
Abstract
Background:
Alcohol and other substance use disorders and major depression often co-occur. A sedentary lifestyle is related to major depression and even moderate exercise may prevent and contribute to the treatment of depression. Studies have found an effect of physical activity on depression in alcohol and other substance use disorder patients even in clinical settings.
Aim:
To investigate the relationship between level of physical activity and depressive symptoms over time in alcohol and substance use disorder inpatients.
Methods:
Eighty-nine substance use disorder inpatients were followed for 6 months during treatment. The International Physical Activity Questionnaire was used to categorize 3 groups of low, moderate, or high level of physical activity. In addition to background variables and alcohol and drug use measures, data on biometric measures and on sleep were gathered. Becks Depression Inventory version II (BDI-II) measured depressive symptoms. A multilevel logistic regression was used to analyze the longitudinal relationship between physical activity and depressive symptoms.
Results:
Most patients (57%) reported low activity, while 24% reported moderate and 19% high activity. Few changed their activity level during treatment. Moderate physical activity was related to lower score on BDI-II (P = .029). Level of physical activity was closely related to insomnia (P = .024). In the multivariate analysis the relationship between depressive symptoms and physical activity did not withstand the adjustment for insomnia. However, in the multilevel logistic regression higher physical activity was related to lower BDI-II score in a dose dependent manner.
Conclusions:
Among these alcohol and other substance use disorders patients in treatment, there was a relationship between depressive symptoms and physical activity. The low level of physical activity identified among these patients was related to a high level of depressive symptoms. The level of depressive symptoms declined over time; but this change was not related to an increase in physical activity.
Keywords
Introduction
Substance use disorders (SUD) is one of the largest public health issues in the world. More than 42 million disability-adjusted life years (DALY) were lost to drug use in 2017. 1 Global prevalence rates of alcohol use disorders (AUD) were in 2010 estimated to range from 10% to 16%. 2 Alcohol and AUD is the leading risk factor for premature mortality and disability among those aged 15 to 49 years. 3
Major depression (MD) is also one of the world’s leading causes of morbidity. 4 The estimates for lifetime prevalence of MD varies between 8% and 12%. 5 There is a strong link between most substance use disorders and mood and anxiety disorders.6-8 Estimates of the prevalence of affective disorders among substance-using patients have been estimated to be as high as 60%. 9
Comorbid major depressive disorder reduces the risk of successful remission from SUD and predicts relapse. 10 This means that SUD rehabilitation treatment should not only focus on the addiction, but also treat comorbid mood or anxiety disorder. 6 Comorbid depressive disorders are also associated with greater disability and heavier use among those seeking treatment for AUD.11,12
A growing body of evidence suggests that exercise and physical training may have multiple beneficial effects in individuals with either MD or SUD. 11 Exercise is associated with positive mood by increasing feelings of vigor and reducing tension, fatigue, and confusion. 13 Cross-sectional studies have identified reciprocal affiliation between physical activity and depressive symptoms. 14 On the other hand, prospective observational studies have demonstrated the preventive effects of physical activity and fitness on the frequency of depressive disorders. 8 Randomized controlled trials have demonstrated that exercise is more effective than either placebo or attentional control groups and produces effects equivalent to other depression treatments. 11
Studies demonstrate that higher physical activity is related to reductions in symptoms of depression. 15 A systematic review and meta-analysis of 21 randomized controlled trials (RCTs) with 1204 AUD patients showed that exercise reduced depressive symptoms. 16 Including physical exercise in the treatment of addictions might both be an effective tool to help in the prevention and treatment of drug dependencies at different levels8,17 and to reduce depressive symptoms.
The aim of the present study was to assess if physical activity among patients in treatment for SUD and mostly AUD was related to the level of depressive symptoms.
Materials and Methods
Study participants
Data were collected in 3 different rehabilitation clinics in the Eastern region of Norway from January 2018 to August 2019. The clinics offer long-term residential treatment stays (>30 days). The patient population comprised adults above the age of 18 years currently receiving in-patient treatment for their AUD and/or other SUDs, where the majority have a diagnosis of AUD. Patients who were unfamiliar with Scandinavian language and who were suffering from a severe somatic illness, psychosis, or cognitive impairment that could limit their ability to provide informed consent or safely participate in the study were not included in the study. The sample consisted of 68 (76%) males and 21 (24%) females, and the median age was 54 (Interquartile range [IQR] 43-58) years.
