
Abstract
Background:
There are multiple, reliable, and authoritative federally managed data sources for understanding the incidence and prevalence of substance use disorder (SUD) and its sequela. However, there remains a gap in metrics representing the need and capacity for treatment and related supports within local communities. To address this challenge, Calculating an Adequate System Tool (CAST) was developed in 2016 by an interdisciplinary group of researchers at the Substance Abuse and Mental Health Services Administration Center for Behavioral Health Statistics and Quality to assess the capacity of the SUD care system within a defined geographic area. It allows for risk assessment of local social and community determinants of substance abuse, as well as an assessment of local service needs across the continuum of SUD care.
Methods:
This article describes the application of the CAST to 2 counties in Ohio and 1 county in Montana. The purpose of using CAST for each area, results of the application, and experiences in utilizing the tool are described.
Results:
Application of the CAST demonstrated unique findings within each of the geographic areas. In Ohio, recovery support services were lacking in both counties assessed, while differences in crime rate and alcohol outlet density were attributed to varying rates of drug-related hospitalization. Notable findings in Montana included an oversaturation of coalitions focused on substance use prevention and gaps in the areas of detoxification services, partial day treatment, recovery residences, and peer support specialists.
Conclusions:
CAST is a useful tool for guiding decision-making relative to substance use care needs and capacities for local geographic areas. Findings should be interpreted thoughtfully and in the context of data availability. CAST continues to be enhanced and further expanded for assessing capacity of local and statewide substance use care systems.
Introduction
Methods for estimating capacity of substance use care systems have been historically limited 1 because they generally lack clear methods for quantification of need and capacity. Network adequacy has evolved as one strategy for addressing this limitation but tends to focus on prevalence and reach of medical professionals. 2 One exception to this pattern is the Calculating an Adequate System Tool (CAST). The prototype of CAST was initially developed by a research team at the Substance Abuse and Mental Health Services Administration (SAMHSA) Center for Behavioral Health Statistics and Quality, including 1 author of this article. CAST was designed to estimate and assess community-specific substance use disorder (SUD) capacity and service redundancy.3,4 Following the initial development of the tool at SAMHSA, Dr. Green and the staff of JG Research & Evaluation (JG) created new versions of the instrument and expanded utilization. CAST provides information to guide decision-making regarding the number of health practitioners, programs, and interventions needed to provide SUD treatment across the continuum of care from prevention to recovery. CAST has 2 core elements: (1) a program saturation estimates for 32 interventions across the continuum of care and (2) a risk score based on social determinants of behavioral health.
This report is a profile of the use of CAST in 2 settings, 2 counties in Ohio and 1 county in Montana. The version of CAST used in each of these assessments was 2.0, which was developed in Microsoft Excel. Since then, JG has developed a web-based version of CAST 3.0 and continued to expand the inventory of interventions that utilize the CAST algorithms for estimating service capacity and saturation along the substance use continuum of care.
Methods
This brief report is based upon participant observations of the article’s authors during their use of CAST in 2 separate projects. During these projects, research team members created field notes about successes, challenges, and opportunities for further development of CAST. These field notes form the basis of content for this brief report. The data required for the calculation of risk scores are accessed through publicly available data on the demographic, social, and community indicators of behavioral health as well as community needs through census data (eg, American Community Survey). The assessment of resources and needs in each study were gathered through primary data collection with a standardized survey instrument, distributed among organizations that provide the interventions examined in each CAST assessment.
Ohio
CAST was applied to 2 different geographic locations in Ohio to gain a better understanding of their unique needs and capacities. Additionally, we were interested in exploring similarities and differences in CAST application between a large, urban county (Franklin County Ohio, and the home of the state’s capital, Columbus) and a small, rural one (Scioto County, home of Portsmouth).
Following the instructions in the CAST manual, 4 each Ohio county-level risk score was calculated based on local demographic characteristics, social indicators of behavioral health (eg, high school dropout rate), and community indicators of behavioral health (eg, alcohol outlet density). The total risk score was then categorized into 1 of 3 risk levels: low (0-9), moderate (10-20), and high (21-33). CAST calculated an adjusted community need, representing the maximum community need (ie, the number of services needed to service the total population in a county) and accounting for its program usage rate. The observed community needs represented the number of existing services available as identified through reliable data sources (eg, SAMHSA service locator, National Directory of Drug and Alcohol Abuse Treatment Facilities, Alcohol Anonymous websites). The estimated service and capacity needs in a community were then calculated by subtracting the observed community need from the adjusted community need. Data on demographic, social, and community indicators of behavioral health were identified using the American Community Survey’s 5-year estimates. 5 Local needs assessment, reports, and online sources (eg, SAMHSA, National Alliance on Mental Illness, Psychology Today) were used to identify the number of existing services locally.
Missoula County, Montana
The United Way of Missoula County Montana was looking to establish a county-wide coalition to address community-level concerns about the adverse impacts of substance misuse in the community. In the planning process for the coalition, key stakeholders identified a need to better understand system capacity throughout the SUD continuum of care. An assessment that could aid the fledgling coalition understand how their efforts would not duplicate those of existing providers and coalitions.
The United Way contracted with JG to complete a CAST assessment of the county. In alignment with the Montana State Substance Use Disorder Task Force Focus Areas, the assessment used CAST algorithms to understand the capacity of Partnerships, Prevention, Treatment & Recovery, and Harm Reduction interventions. One unique element to the project was an effort to understand demand from noncounty residents who utilized services in Missoula County, as it functions as a regional hub for a 5-county region in Southwest Montana.
Results
Ohio Case Study
The key findings from the CAST assessment of Franklin and Scioto Counties included:
A high crime rate and high alcohol outlet density contributed to a higher risk of alcohol and drug-related hospitalization in Franklin County compared with Scioto County.
Gaps in SUD treatment (Franklin County: inpatient and outpatient; Scioto County: outpatient)
A broad lack of recovery support services (RSS) across both counties.
