
Abstract
Background:
This is the final article in a four-part series that presents an operational typology of the field of Traditional, Complementary, and Integrative Medicine (TCIM). Using a series of six “ideal types” (each with two or more subtypes), the TCIM typology provides theoretically driven parameters for classifying the wide range of TCIM therapeutic approaches in use across the globe.
Methods:
The current article, focused on the sixth type—Integrative Therapeutics—closes the series by synthetically elaborating on five distinct “forms” of therapeutic integration (sometimes termed “integrative medicine” or “integrative health care”) at play across the globe: Melting Pot, Co-optation, Multiculturalism, Transculturation, and Third Space.
Results:
Those five forms of integration, elaborated with reference to critical social science and political science literatures and using real-world examples, fall along with a spectrum between the two polarized Integrative Therapeutics subtypes identified in a previous article: (1) Integrative Assimilation and (2) Integrative Equity. These polarities account explicitly for the paradigmatic differences between, and complex differential power relations among TCIM therapeutics and—in particular—with Biomedicine.
Conclusion:
Together, the five forms of Integrative Therapeutics offer an extended typological model for classifying the range of scenarios in which TCIM therapeutics may come to interface with one another, and with Biomedicine, in pursuit of health and well-being for all.
Keywords
Preamble
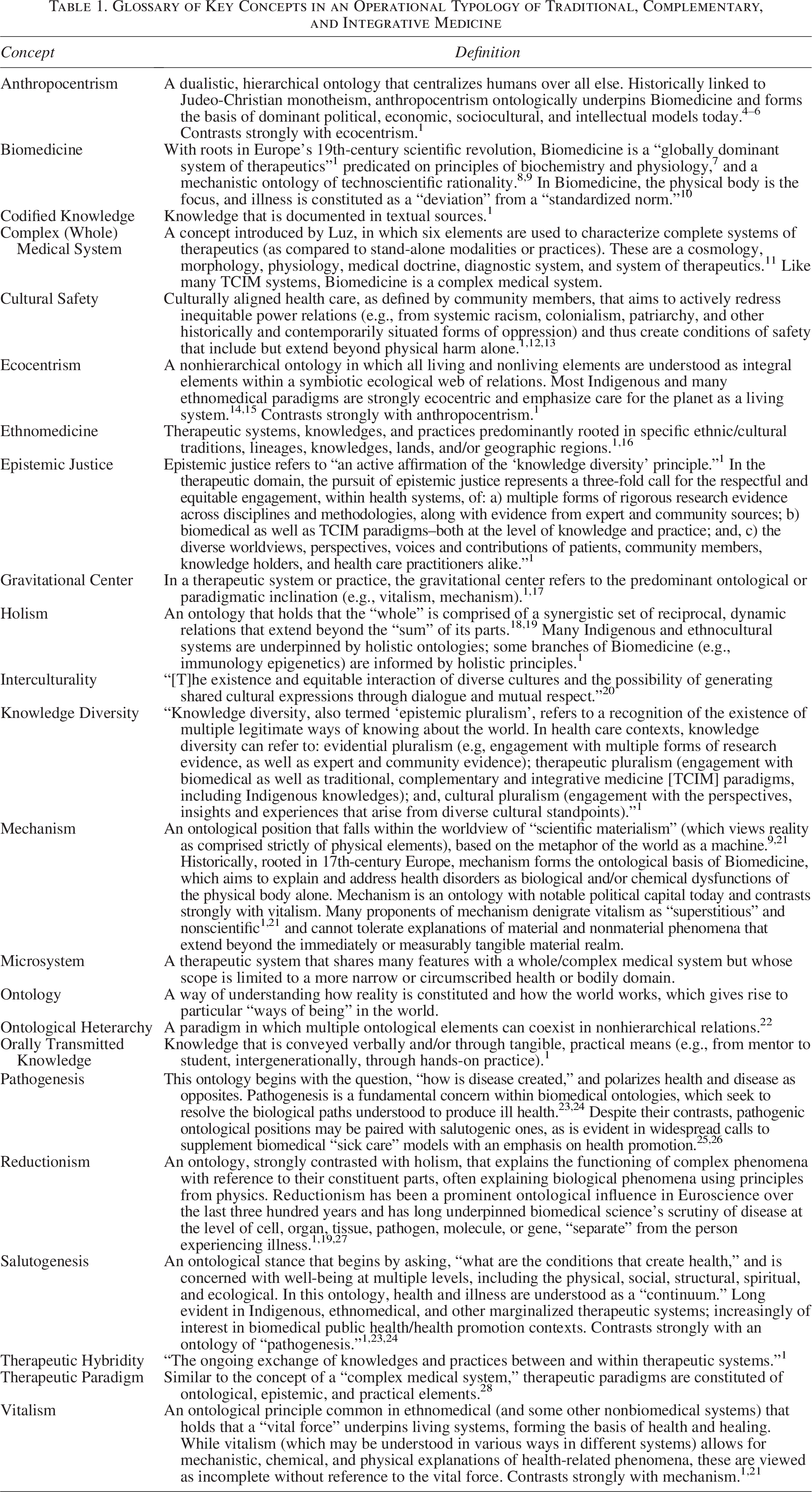
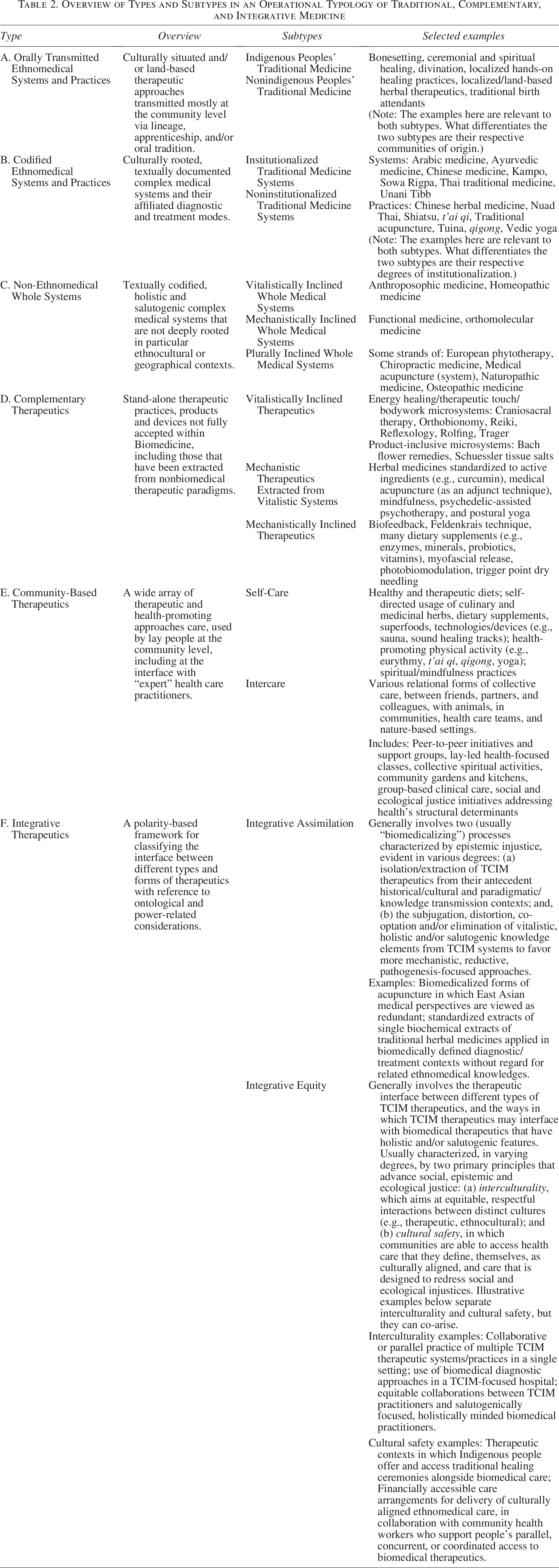
This article is the final in a four-part series presenting an operational typology of the complex and internally diverse field of Traditional, Complementary, and Integrative Medicine (TCIM). Operational typologies are classification models that subdivide broad constructs into meaningful, conceptually driven categories. The first article of the series presents the typology’s conceptual basis; readers may refer to the present article’s glossary (Table 1), for a brief overview. 1 The sixfold typology itself (see Fig. 1 and Table 2) is advanced in the second article of the series. 2 The third article provides knowledge users with a more in-depth explanation of the typology’s application as a classification tool for specific TCIM therapeutics, which are encompassed within the first five types (see Table 2). 3 The current article elaborates in depth on the sixth type, Integrative Therapeutics, which refers to the encounter between multiple TCIM approaches, and with Biomedicine. 