The patients were followed up at baseline, at 6 weeks and at 6 months. Patients received inpatient treatment during this time, consisting of treatment for the addiction disorder, their mental health and somatic health problems. The treatment was individual and consisted of group and/or individual psychotherapy sessions, medicinal drug treatment, and help with social challenges such as housing and economy. Some patients ended their treatment after 3 months and some dropped out of treatment. Patients who discontinued the treatment program or left the clinics before planned discharge before 6 weeks were regarded as dropped out. Because several patients had only planned 3 months treatment, drop-out after 6 weeks was not recorded.
The study was conducted in line with the declaration of Helsinki. Written informed consent was obtained from the patients before enrollment into the study. The Norwegian Regional Ethics Committee provided ethical approval to conduct the study (reference number 2017/1314).
Measures
Baseline data collection consisted of an interview, administration of psychometric questionnaires, a clinical examination, and blood samples. Information about age, sex, level of education, and smoking status was obtained during the interview. Selected modules of the Mini International Neuropsychiatric Interview (M.I.N.I.) version 6.0 were conducted by trained staff, while all other information was collected using self-report forms. The interview and self-report forms were administered at the clinics where the patients were staying.
Physiology and blood samples
Weight and height were recoded to calculate body mass index (BMI; kg/m2) and waist circumference was recorded. Venous blood was drawn from the median cubital vein into serum tubes and ethylene-diamine-tetra-acetic tubes for the analyses of gamma-glutamyl transferase (γ-GT), phosphatidylethanol (PEth; 16:0/18:1), and total cholesterol. The tubes were turned slowly upside down 8 to 10 times, left in a stand for 30 minutes, and centrifuged before transferred to the laboratory for analysis.
Measure of physical activity
Physical activity was measured using the International Physical Activity Questionnaire-Short Form (IPAQ-SF). 18 The IPAQ-SF consists of 7 questions covering activities during work or leisure time, domestic activities and transport, and responses are given in terms of hours and minutes spend doing vigorous or moderate activity or walking. This information is calculated into Metabolic Equivalent of Task per week (MET-minutes/week) and based on set criteria these scores are categorized into “Low,” “Moderate” or “High” levels of activity. 19
Psychopathological measures
Beck et al 20 Depression Inventory version 2 (BDI-II), a 21 item self-report inventory, was used to identify the severity of depression during the past 2 weeks. The Norwegian validated version of BDI-II was used in the study for which a Cronbach’s alpha ranging from .84 to .92 has been reported. 21 Each question of the inventory consists of 4 statements which requires a self-evaluation, and the responses are scored from 0 to 3 (a 4-point Likert Scale). The total score is the sum of individual responses and ranges from 0 to 63. Higher score indicates higher level of depressive symptoms. In the present study, the Cronbach’s alpha for BDI-II was .92.
Sleep condition indicator (SCI)
Subjective sleep quality was measured with the Sleep Condition Indicator (SCI). 22 The SCI has been developed to screen for insomnia and consists of 8 questions including issues such as sleep onset delay, night-time awakenings, extent of the problem and effect on daytime activities, mood and relations. All items have response alternatives ranging from 0 to 4, where 0 indicates a poor state and 4 indicates no/little problems, resulting in a total sum score ranging from 0 to 32. A score of ⩽16 indicates probable insomnia. 22 The SCI has been utilized in a previous publication by our group. 23
Aud- and SUD-related measures
The M.I.N.I. interview was used to diagnose AUD and SUD. The severity of AUD was identified using the Severity of Dependence Scale (SDS) which measures impaired control over alcohol intake, preoccupation, and anxieties regarding drinking over the last year. 24 SDS consists of 5 items that target subjective aspects of dependence during the preceding year. The response alternatives range from (0) “never” to (3) “always” for each question. The responses are summed up into a total score ranging from 0 to 15, where higher score indicates more severe dependence. The Norwegian version of SDS were used, for which Cronbach’s alpha ranging from .72 to .80 across a variety of substances has been reported.25,26 The instrument consists of 5 items and each item is scored in a four-point Likert scale (0-3). The individual scores are summed up and higher score represents more severe AUD or other SUD. In this study, the internal consistency of SDS as measured by Cronbach’s alpha was .78.
