
Abstract
Background:
Implementing buprenorphine medication treatment for opioid use disorder (B-MOUD) in office-based, non-addiction specialty care settings is challenging. Clinical pharmacist practitioners (CPPs) can facilitate this care. The Veterans Health Administration’s (VHA) Stepped Care for Opioid Use Disorder Train the Trainer Initiative (SCOUTT) implemented B-MOUD in primary care, mental health, and pain clinics across 37 VHA facilities. B-MOUD activities provided by CPPs within SCOUTT are not well known.
Objectives:
We sought to examine CPPs’ roles, typical activities, and opportunities to provide B-MOUD.
Design:
We performed a cross-sectional survey of CPPs within SCOUTT facilities.
Methods:
In March 2023, known CPPs in SCOUTT clinics were invited via email to participate in an online survey. We also emailed local SCOUTT leaders to forward the invitation to CPPs not initially invited. The anonymous survey gathered information on clinic settings, CPP roles in 25 B-MOUD related tasks (eg, patient intake, risk assessment, initiation), state licensure, and whether they had or desired controlled substance prescriptive authority for B-MOUD.
Results:
Twenty-two CPPs responded to the survey working in pain (40.9%), primary care (27.3%), mental health (22.7%), and primary care mental health integrated (22.7%) settings. Nearly all (95.5%) reported involvement in naloxone education and distribution and patient management after B-MOUD initiation. Additionally, 90.9% reviewed and interpreted urine drug test results, 90.9% conducted B-MOUD follow-up (assessing side effects or treatment outcomes) and 72.7% assisted in B-MOUD initiation. Most CPPs (95.5%) indicated they work in a team-based environment often acting as a medication expert, were prescribing B-MOUD (27.3%), or desired to do so (86.4%).
Conclusion:
In the VHA’s SCOUTT Initiative, CPPs play a significant role in leading and collaboratively facilitating B-MOUD. The VHA’s SCOUTT approach to CPP management and B-MOUD prescribing efforts may be a model to emulate in other health systems to improve access to and management of B-MOUD care.
Highlights
This evaluation surveyed clinical pharmacist practitioners querying their roles, responsibilities, and views of providing medication treatment for opioid use disorder.
Clinical pharmacist practitioners’ unique roles and responsibilities can facilitate Veteran access to buprenorphine treatment for opioid use disorder outside of addiction specialty care settings.
Many clinical pharmacist practitioners are prescribing buprenorphine for opioid use disorder or wish to do so.
Background
A clinical pharmacist practitioner (CPP) is an interprofessional care team provider who is a licensed practitioner with advanced education and training with a focus on delivering comprehensive medication management within a collaborative, team-based practice. CPP practice has been shown to improve patient outcomes,1,2 enhance access to care, 3 provide cost-effective care,4,5 provide specialized knowledge and expertise, 6 and provide support for complex treatments,7,8 including opioid use disorder (OUD).9-13
CPP practice is common in the Department of Veterans Affairs, Veterans Health Administration (VHA). In July 2025, 53.4% (n = 6263) of all pharmacists in the VHA were CPPs. CPPs are distinct from other pharmacists within the VHA. CPPs within the VHA have independent prescriptive authority under a scope of practice (ie, collaborative practice agreement) which allows them to provide comprehensive medication management (CMM) as part of the care team within their given practice setting (eg, primary care, pain management, mental health). 14 A scope of practice is obtained through review of the pharmacist’s qualifications and competencies as part of the facility’s credentialing and privileging process with oversight by the executive committee of the individual facilities’ medical staff. Evidence of expertise could include post-graduate pharmacy residency training; Board of Pharmacy Specialties certification such as BCPP (Board Certified Psychiatric Pharmacist), BCPS (Board Certified Pharmacotherapy Specialist), and BCPMP (Board Certified Pain Management Pharmacist); or other clinical experience such as mentorship. 15 CPP competency is assessed through professional practice evaluations upon initial appointment and periodically thereafter in line with Joint Commission Standards and VHA policies related to credentialling of healthcare providers.14,16
