
Abstract
Background:
Numerous studies documented an unexpected association between physical activity (PA) and alcohol use, suggesting that higher rates of PA may be linked to increased alcohol use. Evidence is lacking on factors explaining this relation. This study investigated cross-sectional associations between time devoted to different domains of PA and unhealthy alcohol use and tested whether these associations differed by age and sex.
Methods:
Data were drawn from the 2017 Swiss Health Survey. Participants (N = 17 328) are representative of the Swiss population and provided information on 3 PA-domains (hours/day of sport/exercise, leisure, and commuting) and unhealthy alcohol use (chronic risky drinking [≥20 g mean daily ethanol for women; ≥40 g for men], heavy episodic drinking [≥1 occasion/month with ≥40 g for women/≥50 g for men]). Logistic regression models were used to estimate associations between hours/day spent on the 3 PA-domains and unhealthy alcohol use and to test interactions between PA-domains and sex and age separately. All models were adjusted for tobacco use, body mass index, and demographics.
Results:
Hours/day of leisure PA was positively associated with chronic risky drinking (OR = 1.06, P = .030). Hours/day of sport/exercise PA was positively associated with heavy episodic drinking (OR = 1.12, P = .007). No significant association was found for commuting PA. There was a significant interaction between sport/exercise PA and age on heavy episodic drinking (P < .001). Age-stratified analyses revealed positive associations for participants aged 18 to <25 (OR = 1.44, P < .001), 25 to <35 (OR = 1.23, P = .019), and ≥75 (OR = 1.74, P = .003), negative for participants aged 35 to <45 (OR = 0.73, P = .019), and nonsignificant associations for participants aged 45 to <55 (OR = 0.96, P = .720), 55 to <65 (OR = 0.99, P = .909), and 65 to <75 (OR = 1.05, P = .713).
Conclusions:
Our results highlight the importance to account for PA-domains and alcohol use patterns when studying the PA-alcohol relationship. Associations between sport/exercise and heavy episodic drinking differed by age, possibly reflecting the socio-environmental context’s impact across the lifespan. Findings may have implications for alcohol screening and interventions among physically active people.
Highlight
Evidence is lacking regarding the factors explaining the association between physical activity and alcohol use.
Time spent on sports/exercise was positively associated with heavy episodic drinking.
The association between sports/exercise participation and heavy episodic drinking differed by age.
These findings may have implications for screening and interventions among physically active people with unhealthy alcohol use.
Introduction
The general health benefits of physical activity (PA), defined as any bodily movement requiring energy expenditure, are well-established. 1 PA is one of the best-known health-promoting behaviors, fostering normal growth and functioning and reducing mortality.1,2 Research has also shown that PA is linked with better mental health, with evidence supporting a reduced risk of depression and anxiety among physically active people and symptom alleviation among people with mental health problems.2,3 PA also appears protective against tobacco and illicit substance use during adolescence and young adulthood, when substance use initiation is most likely to happen.4,5
Despite these benefits on health, the scientific literature reports conflicting evidence regarding PA’s impact on alcohol use. Although PA programs have received a lot of attention recently as potential treatments for people with alcohol use disorders, 6 systematic reviews of epidemiological studies have documented a counterintuitive association between PA and alcohol use, implying that higher rates of PA may be linked to greater alcohol use.7-9 This association has been repeatedly reported in the general population, particularly among young adults. 9 For instance, a prospective cohort study of young males in Switzerland reported a positive dose-response relationship between PA at baseline and hazardous alcohol use 2 years later. 10 Nevertheless, some studies have suggested a curvilinear association between PA and alcohol use in which people who present hazardous drinking patterns or are abstinent do less PA than people who drink moderately.11,12 One recent study exploring intraindividual variations in drinking and PA in a limited sample of college students found negative associations (ie, more PA was associated with less drinking), 13 whereas a study among community-dwelling adults found positive associations. 14 These findings suggest a complex relationship between PA and alcohol use, one that cannot merely be explained by errors in retrospective self-reporting or procedures that aggregate behavior over time. 15
The factors explaining this complex relationship have not yet been studied extensively. 4 The relationship between PA and alcohol use may differ by age and sex as a result of the effects of life transition events on the socio-environmental contexts affecting drinking patterns 16 and PA participation. 17 Indeed, a general population survey in the United States found that vigorous PA was associated with more alcohol use among people under 50 but not among those older and that moderate PA in the past year was linked to more alcohol use among male participants. 18 According to that survey’s authors, their results may suggest that socio-environmental contexts facilitating both drinking and PA may be more prevalent among young populations and men. However, most studies to date have demonstrated limitations related to assessment of PA. PA is often reported in qualitative levels of overall PA (ie, low, moderate, and high) without differentiating the specific domains in which that PA takes place (during exercise, leisure activities, work, or housework)—they often focus on sport and exercise exclusively. Recent research indicates that PA’s impact on mental health is influenced by the domain in which it occurs,19,20 underscoring the importance of accounting for that domain when studying the PA-alcohol relationship. Exploring this association by domain of PA may inform us about the processes at play in the PA-alcohol use paradox. Another limitation in prior studies is related to measuring alcohol use. Several epidemiological studies of the PA-alcohol use relationship have reported total volumes of alcohol used over time. While this is indicative of total exposure to alcohol, it cannot assess relationships between PA and specific drinking patterns, notably heavy episodic drinking (ie, consumption of a significant amount of alcohol in 1 occasion). For instance, social motives related to participating in team sports have been proposed as possible contributors to heavy episodic drinking.4,21 Thus, studying relationships between PA and drinking patterns may provide additional information.