Statistical analyses
A non-normal distribution was expected due to a low number of participants, thus medians and interquartile ranges (IQR; 25th and 75th percentile) is reported and non-parametric statistics were utilized. In the logistic regression odds ratio (OR) along with 95% confidence intervals were reported. Statistical tests were 2-tailed with a significance level of α = .05. Chi-square tests were used to compare categorical variables, while Mann-Whitney U tests were used to compare continuous variables. Exact P-values were given, but P-values below .050 were considered significant.
For some variables, the cases with missing data were excluded. For some data points, imputations of missing values were done: For BDI-II mean values from the answered questions were imputed if 17 or more of the 21 questions were answered (N = 67). For SCI mean values from the answered questions were imputed if 6 or more of the 8 questions were answered (N = 83).
Linear regression models were constructed for adjustment of relevant covariates. Variables that were significant in the bivariate analyses were added for adjustment in a stepwise manner: Age and sex (Step 1); SDS (Step 2); Insomnia (Step 3). To investigate longitudinal effects linear multilevel models were constructed and stepwise adjustment was applied. The fixed effects of physical activity and time were estimated, and subject id was set as random intercept. A model containing time as random slope was considered but model fit was not improved compared to the model without random slope as measured by a likelihood ratio test (P = .911). Restricted maximum likelihood (REML) was used in all multilevel models, and missing data point were defined as missing completely at random (MCAR).
Results
Table 1 shows characteristics of patients with low (N = 51; 57%), moderate (N = 21; 24%), or high (N = 17; 19%) physical activity levels. Only few patients changed their activity group during the first 6 weeks of treatment, with 43 of 58 with observations at all time points (74%) not changing group, while 8 and 7 respectively decreased or increased their activity (Supplemental Table S1). The groups were similar on sociodemographic variables. The group with low activity level had higher γ-GT level (P = .014). Insomnia was more prevalent in the low activity group than the moderate activity level group (P = .015). Patients with moderate activity level had fewer depressive symptoms than those with low activity level (P = .029). Characteristics among the patients stratified by mild (N = 49; 55%), moderate (N = 22; 25%), or severe (N = 18; 20%) level of depressive symptoms are shown in Table 2. The percentage of women was higher in the severe than in the mild symptom level group (P = .017). There were more smokers among patients with moderate than mild depressive symptom level (P = .040). Patients with moderate or severe symptom level scored higher on severity of dependence (P = .014).
Characteristics of patient sample categorized by IPAQ-S categories at baseline (N = 89).

Abbreviations: γ-GT, gammaglutamyltransferase; BDI-II, Beck depression Inventory version 2; BMI, body mass index; IPAQ-S, international physical activity questionnaire short version; PEth, phosphatidylethanol.
Descriptive statistics given as N and percentage for categorical variables and as medians and interquartile range (IQR) for continuous variables. Group differences were tested with Wilcoxon rank sum test for continuous variables and with Pearson’s χ2-test for categorical variables. Significant values (P < .05) are shown in bold.
χ2/Fisher’s exact test or Kruskal Wallis test.
χ2/Fisher’s exact test or Wilcoxon Rank Sum test.
Characteristics of patient sample categorized by BDI severity at baseline (N = 89).