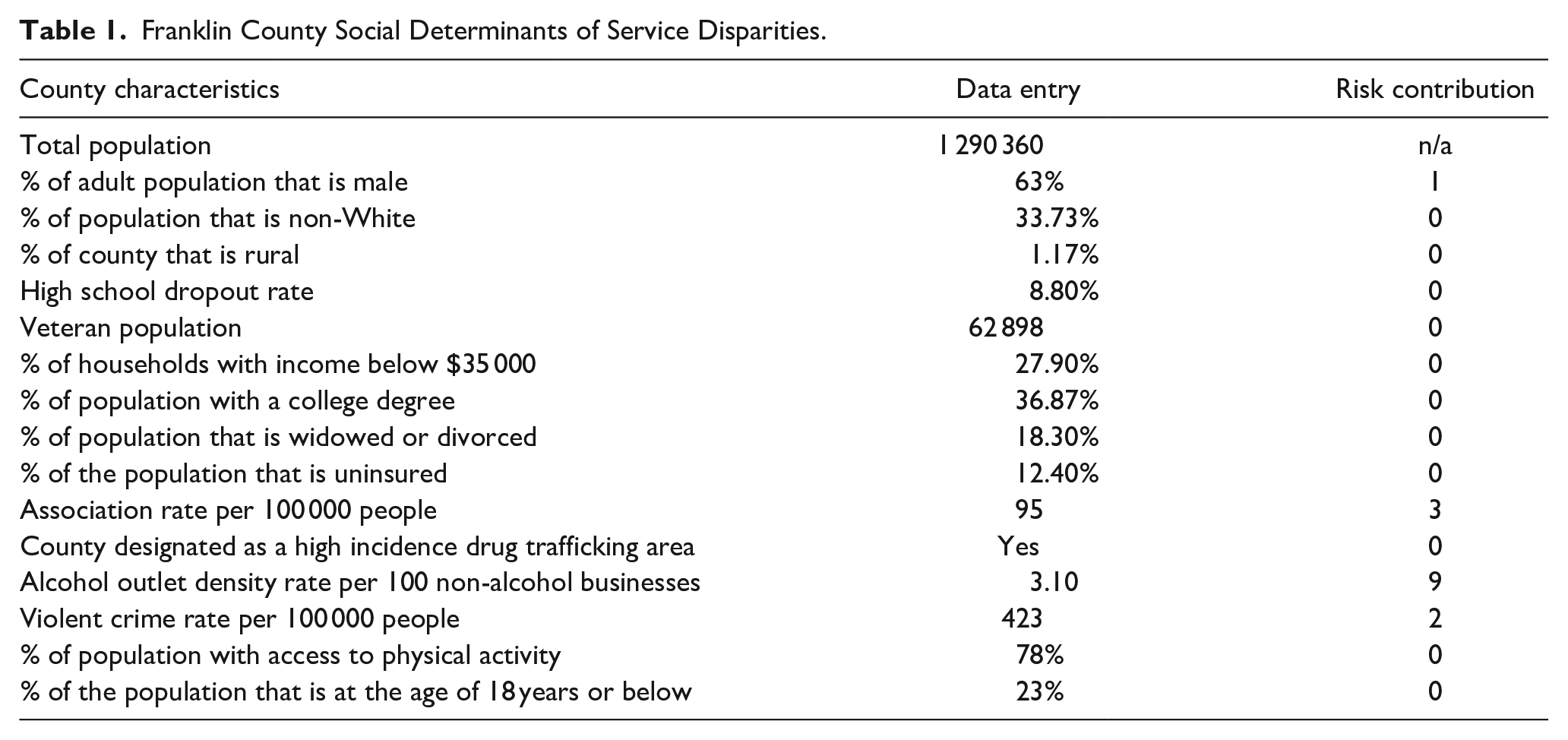
The social determinants of service disparities of Franklin County are presented in Table 1. Based on these determinants, Franklin County has a risk score of 15 (medium risk). The risk score of Franklin County is 0% to 25% above that of the national median for hospitalization due to drugs or alcohol. A high proportion of the male population, low social association rates, relatively high crime rate, and high alcohol outlet density contributed to the risks of SUD-related hospitalization. Improving social connectedness, reducing the crime rate, and reducing alcohol outlet density may help reduce the substance use-related hospitalization risk in Franklin County. Furthermore, community capacity assessment (Table 2) using CAST shows that Franklin County has service gaps in inpatient SUD treatment, outpatient SUD treatment, and RSS. Franklin County has a deficit in every category of RSS except for educational support. The county also needs 854 additional weekly substance abuse support groups and 203 additional housing assistance programs to meet the local needs.