1 In this sense, the Integrative Therapeutics category is similar to, but extends beyond, what is increasingly termed “integrative medicine,” “integrative health care,” or “whole health.” Building on two Integrative Therapeutics subtypes presented in the second article of the series, 2 readers will find in the pages that follow a framework consisting of five “forms of integration”: Melting Pot, Co-optation, Multiculturalism, Transculturation, and Third Space (see Table 3 and Fig. 2). This framework offers a comprehensive, conceptually driven tool for analyzing the range of complex ways in which TCIM and Biomedicine may interface within health care contexts, drawing close attention to paradigmatic dynamics and power relations at play.
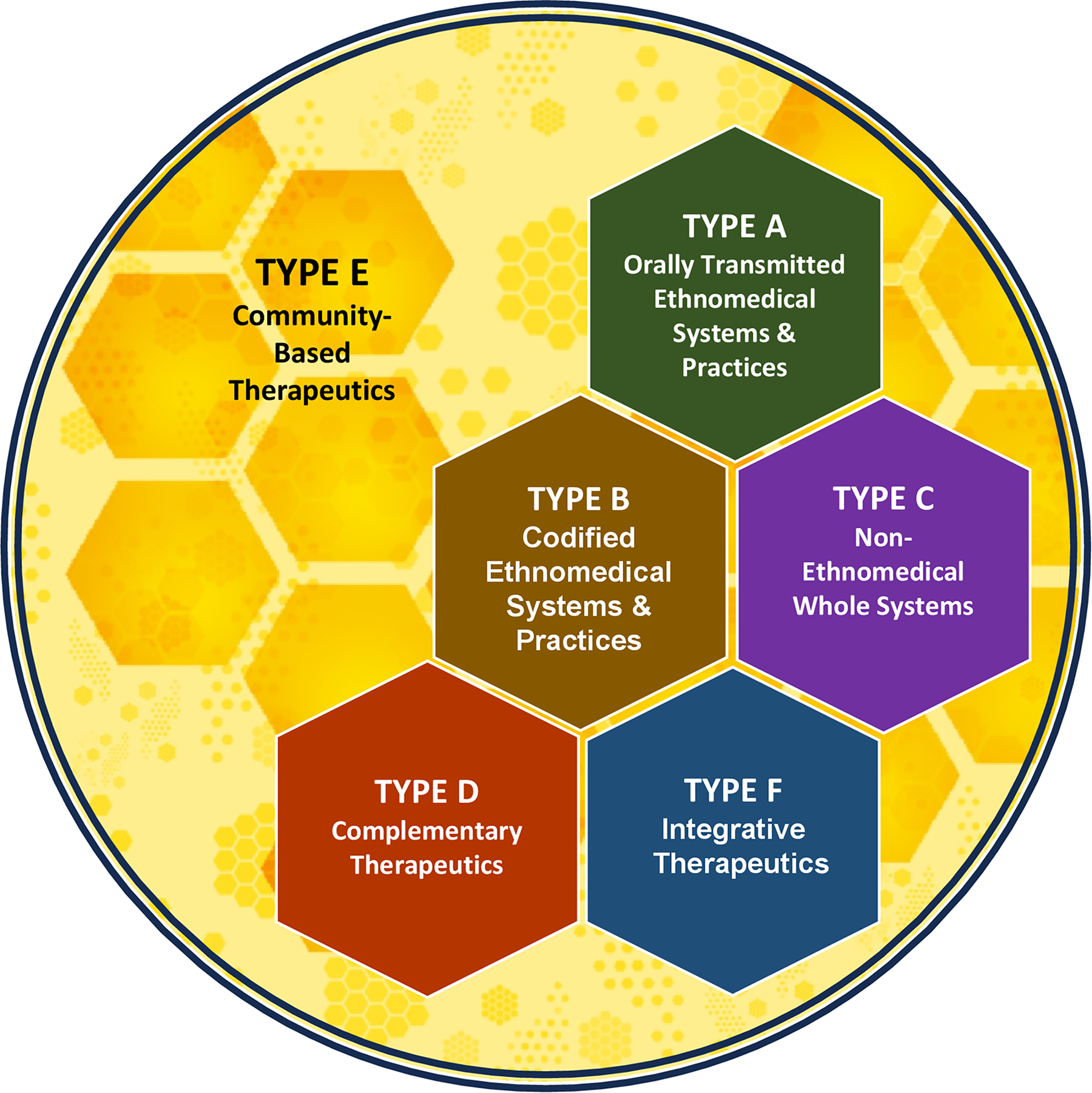
Operational typology of traditional, complementary, and integrative medicine. This figure provides a graphical overview of the six primary types in an operational typology of traditional, complementary, and integrative medicine.
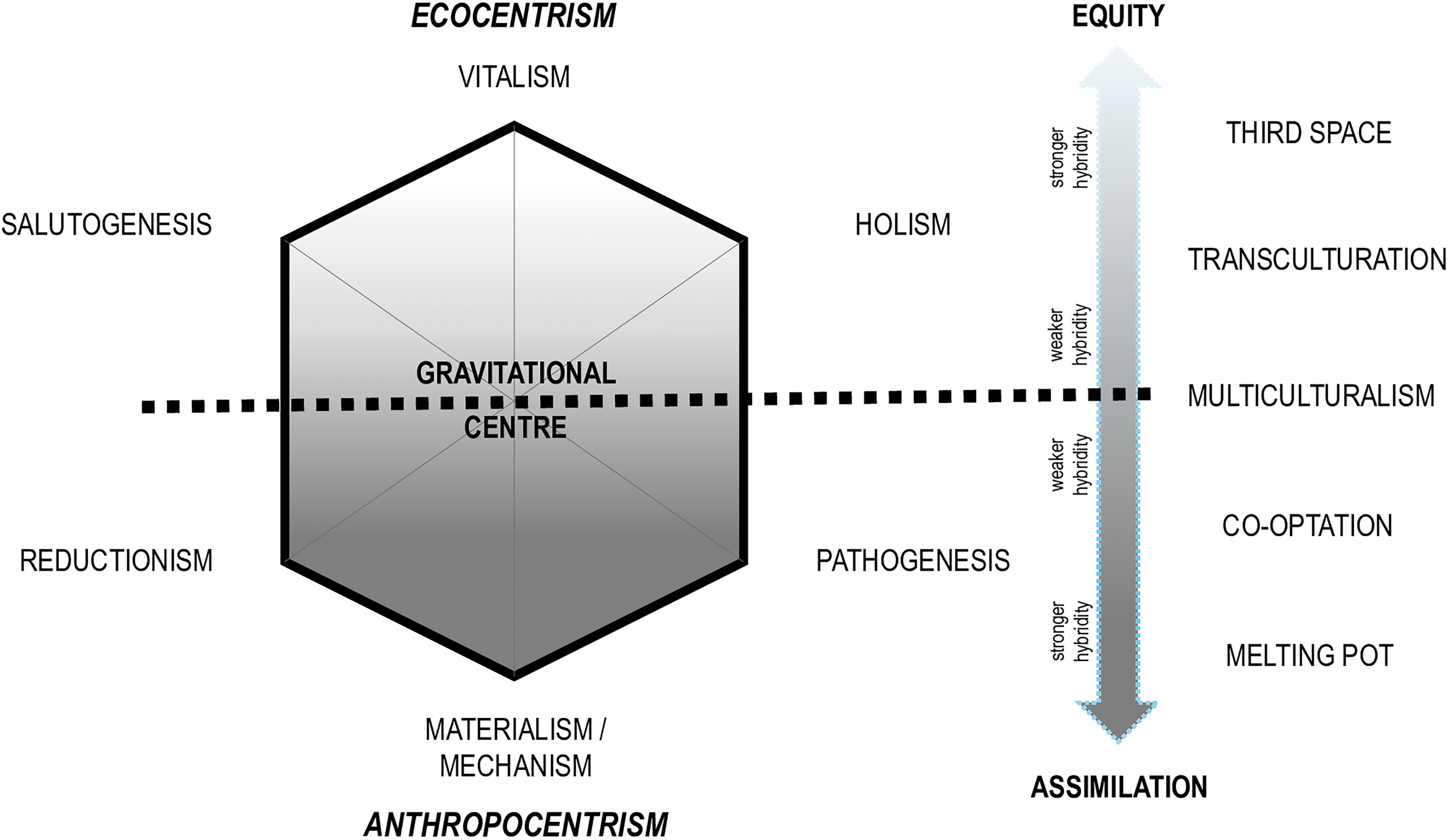
Therapeutic integration framework for traditional, complementary, and integrative medicine. This figure provides a graphical overview of a spectrum of forms of Integrative Therapeutics with reference to two major subtypes (Equity and Assimilation) and key paradigmatic elements.
