
Abstract
Background:
Evidence-based practices to treat opioid use disorder (OUD) include behavioral interventions and medications to treat OUD (MOUD). Each type of treatment has unique systems-level challenges that limit care access and care engagement. It is important to identify and address these challenges and provide evidence-based strategies to reduce barriers.
Methods:
In this narrative review, systems-level barriers that impede OUD treatment service delivery are reviewed by treatment type (MOUD, cognitive behavioral therapy, and contingency management), and how recent regulatory changes have the ability to reduce or alter these barriers are discussed. To do so, we review empirical literature and regulatory documents to cover the breadth of this topic.
Results:
Several OUD treatments that have established effectiveness are not able to reach full potential (ie, dissemination, uptake) because of systems-level barriers, notably related to rigid regulations, broad perceptions of treatment, and training and financing constraints. Recent changes aim to lessen restrictions surrounding MOUD delivery (eg, greater allowance for take-home doses of methadone) and allow for delivery of MOUD in innovative settings (eg, mobile health units). There are also reduced restrictions at the treatment provider level, including removal of the X-waiver. Despite lowering some barriers, OUD treatment delivery is still barred by strong forces related dominantly to stigma and financing.
Conclusions:
Future research directions to further understand and enhance effective OUD treatment delivery are identified, including the need to address individual, organizational, and external factors that surround the implementation of regulatory changes.
Keywords
Highlights
Systems-level barriers impede the delivery of all opioid use disorder treatments.
Recent regulatory expansions have improved some access.
Further research/practice areas identified to further improve access and engagement.
Background
Despite the significant harms associated with opioid use in the United States (US) over the past 2 decades, treatments for opioid use disorder (OUD) are not effectively delivered.1,2 There is a well-documented gap in the use of such treatments for OUD, including medications to treat OUD (MOUD) and psychosocial interventions. 1
Each type of OUD treatment has unique individual- and systems-level challenges that limit access to services and engagement with care. Systems in the US, for example, the health care, criminal-legal, and social service systems, are all key to accessing health services for people with OUD. 3 These structures have policies and practices that can facilitate or impede individuals’ ability to access care. 4 Some of these barriers are objective (eg, lack of funds) while others are subjective (eg, culture of stigma). 4 Systems-level challenges require more effort to mitigate, compared to individual-level factors. 5 To expand care access, it is important to address these challenges and identify solutions as they relate to the current landscape of OUD treatment in the US.
Previous reviews have discussed the individual and systems-level challenges associated with the treatment of OUD in the US1,6,7 but have not considered the type of OUD treatment or recent regulatory changes. For example, permanent expansion of take-home methadone dosing and telehealth initiation of MOUD under 42 CFR Part 8; removal of prescriber waiver requirements for buprenorphine; consideration of allowing pharmacy dispensing of methadone; updated Medicaid eligibility and prior-authorization rules; and state limits on initial opioid prescriptions.8-10 Prior reviews have found that research on OUD treatment encompasses many treatment types, although only a few treatments are substantially effective in reducing health and social harms associated with opioid use.1,6,7 To our knowledge, this review is the first to directly examine systems-level challenges to each OUD treatment type and address how these challenges may be addressed in an evidence-based way. The objective of this review is to provide an overview of systems-level challenges to OUD treatments and to propose future directions to alleviate these barriers.