Collaborative practice settings where CPPs practice are ubiquitous in the clinical environments of the VHA. For example, patient-aligned-care-teams (PACTs) are the VHA’s primary care medical home model where prescribers are teamed with nurse care managers, pharmacists, social workers, and other professionals to provide primary care and wrap around care to Veterans.17,18 Similar collaborative care models exist with the VHA’s outpatient mental health and pain clinic environments, among other specialty and acute practice areas. These environments enable Veteran patients to be served by teams of clinicians in a longitudinal approach to address chronic health conditions, such as OUD. Within these environments, CPPs have been known to work collaboratively with a controlled substance prescriber to initiate medication treatment for opioid use disorder (MOUD), adjust dose and frequency of MOUD, and/or discontinue MOUD along with more traditional roles of monitoring MOUD outcomes, provide naloxone education and distribution, and provide non-pharmacological treatments.8,12,19
With the passing of the US’ 2022 Mainstreaming Addiction Treatment Act as part of the US Consolidated Appropriations Act of 2023, the DATA-2000 Waiver program was eliminated, including qualifying practitioner restrictions. 20 With this legislative change, DEA-registered CPPs could now prescribe formulations of buprenorphine for MOUD (B-MOUD) in the states that allowed CPPs to prescribe Schedule 3 medications in collaborative practice settings.21-23 As of this writing, while all 50 states authorize dependent, collaborative, or autonomous pharmacist prescribing, only 14 states authorize CPPs to obtain DEA registration and more states are considering expanding controlled substance prescribing authority by CPPs, with a particular emphasis on improving access to B-MOUD.24,25 VHA CPPs have been early adopters of B-MOUD prescribing: in 2023, over 1090 Veterans were prescribed B-MOUD by 110 CPPs in over 30 states. 26 VHA CPPs may be licensed in any state across the US and, if licensed in a state with prescriptive authority, are able to provide B-MOUD care in any VHA location.
The VHA’s Stepped Care for Opioid Use Disorder Train the Trainer Initiative (SCOUTT) began in 2018 with a goal of facilitating access to MOUD, primarily B-MOUD, in non-substance use disorder specialty settings, namely primary care, mental health, and pain clinic settings. 27 The impetus for SCOUTT was that, historically, MOUD treatment had been relegated to substance used disorder (SUD) specialty care environments. These environments could reduce access to MOUD care as patients may be averse to attending SUD specialty care or engaging in OUD treatment in an episodic way.28,29
Through the first 4 years of SCOUTT, 37 facilities implemented MOUD in over 70 non-SUD-specialty clinic settings, improving access and retention to B-MOUD. This occurrence wasn’t limited to SCOUTT clinics and was observed in non-SCOUTT intervened facilities as well.30-33 Further, notable outcomes of SCOUTT included positive perspectives of providers,34-36 and improved health care utilization.37,38 Originally funded as a quality improvement project, SCOUTT continues today with VHA operational funding.
In expanding this B-MOUD access, several different clinic models developed, including OUD collaborative non-prescriber care. In the initial SCOUTT training in 2018, the first collaborative care model taught to SCOUTT teams was the nurse care manager collaborative care model.27,39-41 CPP collaborative care was not an original target intervention in SCOUTT; CPPs were not required to participate in SCOUTT clinics, although the original SCOUTT trainings had an unknown number of CPPs who attended. In these collaborative models of care, we observed that non-prescribing health care providers (eg, CPPs, nurse care managers, social workers) were the point of care contacts for patients to receive B-MOUD care and its care management. To date, the VHA employs 6263 CPPs, although not all facilities in the VHA have a CPP involved in providing B-MOUD; over 20 SCOUTT facilities were known to have engaged with CPPs. While there are some descriptions of how CPPs may manage MOUD within the VHA,8,12 the specific roles and responsibilities that CPPs had regarding patient intake, initiation, monitoring and risk assessment, follow-up activities, and quality assurance/outcomes were unknown.