Glossary of Key Concepts in an Operational Typology of Traditional, Complementary, and Integrative Medicine
Overview of Types and Subtypes in an Operational Typology of Traditional, Complementary, and Integrative Medicine
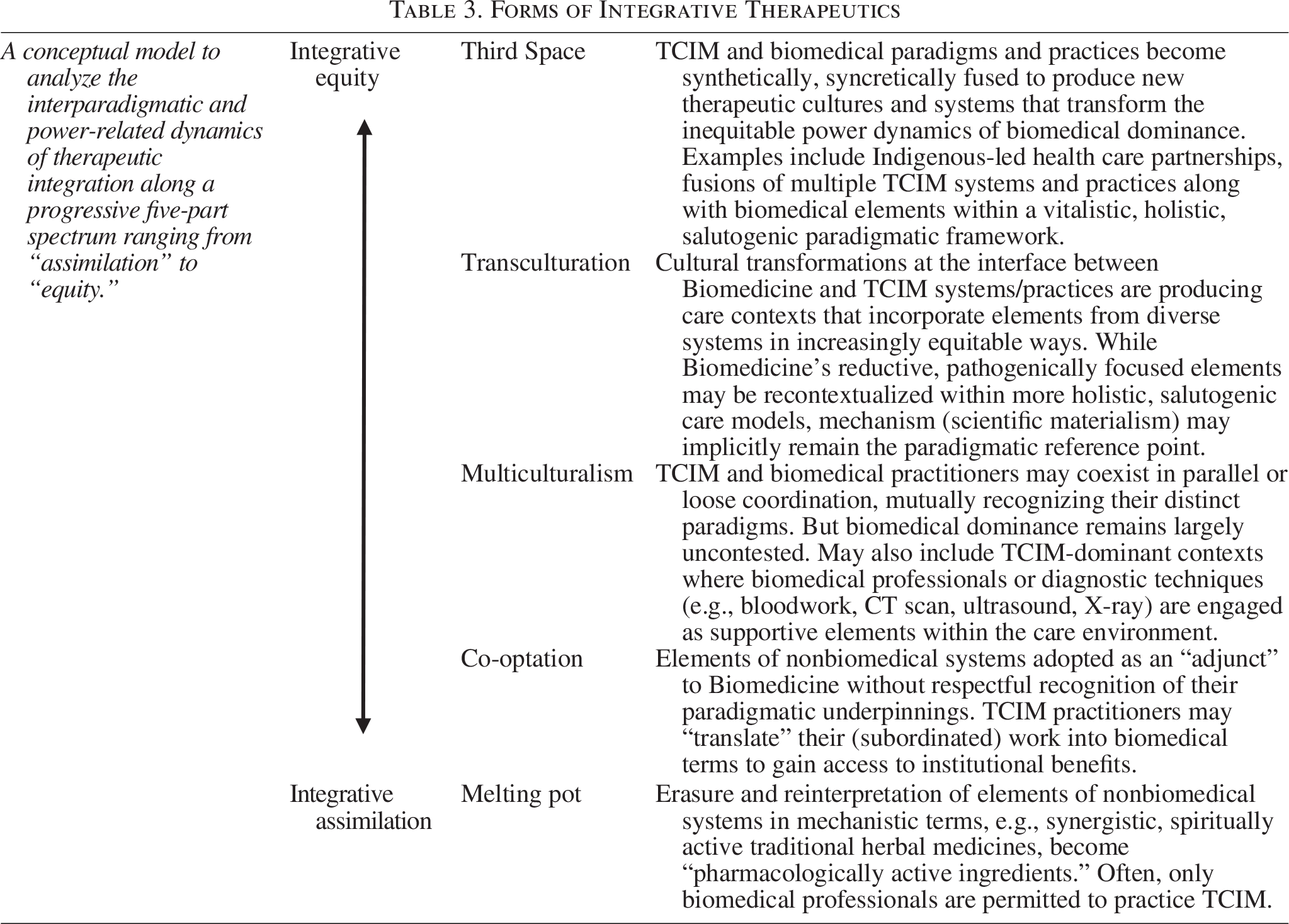
Forms of Integrative Therapeutics
Background
In recent decades, there have been various scholarly efforts to define and/or otherwise constitute categories related to therapeutic integration between TCIM and Biomedicine. In 2004, for example, Boon and colleagues—health systems scholars—used a qualitative content analysis approach to analyzing related literatures of the time to propose a working definition of integrative health care. 29 This definition was aspirational, reflecting a vision of what therapeutic integration might ideally entail. That same year, the same group of researchers advanced a conceptual framework for characterizing “different models of team-oriented health care practice” along with a spectrum from “nonintegrative to fully integrative” in terms of their approach “to patient care.” 30 Also in 2004, Mann and colleagues outlined various models of integrative care, focused on the different settings, practice patterns, and interoccupational referral modes involved. 31
Around the same time period, critical social scientists were documenting the paradigmatic tensions and differential power relations between TCIM and Biomedicine in integrative pursuits.32–35 As Hollenberg for example observed, echoing Shuval’s earlier work, 34 integrative health care settings “may contain health practitioners from ontologically diverse health paradigms,” and that biomedical professionals continued to exert various strategies to “maintain [their] dominance.” 33 Kaptchuk and Miller similarly noted that the “philosophical, epistemological, and practical differences between mainstream medicine and CAM [complementary and alternative medicine] systems” posed a major impediment to their mutual engagement “as equal partners.” 32
By 2009, Adams and colleagues argued that existing “ideal types” addressing therapeutic integration did not sufficiently map “to the empirical reality of integration as identified by research.” 36 They called for a “critical social science perspective” with an emphasis on “a contextual analysis of power [and] knowledge.” Such an analytic approach, they indicated, would situate “health care activities and trends within macro structural and historical specificities” as well as “social and political parameters.” Baer and Coulter similarly called for a critical social science approach to analyzing integrative therapeutics that would account for interparadigmatic tensions between dominant biomedical interest holders and the “vitalistic elements” characteristic of many TCIM systems and practices. 37 They asked:
[Is] what is occurring between biomedicine and CAM … truly integrative as opposed to co-optation or, coadaptation [?] By which we mean, is CAM simply being co-opted into the biomedical paradigm at the level of therapy but not at the more philosophical level? Under this approach, integrative medicine turns out to be biomedicine with CAM therapies added. In other words, the vitalist elements of the paradigm are relinquished in this approach.