A better understanding of the relationships between specific domains of PA and alcohol use patterns will enable better targeting of individuals likely to benefit from PA, better tailoring of prevention interventions, and more individualized recommendations about health behaviors.
The present study aimed to investigate the cross-sectional associations between the time devoted to 3 different domains of PA (hours/day spent on sport and exercise, leisure, and commuting) and unhealthy alcohol use (chronic risky drinking and heavy episodic drinking). It also sought to test whether these associations differed by age and sex, in a large representative sample in Switzerland.
Methods
Sample
The present study used anonymized data from the Swiss Health Survey (SHS), a cross-sectional survey on health status, health service utilization, and health-related behavior. 22 Switzerland’s Federal Statistical Office conducts the SHS every 5 years in a representative sample of the population aged 15 and over. Participants were interviewed by telephone or face-to-face and invited to return a written questionnaire. The present study used data from 2017’s SHS, including participants who had undergone an oral interview, responded to the written questionnaires, were at least 18 years old, and had no missing data. We decided to limit our analyses to participants aged 18 or older, the age when all types of alcoholic beverages can be legally purchased in Switzerland (between 16 and 18, young people can legally purchase beer and wine but not spirits). The final sample consisted of 17 328 of the 18 832 respondents to 2017’s SHS after excluding individuals under the age of 18 (N = 724) and individuals with missing values (N = 780).
No ethics committee approval is required to analyze anonymized data in Switzerland. Access to SHS data is only granted by the Survey’s steering committee after the submission of a research project protocol. Our protocol was submitted on July 6, 2022, and data were obtained on August 22, 2022.
Measures
Physical Activity
Sport and Exercise
Participants were asked to report the mean amount of time (in hours and minutes) they devoted to sport and exercise each week (“How much time do you usually devote to gymnastics, fitness, or sports each week?”). This was subsequently transformed into mean hours of sport and exercise per day.
Leisure
Participants were asked to report the amount of time they devoted to less intensive forms of movement during leisure activities. This was defined as “physical activities during which you are at least a little out of breath but which do not necessarily make you sweat. For example, brisk walking, excursions on foot, dancing, gardening.” The survey questions were as follows: “How many days a week do you do such physical activities? What is the mean duration of these physical activities on these days?” Responses were used to derive a mean number of hours of leisure per day.
Commuting
Participants who indicated bicycling or walking as a means of transport were asked to report how much time (in hours and minutes) they devoted to these activities each day, and this was transformed into mean hours per day (“How much time do you usually spend walking and cycling each day in total?”).
Unhealthy Alcohol Use
Chronic Risky Drinking
Chronic risky drinking was measured using average grams of pure alcohol consumed per day. Participants were identified as presenting with chronic risky drinking if they consumed ≥20 g of pure alcohol per day for women and ≥40 g for men. These sex-specific cutoffs were defined according to the World Health Organization drinking risk levels. 23 A dichotomous categorical variable was created according to these cutoffs: no use and low risk versus chronic risky drinking.
Heavy Episodic Drinking
Heavy episodic drinking was defined as the consumption of ≥40 g of pure alcohol on a single occasion for women and ≥50 g for men. 24 A dichotomous categorical variable was created according to the frequency of these occasions: no use and heavy episodic drinking <once/month versus heavy episodic drinking ≥once/month.
Moderators
Participants’ ages were coded into 7 groups: 18 to <25; 25 to <35; 35 to <45; 45 to <55; 55 to <65; 65 to <75; ≥75. 25 Sex was coded as female or male.
Control Variables
We used the following covariates as potential confounders in the associations between PA and alcohol use: body mass index (BMI) (“underweight (BMI <18.5) or normal (18.5 ≤ BMI < 25),” “overweight (25 ≤ BMI < 30),” “obese (BMI ≥30)”); tobacco use (“yes,” “no”); language (“German [including Rhaeto-Romansh],” “French,” “Italian”); education (“lower secondary school,” “vocational upper secondary school,” “general upper secondary school,” “tertiary”); marital status (“married,” “not married”); and type of community (“rural,” “urban,” “intermediate”).