Methods
This narrative review details systems-level barriers that impede OUD treatment service delivery, recent regulatory changes that have the ability to reduce or alter these barriers, and areas for future research. Given the focus on examining current literature on this broad topic, plus a distillation of future research and areas for practice, a narrative review was an appropriate methodology for this research question. 11
Empirical literature was reviewed in conjunction with regulatory documents to gain a full scope of the current knowledge base on regulatory changes and how they impact OUD treatment delivery. Narrative reviews do not seek to cover all articles or references on a given topic. 11 References selected to be included in this review were appraised by the authors as, collectively, providing a comprehensive understanding of the topic (ie, treatment type, barrier type, and regulatory change) with the use of rigorous methods, when possible. Per typical narrative reviews, we sought to provide a breadth of knowledge on systems-level barriers to OUD treatment, not depth. Included references were published in peer-reviewed journals, gray literature, and government websites or reports. Specifically, for peer-reviewed articles, we reviewed literature indexed in PubMed that pertained to the term “opioid use disorder.” Our search for literature snowballed from the initial PubMed search, with additional peer-reviewed sources sought on specific topics that arose (eg, take-home methadone dosing), and, when relevant, additional governmental sources were sought for relevant regulations and statistics. Literature relevant to the past 5 years of regulatory changes related to OUD treatment (since January 2020) was considered. Literature could have pre-dated 2020 but had to be pertinent to current systems-level issues in this space. All studies reviewed were published in English. Most were published within the US, given the geographic focus of this review.
Primary coverage is given to the leading treatments for OUD in the US, for which there is empirical literature supporting effectiveness. First, for each treatment, the manuscript describes the treatment and its effectiveness, examines current barriers to each treatment at the systems-level, and, in light of these barriers, outlines areas for future research addressing each treatment. Second, an overview is provided of important regulatory changes and their impact on barrier mitigation, including positive impact, potential, and limitations. In accordance with determinant frameworks used in the interdisciplinary field of implementation science, 12 in this review, we sought to identify determinants of success for OUD treatments; we provide a breakdown of these determinants for each treatment type (barriers and facilitators) in Table 1 so that findings can be readily interpretable for future research that seeks to advance the success of the implementation of MOUD-delivering interventions.