To further understand how CPPs were integrated within SCOUTT, we sought to examine CPPs’ roles, typical activities, and opportunities to provide MOUD within SCOUTT. We sought to examine whether CPPs affiliated with SCOUTT wished to prescribe (or were prescribing) B-MOUD to Veterans. Finally, we wished to explore opportunities to expand CPP practices within SCOUTT and across the VHA to continue to further expand access to B-MOUD.
Methods
We performed a cross-sectional study of CPPs affiliated with SCOUTT to examine their roles, responsibilities, and opportunities for B-MOUD care and care management. We used the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines in reporting our study and results. 42 To be eligible for our study, the respondent affirmed that they were a CPP within a SCOUTT-intervened facility (n = 49 within 29 US States at the time of the survey). The VA Salt Lake City Health Care System and University of Utah Institutional Review Board confirmed that this quality improvement evaluation did not require approval as human subject research.
In March 2023, we emailed known CPPs affiliated with VHA SCOUTT clinics (n = 21) to participate in an online Research Electronic Data Capture (REDCap) survey regarding their practices within SCOUTT related to B-MOUD. The email indicated the purpose of the survey and included basic instructions to complete it through a link that would be sent directly to their email. Two days after the initial email, we employed a snowball sampling method and emailed SCOUTT leaders with instructions to forward the invitation to CPPs not initially invited. To help expand our list of CPPs, we also advertised this survey opportunity in several monthly national SCOUTT webinar community of practice calls. We requested survey completion within 16 days of the initial invitation and sent an email reminder to complete the survey 14 days later. Responses to this questionnaire were anonymous and to preserve anonymity, we did not inquire about demographic or practice characteristics. Respondents provided implicit consent to participate in this evaluation and could have terminated their participation at any time. The survey indicated the purpose of the study and the voluntary nature of the subjects’ participation. The VA Salt Lake City Health Care System and University of Utah Institutional Review Board did not require an informed consent document to be signed for this anonymous survey.
The survey structure and content were pilot tested by the authors, which included CPPs, and iteratively modified prior to execution. The survey content (see Supplemental Appendix for the complete survey) included information on clinic settings, CPP roles in 25 B-MOUD related tasks (eg, patient intake, initiation, monitoring and risk assessment, follow-up activities, quality assurance/outcomes), state licensure (specifically whether they had prescriptive authority for buprenorphine), and whether they desired (or had) controlled substance prescriptive authority for B-MOUD. The survey was developed by the authors, including VA Pharmacy Benefits Management Clinical Pharmacy Practice Office program managers, VA clinical investigators, and staff and based on typical CPP roles, responsibilities, authority, and standards of care. 5 We inquired whether each of the B-MOUD related tasks were typically conducted by the CPP and/or other members of the clinical team. The survey also included 3 yes/no questions that provided opportunity for comments that inquired (1) whether the respondent believes they are providing care formally as a CPP; (2) whether they function as a “primary conduit” for the OUD patient to the health care team; and (3) whether the CPPs do or would prescribe B-MOUD if their state license would allow it. Our a priori intentions were not to analyze these results through any qualitative methodology and subsequently did not.
Study data were collected and managed using REDCap electronic data capture tools hosted at the VA Information Resource Center.43,44 Data was collected and analyzed using descriptive statistics; we did not need to adjust for any missing data.
Results
Twenty-two CPPs responded to the survey. Respondents indicated they were licensed to practice in 17 different states and reported practicing in 15 states. Respondents worked in pain clinics (40.9%), primary care (27.3%), mental health (22.7%), and mental health-primary care integrated clinics (22.7%; multiple settings could be chosen).