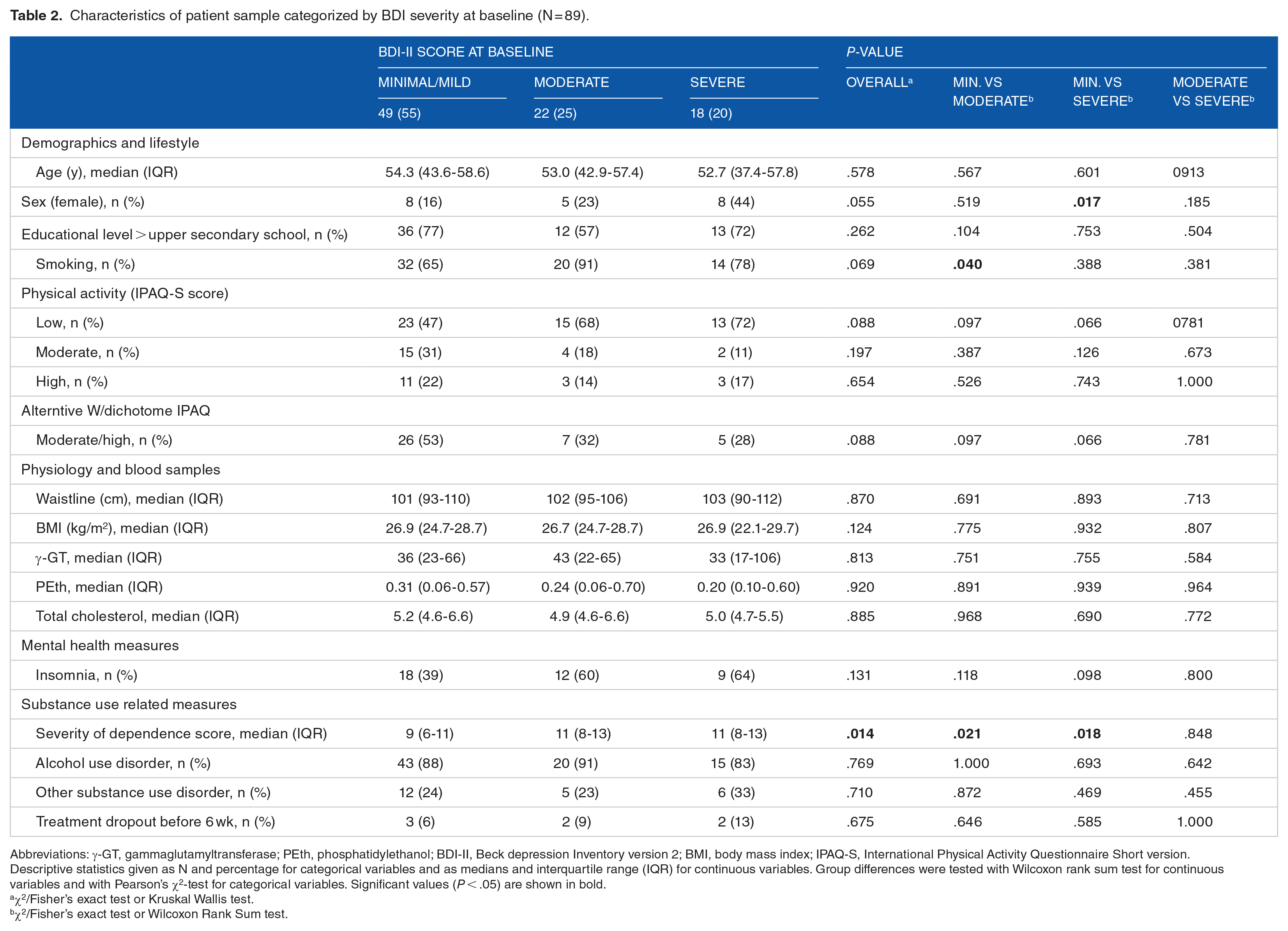
Abbreviations: γ-GT, gammaglutamyltransferase; PEth, phosphatidylethanol; BDI-II, Beck depression Inventory version 2; BMI, body mass index; IPAQ-S, International Physical Activity Questionnaire Short version.
Descriptive statistics given as N and percentage for categorical variables and as medians and interquartile range (IQR) for continuous variables. Group differences were tested with Wilcoxon rank sum test for continuous variables and with Pearson’s χ2-test for categorical variables. Significant values (P < .05) are shown in bold.
χ2/Fisher’s exact test or Kruskal Wallis test.
χ2/Fisher’s exact test or Wilcoxon Rank Sum test.
The linear regression of cross-sectional baseline observations showed statistically significant associations between depressive symptom level, and sex, moderate physical activity level, severity of dependence (SDS) and insomnia when unadjusted for covariates (Table 3). Moderate physical activity was associated with levels of depressive symptoms when adjusted for the effects of sex and age (models 1 and 2), and even adjusting for SDS (model 3), but not when adjusting for the effect of insomnia (model 4).