As Wiese and colleagues synthetically indicated in a 2010 literature review, there was at once a “lack of adequate theorization” of the integrative medicine phenomenon, and a concurrent “need for a theoretical approach to address the broader social context” of integration, including issues of paradigm and power. 38
Since that time, various theoretical approaches have been advanced to support scholarly analyses of the interface between TCIM therapeutics and Biomedicine. These have included the use of multiple critical social science theories in TCIM-focused studies. 39 However, few specific frameworks for understanding or classifying therapeutic integration have emerged.
In 2014, Lin et al used primary research data to inform a threefold conceptual model that links, in the context of integrative care, national policy models with practitioner delivery models and ultimately, to “consumer” experiences of care. 40 In a 2015 study, Witt and colleagues applied the concept of corporate culture mergers to illuminate and propose paths to transform various challenges evident in integrative therapeutic contexts. 41 Park and Canaway, in a 2019 commentary, proposed a typological “conceptualization of [therapeutic] integration based on the level of institutionalization” of traditional and complementary medicine in particular countries. 42 Their policy-based model descriptively classifies countries as being characterized by “well-established integration strategies; in-process of developing and implementing integration policies, mixed-level of integration; or [I]ndigenous traditional medicine practiced outside the national health care system.” The aforementioned works represent important contributions to the global context of research related to therapeutic integration. However, they do not serve the function of being able to classify, with detailed scholarly nuance, the range of integrative therapeutic contexts in ways that deeply account for issues of paradigm and power. The current article aims to fill this gap.
An Analytic Framework Addressing Therapeutic Integration
As detailed in the previous articles in this series,1–3 TCIM is a complex field that includes a wide variety of distinct therapeutic approaches (see Table 1 and Fig. 1). This includes: (A) Orally Transmitted Ethnomedical Systems and Practices; (B) Codified Ethnomedical Systems and Practices; (C) Non-Ethnomedical Whole Systems; (D) Complementary Therapeutics; (E) Community-Based Therapeutics; and finally, (F) Integrative Therapeutics, the focus of the present work.
Article two of this series characterizes Integrative Therapeutics as a “relational category” that “encompasses the wide range of possible interplays between TCIM therapeutics of various kinds, as well as with Biomedicine.” 2 Such intersections may take place at the level of the individual “lay” person or health care practitioner, within a particular community, between multiple health care practitioners, in a health care facility or institution, within a local or regional health system, and/or at the national health systems level. Integration may involve engagements between community members, local knowledge holders and community leaders, licensed and unlicensed health care practitioners, policy makers, medicine growers and manufacturers, civil society organizations, as well as corporate actors. Therapeutic blendings may take place concurrently or in sequence, in parallel, in co-ordination, or in collaboration, and sometimes with reference to an explicit “model of care.” Integration’s dynamics will also be informed by context-specific conditions, including interpersonal, historical, cultural, economic, and political factors.
The second article in the series, which presents an operational typology of the field of TCIM as a whole, delineates two primary subtypes in Integrative Therapeutics, conceptualized as the polarities of: (a) Integrative Assimilation and (b) Integrative Equity. 2 These polarities “explicitly account for the differential power relations between Biomedicine, with, and between the wide range of” TCIM approaches in practice in particular contexts. Recognizing that therapeutic integration represents a form of therapeutic hybridity,1,2 and as detailed below, these power relations may be understood at least partly with reference to the paradigmatic features of interfacing health care approaches. As explained, all therapeutic approaches have their own paradigmatic “gravitational centers” in which particular “ontological” (i.e., philosophical) elements (e.g., mechanism/materialism, vitalism, reductionism, holism, pathogenesis, salutogenesis) will predominate. (Readers wishing to refresh their understanding of those concepts may refer to articles 1 and 2, and/or refer to the glossary in Table 1).1,2
The subtype of Integrative Assimilation refers to a “‘biomedicalizing’ process, that is, a unidirectional assimilative process of incorporating nonbiomedical practices (separated from their concomitant knowledges) ‘into’ existing biomedically dominant health systems.” 2 It most often takes place in contexts wherein “one or more TCIM approaches are interfacing with forms of Biomedicine characterized concurrently by mechanistic, reductionist and pathogenic ontologies.”
Integrative Equity, conversely, is a subtype characterized by a joint impulse toward social, epistemic, and ecological justice. Here, “multiple ‘therapeutic cultures’…interface in ways that seek to honor their respective paradigmatic…features,” and proactive efforts are made to redress “the power imbalances inherent in the health care system” including “structural racism and discrimination” as well as those related to gender and other categories of identity. Such scenarios are more frequently evident in contexts of interface “among multiple TCIM therapeutics” (with predominantly vitalistic, holistic, and/or salutogenic characteristics) as well as “between TCIM therapeutics and a range of forms of Biomedicine that have some salutogenic and/or holistic ontological features.”