We adjusted for variables that (i) were related to PA and to the alcohol use outcomes and (ii) were available in our dataset. More precisely, BMI has been found to be associated with low PA, suggesting that increased PA may reduce the likelihood of obesity, 26 while being overweight or obese significantly increases the odds of any alcohol use disorder. 27 Monthly changes in smoking prevalence have been positively linked to the prevalence of high-risk drinking. 28 Previous research has shown a connection between the type and intensity of sports and tobacco/nicotine use, with people practicing high intensity sports being less likely to smoke cigarettes. 29 Education also plays a role in these behaviors, as higher educational attainment is related positively to PA 30 and reduced risk of alcohol dependence. 31 Furthermore, while marriage does not seem to promote PA engagement, 32 it appears to be protective against the development of an alcohol use disorder. 33 With respect to the type of community, most studies have shown that rural residents are more likely to engage in hazardous alcohol use or alcohol-related harm compared with their urban counterparts. 34 As for PA, living in a rural area has been linked to similar levels of total PA, but lower levels of leisure-time PA than urban residents. 35 Regarding language, differences in culture and substance use prevalence exist between the linguistic regions of Switzerland. 24 Given this regional variation, we included language in our analyses to control for potential confounding effects related to cultural differences and substance use patterns across these regions.
Statistical Analysis
All analyses were conducted using the IBM SPSS Statistics software, version 27. Survey weights were applied to all analyses in order to adjust the results to accurately represent Switzerland’s population and to correct for some of the nonresponses. Descriptive statistics were used to describe sample characteristics and are presented as number and unweighted percentages, as well as weighted percentages and their 95% confidence interval (95% CI).
