated with critical illness. Non-patient factors include mechanical ventilation (MV) time, red blood cell input, intensive care unit (ICU) hospitalization time, renal replacement therapy, and others.15–17 Prolonged length of stay on ECMO is also associated with an increased risk of acquiring an HAI.18–20
Studies have shown significant variability in the timing criteria for HAI definitions, ranging from 24 to 72 h after cannulation and from 24 to 72 h after circuit discontinuation. 21 Previous studies have reported that gram-positive infections typically occur earlier than gram-negative infections in patients on ECMO, with Klebsiella pneumoniae and Escherichia coli being frequently isolated pathogens.19,22,23 However, comprehensive data on antibiotic resistance patterns and the impact of HAIs on clinical outcomes in this population remain limited and inconsistent.19,22,23 The heterogeneity of HAI definitions used in the studies may also contribute to this inconsistency in the results. 21 In this study, our objective was to describe the incidence of HAIs in patients on ECMO secondary to respiratory or cardiac failure, the microorganisms involved, and antibiotic resistance, and to identify risk factors associated with the incidence of HAIs.
Methods
Study Design and Population
This is a retrospective cohort study that included adult patients (15 years or older) who were on VV-ECMO or VA-ECMO secondary to respiratory or cardiac failure and who were admitted to the Instituto Nacional del Tórax (Santiago, Chile) between January 2022 and October 2024. The Instituto Nacional del Tórax is a Chilean tertiary referral center for the management of respiratory and cardiac diseases.
We excluded patients on ECMO for less than 24 h, those for whom the indication was due to respiratory failure caused by SARS-CoV2, and those for whom data were missing from medical records.
This study's reporting conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement. 24
Data Collection and Definition of Operational Variables
We designed a form to collect the data. Two researchers extracted data from medical records, and a third researcher reviewed this data extraction.
We extracted sociodemographic data to characterize our study participants, including age, sex, weight, height, and comorbidities (hypertension, diabetes mellitus, asthma, chronic obstructive pulmonary disease, and heart failure with left ventricular ejection fraction (LVEF) <30%). Concerning ECMO, we extracted information on the patient's type of organ failure (pulmonary, cardiac, or mixed), admission and indication for ECMO, type of ECMO (VV-ECMO, VA-ECMO, or other), site of cannula insertion, and length of stay on ECMO. We collected information on clinical outcomes such as use of MV before ECMO, MV duration, need for tracheostomy, total hospital stay, and mortality.
Although no standardized temporal definition exists for HAIs in patients on ECMO, studies have demonstrated significant variability in infection timing criteria, ranging from 24 to 72 h after cannulation and 24 to 72 h after circuit discontinuation. 21 Based on this evidence, clinical considerations, and the guidelines established by the Chilean Ministry of Health (MINSAL), we define HAI in patients on ECMO as any confirmed infection between 24 h after ECMO initiation and 48 h after cannulation removal. 21 Microbiological confirmation was obtained through positive cultures, positive pneumonia FilmArray results, or elevated bronchoalveolar lavage galactomannan levels (>1 mg/L). We collected data on the site of infection, the identified microorganism, the antibiotic treatment administered, and the resistance detected.
Statistical Analysis
Statistical analyses were performed in the JASP program (JASP Team; 2024—Version 0.19.1 [Computer software]). We used a statistical threshold of < 0.05. Graphics were performed in GraphPad Prism (version 10.4.1 for Windows, GraphPad Software, Boston, Massachusetts, USA, www.graphpad.com).
We described categorical variables with absolute numbers and percentages. Quantitative variables are described by mean and standard deviation (SD), median and interquartile range (IQR), or minimum-maximum (Min-Max) according to their distribution. We evaluated the distribution of quantitative variables using the Shapiro-Wilk test.
To identify factors associated with the incidence of HAI, we performed a logistic regression analysis. First, we conducted simple regression analyses to identify variables significantly associated with HAI incidence. Then, to determine factors independently associated with HAI incidence, we performed multiple regression analysis, including all variables significantly associated (p ≤ 0.25) with HAI incidence in the simple regression analysis. 25 We report odds ratios (ORs) and their 95% CIs.
Results
Study Population Description
Ninety-eight patients on ECMO between January 2022 and October 2024, of whom 72 (73.47%) met our eligibility criteria (Figure 1). The median age of the patients was 46 years (IQR 29.75-59), and 40 (55.56%) were male. Forty-six (61.11%) had one or more diagnosed comorbidities. Most patients on ECMO were due to heart failure (51.39%), with cardiogenic shock being the principal connecting diagnosis (43.06%) (Table 1). Because of this, most patients on VA-ECMO (55.56%) were via peripheral cannulation (65%). The median length of stay on ECMO was 7 days (IQR 1-113) (Table 2).