Linear regression with BDI-II score (continuous) as outcome variable and with baseline exposure variables.

Abbreviations: CI, confidence interval; IPAQ-S, international physical activity questionnaire short version; LL, lower limit; UL, upper limit.
Significant values (P < .05) are shown in bold.
Per 1-year increase of age.
Per 1-point increase of Severity of dependence scale (SDS).
Figure 1 shows the average BDI score at 3 times for the different IPAQ-S groups. There all observations (with varying N) are shown, with only a few differences between groups (mostly a higher score for low activity at baseline and 6 weeks). However, a multilevel linear regression including longitudinal data, confirmed the main effects found in the cross-sectional analysis from baseline: indicating more depressive symptoms in females, among those with higher SDS and insomnia. In addition to a statistically significant association between moderate physical activity and depressive symptoms this analysis also found that high physical activity level patients had fewer depressive symptoms (Table 4). The main effect of time was statistically significant, but there were no interactions between time and the outcome or the covariates.
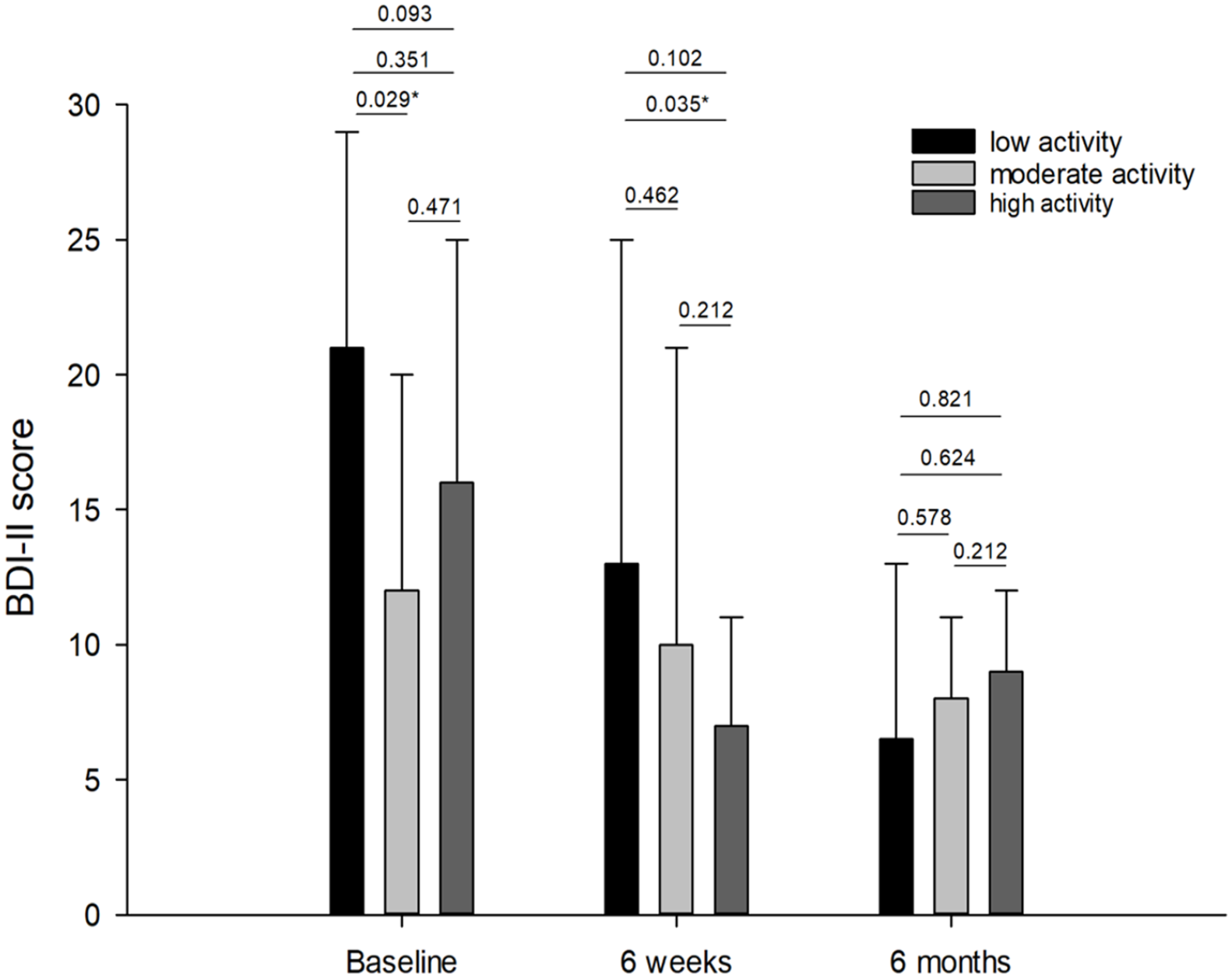
The average score on Beck Depression Inventory ver. II (BDI-II) for the included AUD and SUD patients at baseline, after 6 weeks and after 6 months for the 3 different groups stratified by score on IPAQ-S. The figure includes all observations, regardless of if the scores were noted at all time points, thus no comparisons between the time points were made. The figures represent the overall χ2 score, followed by the post hoc P-values comparing low versus high, low versus moderate and moderate versus high IPAQ-S scores.