Key Systems-Level Determinants (Barriers and Facilitators) Influencing the Delivery and Uptake of Different OUD Treatments.
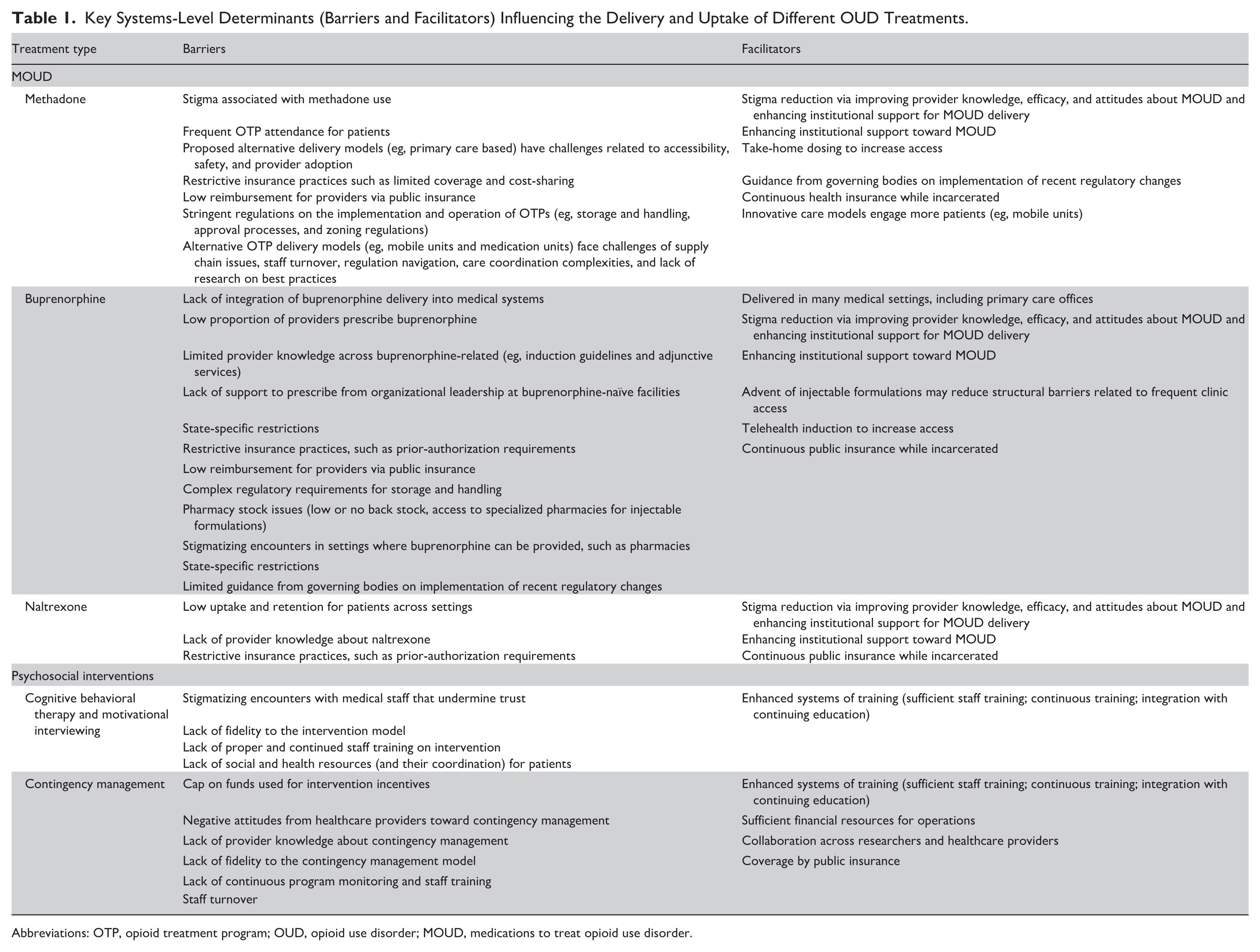
Abbreviations: OTP, opioid treatment program; OUD, opioid use disorder; MOUD, medications to treat opioid use disorder.
Results
Medications to Treat OUD
Methadone, buprenorphine, and naltrexone are the Food and Drug Administration-approved MOUD. 13 The goal of MOUD utilization can be: (1) opioid abstinence, (2) withdrawal reduction, (3) short-term detoxification, and (4) long-term maintenance. 14 Because of the risk of returning to opioid use and overdose while completely abstinent from medication, maintenance on MOUD is often the most effective care for individuals with OUD.4,15 MOUD are essential to reduce health risks associated with OUD, including fatal overdose. 16 Below, systems-level challenges to MOUD delivery are discussed.
Methadone
Methadone is administered orally and dispensed from licensed clinics called opioid treatment programs (OTPs), certified and regulated by the Substance Abuse and Mental Health Services Administration (SAMHSA). 14 Methadone is well-researched with documented safety, efficacy, and effectiveness.4,17,18 Despite the effectiveness of methadone, there are still many barriers to delivery in the US.
The largest barrier to methadone delivery is the stigma associated with methadone use. Stigma is perpetuated by players involved in the OUD cascade of care, 19 including medical providers, pharmacists, family and friends, and other community members. Provider and support staff concerns about patient methadone diversion may deter offering methadone at all, exclude certain patients, or prevent staff from appropriately increasing methadone dosage. 20 Stigma is pervasive; it can be internalized and perpetuated by individuals with OUD. 21 In turn, individuals who experience stigmatizing interactions are less likely to engage in methadone treatment. 22
Other contextual factors surrounding methadone delivery systematically exclude patients. Historically, patients were required to physically attend an OTP daily, sometimes twice daily, to receive their methadone dose while being monitored by staff. This schedule was difficult to maintain for most patients, and especially for patients who were employed, who had limited transportation options, and who were parents. Ultimately, this restrictive structure, along with other factors related to methadone prescription, has led patients to describe the system for receiving methadone as “liquid handcuffs.” 23 Provision of methadone from primary care offices is being considered to alleviate stigma in methadone delivery. 24 However, challenges associated with the office-based methadone delivery model need to be addressed, such as providers not electing to provide methadone 14 and concerns over accessible training to appropriately and safely administer methadone.