Table 1 indicates 25 patient tasks associated with intake, initiation, monitoring and risk assessment, follow-up, and quality assurance/outcome activities typical for CPPs which were specific for B-MOUD episodes of care. The highest CPP reported tasks involved naloxone education and distribution (n = 21, 95.5%), follow up management (n = 21, 95.5%), SUD medication review (n = 20, 90.9%), general medication review (n = 19, 86.4%), relapse prevention (n = 19, 86.4%), and opioid/B-MOUD tapering (n = 18, 81.8%). Conversely, prescribing controlled substances (n = 5, 22.7%) and initiating MOUD by prescribing (n = 6, 27.3%) were the lowest reported activities by CPPs.
Buprenorphine Medication Treatment for Opioid Use Disorder Tasks (n = 22 Respondents).

Participants were allowed to select more than 1 person with primary responsibility so columns can exceed 100%.
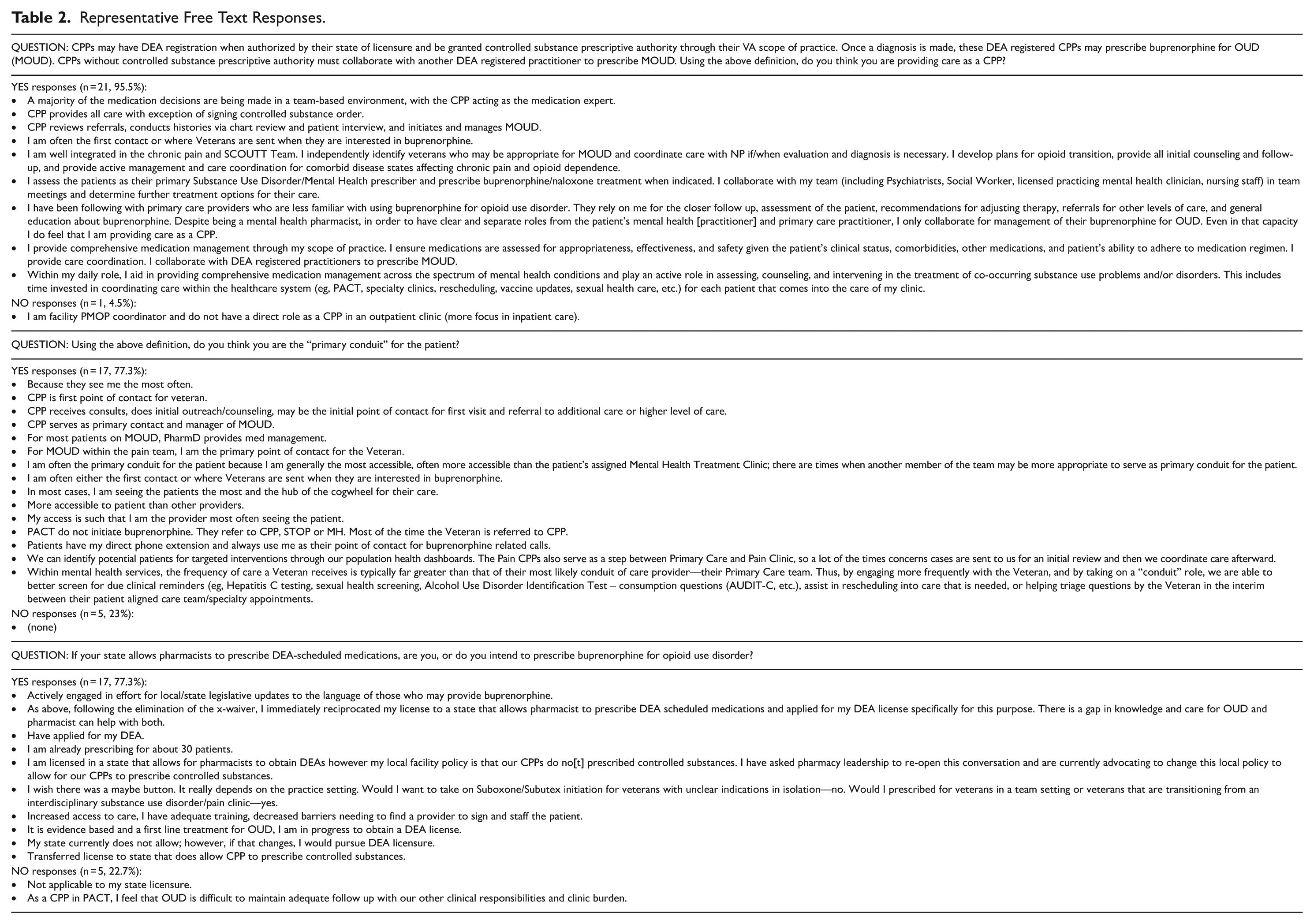
CPPs overwhelmingly agreed that activities and tasks they work on meet a formal definition of a CPP providing B-MOUD care (n = 21, 95.5%). In addition, many reported functioning as the “primary conduit” for the OUD patient to the health care team (n = 17, 77.3%) and would prescribe B-MOUD if their state license allowed it (n = 17, 77.3%).