Selection of study participants. ECMO: extracorporeal membrane oxygenation; h: hours.
Characteristics of study participants.

IQR: interquartile range; SD: standard deviation; LVEF: left ventricular ejection fraction; ECMO: extracorporeal membrane oxygenation; ARDS: acute respiratory distress syndrome.
ECMO connection characteristics.

ECMO: extracorporeal membrane oxygenation; VV: venovenous; VA: venoarterial; VVA: venoveno-arterial; Min: minimum; Max: maximum.
Almost all patients (98.61%) were on MV for > 24 h, of which 32 (44.44%) required MV before ECMO (Table 3). The median hospital stay was 30 days (IQR 18-70.25); 13 (18.06%) patients underwent tracheostomy. In-hospital mortality was 47.22%.
Mechanical ventilation description.
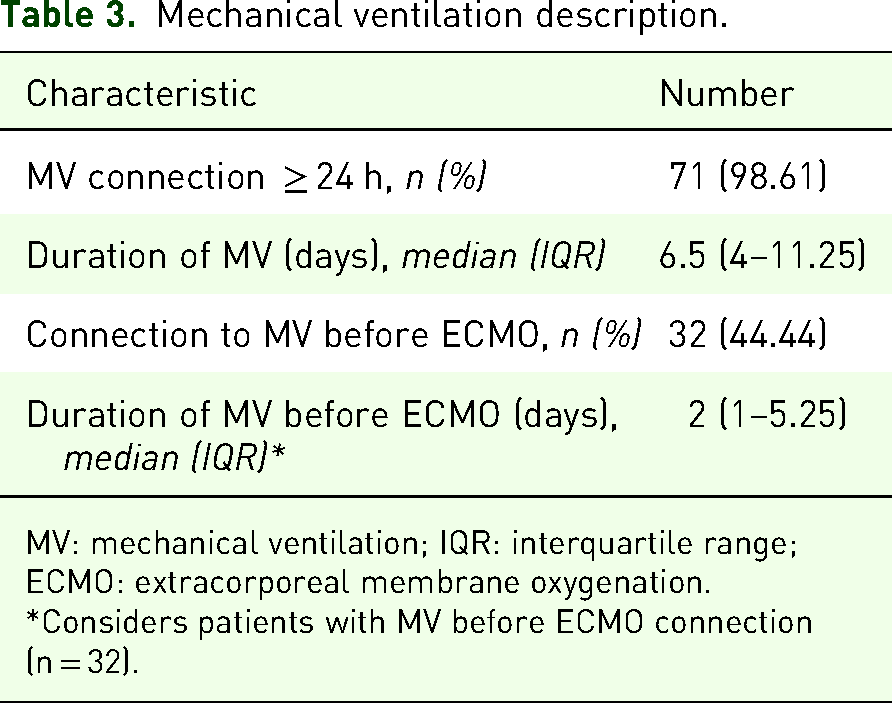
MV: mechanical ventilation; IQR: interquartile range; ECMO: extracorporeal membrane oxygenation.
*Considers patients with MV before ECMO connection (n = 32).
Incidence of HAIs, Identified Micro-Organisms, and Antibiotic Resistance Patterns
Thirty-eight (52.78%) patients had confirmed HAI, with a respiratory focus being the most frequent (84.21%). We identified 70 microorganisms, with gram-negative bacilli being the most prevalent. Among these, the majority were Pseudomonas spp. (32.65%), Klebsiella spp. (20.41%), and Enterobacter spp. (16.33%). Among the gram-positive cocci, the most frequently detected microorganism was Staphylococcus aureus (57.9%) (Figure 2). We provide details of the microorganisms detected in Supplemental Table 1. Regarding antibiotic resistance, we identified methicillin-susceptible Staphylococcus aureus (n = 9) and carbapenemase-producing organisms (n = 10). Among the carbapenemase producers, four (40%) carried New Delhi metallo-beta-lactamase (NDM) and six (60%) carried Verona integron-encoded metallo-beta-lactamase (VIM). No Clostridioides difficile resistance was detected (Figure 3).