Associations between the time spent on the 3 different domains of PA (sport and exercise, leisure, and commuting) were estimated using separate logistic regression models for chronic risky drinking and heavy episodic drinking. Model 1 estimated the bivariate associations between each distinct domain of PA and each drinking pattern. Model 2 estimated the associations between each distinct domain of PA and each drinking pattern, adjusted for the other 2 domains. Model 3 estimated the associations between each distinct domain of PA and each drinking pattern, adjusted for the other 2 domains, covariates and sex, age. The significance level was set at P < .05. To test whether the associations between time spent on the 3 different domains of PA and each drinking pattern were moderated by sex and age, interactions were tested separately by sex and age in Model 3. When interactions were significant, the sample was stratified by the tested moderators, and the associations between the respective domains of PA and the respective outcomes were tested for each level of the moderator.
Before running any analyses, we evaluated for multicollinearity using the variance inflation factor (VIF) for each covariate and interaction. No evidence of multicollinearity was found since the highest VIF value (all VIFs <2.954) was inferior to values (VIF = 4 or VIF = 10) indicative of possible multicollinearity issues. 36
Results
Participants Characteristics
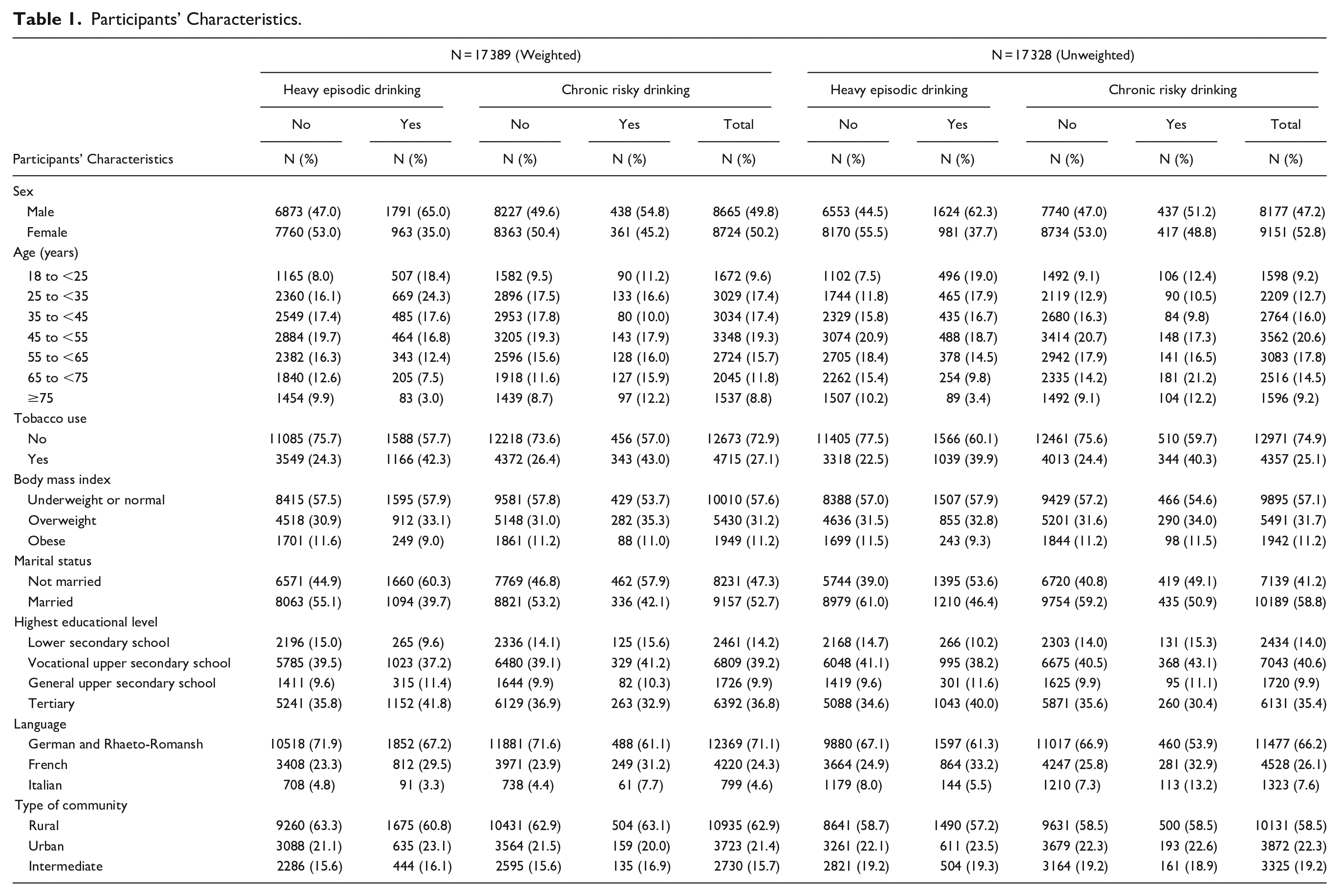
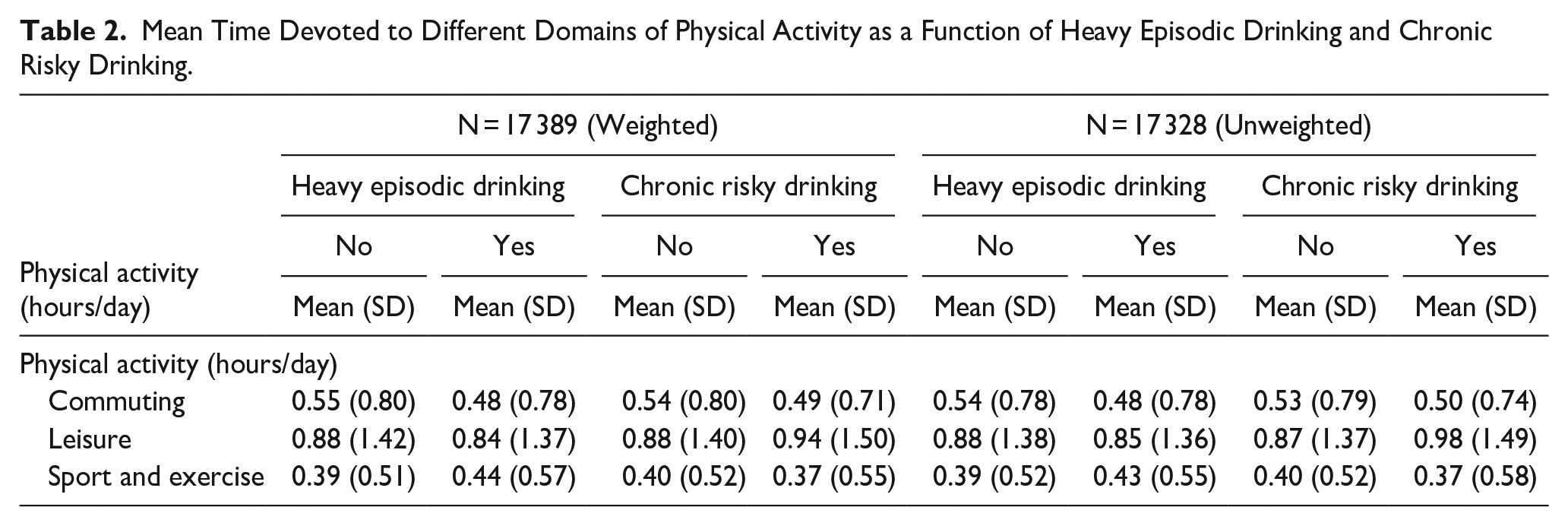
Table 1 describes the participants’ characteristics. Among the 17 328 participants, 2605 (15.0%) reported at least 1 monthly episode of heavy episodic drinking, and 854 (4.9%) reported chronic risky drinking. Table 2 describes the mean hours/day devoted to different domains of PA as a function of heavy episodic drinking and chronic risky drinking.
Participants’ Characteristics.
Mean Time Devoted to Different Domains of Physical Activity as a Function of Heavy Episodic Drinking and Chronic Risky Drinking.