Table 2 indicates corresponding free text responses under each of the free-text questions. Regarding their roles as a CPP in B-MOUD prescribing, many indicated that they are “integrated,” serve as a “medication expert,” and provide “comprehensive medication management.” CPPs indicated that for the most part they are the point of contact for patients with OUD interested in MOUD. Many CPPs indicated they were prescribing B-MOUD, were working toward prescribing, or were willing to prescribe.
Representative Free Text Responses.
Discussion
In a survey of VHA CPPs participating in SCOUTT, we found CPPs engaging in roles and activities that facilitate access to B-MOUD in non-specialty SUD settings. We found that responding CPPs participate in various aspects of patient care including serving as medication experts and medication management providers and were comfortable making or suggesting B-MOUD medication changes for their Veteran patients. Not all the 25 tasks we inquired about were performed by all CPPs, however, enhancing access to B-MOUD and care management of patients on B-MOUD are frequent tasks performed by SCOUTT CPPs. Opioid risk and risk mitigation activities (eg, prescription drug monitoring program checks, naloxone education and distribution) were near universal tasks performed by SCOUTT CPPs. We found that many SCOUTT CPPs were performing “initial reviews” of patients being considered for B-MOUD. This bodes well for potential expanded access in B-MOUD, especially if CPPs have prescriptive authority to prescribe B-MOUD.
Seventy-three percent (n = 16) of CPPs reported that they prescribe non-controlled medications for medical and mental health conditions while less than a quarter reported prescribing controlled substances. Controlled substance laws play a significant influence in CPP prescriptive authority in providing MOUD.26,45 However, even in areas where state law does not authorize pharmacist DEA registration, CPPs still provide a valuable perspective on how to manage opioid withdrawal, assisting patients with initiating MOUD and timely follow-up, and prescribing non-controlled substances that could aid in relieving discomfort or co-morbid conditions and improving outcomes. CPPs in our survey indicated involvement in most tasks associated with B-MOUD care management.
Our results provide more evidence of the expanding role of CPPs in addressing and treating OUD and preventing overdoses. Most respondents (n = 17, 77.3%) saw themselves as the primary conduit for connecting the patient to health care services, including MOUD. Our results may demonstrate that CPPs are prepared and willing to engage in the different phases of patient care for OUD, including the direct prescribing of B-MOUD. In our survey, 21 out of 22 CPPs self-reported having a DEA registration to prescribe B-MOUD or collaborate with another DEA registered practitioner to prescribe B-MOUD after the OUD diagnosis is made. They indicated that they served as the medication management provider and were comfortable making or suggesting medication changes for their patients.