Structural Economic Barriers Exist
The delivery of methadone is shaped by the financing and payment structures of healthcare. A recent review by Bowser et al identified distinct payment-related obstacles to methadone access and retention for patients and providers. 25 Patient engagement in methadone treatment is constrained when commercial insurances or state Medicaid programs limit coverage of treatment services, impose cost-sharing or restrict take-home doses, and when indirect expenses (eg, childcare) prevent attendance. For providers, low Medicaid reimbursement or onerous prior-authorization requirements discourage providers from offering or expanding methadone, which in turn limits the availability of care. 25 Hence, the way in which medication is covered for patients plays a driving role in methadone delivery. Aligning delivery reforms, such as expanded telehealth or take-home dosing, demands parallel payment reform to reduce these structural economic barriers.
Government regulation can also present as a significant barrier to methadone delivery. Unlike many other health services, the establishment of an OTP is not simply an organizational decision. It is tightly regulated at the federal, state, and local levels, creating substantial obstacles to program expansion. Regulations dating back decades continue to require that methadone for OUD be dispensed predominantly through federally certified OTPs, and states often layer additional restrictions such as caps on the number of clinics, lengthy approval processes, or community support requirements. 26 In some jurisdictions, state moratoria and restrictive land-use or zoning laws further impede new OTP development, effectively limiting access even in areas with high overdose rates. 27 These regulatory constraints contribute directly to the marked geographic disparities in methadone access, with many rural and underserved regions lacking a single OTP, despite need. 28 Addressing these barriers requires modernizing federal OTP regulations and curbing local and state restrictions that unnecessarily constrain the treatment landscape.
Buprenorphine
Buprenorphine effectively treats OUD and reduces overdose risk, physical dependence, and withdrawal symptoms. 4 Buprenorphine can be favorable to methadone because it can be prescribed in an office-based setting, such as primary care. Buprenorphine is administered sublingually and through long-acting injectable formulations. 29
While buprenorphine is prescribed in more settings than methadone, retention rates for buprenorphine are often lower than those for methadone. 15 On the systems-level, there is a lack of integration of buprenorphine delivery into medical systems, and there are few providers who prescribe buprenorphine. Historically, prescribing providers were federally required to complete additional training to be certified to legally prescribe buprenorphine outside of an OTP (“X-waivered”) with a limit on the number of patients who could receive buprenorphine (Drug Addiction Treatment Act 2000-Waiver Program). Under the Consolidated Appropriations Act, 2023, prescribers were no longer required to receive this certification and no longer have a limit on the number of patients prescribed buprenorphine (Section 1262).30,31 The removal of these requirements aimed to increase the number of providers who prescribe buprenorphine and expand access to care.
Although the number of prescribers has increased over the past decade, 32 the growth in overall prescribing rates has lagged. 33 Efforts to expand buprenorphine access emphasize greater integration into medical systems, including a protocol for buprenorphine induction in emergency departments followed by referral to long-term care. 4 Barriers to buprenorphine prescribing among medical professionals include limited knowledge regarding induction guidelines and adjunctive services, lack of support to prescribe from organizational leadership,34,35 and state-specific restrictions. 36
Healthcare financing and payment systems pose barriers for organizations providing buprenorphine. Insurers, both private and public, often require burdensome prior-authorization processes that delay treatment, and many programs report inadequate reimbursement from insurers. 35 Organizations must invest in infrastructure and staffing to support medication management, yet low reimbursement rates may not cover care coordination, laboratory monitoring, or nursing time, making the office-based model financially unsustainable. Moreover, even when coverage is available, providers must still comply with complex regulatory requirements: for example, dispensing buprenorphine means complying with federal Drug Enforcement Administration (DEA) rules on storage and administration of controlled substances, which require locked cabinets, detailed logs, and readiness for DEA audits. Together, these payment and regulatory burdens discourage many organizations from offering buprenorphine or limit the number of patients they serve, thereby reducing access to this medication.