The second article in this series illustrated, with reference to the examples of turmeric, acupuncture, and birth workers, how Type F of the typology (Integrative Therapeutics) and its polarized subtypes might be understood. 2 Those examples will not be repeated here. Instead, to support readers in applying Type F to characterize the complex dynamics of diverse integrative therapeutic contexts, the current article introduces a more detailed conceptual model. This model, shown in Figure 2 and summarized in Table 3, delineates five distinct “forms” of therapeutic integration, incrementally positioned between the two polarized subtypes identified within the typology itself. Those “forms” closer to the top of Figure 2’s vertical spectrum are more paradigmatically inclined toward Equity, with those toward the bottom more inclined to Assimilation dynamics. This spectrum may be theoretically understood with reference to the hexagon on the Figure’s left, which shows the paradigmatic elements of integrative therapeutic hybrids.
In cases where one sees vitalistic, salutogenic, and/or holistic ontological tenets predominating or shared between the multiple therapeutic approaches being integrated, one may anticipate an “antigravitational” (upward along with Fig. 2’s linear spectrum) toward creation of new therapeutic hybrids characterized by Integrative Equity principles. Conversely, where one sees the principles of mechanism, reductionism, and/or pathogenesis strongly predominating in even one of the therapeutic approaches in interface, one might anticipate a downward “gravitational” trend toward Assimilation. This is because, as elaborated in the first article in this series, 2 materialistic/mechanistic, reductionistic and pathogenetic ontologies are characterized by a kind of philosophical “monotheism” which renders them unable to “tolerat[e] alternative paradigms.” 43 By contrast, vitalism, salutogenesis and holism are more “inclusive” ontological positions that may readily “accept” or “absorb” the premises of alternate perspectives, without compromising their own integrity. 2
The sections that follow elaborate on the five distinct forms of therapeutic integration, with examples, and with reference to the principles underlying the two Type F subtypes identified in the typology itself. These five forms may be understood as an extended elaboration of those two subtypes, meant to support the typology’s application with reference to the complex nuances of therapeutic integration across health systems.
Melting pot
The “melting pot” refers to a principle most famously implemented as a political framework in the United States of America (USA), wherein “immigrants are expected to become members of the US American society by discarding their old World identities and taking on cultural traits, traditions, and habits of the dominant society.” 44 This “assimilationist” model, conceptually, holds that the norms of a sociopolitically dominant group should persist, and “not [be] expected to be altered by, or to accommodate” the “cultural traits” of groups that enter the dominant culture. With reference to therapeutic integration, the “melting pot” conceptually legitimates biomedical science as a hegemonic form of knowledge, exemplifying what Hollenberg and Muzzin term “paradigm assimilation.”43,44 Biomedicine’s (mechanistic) paradigm “not only appropriates or takes over another entire healing paradigm or system but reinterprets it.” In this process, the “theoretical attributes and characteristics of the appropriated paradigm are then eliminated, redefined, or given new names and meanings by the assimilating paradigm.” They provide the following examples:
[A]cupuncture, understood in traditional Chinese medicine as stimulating the flow of Qi along the body’s meridians to resolve Qi obstruction and to promote healing, becomes instead, in biomedicine, the stimulation of cells to release pain-relieving endorphins. Indigenous herbs that are locally viewed to have synergistic spiritual, psychoactive, and healing properties are biomedically reduced to having pharmacologically active ingredients. The healing and social relationship between patient and healer…become mere placebo.
Another example of melting pot-style integration would be contexts in which only biomedically trained professionals are permitted to practice TCIM therapeutics, and do so exclusively from a mechanistic, biomedical standpoint.
Because of the strong gravitational force exerted both by Biomedicine’s hegemonic global dominance and by mechanistic ontological perspectives, the assimilative melting pot may be understood as the “default” mode of therapeutic integration that may take hold across global contexts, unless actively resisted. However, with deliberate effort, the epistemic injustice that the melting pot entails and enacts may be transformed in other modes of therapeutic integration.
Co-optation
Co-optation is another political science concept that refers to a dominant group’s adoption of elements from an opposing or subordinated group into its own dominant discourses or frameworks, without reinterpreting these elements to the degree evident in paradigm assimilation. Hollenberg and Muzzin’s concept of “paradigm appropriation” is useful here, characterizing situations in which “biomedicine appropriates certain aspects from other healing systems or traditions without fully acknowledging the paradigmatic worldview from which the particular treatment aspect was taken.” 43 In other words, therapeutic practices from vitalistic systems may be taken up within biomedically dominant contexts, whether by biomedically trained clinicians or even by practitioners who (quietly) draw on vitalistic concepts to implement these practices. Here, however, the appropriated therapeutic elements are contextually framed “as technically ‘complementing’ biomedicine, versus as a legitimate healing system.” For example, a practitioner of East Asian medicine might practice acupuncture as a “technical adjunct” to biomedical practice but would not expect their paradigmatic explanations for the treatments they offer to be given any professional weight. Rather, within the context of an interdisciplinary, biomedically dominant team, the East Asian medicine clinician might continuously engage in rough “translations” of their therapeutic approaches in biomedical terms, ultimately subordinating, rendering invisible their work’s “key theoretical elements.”
As Fenner has reviewed, “models of co-optation tend to fall into (or combine) two general categories: transactional models and acculturation models.” 45 Transactional models are those characterized by an “exchange of benefits for political support,” wherein opponents of a dominant regime “agree to contain or limit their opposition as long as the right level of benefits continue to flow.” For example, a TCIM practitioner might choose to be gainfully employed in a biomedically dominant setting under conditions of assimilative co-optation. Despite an acute awareness of the epistemic violence that their experience might entail, they may remain silent about it to preserve their professional or financial security. Acculturation models of co-optation, by contrast, are those in which “the commitments” of incorporated groups are “fundamentally alter[ed]” through co-optation, as they come to “identify with the dominant regime and thus moderating…aspiration to an alternative model.” For example, a TCIM practitioner community may choose to adopt or align itself strongly with Biomedicine’s epistemic, evidentiary, educational and professionalization modes to advance its sociopolitical standing and gain entry to work in biomedically dominant settings and/or gain access to third-party insurance coverage. Despite these apparent short-term advantages, key ontological elements of their work may be lost and even forgotten along with the way, especially for the “next generation” of practitioners.