When asked if they are prescribing buprenorphine for OUD (or would if their state allowed pharmacists to prescribe DEA-scheduled medications), a vast majority (86.4%) stated they would. CPP prescribing may be ideally suited to prescribe B-MOUD or assist busy primary care, mental health, or pain clinicians in prescribing B-MOUD in non-SUD-specialty care settings. As pharmacists are among the most trusted health care providers, 46 B-MOUD prescribing or assistance in prescribing B-MOUD, may reduce stigma of OUD and ultimately improve access to barrier-free B-MOUD treatment. While much attention has been given to pharmacies not stocking formulations of B-MOUD—perhaps due to stigma against patients with the disease, the disease itself, and/or the B-MOUD treatment—CPPs, as treatment providers, may serve as another member of the health care team to engender trust and rapport with patients with OUD.47-50 In addition, CPPs are a willing and capable resource available to provide B-MOUD in busy non-specialty clinics, thus enhancing reducing the care burden of other providers.
In July 2024, the American Society of Addiction Medicine called on “states to develop programs to promote best practices in, and incentivize appropriately qualified, licensed physicians and pharmacists to engage in, patient-specific collaborative practice agreements for addiction medications, including reimbursement for pharmacists’ services.” 51 While there has been recognition of the clear potential for CPPs and pharmacists to expand access to B-MOUD in the US, several challenges to implementation remain.11,52 It may be easier for CPPs to engage in B-MOUD care and/or prescribing in large health care settings like the VHA, it may be more difficult to establish collaborative practice agreements within community pharmacies, particularly in remote, rural areas. To expand pharmacists’ roles in B-MOUD care, developing competencies in this care through training and certification (eg, through the pharmacy boards), may require time, effort, and resources. Reimbursement models for this type of care likely need to be further developed.
Limitations
Our results are limited due to the convenience sample of CPPs at select VA facilities within primary care, mental health, or pain clinic environments that affiliated with SCOUTT; CPPs in other settings may not have responded similarly. In addition, we did not seek to or report on the different roles that CPPs may have had in different clinics (primary care, mental health, or pain clinics). We are unable to determine if we were able to capture the responses of all CPPs who are involved in SCOUTT. The survey was designed and pilot tested by the authors prior to execution; no further validation of the survey occurred. In addition, CPPs in the survey were not provided contexts regarding B-MOUD care or roles and responsibilities of other team members and respondents may not have responded to the survey based on similar clinical environments or staff. However, the VHA has standard clinical structures in primary care, mental health, and pain clinics where the roles and responsibilities of team members are relatively well defined, and our work further defines what roles and responsibilities CPPs may play for OUD and MOUD care in VHA environments.8,12 In addition, the VHA is unique; the VHA provides clinical care within a team-based, collaborative care environment to address OUD and MOUD. The SCOUTT primary care, mental health, or pain clinic environments to provide MOUD care are not common outside the VHA; CPPs in primary care, mental health, or pain clinic environments outside the VHA may have responded quite differently to our survey. Finally, CPPs or community pharmacists outside the VHA may be ill-equipped or not credentialed to provide OUD and/or MOUD care. While we found that CPPs within SCOUTT are willing and able to provide OUD and MOUD care, it is not certain that this model can be implemented outside of SCOUTT or in non-VHA environments.
Conclusions
Despite these limitations, we found that CPPs who responded to a survey within SCOUTT provide a variety of services in VA clinics to enhance access to MOUD and specifically B-MOUD. Further research is needed to examine how this model of care can be expanded within and outside the VHA, including need for training, state practice acts that authorize pharmacist DEA, reimbursement models for this care, and addressing implementation challenges. Further inclusion of CPPs in B-MOUD activities, including prescribing, may improve the access of B-MOUD for patients and improve outcomes for patients with OUD.