Lastly, for buprenorphine barriers, low or no back stock of buprenorphine at pharmacies and access to specialized pharmacies for injectable buprenorphine present a significant barrier to patients and can delay patient access, even if it has been prescribed. 37 Pharmacy-related barriers, including no stock, insurance issues, and stigmatizing encounters with staff, can deter patient utilization of buprenorphine.38,39
Naltrexone
Naltrexone is a treatment for OUD,40,41 though it is not considered a first-line treatment. 42 Naltrexone is most often provided intramuscularly via a monthly extended-release injectable formulation. 40 Compared to a placebo, naltrexone has some benefits.40,43 However, retention is low compared to buprenorphine and methadone.15,44,45 The antagonist mechanism of naltrexone poses barriers as it traditionally requires patients to be in complete withdrawal from opioids before initiating naltrexone and may not alleviate cravings. 7 Low rates of naltrexone utilization indicate that patients do not desire it or experience additional barriers to initiate and continue naltrexone compared to other MOUD.46,47 For providers, other barriers to office-based naltrexone delivery exist, including prior authorization and complicated requirements for health insurance coverage, and a lack of provider knowledge about naltrexone.47-49
Future Directions for MOUD
For MOUD delivery, first, future research and practice directions mostly center on stigma reduction efforts, such as the development of interventions to reduce stigma toward methadone and MOUD broadly, among community members and medical providers.20,50 Key strategies to reduce stigma include improving provider knowledge, efficacy, and attitudes about MOUD and enhancing institutional support for MOUD delivery.51,52 Second, evaluating MOUD outcomes by type is essential to determine which course of treatment is most effective and might be most helpful for individuals with certain characteristics or behaviors. 53 The use of a monthly injectable buprenorphine product is especially of interest for patients who have more difficulty accessing a daily dose of medication (eg, transportation barriers), and it additionally reduces diversion risk, which interests relevant stakeholders. 54 Future research efforts will need to compare retention between the extended-release formulations of buprenorphine, naltrexone arm implants, and methadone.7,55
Psychosocial Interventions
Psychosocial interventions for OUD encompass a range of evidence-based approaches and include psychological and behavioral treatments and services that can be provided in a variety of settings. These interventions can have some benefit and can be paired with MOUD, counseling, and social support. Psychosocial interventions address underlying thought processes and comorbidities that exacerbate OUD while also encouraging MOUD. 56 Common psychosocial interventions include cognitive behavioral therapy (CBT), contingency management (CM), and motivational interviewing (MI).57,58 The choice of psychosocial intervention should be individualized. Several evidence-based options have established effectiveness for OUD treatment.
CBT and MI
CBT focuses on cognitive (ie, motivational enhancements) and behavioral (ie, replacing cues to use opioids) elements of recovery. Compared to no treatment, CBT effect sizes are large; however, compared to MOUD, CBT alone is not comparable.59,60 CBT is most effective in treating OUD in conjunction with MOUD.59,61 Alternatively, MI is used to initiate patients in treatment and enhance motivation to engage in treatment and related behaviors. Specifically, a counselor forms a collaborative and supportive relationship with a patient to target ambivalent thoughts about behavior change and discusses how to manage barriers to change. MI has limited effectiveness in treating OUD when not combined with other treatment services. 61 Both interventions are key tools to improve mental health and well-being, especially for individuals with OUD who have a co-occurring mental health condition. 61 Systems-level challenges to CBT and MI are barriers faced by most other OUD treatment interventions, such as the experience of stigmatizing encounters with medical staff that undermine trust, fidelity to the treatment model, proper and continued staff training, and lack of social and health resources (and their coordination).52,61
CM
CM interventions provide positive reinforcement for desired behaviors. Patients are rewarded for abstinence from or reductions in substance use as evidenced by negative urine drug screens. Researchers are exploring rewards for medication adherence and appointment attendance, but these have shown limited outcomes and face legal barriers.62,63 The goal of CM is to reinforce positive behaviors and enhance retention in CM. The most common reinforcements for each positive behavior utilized are (1) a voucher system, where a patient receives vouchers redeemable for an item, and (2) a prize-based or cash system. The amount/magnitude of reinforcement increases over time as the participant achieves longer periods of positive behavior (often longer periods of no substance use).64,65 CM is the only behavioral intervention proven to improve MOUD outcomes, compared to other psychosocial approaches like CBT or MI. 59 CM in conjunction with MOUD is associated with a higher rate of treatment retention compared to only MOUD 60 and reduces opioid and cocaine use. 66 CM remains underutilized in the US 67 there are systems-level challenges to CM delivery.