Franklin County Social Determinants of Service Disparities.
Franklin County Service Needs.
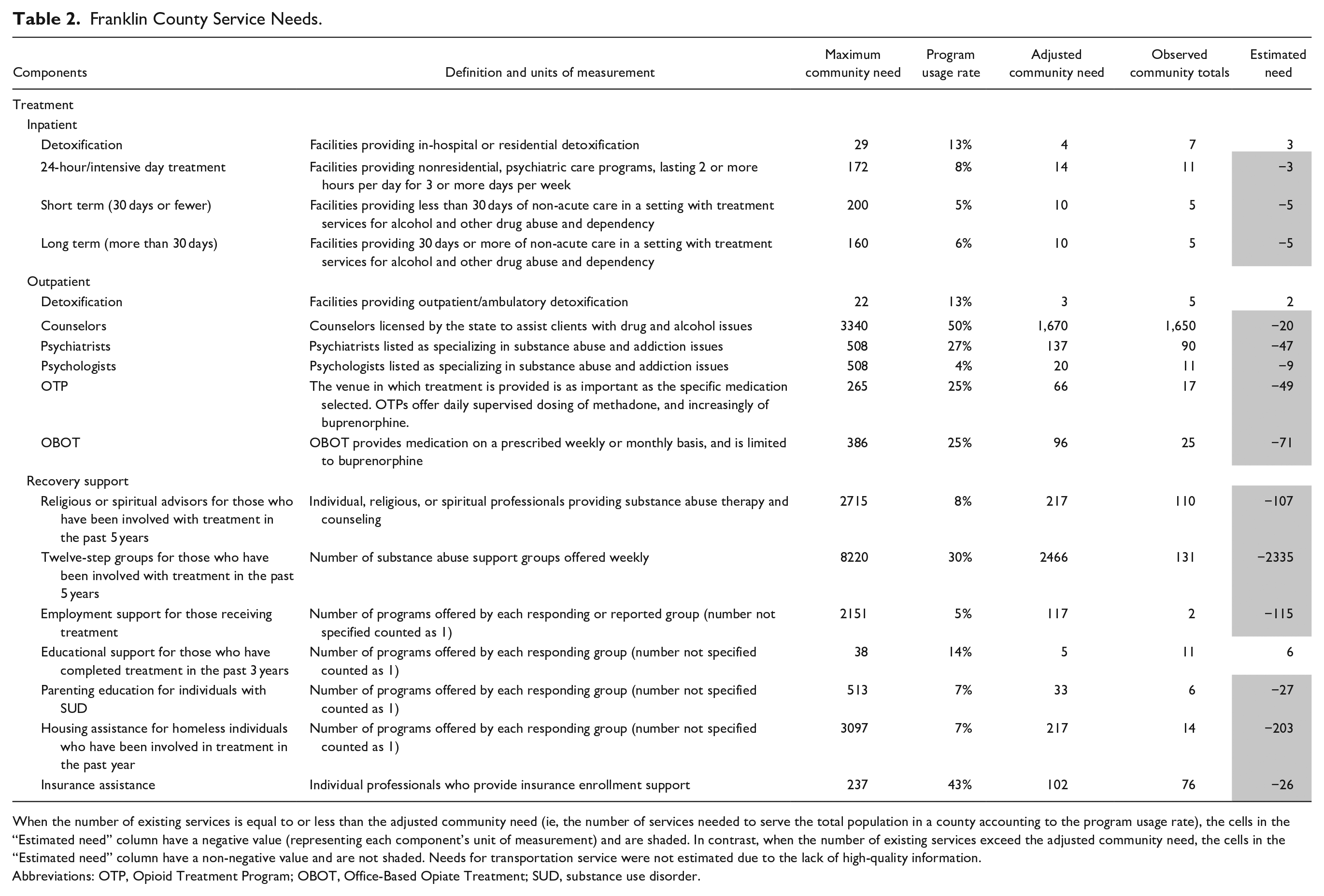
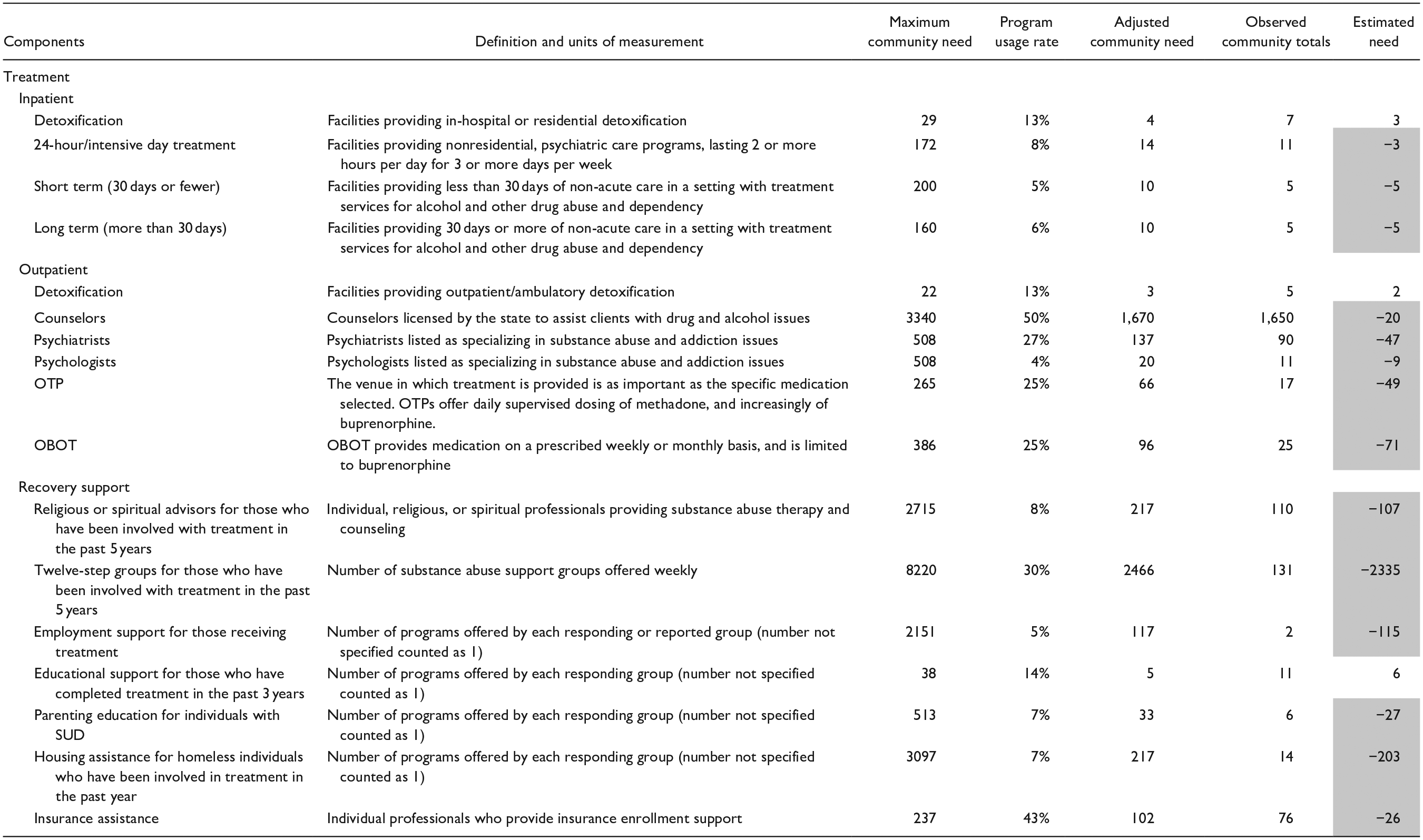
When the number of existing services is equal to or less than the adjusted community need (ie, the number of services needed to serve the total population in a county accounting to the program usage rate), the cells in the “Estimated need” column have a negative value (representing each component’s unit of measurement) and are shaded. In contrast, when the number of existing services exceed the adjusted community need, the cells in the “Estimated need” column have a non-negative value and are not shaded. Needs for transportation service were not estimated due to the lack of high-quality information.
Abbreviations: OTP, Opioid Treatment Program; OBOT, Office-Based Opiate Treatment; SUD, substance use disorder.