Associations Between PA and Chronic Risky Drinking
The bivariate model (Model 1) found no statistically significant associations with any of the 3 domains of PA individually, and neither did Model 2, adjusted for the other 2 domains of PA. Only time devoted to the PA of leisure was positively associated with chronic risky drinking in fully adjusted Model 3 (OR = 1.06, 95% CI = 1.01-1.11). Table 3 shows the results of the 3 different regression models. The detailed statistical analysis results are provided in Table A1 in the Supplemental Appendix.
Results of Logistic Regression Models Investigating the Associations Between Different Domains of Physical Activity and the 2 Drinking Outcomes.
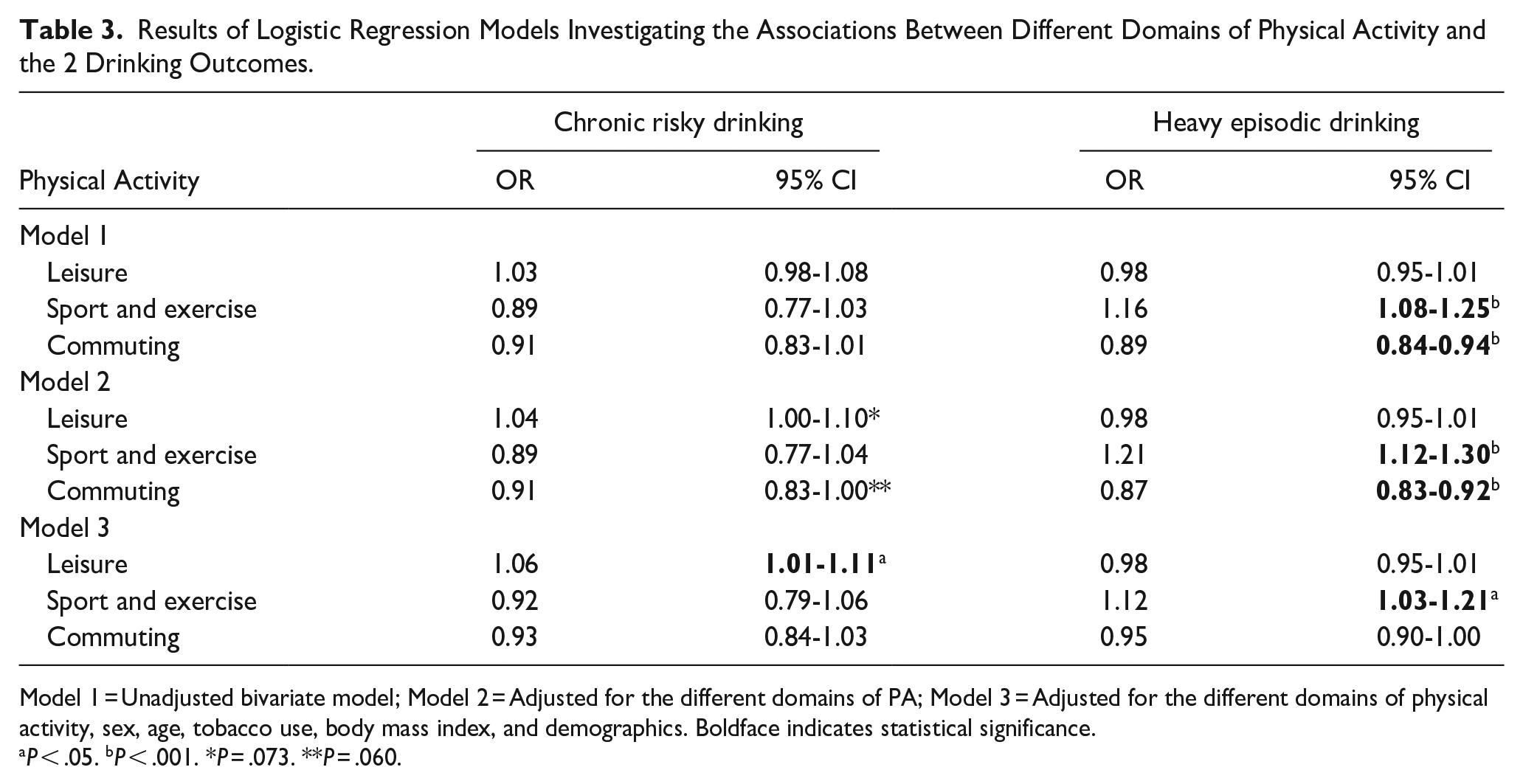
Model 1 = Unadjusted bivariate model; Model 2 = Adjusted for the different domains of PA; Model 3 = Adjusted for the different domains of physical activity, sex, age, tobacco use, body mass index, and demographics. Boldface indicates statistical significance.
P < .05. bP < .001. *P = .073. **P = .060.