Microorganisms identified in ECMO patients.

Antibiotic resistance detected.
Factors Associated With HAI Incidence
Simple logistic regression analysis identified the duration on ECMO as the only risk factor for developing HAI (Table 4). This was confirmed in the multiple regression analysis, resulting in a risk of 7% (95% CI 1.0-13.4) for each additional day on ECMO, independent of LVEF, type of organ failure, and diagnosis leading to initiation of ECMO (Table 5).
Assessment of the association of variables with the incidence of HAIs (simple logistic regression).

MV: mechanical ventilation; ECMO: extracorporeal membrane oxygenation; VV: venovenous; VA: venoarterial; VVA: venoveno–arterial; LVEF: left ventricular ejection fraction; ARDS: acute respiratory distress syndrome; BMI: body mass index.
* Wald test, ** Reference category, ¥ Statistically significant, † Variables included in the multiple logistic regression model.
Assessment of the association of variables with the incidence of HAIs (multiple logistic regression).

ECMO: extracorporeal membrane oxygenation; LVEF: left ventricular ejection fraction; ARDS: acute respiratory distress syndrome.
* Wald test, ** Reference category, ¥ Statistically significant.
Discussion
In this study, the occurrence of HAIs in adult patients on ECMO secondary to cardiac or respiratory failure was 52.78%. Gram-negative bacteria were the most identified pathogens, with carbapenem resistance being the most frequently observed form of antibiotic resistance. Among the potential risk factors analyzed, our findings indicated that only the length of stay on ECMO was independently associated with the development of HAI.
Fifty percent of patients included in our study had HAI. This rate is notably higher than the 26% (95% CI 14-38%) reported in a systematic review and meta-analysis encompassing 18 studies with 3424 patients. 16 Similarly, a retrospective analysis from 2012 to 2015 reported a 26% (CI 95% 17.2%-34.7%) infection rate among adult patients on ECMO. 26 The Extracorporeal Life Support Organization (ELSO) registry cites an infection rate of 11.7%. 27 However, other studies have documented infection rates exceeding 50%, indicating significant variability across different centres. 28 This disparity may stem from differences in patient populations, infection control practices, and definitions of nosocomial infections. 29 To our knowledge, this is the first study to report HAI incidence in adult patients on ECMO in South America.
Our study identified length of stay on ECMO as the sole independent risk factor for HAI (7% increased risk per day), which is consistent with multiple studies. Hsu et al found prolonged ECMO use to be the only independent risk factor, 30 while Li et al reported that the length of stay on ECMO >4.5 days significantly increased infection risk. 31 Juthani et al identified a duration >10 days as a major risk factor (OR = 14.65), 32 and Sun et al confirmed a significant correlation between the length of stay on ECMO and nosocomial infections. 33 These studies collectively highlight the importance of minimizing ECMO duration when clinically feasible to reduce the risk of nosocomial infections. 34 While some studies report additional risk factors such as ECMO type or mechanical complications, we did not find a similar association and our analysis suggests that the length of stay on ECMO remains the predominant predictor across different healthcare settings.
Our study identified Pseudomonas aeruginosa, Staphylococcus aureus, Klebsiella pneumoniae, and Enterobacter species as the predominant pathogens in nosocomial infections among patients on ECMO. These findings align with the existing literature.29,35,36 Pseudomonas aeruginosa is notably associated with ventilator-associated pneumonia and bloodstream infections in critically ill patients, including those on ECMO. Similarly, Staphylococcus aureus, particularly methicillin-resistant strains, is a well-documented pathogen in ICUs, contributing to various infections from pneumonia to surgical site infections. 35 The detection of Klebsiella pneumoniae and Enterobacter species in our cohort is consistent with global reports.31,37,38 Klebsiella pneumoniae, for instance, has been identified as a cause of urinary tract infections, pneumonia, and bloodstream infections, with certain hypervirulent strains posing significant treatment challenges due to antibiotic resistance. Enterobacter species are similarly known to cause infections in immunocompromised patients, often exhibiting resistance to multiple antibiotics. The prevalence of these pathogens highlights the vital importance of strong infection control measures and careful antimicrobial stewardship in managing patients on ECMO, who are especially vulnerable to such infections due to the invasive nature of the therapy and their underlying critical conditions.