One significant challenge to the implementation of CM is the federal restriction that prohibits federal spending of over $75/year for individual patients. 68 CM provided under these regulations is insufficient to promote behavior change and reduces CM effectiveness. 69 However, a recent SAMHSA advisory has increased this limit to $750/patient annually, thereby providing substantially greater flexibility to implement the higher-magnitude incentives shown in research to sustain patient engagement, improve treatment adherence, and ultimately reduce substance use and relapse rates. 70 This 10-fold increase is anticipated to enhance both the effectiveness and scalability of CM interventions funded through federal mechanisms.
Behavioral health and medical providers’ perceptions of CM challenge delivery and include stigma, attitudes, and lack of knowledge, are challenges to CM delivery. For example, providers may be concerned that patients will use CM cash prize to buy substances and that CM is not addressing the individual’s readiness to change. Although none of these concerns have been found to negatively impact patient outcomes, CM interventionists may consider managing these perceptions when they work with providers.63,67 These perceptions may be exacerbated by the lack of formal CM education, the disconnect between research on CM and practice of CM, and the lack of continuous monitoring for program fidelity. 71 Additional CM-delivery-related barriers (eg, continuous training, staff turnover) can muddy the success of implementation in healthcare settings. 72 Overall, these challenges can reduce the effectiveness of CM delivery and have the potential to cloud the evidence base of CM outcomes.
Future Research Directions for Psychosocial Intervention
The evidence base generally supports that psychosocial interventions can provide benefit for some individuals with OUD when combined with MOUD, though the extent of benefit varies across interventions and populations. 61 Given the promise of psychosocial interventions to benefit individuals with OUD, especially those with co-occurring mental health conditions, use of these interventions with MOUD may mitigate key mental health issues. Key barriers to CBT and MI should be addressed so that these interventions can benefit more individuals who are receiving MOUD, like integration of services within multidisciplinary treatment clinics for greater care coordination and robust staff training. 73 Because of the promising outcomes of CM plus MOUD, there are several future directions for the delivery of CM.
To address workforce issues related to CM, enhanced training, resource development, and collaboration are needed. For example, increasing the skills and competencies of clinical staff. Evidence-based training should be intensive, didactic, and include the use of case examples and role-play activities. To support sustained benefits, training should extend over multiple sessions rather than a single encounter, allowing participants enough time to reinforce and retain key concepts.63,69 Some examples of resources for training include the development of practical materials to train CM providers and to inform implementers’ planning efforts 66 ; and other specific training programs.74,75 In addition, enhancing systems of training (such as integrating CM education into continuing education credit programs and partnering with major providers of addiction services training) can help build a more knowledgeable, confident, and sustainable workforce. By embedding standardized CM training within widely accessed professional development platforms, health systems can increase provider competency, support fidelity to evidence-based protocols, and expand the pool of clinicians equipped to deliver CM effectively. 76 Lastly, it is pertinent to enhance academic/research and practice collaboration to seamlessly translate evidence-based research into practice.63,67
Take-Homes, Telehealth, and Section 1115
Considerable policy efforts have been enacted to lessen restrictions surrounding methadone and buprenorphine delivery to better engage individuals. A few changes included allowance of take-home doses of methadone, including allowing patients to receive take-home doses upon entering treatment, and allowing initiation of buprenorphine via telehealth with a trained medical provider, for indicated patients and based upon clinical judgment.77-79 These changes contributed to many benefits, such as increased patient autonomy, with no attributable increases in opioid-related mortality.80-87 At the onset of these lessened restrictions, providers reported uncertainties around how to appropriately administer these changes 81 ; suggesting that governing bodies should provide more guidance and technical assistance. In addition, patients may face more salient barriers to receiving MOUD, such as issues picking up buprenorphine from pharmacies 37 and unstable housing (complicating MOUD storage). 88
Despite relaxed flexibilities, restrictive requirements to prescribe and dispense methadone and buprenorphine remain. The ability to practice with these lessened regulations is dependent on the state in which a provider is practicing, meaning that providers in restrictive states do not have the same agency to provide care to patients compared to states that have lessened regulations. In addition, provider use of discretion can limit access for patients, based upon clinical judgment. These discretionary roles can limit or expand access to take-home doses and telehealth appointments for patients.