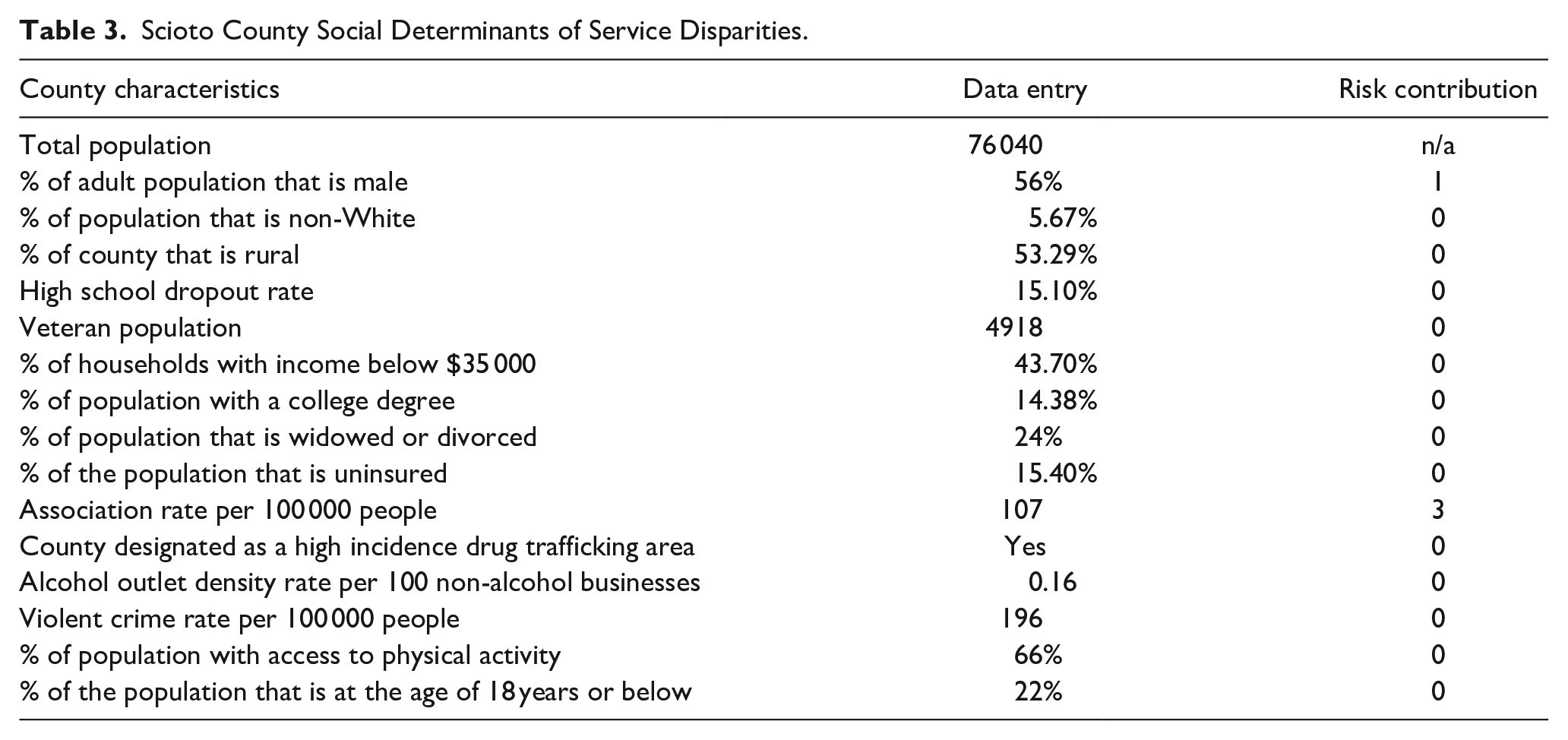
The social determinants of service disparities of Scioto County are presented in Table 3. Based on these data, Scioto County has a risk score of 4 (low risk), suggesting a risk equal to or lower than the national median for hospitalization due to drugs or alcohol. Low rates of social association are the major factor contributing to the risk of substance use-related hospitalization in Scioto County. Improving social connectedness plays an important role in reducing the substance use-related hospitalization risk in Scioto County. Additionally, CAST shows that Scioto County has service gaps in outpatient SUD treatment and RSS (Table 4). Specifically, Scioto County shows a deficit in 3 categories of RSS (ie, transportation, employment support, and housing assistance). An estimated 2180 transportation vouchers and an additional 5 employment support programs and 8 housing programs are needed for those in recovery.
Scioto County Social Determinants of Service Disparities.
Scioto County Service Needs.
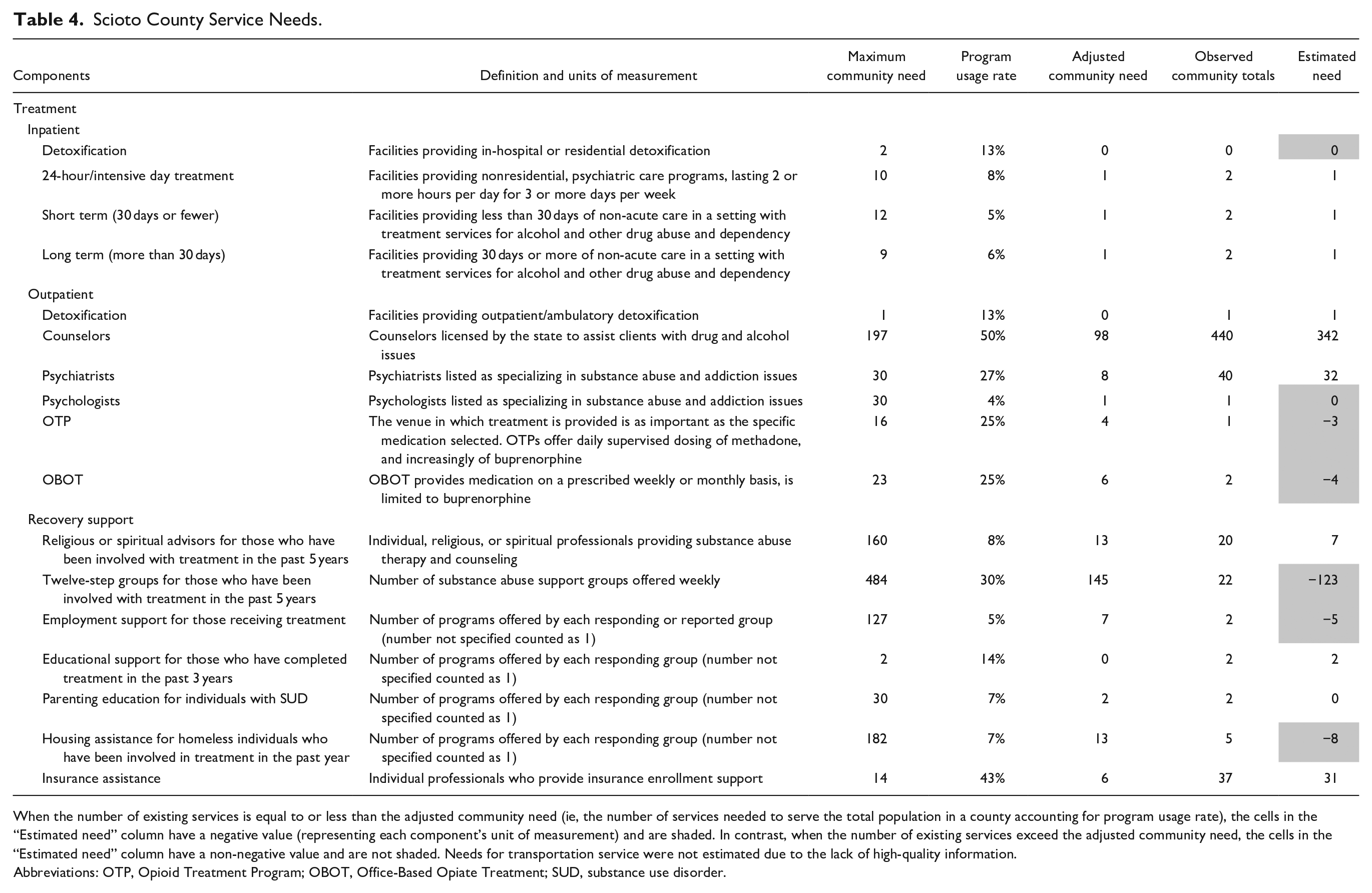
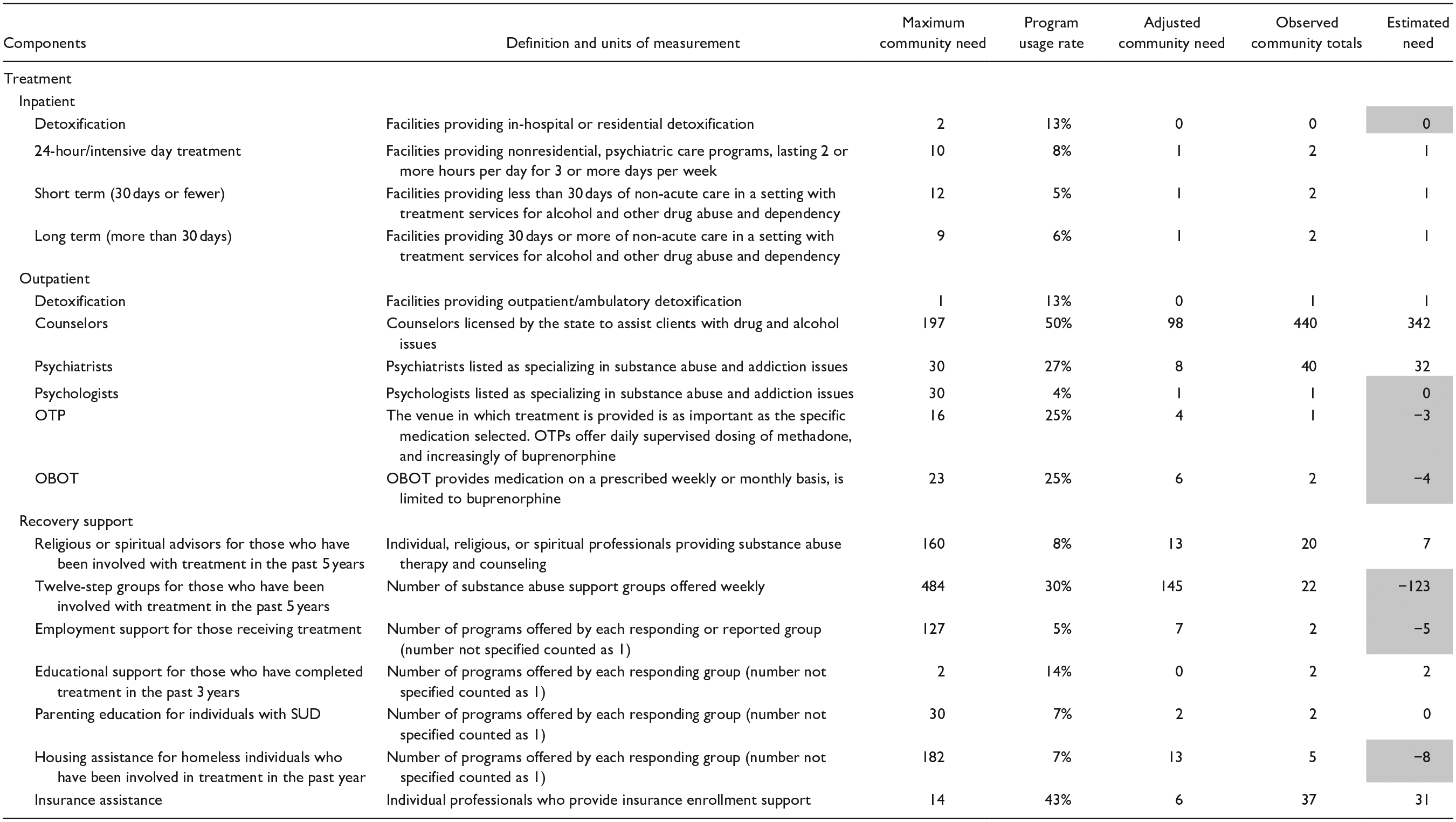
When the number of existing services is equal to or less than the adjusted community need (ie, the number of services needed to serve the total population in a county accounting for program usage rate), the cells in the “Estimated need” column have a negative value (representing each component’s unit of measurement) and are shaded. In contrast, when the number of existing services exceed the adjusted community need, the cells in the “Estimated need” column have a non-negative value and are not shaded. Needs for transportation service were not estimated due to the lack of high-quality information.
Abbreviations: OTP, Opioid Treatment Program; OBOT, Office-Based Opiate Treatment; SUD, substance use disorder.
Missoula County, Montana (MT) Case Study
The key findings from the CAST assessment of Missoula County:
A need for additional community-based prevention and health education programs.
An oversaturation of coalitions focused on substance use prevention, which may in turn dilute resources and focus.
Gaps in services for detoxification, partial day treatment, recovery residences, and peer support specialists.
Supply of inpatient capacity is adequate for the county but inadequate for the region.