We observed a notable prevalence of carbapenem-resistant pathogens among patients on ECMO. This finding aligns with recent research indicating a high incidence of infections due to carbapenem-resistant organisms in patients on ECMO. 39 The emergence of carbapenem-resistant enterobacterales has been a significant concern in nosocomial infections. 40 These resistant strains complicate treatment options and are associated with increased morbidity and mortality. However, knowledge of common antibiotic resistance in patients on ECMO may help to design specific empirical treatment strategies and thus achieve more favorable outcomes for these patients. This should be studied using a quality improvement project study.
Our study has limitations. There was a possible selection bias due to excluding patients on ECMO for less than 24 h or those with SARS-CoV-2-induced respiratory failure. Furthermore, we cannot dismiss the possibility that a patient may present with any HAI before ECMO that is subsequently detected 24 h after cannulation, which could incorrectly attribute the HAI to ECMO. Additionally, the retrospective design may limit the ability to establish causality and is subject to the constraints of available medical records. Conversely, our study had several strengths. The robust data mining process, involving dual extraction and independent review, enhanced data accuracy and reliability. To our knowledge, this was the first study to report HAI incidence in adult patients on ECMO in South America, 41 contributing meaningful data pertinent to ECMO in this region.
Future studies should adopt a prospective design to control confounding factors and establish causal relationships more effectively. Employing a multicenter approach would also help account for center-specific variations in clinical practice and improve external validity. Moreover, future research should aim to collect more detailed data on clinical interventions and long-term outcomes to provide a deeper understanding of HAIs in patients on ECMO.
Conclusion
One in two patients on ECMO secondary to respiratory or cardiac failure developed any HAI. The most frequent microorganisms were Pseudomonas aeruginosa, Staphylococcus aureus, Klebsiella pneumoniae, and Enterobacter, and the primary antibiotic resistance detected was for carbapenems. The only independent risk factor for developing HAI was the length of stay on ECMO.
Supplemental Material
sj-docx-1-cra-10.1177_29768675251395844 - Supplemental material for Incidence of Healthcare-Associated Infections in Patients on Extracorporeal Membrane Oxygenation Secondary to Respiratory or Cardiac Failure: A Retrospective Cohort Study
Supplemental material, sj-docx-1-cra-10.1177_29768675251395844 for Incidence of Healthcare-Associated Infections in Patients on Extracorporeal Membrane Oxygenation Secondary to Respiratory or Cardiac Failure: A Retrospective Cohort Study by Mariana Arias, Valentina Peralta, Gloria Marín, Alexander Matus and Ruvistay Gutierrez-Arias in Therapeutic Advances in Pulmonary and Critical Care Medicine
Supplemental Material
sj-docx-2-cra-10.1177_29768675251395844 - Supplemental material for Incidence of Healthcare-Associated Infections in Patients on Extracorporeal Membrane Oxygenation Secondary to Respiratory or Cardiac Failure: A Retrospective Cohort Study
Supplemental material, sj-docx-2-cra-10.1177_29768675251395844 for Incidence of Healthcare-Associated Infections in Patients on Extracorporeal Membrane Oxygenation Secondary to Respiratory or Cardiac Failure: A Retrospective Cohort Study by Mariana Arias, Valentina Peralta, Gloria Marín, Alexander Matus and Ruvistay Gutierrez-Arias in Therapeutic Advances in Pulmonary and Critical Care Medicine
Footnotes
Acknowledgements
We sincerely thank the Medical Records Team at the Instituto Nacional del Tórax, Santiago, Chile, for their invaluable support in accessing and organizing the data required for this study. Ixca Kosok Florsheim and Rafael Urrutia Diaz's dedication and professionalism were essential to completing this work.
Author Contribution(s)
Availability of Data and Materials
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
The affiliated university (Universidad Andrés Bello) does not have a scientific ethics committee accredited by Chilean law.
The patients included in our study are from the Instituto Nacional del Tórax, a health institution affiliated with the Servicio de Salud Metropolitano Oriente (SSMO) of Chile. The study was approved on July 23, 2024, by the Scientific Ethics Committee of the SSMO, Santiago, Chile (CECSSMOriente230724). This ethics committee granted a waiver of informed consent for this study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.