Importantly, the SAMHSA final rule on MOUD delivery in 2024 does not address the provision of care for individuals who are incarcerated (at a facility not registered with the DEA as a hospital/clinic) or transitioning into the community upon release from correctional settings.8,77 This population is particularly in need of continuous healthcare services due to complex health needs and health insurance discontinuity. 89 Encouragingly, the US Department of Health and Human Services authorized 11 states to expand Medicaid and provide coverage for mental health and drug treatment for incarcerated populations in US states 90 days before their release from incarceration (among those who are otherwise eligible for Medicaid; Section 1115 of the Social Security Act [42 U.S.C. § 1315]). 90 This expansion has critical implications for substance use treatment provision during the critical period upon release into the community.91,92
X-Waiver
Findings across multiple settings suggest either no changes in the number of providers prescribing buprenorphine or no significant increases in the number of patients receiving buprenorphine after the X-waiver removal.93-95 Findings to date suggest that other, more salient factors limit the expansion of buprenorphine prescribing. 95 The changes heralded by the Consolidated Appropriations Act warrant further research to see whether systems will need to incentivize prescribers to provide buprenorphine (eg, increase protected provider time), to break down ideological barriers (ie, stigma) among healthcare systems and providers, or to enhance knowledge and self-efficacy among primary care providers.96,97
Mobile Provision of Medication
For over a decade, OTPs could not receive DEA approval to operate mobile units (ie, van) to prescribe or deliver methadone. 98 In June 2021, regulations were modified to allow OTPs to operate mobile units that provide methadone to clients.99,100 As of October 2025, 75 methadone-providing units were registered in the US. 101 The operations of mobile units are further supported by modifications addressed in SAMHSA’s final rule (2024; ie, expansion of geographic access for medical units; take-home dosing, telehealth). 8 While the changes in regulations and growth in mobile unit rollout are promising, there are still logistic concerns. These include: upfront expenses, supply chain issues, and vehicle maintenance; barriers related to staff turnover, shortages, and coordination of schedules; complex process of obtaining licensure and certifications to expand service provision (eg, rapid infectious disease testing); lack of research on best practices; long-term reimbursement for telehealth services; and the need to engage more communities and participants with this innovative model.25,99,102-104
CM Expansion
California is the first to expand CM reimbursements via the use of Medicaid funds for individuals with stimulant use disorder (CalAIM1115 Demonstration).105,106 This pilot is essential to demonstrate the process and outcomes of expanded CM access on a larger scale. Preliminary process data from the implementation of CalAIM115 show encouraging participation with the program, suggesting a path forward for broader expansion. 107
Discussion
Barriers that challenge the delivery of OUD treatment are evident within several systems that impact the health of people with OUD, including OTPs, primary care offices, other treatment centers, criminal-legal facilities, and the general community. Recent regulatory changes and proposed changes aim to reduce some of these barriers to care via lessening regulations surrounding MOUD delivery and allowing for delivery of MOUD in more innovative settings, and reducing regulatory restrictions for the treatment provider and the system they work within. Despite lowering some barriers, systems-level challenges remain for OUD treatment delivery. Community, organizational, and provider stigma, and medical and behavioral health workforce development challenges remain as significant barriers. We provide holistic future directions for research and practice.