Multilevel linear regression for predictors of BDI-II over a 6-month period.

Abbreviations: CI, confidence interval; IPAQ-S, international physical activity questionnaire short version; LL, lower limit; UL, upper limit.
Significant values (P < .05) are shown in bold.
Per 1-year increase of age.
Per 1-point increase of Severity of dependence scale (SDS).
Discussion
The current study shows that most of the AUD and other SUD patients had a low level of physical activity at treatment entry and that very few changed their activity during the treatment. A low activity level was related to larger waist circumference, higher γ-GT, and insomnia. Depressive symptom level was higher in females and in those with higher severity of dependence and insomnia. Most importantly, those with a moderate physical activity level reported fewer depressive symptoms, even after adjusting for sex, age, and severity of dependence, but not when adjusting for the effect of insomnia. These findings were confirmed in multilevel linear regression including longitudinal data. A reduction in depressive symptoms was seen in all activity groups but this reduction was not related to or dependent on level of physical activity.
In the general population there is a positive relationship between physical activity and alcohol intake, even when including heavy drinkers. 27 Others have suggested an inverted J-shaped relationship between alcohol consumption and physical activity, with less physical activity both among abstainers and heavy drinkers. 28
There is a relative scarcity of studies on physical activity and fitness in people with AUD. 29 Still, there is an understanding that patients with alcohol and drug problems often lead unhealthy lives with smoking and low physical inactivity and have weight problems. 30 Compared to healthy controls AUD inpatients are less physically active, and lower level of physical activity is related to longer illness duration. 29 In one study, as many as half of AUD patients entering treatment programs were classified as sedentary, while 1 in 6 were moderately active, and 1 in 3 were characterized as very active. 31 In that study only a slight increase in activity was found over the treatment period. 29 These findings are much in line with our study showing a low level of physical activity and only small changes in activity level during the treatment stay. As in other studies we observe a close relationship between physical activity and waist circumference. 32
In the general population there is a growing body of evidence showing that physical activity is associated with reduced risk for depression. However, the causality and direction of this association is not clear; physical activity may reduce depressive symptoms, or/and depressive symptoms may cause more functional impairments and thus reduce physical activity. 33 There also seems to be a dose-response relationship between physical activity and depression. 15 A meta-analysis has suggested an inverse curvilinear association between physical activity and risk of depression, with the greatest reduction in risk coming from changing from a sedentary lifestyle to moderate physical activity, 34 not unlike some of the results in the present study.