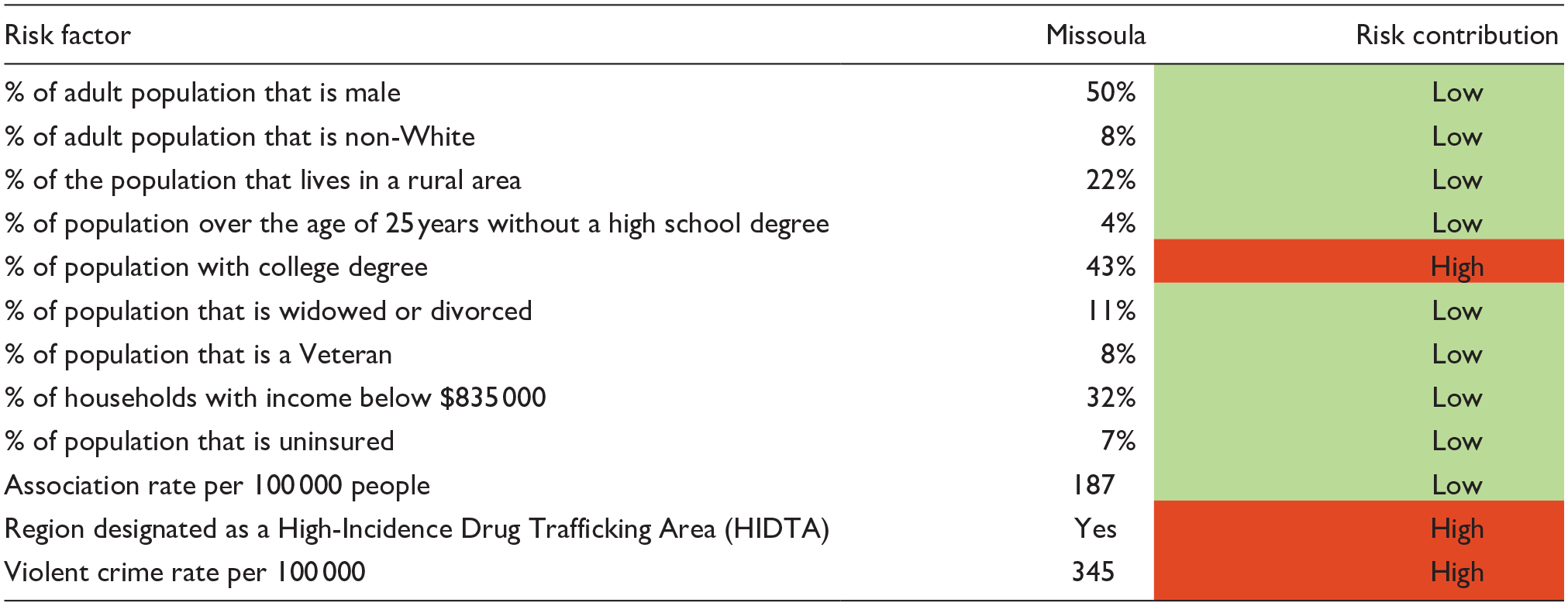
As with the Ohio project, the social determinants of behavioral health were utilized in Missoula County to identify areas of social risk that could be the focus of sustained, community-based prevention and education. Table 5 provides a summary of the results, showing a low risk level in the county overall.
Risk Factors in Missoula County for Increased Emergency Department Utilization for Behavioral Health Condition.
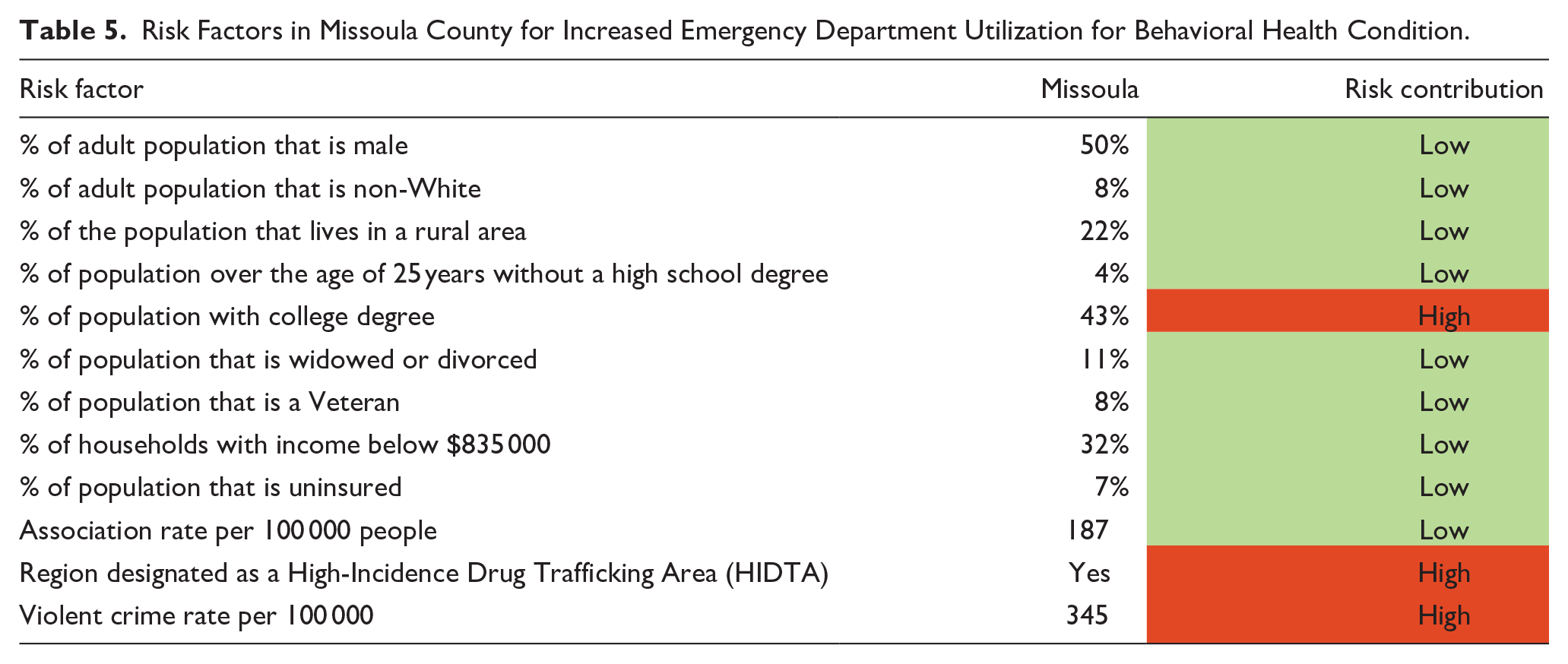
As noted, CAST uses estimates of need and utilization from the population within a bounded geography and compares this population estimate with the totals of programs provided within the community over 1 year. In the Missoula assessment, prevention programming was a key priority area for the coalition, and the assessment concentrated on a detailed assessment of prevention programs across the universal, selected, and indicated prevention continuum.
Figures 1 to 3 provide the results of the assessment of program saturation for universal, selected, and indicated prevention activities in the county. The key takeaway from the utilization of CAST in Missoula County was the need for the emerging coalition to concentrate their efforts on expanding selected and indicated prevention programming efforts, which would in turn improve penetration of prevention programming for at-risk populations. During their discussion prior to the assessment, they had intended to develop robust universal prevention programs. However, the quantification of program saturation within the community clarified the gaps and allowed the coalition to concentrate their efforts in a manner that complimented existing community-wide efforts and improved the prevention continuum for their county.