Organization culture (eg, lack of administrative support and staff turnover) and, relatedly, workforce education (ie, knowledge, awareness, and exposure) appeared to be salient barriers to OUD treatment delivery across treatment contexts, including at OTPs that reliably deliver methadone, mobile units that recently began operating as extensions of OTPs, and in pharmacy-based settings (ie, where buprenorphine can be delivered, where it has been proposed methadone can be delivered). These barriers of culture and education are interwoven with stigma toward patients and treatment as well, for example, lower knowledge being associated with negative provider attitudes toward MOUD. 108 Similar patterns are evident in other geographic and regulatory contexts. In the United Kingdom, where methadone can currently be accessed at a pharmacy, organizational culture and workforce barriers to methadone delivery include high pharmacist workload and stigma toward patients receiving methadone. 109 Therefore, findings from UK demonstrate similar gaps and areas for improvement in OUD delivery cascades, centering on continued, comprehensive, and formalized education for providers, which is enforced and supported by governing bodies.
Systems-level barriers described in this review are faced in other communities around the globe. Amsterdam operated one of the earliest documented mobile units to provide methadone 110 and led in policy-supported harm reduction practices in the late 20th century. Despite being early adopters of these practices, the provision of OUD treatment and related healthcare in Amsterdam in the past few decades has been hampered by systems-level social and political barriers (ie, focus on crime prevention over rehabilitation or support, lack of funding for services). 111 Such barriers related to a lack of political support and funding impact the delivery of OUD treatment types in the US. In response to these barriers, in the context of Amsterdam, some proposed solutions include regulations that center the health of people with OUD and who use substances (eg, legal regulation of substances) and allowing people with lived experience to have a central voice in policy and practice changes. 111 These proposed solutions to some systems-level barriers highlight the role of using patient voices to effectively adapt policies or practices.
Across OUD treatment-related interventions, it is essential to think about how to effectively reduce stigma in medical and community settings14,55 and efficiently personalize OUD treatment delivery to enhance outcomes,53,112 although these efforts may require further coordinated systems-level change. An overarching area for future research is to study whether recent regulatory changes increase access to and provision of treatment, and enhance the quality of the treatment provided to individuals; whether clinical staff and organizations find the implementation of these new strategies to be feasible and effective to keep patients engaged with care; and how other external factors (in addition to the regulatory changes in question) may impact patient-level outcomes and the ability for systems of care to adopt these strategies. Throughout the integration of bringing regulatory changes into practice, it will also be necessary for implementers to monitor which stage of the process the changes are in and whether that stage impacts the ability of the regulatory change to increase access to care (ie, planning, implementation, and sustainment).113,114 Since certain providers, organizations, and federal policies all impact whether the regulatory changes will be adopted, it will also be necessary to examine how lessons can be learned from those who adopt the practices earlier to inform the process of systems-level change for organizations that adopt the changes later on. 113
Conclusions
Significant barriers to OUD treatment exist in the US, especially for MOUD – the most effective OUD treatment. We identify future research recommendations to further understand and enhance effective OUD treatment delivery, including the need to address individual, organizational, and external factors that surround the implementation of recent regulatory changes.
Footnotes
Ethical Considerations
Ethics approval was not required in the crafting of this manuscript as no data were collected or analyzed.
Author Contributions
AB and RAM conceptualized the paper. AB and AWK wrote the original draft. RAM provided feedback/revision.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors are funded by the National Institute of Health under the National Institute on Drug Abuse (Bailey: 1F31DA061612; Martin: 3U01DA050442).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.