PA and Heavy Episodic Drinking
Of the 3 domains of PA, time devoted to sport and exercise and to commuting were significantly associated with heavy episodic drinking in bivariate Model 1: positively for sport and exercise (OR = 1.16, 95% CI = 1.08-1.25) but negatively for commuting (OR = 0.89, 95% CI = 0.84-0.94). These associations persisted when adjusted for other domains of PA using Model 2 (OR = 1.21, 95% CI = 1.12-1.30 for sport and exercise; OR = 0.87, 95% CI = 0.83-0.92 for commuting). However, only the association between time devoted to sport and exercise and heavy episodic drinking remained significant in fully adjusted Model 3 (OR = 1.12, 95% CI = 1.03-1.21). The PA of leisure was not significantly associated with heavy episodic drinking in any of the models. Table 3 shows the results of the 3 different regression models. The detailed statistical analysis results are provided in Table A1 in the Supplemental Appendix.
Interactions Between Domains of PA and Sex and Between Domains of PA and Age
Table 4 shows the results of the logistic regression models testing the interactions between time devoted to each domain of PA and age groups, and between the 3 PA-domains and sex. There were no significant interactions with sex. For the age groups, the only significant interaction was between the time devoted to sport and exercise and the outcome of heavy episodic drinking (Wald = 23.8, df = 6, P < .001). The sample was thus stratified by age groups to further evaluate the relationships between time devoted to sport and exercise and heavy episodic drinking. As Figure 1 illustrates, age-stratified, fully adjusted analyses revealed positive associations for participants aged 18 to <25 (OR = 1.44, 95% CI = 1.20-1.73), 25 to <35 (OR = 1.23, 95% CI = 1.03-1.46), and ≥75 (OR = 1.74, 95% CI = 1.20-2.25), negative associations for participants aged 35 to <45 (OR = 0.73, 95% CI = 0.56-0.95), and nonsignificant associations for participants aged 45 to <55 (OR = 0.95, 95% CI = 0.76-1.20), 55 to <65 (OR = 0.99, 95% CI = 0.77-1.26), and 65 to <75 (OR = 1.05, 95% CI = 0.82-1.33). The detailed statistical analysis results are provided in Table A2 in the Supplemental Appendix.
Results of the Regressions Models Testing the Interactions Between Time Devoted to Each Domain of Physical Activity, Age Groups, and Sex as Predictors, and the 2 Drinking Outcomes.
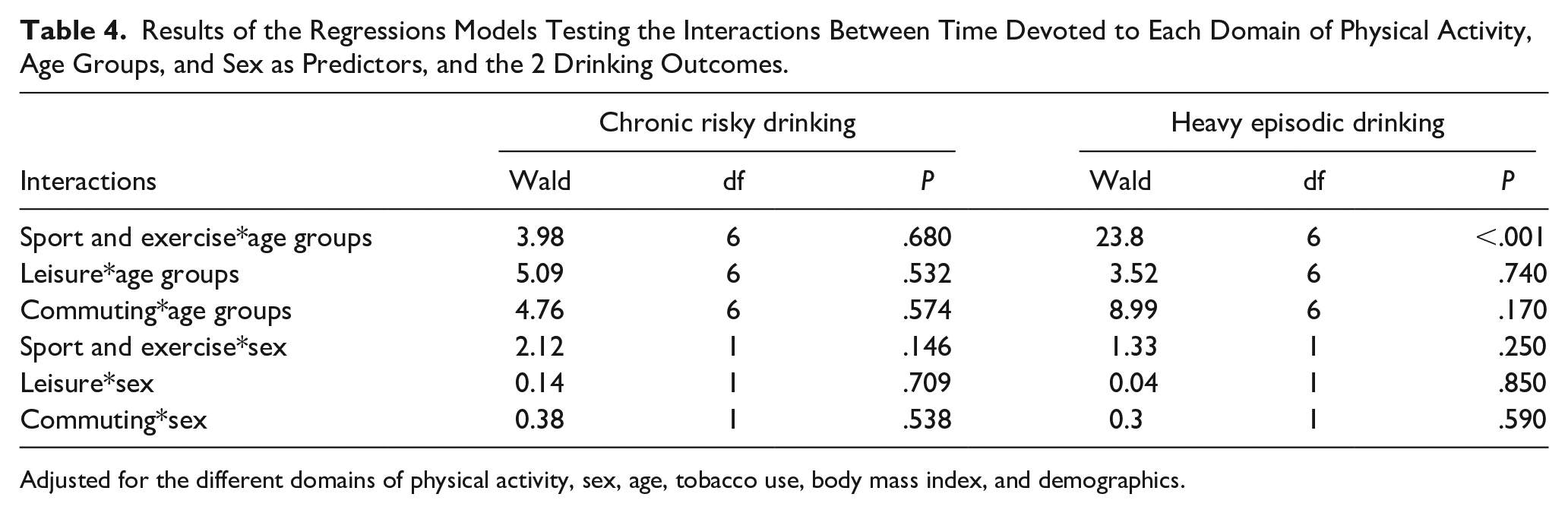
Adjusted for the different domains of physical activity, sex, age, tobacco use, body mass index, and demographics.