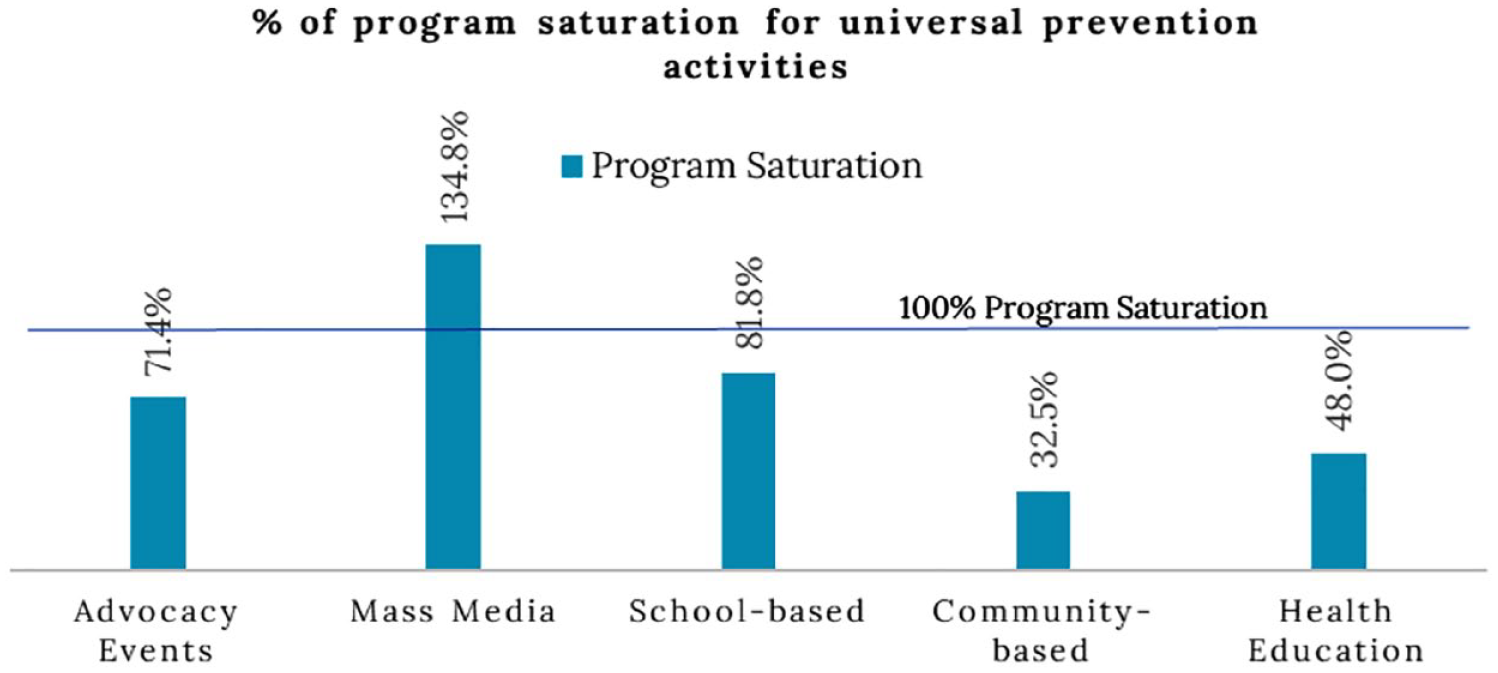
Program saturation for universal prevention activities in Missoula County, Montana.
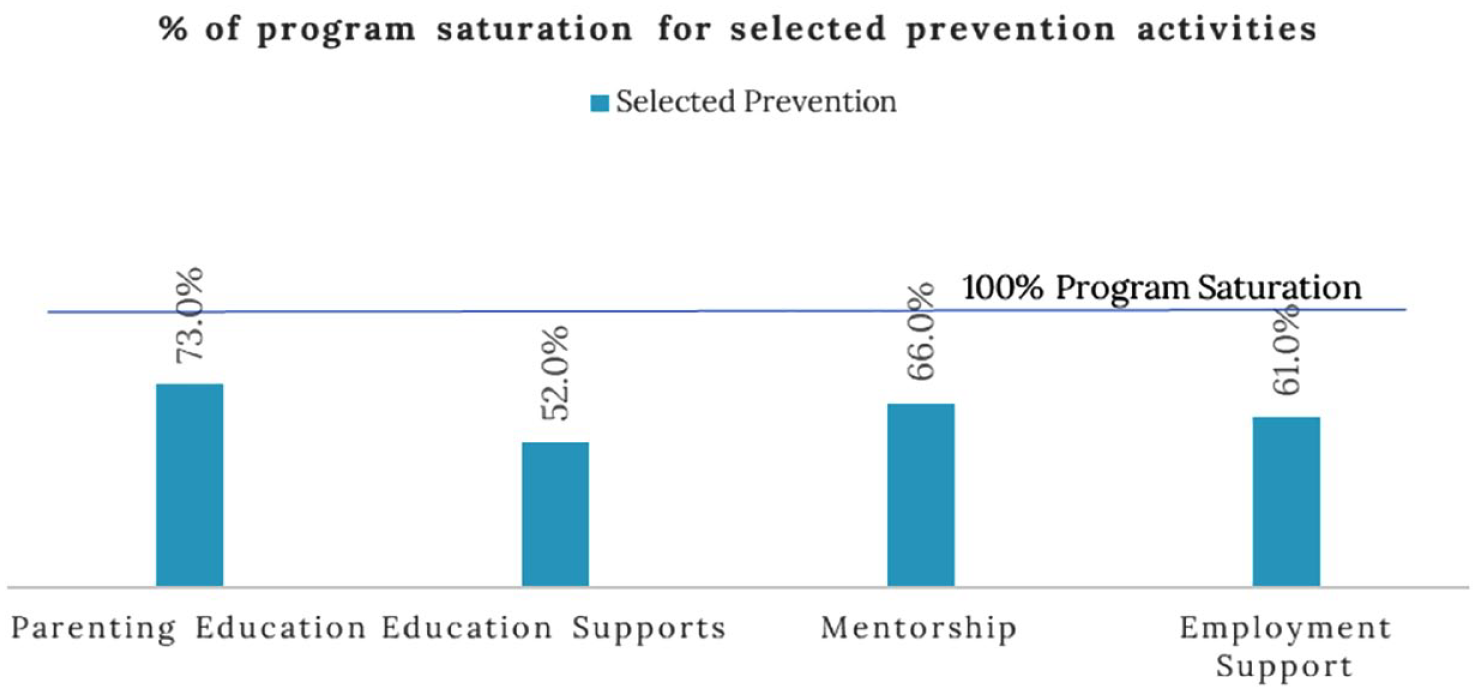
Program saturation for selected prevention activities in Missoula County, Montana.