Multiculturalism
In contrast to the melting pot and co-optation, which subsume vitalistic knowledges in varying degrees, multiculturalism is a political science principle describing a mode of integration that “seeks to actively preserve minority cultures against assimilatory pressures of the mainstream culture.” 46 In therapeutic contexts, one may see scenarios in which TCIM practitioners are working in ways that explicitly align with their therapeutic paradigms, often in parallel or loose co-ordination with biomedical or other TCIM practitioners. As Ashcroft and Bevir note, however, multiculturalism regimes “aim at accommodating difference without disturbing the status quo.” 47 In other words, Biomedicine’s mechanistic ontology and its associated professional norms would still be constituted as the normative therapeutic paradigm in multiculturalist contexts. Vitalistically inclined TCIM practitioners may be granted certain concessions to work explicitly in line with their knowledge paradigms but might only be permitted to practice following referrals from gatekeeping biomedical physicians, or be denied the reimbursement or other institutional privileges granted to biomedical providers. Furthermore, conceptually speaking, multiculturalism “involves a notion of cultural authenticity rooted in purity…[that] views cultures as separate and timeless traditions.” 46 As such, there is not usually a strong effort to “merge” multiple therapeutic paradigms in multiculturalist contexts, but rather to have them coexisting in parallel.
Nevertheless, there may also be multiculturalist contexts of therapeutic integration whose gravitational centers rise up along with the spectrum shown in Figure 2, in the direction of Integrative Equity. Some examples might include therapeutic settings in which traditional medicine practitioners and their therapeutic approaches are the predominant form of care, with biomedical professionals being called on as support-personnel, or biomedical diagnostic techniques (e.g., x-ray, blood work, CT scan) being employed as an adjunct. Alternatively, a biomedically dominant treatment context in which the principles of holism and salutogenesis are centralized may also provide more equitable (intercultural/culturally safe) conditions in which biomedical and nonbiomedical clinicians may offer care consistent with their own paradigms, without changing the overall character of their respective work or the care context as a whole.
Transculturation
As Lull explains, 48 transculturation “refers to a process whereby cultural forms literally move through time and space where they interact with other cultural forms and settings, influence each other, produce new forms, and change the cultural settings.” In contrast to multiculturalism, culture is treated in transcultural contexts as dynamic and permeable (rather than fixed and bounded), creating space for the emergence of new therapeutic meta-theories, practices, and transformed therapeutic cultures. However, as Rogers observes, new or emerging cultural forms remain situated within, and informed by the dynamics of “unequal power of cultural dominance and exploitation” evident within broader sociopolitical contexts, including “globalization, neocolonialism, and the increasing dominance of transnational capitalism vis-à-vis nation states.”
The concept of “whole health” as described in a 2023 report of the U.S. National Academies of Medicine, and as implemented across parts of that country’s Veterans’ Administration, offers a tangible example of therapeutic transculturation. 49 As the report indicates, its holistic, salutogenic vision of whole health is:
intended to shift the focus from a reactive disease-oriented
Also integral within the whole health vision are “improvements in the social and structural determinants of health,” such as “poverty…structural racism and oppression, gender bias…access to healthy food and having a place to live.” These factors are constituted as “the true reasons for health inequities,” which cannot be redressed through individual-level medical care alone. Furthermore, central to the whole health model is that it “integrates evidence-based conventional medical care with complementary and integrative health.” Ultimately, the shift to a whole health care model is described in the National Academies report as a form of “cultural transformation.”
The whole health model, as implemented within the U.S. Veteran’s Administration, may be understood as representing a transcultural shift “upward” along with the integration spectrum. Here, integration’s gravitational center shifts upward as principles of holism and salutogenesis become centralized over what the National Academies report terms “the reductionist biomedical model” and its “reactive disease-oriented medical care system.” The model’s interculturality is also evidenced by its inclusion of “complementary and integrative therapies” (such as “acupuncture, biofeedback, clinical hypnosis, guided imagery, massage therapy, meditation, Tai Chi/qigong, and yoga”) as central therapeutic elements along with biomedical care.
Paradigmatically speaking, despite its holism and salutogenic focus on health’s social and structural determinants, the National Academies report remains substantially anthropocentric in its vision of health. While “air pollution” and “clean water” are addressed in the report, as are “safe built and natural environments,” these are primarily constituted with reference to human well-being alone, rather than planetary health more broadly. Furthermore, the report substantially constitutes nonbiomedical therapeutic approaches as “complementary and integrative modalities” rather than as whole medical systems or therapeutic paradigms in their own right. It is made clear in a single passage that the report’s authors are aware that “complementary and integrative health…embrac[es] more holistic, complementary concepts and methods whose theory and practice may not be part of traditional western biomedicine.” On the one hand, practitioners working from within nonbiomedical, vitalistic paradigms may be warmly welcomed in “whole health care” contexts. But, the lengthy (and heavily conceptual) report does not explicitly recognize the conceptual contributions of nonbiomedical knowledges to the whole health model, ultimately weighing that model toward a holistic, salutogenic gravitational center underpinned by biopsychosocial Biomedicine’s underlying mechanistic ontology. In this way, this example clearly illustrates the paradigmatic differences between transcultural forms of integration (e.g., the whole health model) and those discussed next, with reference to the Third Space.