Associations between time devoted to sport and exercise and heavy episodic drinking by age groups.
Of note, we also replicated the same analyses among participants reporting alcohol consumption (N = 14 798), excluding abstainers (N = 2530), and the results were largely consistent. The complete statistical analysis results are presented in Tables A3 to A5 in the Supplemental Appendix.
Discussion
The present study sought to expand the literature on the relationship between PA and alcohol use by examining associations between 3 distinct domains of PA (sport and exercise, leisure, and commuting) and 2 distinct unhealthy alcohol use outcomes (heavy episodic drinking and chronic risky drinking). To the best of our knowledge, no previous study had examined this relationship from this perspective. We also tested whether these associations differed according to age and sex.
We observed notable differences in how each domain of PA was associated with the 2 defined drinking outcomes, suggesting that the contexts in which PA takes place may contribute differently to its association with drinking. More precisely, for chronic risky drinking, we only found a positive association with the PA of leisure, which in our sample corresponds to mild forms of PA, not including sport and exercise. This was in line with a previous study reporting that light-to-moderate PA was associated with more alcohol use. 18 One possibility is that both behaviors appeal as ways to unwind—alcohol can act as a reward after physical effort, 37 and both behaviors can co-occur in given social contexts (eg, nightclubbing and dancing, golf participation 38 ). Personality predisposition may also offer an explanation about the observed association. Indeed, a previous study in a limited sample of students found that positive urgency and sensation seeking, both dimensions of impulsivity, moderated the positive association between moderate PA and number of drinks per week. 39 According to the authors of this study, this may be due to the fact that both activities can provide an opportunity for immediate gratification among individuals scoring high on these personality dimensions.
Only the PA domain of sport and exercise appeared to be significantly associated with a greater frequency of heavy episodic drinking (once per month or more) in our sample. We only found significant interactions between age and sport and exercise for the outcome of heavy episodic drinking. Interestingly, the direction of the association varied across the population’s lifespan, with a detrimental (ie, more PA, more heavy drinking) significant association between PA and heavy episodic drinking among younger adults between 18 and <35 and older ones aged ≥75, and a favorable (ie, more PA, less heavy drinking) significant association for those aged between 35 and <45 years old, and a nonsignificant negative association for those aged between 45 and <75. We found no statistically significant interactions between sex and PA in our sample. These results differed from those of a previous epidemiological study showing that age and sex moderated the association between PA and alcohol use and that PA was associated with alcohol use among individuals below 50 but not those over 50. 18 This inconsistency may be attributable to different study designs, namely, age aggregation, the definition of specific domains of PA, and different alcohol use outcomes, rather than the intensity of PA and levels of alcohol consumption. Regarding associations between heavy episodic drinking and sport and exercise among people aged 18 to <35, our results are consistent with previous research reporting links between increased heavy episodic drinking and doing sports among younger adults.5,40 As suggested previously, 15 this association may reflect overlapping motives underlying both behaviors (ie, drinking or exercising following intrapersonal motivations, such as coping with negative affect or following sensation-seeking motives). Alternatively, it may reflect social, enhancement, and reward motives among young people (ie, drinking to socialize, promote cohesion, and enhance positive emotions within the context of participating in a team sport, or drinking as a reward after physical effort). 41 Furthermore, exercise may appeal as a way to compensate for calories ingested through alcohol.13,42 Our results indicated that the effect size of the observed positive associations between sport and exercise and heavy episodic drinking decreased between the age groups of 18 to <25 and 25 to <35 and then became negative for those aged 35 to <45, possibly coinciding with the process of “maturing out,” during which people tend to diminish their alcohol use as they transition from early adulthood to working life and adult responsibilities. 43 This life stage may overlap for some with what is commonly referred to as a “mid-life crisis,” a time when individuals recognize the need to take action in order to make the most of their remaining years. 44 During this challenging developmental period 45 PA may serve as a resource, helping promote emotional regulation.46,47 A recent study found that people high in negative urgency, a trait marked by the urge to act impulsively as a reaction to negative emotions, 48 linked to heavy episodic drinking severity, 49 decreased their alcohol use as they increased vigorous PA engagement. 50 This possibly suggests that vigorous PA can help reduce alcohol use among those using alcohol to cope with negative affect. However, the observed association in our sample could also reflect a cohort effect. To the best of our knowledge, no previous study has reported a link between sport and exercise and heavy episodic drinking among older adults aged ≥75. Indeed, there is very limited evidence on PA’s effects on alcohol use among older adults. 4 However, in line with our results, one recent study showed that daily alcohol use was associated with the increased likelihood of older adults being physically active compared with those who do not drink. 51 Recent cohort studies have found that physically active individuals tend to have a longer, disability-free life expectancy 52 and that there is an increase in PA among older adults suffering from fewer chronic conditions after retirement. 53 Regarding alcohol, heavy episodic drinking tends to decrease with age, although drinking occasions become more frequent in older age.16,54 Additionally, poor health has been linked to declines in both drinking and PA among older adults.55,56 Thus, our findings may reflect that in a specific subgroup of physically active people, who do not have to deal with physical health problems and can still invest in sport and exercise, drinking may be more frequent due to reward or social motives linked to participation. They may also reflect increased occasions for drinking among older adults who remain physically active and free of disability. It is noteworthy that the PA of commuting was not associated with neither of the 2 drinking outcomes, perhaps because it is usually a solitary, less rewarding activity and is thus less likely to be associated with alcohol use.