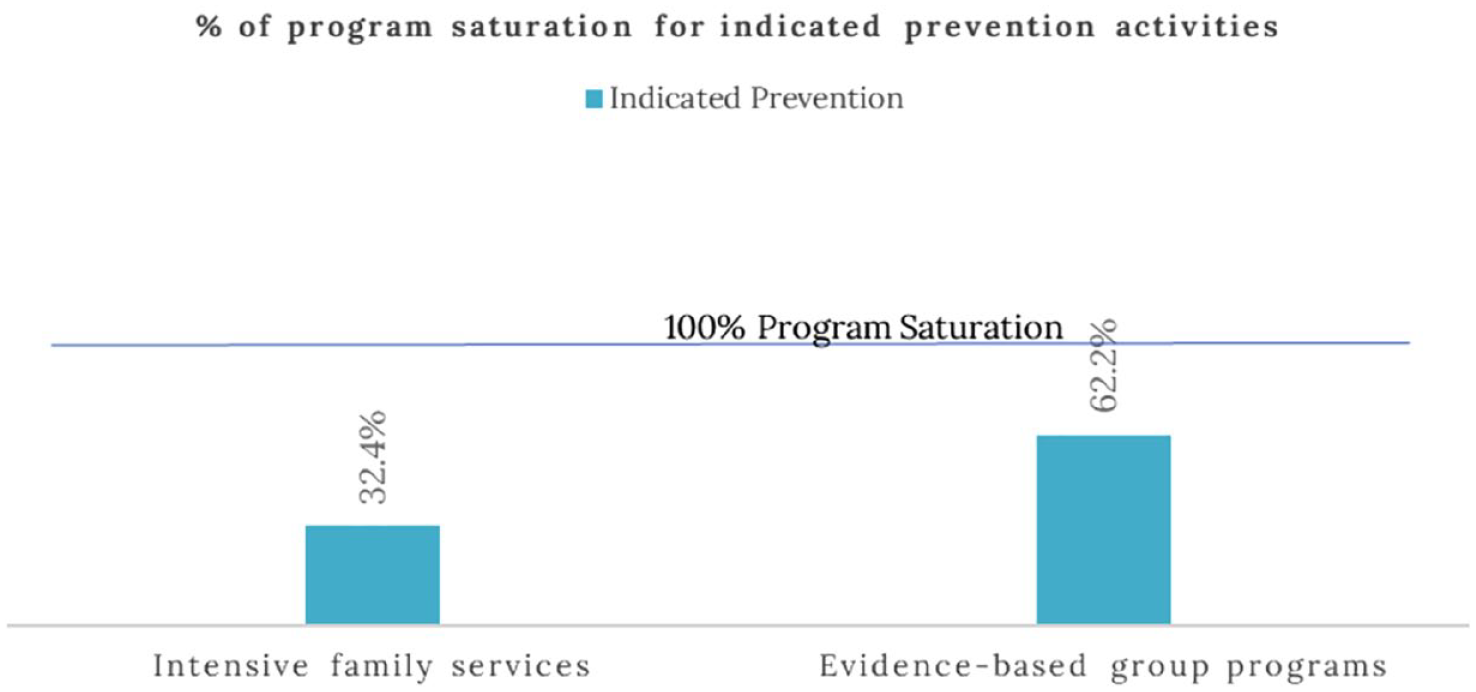
Program saturation for indicated prevention activities in Missoula County, Montana.
Conclusions
CAST is designed to assist with short- and long-term planning for improving the behavioral health of communities. Program saturation, estimated with CAST algorithms, should be interpreted as a guide for decision-making and not a rigid boundary for program activity levels. CAST is predicated on the assumption that resources are finite and decisions need to be made about how financial and human capital are allocated within a given community. It is important to note that CAST estimates are based upon data that were provided by community organizations and not all organizations that responded to the survey provided detailed program activity information. In both the Ohio and Montana projects presented in this research brief, the logic of CAST and the quantification of need were able to elucidate community-level needs and differences in a manner that allowed for meaningful action among the coalitions that commissioned the studies.
Since the completion of the 2 assessments presented in this research brief, CAST has continued to be updated and expanded by staff at JG. CAST was utilized to complete a statewide assessment of the substance use care continuum in Nevada in 2022 and in Oregon in 2023. In each of these projects, state legislatures allocated funding for the completion of statewide assessments that “quantified need” by region. Through conversations with the principal investigators of each of these projects, staff at JG provided support for the independent utilization of the instrument, demonstrating the potential for broader adoption of the methodology. Additional expansion of CAST took place in Ohio following the application of the CAST to Franklin and Scioto Counties in Ohio. Ohio Recovery Housing (ORH), a state affiliate of the National Alliance for Recovery Residences, chose to adopt the web-based CAST for its use. ORH uses a peer review certification process to create and maintain standards of excellence for recovery housing.
Throughout the projects identified in this research brief, it has become clear that there is a need for further expansion and refinement of quantitative methods for assessing the capacity of the substance use care systems. One of the distinctive elements of CAST, as highlighted in the Missoula County case study, is quantification of prevention programming. Future research and additional efforts should be made to offer mathematical models of demand and program saturation, leveraging the progress made with CAST to improve the ability of community needs assessments to inform resource allocation.
As noted, JG has completed the development of CAST 3.0 as a web-based assessment instrument. All secondary data utilized to produce risk scores are embedded in the application, and users can enter programmatic data to produce saturation estimates for their study. Utilization of the tool is likely to expand, allowing further refinement of the estimate equations and the development of a comparative dataset for understanding system capacity across states and counties. Our hope is that this information can be utilized to refine estimation approaches and strategies for informing resource allocation within substance use care continuums.
Footnotes
Acknowledgements
The authors wish to thank Gretchen Clark Hammond, PhD, MSW, LSW, LCDCIII, TTS, for her support in this work.
Author contributions
B Green - Primary author with responsibility for authorship. K. Cao - Primary co-author with responsibility for authorship. R. McCloskey - Secondary author with responsibility for review and feedback. F. Kim - Secondary author with responsibility for review and feedback.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Compliance,Ethical Standards,and Ethical Approval
Institutional Review Board’s approval was not required.