Third Space
The Third Space is a theoretical construct introduced by the postcolonial scholar Homi Bhabha to characterize cultural hybridizations enacted within and by marginalized communities that “move beyond the binary dialectic” and its “politics of polarity” to create new, “liberatory” cultural forms. 50 As in transculturation, the Third Space is “based not on the exoticism of multiculturalism or the diversity of cultures” but on a continuous, dynamic interface between them that defies any notion of cultural “purity.” In the Third Space, furthermore, it is not just a synthetic, syncretic blending of cultural elements—both dominant and marginalized—that takes place, but a transformation of the power dynamics that usually accompany them. This is achieved through what Bhabha terms “mimicry,” in which new cultural forms may variously appear, at their surface, to echo dominant cultural discourses. However, these echoes, enacted by—and from the vantage point of—the marginalized, “‘rupture’ the discourse” of dominant power in ways that pose “an immanent threat to both ‘normalized’ knowledges and disciplinary powers.”
Within the context of therapeutic integration, the gravitational center of the Third Space is ecocentric, with strong vitalistic, holistic and salutogenic paradigmatic influences. Here, however, mechanism and vitalism, holism and reductionism, as well as salutogenesis and pathogenesis, may interface in what Indigenous scholar Willie Ermine terms an “ethical space of engagement.” 51 In this ethical “third” space, “disparate worldviews” become reconciled “in a meeting place…a neutral zone” beyond “institutionalized monoculture” and “notions of universality.” 51 Furthermore, one will often see the principle of cultural safety actively enacted within Third Space integration contexts.
The Third Space of therapeutic integration might be evident within Indigenous-led health care partnerships, wherein “health interventions in Indigenous communities are holistic and informed by cultural knowledge or local spiritual worldviews,” but also infused with biomedical therapeutics, 52 as in the U.S. case of the Nuka System of Care, a “Native-owned…health center…serving nearly 65,000 Alaska Native and American Indian people.” 49 There, both “traditional [Indigenous] healing” and “complementary medicine” are not only offered in conjunction with biomedical treatment as integral elements of care 49 but the system’s “operating principles are derived from Alaska Native culture and values.” 53
At times, it may be vitalistically inclined, biomedically trained professionals who engage what Bhabha terms “the innovative energy of the ‘third’ space” to create new therapeutic paradigms. For example, the Sintergética system of integrative therapeutics, developed by the Colombian medical doctor Jorge Carvajal, fuses conceptual and practical elements from Chinese medicine and Ayurveda, Indigenous healing traditions, auriculotherapy, neural therapy, as well as cybernetics and systems science, into a vitalistic, holistic, salutogenic system of bioenergetic therapeutics. 54
Another example might involve the fusion of more than one type of ethnomedical or otherwise vitalistically informed care. One such case involves the British herbalist Jeremy Ross’s application of Chinese medicine principles to the use of European herbs, also informed by data from clinical and pharmacological research. 55 As Ross explains, this synthesis permits the fruitful application of Chinese medicine’s sophisticated diagnostic approaches, while minimizing the ecological impacts of long distance industrial herbal transport, as well as heightening (European) clinicians’ relationality with the medicines they use.
Ultimately, the Third Space of therapeutic integration represents a creative aspirational space of social, epistemic, and ecological justice. Here, therapeutic knowledges and cultures, and those who seek and offer health care, meet as equals, generating new healing knowledges and practices to meet the needs of the present and future, informed by multiple pasts.
Conclusions
This work, the final article in a four part-series presenting a comprehensive operational typology of the TCIM field, advances a novel framework for conceptualizing therapeutic integration along with a spectrum framed by the polarities of Integrative Assimilation to Integrative Equity. Using a critical social science lens informed by insights from political science, and with reference to real-world examples, this framework characterizes five distinct forms of therapeutic integration that account concurrently for issues of paradigm and power. The framework, ultimately, represents the culmination of the typology, synthesizing its conceptual and practical elements. This synthesis takes the work beyond a classification model for individual TCIM approaches, to a framework that brings this range of classified approaches into dialogue with one another, with Biomedicine and beyond.
The conceptually informed operational typology of TCIM detailed in this four-part series1–3 comprises the first scholarly tool of its kind in the field. The typology is transparently elaborated with reference to conceptual parameters informed by WHO indications, as well as critical social scientific perspectives. The typology clarifies how the TCIM construct—often defined by “what it is not” (i.e., Biomedicine)—may be rigorously subdivided into categories that characterize the world’s diverse range of ethnomedical and otherwise subordinated therapeutic approaches in their own right, for “what they are.” This classification model draws close attention to historical, cultural, paradigmatic and health systems considerations at play across the diverse TCIM field. The typology furthermore attends closely to the complex, multidirectional power dynamics that underpin the ongoing hybridizations of diverse therapeutic knowledge systems and practices, as well as the “integrative” interface between them.
For interest holders and knowledge users across multiple sectors, this TCIM typology has the potential to deeply inform research, pedagogy, policy and practice alike. For example, researchers may use the typology to formulate more precise and field-appropriate definitional parameters for scholarly searches, study designs, and analyses, and to select appropriate research designs that fit the paradigmatic and practice features of the TCIM being studied. Educators may draw upon various aspects of the work to support trainees in understanding the TCIM field’s complex historical, cultural, and paradigmatic features, in addition to engaging with the typology’s classification frameworks. Decision makers, in turn, will find in the typology a tool for determining the focus and form of appropriate research evidence to inform TCIM-related policy questions, and a language to support evaluations of existing TCIM health services and structures. Across global contexts characterized by biomedical dominance, the typology may also provide a narrative framework for reframing and more equitably and inclusively representing TCIM therapeutics of many kinds. Ultimately, this work is a resource that may help to consolidate many strands of activity in the TCIM field toward greater health and well-being for people and planet.
Footnotes
Acknowledgments
The author is grateful to Anne Taillefer, to readers of the SSRN preprint, and to the respected journal peer reviewers for their valuable critical feedback and questions on earlier versions of this work. The author would also be remiss not to recognize the fluffy companionship of my ginger cats, and the compassionate guidance of her community of plant beings, through the many phases of this work’s choreography.
Author Disclosure Statement
No interests to disclose.
Funding Information
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Data Availability
No data were generated or collected for the present work.