Our findings contribute to the existing literature by highlighting the impact of specific domains of PA on alcohol use patterns and by informing about the possible processes underlying the paradox of PA and alcohol use. This could have implications for the prevention of alcohol use problems. First, our findings suggest that the positive association between PA and alcohol use, also observed by previous epidemiological studies, may specifically concern the association between sport and exercise and heavy episodic drinking, particularly among people in specific age ranges, namely, younger and older adults. This knowledge could also enable more targeted prevention interventions. Although this association has been reported repeatedly among students, it has never been reported among older adults, to the best of our knowledge. Previous studies of the general population assessing qualitative levels of total PA and levels of alcohol consumption may thus have failed to capture these specific effects. Therefore, our results suggest that certain ages that are characterized by fewer responsibilities and more leisure time, namely, early and late adulthood, may facilitate both drinking and sport and exercise. Based on our findings and the existing published evidence, it appears that the relationship between PA and alcohol use is complex. These results suggest that PA will not necessarily have a beneficial effect on alcohol use and that recommendations should take into account the context, the type of activity, and individual factors. Future research should focus on identifying the specific types of PA and contexts that might be beneficial for different individuals.
The present study has some limitations. Its cross-sectional design means that no causal inferences should be drawn regarding the directions of the observed associations; these could reflect an underlying factor impacting both PA and drinking. Also, the age group differences observed may be due to cultural and historical differences rather than developmental trajectories. While we used education and marital status as proxy of socioeconomic status, there was no measure of income included in the analyses. Thus, residual confounding from socioeconomic status might be present. All the data relied on self-reported information, which is subject to recall bias, and alcohol use could be underreported or the time devoted to PA overestimated for social desirability reasons. Nonetheless, a recent study reporting a positive association between cardiorespiratory fitness and alcohol use (ie, higher fitness levels were associated with greater alcohol use) found a similar pattern when examining the association between self-reported PA (instead of measured cardiorespiratory fitness) and alcohol use. 57 Lastly, our questions did not enable us to identify the precise nature of participants’ PA (eg, team or individual sports), and this might have helped to generate more precise hypotheses regarding the processes underlying the association between PA and alcohol use. Future studies could look at different types of sports and their associations with alcohol use.
This study also has some notable strengths, including its large, representative population sample and its questions assessing alcohol use patterns and times spent on specific domains of PA.
Conclusion
The present work’s results highlighted the importance of examining different alcohol use patterns and domains of PA when studying the relationship between PA and alcohol consumption. Furthermore, the association between sport and exercise and heavy episodic drinking differed by age, possibly reflecting the impacts of different socio-environmental contexts across a lifespan. These findings may have implications for alcohol screening and prevention interventions among physically active people. Further research should focus on the prospective associations between different domains of PA and subsequent drinking patterns across lifespans to further evaluate PA’s impact on drinking behaviors.
Supplemental Material
sj-docx-1-saj-10.1177_29767342251323782 – Supplemental material for Unraveling the Relationship Between Physical Activity and Unhealthy Alcohol Use in the General Population: A Cross-Sectional Study
Supplemental material, sj-docx-1-saj-10.1177_29767342251323782 for Unraveling the Relationship Between Physical Activity and Unhealthy Alcohol Use in the General Population: A Cross-Sectional Study by Marianthi Lousiana Deligianni, Joseph Studer and Nicolas Bertholet in Substance Use & Addiction Journal
Footnotes
Acknowledgements
The authors thank the participants of the Swiss Health Survey.
Author Contributions
MLD, JS, and NB involved in conceptualization, design of the analyses, and data interpretation. MLD analyzed the data and drafted the initial manuscript. All authors contributed to this article, revised the manuscript, and approved the submitted version.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: MLD received a scholarship (“scholarships for clinicians-researchers”) from the Department of Psychiatry at the Lausanne University Hospital, who made possible the realization of this study.
Compliance,Ethical Standards,and Ethical Approval
Institutional review board approval was not required.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.