Supplemental Material
sj-docx-1-sat-10.1177_29768357251381070 – Supplemental material for The Roles, Activities, and Opportunities of Clinical Pharmacists in a National Initiative to Improve Office-Based Buprenorphine Care
Supplemental material, sj-docx-1-sat-10.1177_29768357251381070 for The Roles, Activities, and Opportunities of Clinical Pharmacists in a National Initiative to Improve Office-Based Buprenorphine Care by Spencer G. Calder, Marie E. Kenny, Veldana Alliu, Terri L. Jorgenson, Tera Moore, Hildi J. Hagedorn, Eric J. Hawkins and Adam J. Gordon in Substance Use: Research and Treatment
Footnotes
Acknowledgements
The authors wish to acknowledge the contribution of Karen Drexler and Joseph Liberto for their leadership in the SCOUTT Initiative. Furthermore, the authors wish to acknowledge Veteran Health Administration clinicians who contributed to the vision and success of the implementation of the SCOUTT, particularly the clinical practice pharmacists who are participating in SCOUTT and were willing to complete our questionnaire.
Acronyms
AUDIT-C: Alcohol Use Disorders Identification Test
B-MOUD: Buprenorphine Medication treatment for Opioid Use Disorder
CPP: Clinical Pharmacist Practitioner
DEA: Drug Enforcement Agency
MH: Mental Health
MOUD: Medication treatment for Opioid Use Disorder
NP: Nurse Practitioner
OUD: Opioid Use Disorder
PACT: Patient Aligned Care Team
PDMP: Prescription Drug Monitoring Program
PharmD: Doctor of Pharmacy
PMOP: Pain Management Opioid Safety and Prescription Drug Monitoring
PROMS: Patient Related Outcome Measures
REDCap: Research Electronic Data Capture
SCOUTT: Stepped Care for Opioid Use Disorder Train the Trainer Initiative
STROBE: Strengthening the Reporting of Observational Studies in Epidemiology
SUD: Substance Use Disorder
VA: Department of Veterans Affairs
VHA: Veterans Health Administration
Author Note
The views expressed in this article are those of the authors and do not necessarily reflect the position or policy of the US Department of Veterans Affairs or any academic institution.
Ethical Considerations
The VA Salt Lake City Health Care System and University of Utah Institutional Review Board confirmed that this quality improvement evaluation did not require approval as human subjects research.
Consent to Participate
Respondents to the anonymous survey provided implicit consent to participate in this evaluation and could have terminated their participation at any time.
Author Contributions
All authors contributed consistent with CReDiT criteria. AJG, MK, and SC conceptualized this study. AJG acquired funding. MK and SC obtained, curated, and analyzed the data. SC and AJG initially drafted the manuscript. All authors contributed to the writing, review, and final approval of the manuscript prior to submission.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the U.S. Department of Veterans Affairs (VA), Office of Mental Health, Veterans Health Administration (VHA); the Vulnerable Veteran Innovative Patient-Aligned-Care-Team (VIP) Initiative at the VA Salt Lake City Health Care System; the VA Center of Excellence in Substance Addiction Treatment and Education (CESATE); the VA Health Systems Research (HSR) Quality Enhancement Research Initiative (QUERI) Partnered Evaluation Center (PEC) grants #19-001 (principal investigator: author AJG) and #18-203 (principal investigator: author EJH). Infrastructure support for author AJG was provided, in part, by the Greater Intermountain Node (GIN; NIH/NIDA 1UG1DA049444) of the National Institute on Drug Abuse Clinical Trials Network and the Department of Veterans Affairs Health Systems Research Informatics, Decision-Enhancement, and Analytic Sciences (IDEAS; CIN 13-414) Center of Innovation. Supporting organizations had no further role in the design and conduct of the evaluation; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: TLJ is on the Board of Directors for the Maryland Society of Health System Pharmacists and is a member of the House of Delegates for the American Society of Health System Pharmacists and receives no renumeration for either role. AJG reports an honorarium from the medical online resource UpToDate, Inc, for an authored chapter unrelated to this work. AJG has served, in the last 3 years, on the board of directors for the American Society of Addiction Medicine (ASAM), the Association for Multidisciplinary Education and Research in Substance Use and Addiction (AMERSA), and the International Society of Addiction Journal Editors (ISAJE), all not-for-profit organizations that he received no remuneration. AJG receives remuneration from AMERSA for his Editor-in-Chief role of the organization’s peer reviewed journal.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.