Most of the studies on the relationship between physical activity and depression have been performed in nonclinical populations. 35 Some other research, however, suggests that depression levels even in patients with SUD/AUD is associated with level of physical activity, 16 indicating the association is similar in AUD/SUD patients. This is also confirmed by the findings from the current study. Furthermore, our results indicate a dose-response relationship for the association between physical activity and depression. Patients with moderate physical activity, reported fewer depressive symptoms. Similar results are found in other studies, were insufficient physical activity, measured by IPAQ, was found to be associated with more depression. 36
In the present study, the association between physical activity and depression was, as mentioned above, found even after adjustment for sex, age, severity of dependence, but not when adjusting for the effect of insomnia. Disturbances of sleep continuity often accompanies affective disorders. 36 Present day research takes the view on insomnia as a transdiagnostic symptom for many mental disorders, being most closely related to depression. 37 From earlier studies we know that an increase in physical activity can significantly reduce both depressive symptoms and insomnia symptoms. 38 We also know that the sleep-depression relationship needs to be conceptualized as bidirectional. Both conditions have been shown to be triggered by psychosocial stressors. 36 The apparent relationship between physical activity and depression did not withstand adjustment for insomnia. This could be due to insomnia being an integral part of depression 39 or that the relationship between physical activity and depression is mediated through insomnia. 40 We know from earlier research that treating insomnia early has the potential to prevent or reduce depressive symptoms. 41 It may be argued that adjusting for insomnia is an over adjustment but chose to present the results as is.
We saw a reduction of the depressive symptoms for all, regardless of activity groups. The patients received individually tailored treatment for their mental, somatic, and social problems, including treatment for major depression. All this may have contributed to a general improvement in depressive symptoms. However, the study found no interaction between physical activity and depressive symptoms over time. The results from the current study may thus not be used as an argument for physical activity to treat of depression in AUD/SUD patients. On the other hand, we have no indication that physical activity is not helping depressive symptoms. Thus, the current results cannot be used to argue for or against the impact of physical activity on depression in patients with AUD/SUD. One reason for this shortcoming of the paper is that so few patients changed their activity level during the treatment period, making it difficult to identify any potential effect.
Still, the relationship between physical activity and depressive symptoms found in the present study should have clinical implications. The frequency of depressive disorder in patients with AUD is very high and increasing physical activity could be a low-threshold and effective intervention in the rehabilitation of these patients. As the relationship between depressive symptoms and AUD most likely is bidirectional, 42 increasing physical activity can also be viewed as both a preventive measure and a potential treatment.
Strengths and limitations
The study included male and female patients at different activity levels, but the sample size was limited. The study included a rather broad investigation of potential confounders for the relationship between physical activity and depressive symptoms, making it possible to single out this relationship. However, the observational nature of the study may have missed some potential confounders, the most obvious what kind of treatment the patients received for depression, including medicinal drug treatment. Limitations also include IPAQ being a relatively complex instrument for reporting physical activity 43 and many of the patients had challenges in scoring their activity level. For example, the participants answered the questions based on their own interpretations on what constitutes vigorous, moderate, or low intensity physical activity. Our impression was that patients to a certain degree underestimated their level of physical activity. This may be due to the fact that IPAQ was designed for population-level surveillance, and may be less appropriate for small-scale clinical studies.
Conclusion
In conclusion, the current study shows that inpatients with AUD or other SUDs seem to benefit from physical activity for level of depressive symptoms. Physical activity can be one treatment strategy that can be efficacious in reducing depressive symptoms, at least up to a certain level of physical activity. This suggests that engaging in physical activity during treatment could reduce depressive symptoms and at least indirectly improve treatment outcomes. Future research should design specific interventions using different levels of physical activity in a more systematic way to investigate the impact of such interventions on depressive symptoms.
Supplemental Material
sj-docx-1-sat-10.1177_11782218231175813 – Supplemental material for The Association Between Regular Physical Activity and Depressive Symptoms Among Patients in Treatment of Alcohol and Substance Use Disorders
Supplemental material, sj-docx-1-sat-10.1177_11782218231175813 for The Association Between Regular Physical Activity and Depressive Symptoms Among Patients in Treatment of Alcohol and Substance Use Disorders by Endre Berger, Ingeborg Bolstad, Lars Lien and Jørgen G Bramness in Substance Abuse: Research and Treatment
Footnotes
Acknowledgements
We would like to thank the participants in this study and the clinics from which they were recruited—Riisby, Blue Cross East and Trasoppklinikken treatment centers—for their contributions to this project.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
JGB and LL had the original idea to the study and designed it. IB gathered all the data and did some statistical analysis. EB wrote the first draft of the manuscript and did some statistical analysis. All authors contributed equally to the writing of the final manuscript and all authors approved it before submission.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.