
Abstract
Background:
The field of Traditional, Complementary, and Integrative Medicine (TCIM), which comprises a vast and diverse range of therapeutic approaches that fall outside of Biomedicine’s standard of care, may be classified with reference to six primary categories, or ideal “types.” These categories, outlined in an operational typology in the second article of this four-part series, are: (A) Orally Transmitted Ethnomedical Systems and Practices; (B) Codified Ethnomedical Systems and Practices; (C) Non-Ethnomedical Whole Systems; (D) Complementary Therapeutics; (E) Community-Based Therapeutics; and, (F) Integrative Therapeutics.
Overview:
The current article, the third of the series, uses a series of tangible examples to support users in understanding how to classify specific TCIM therapeutics within Types A through E, within larger health systems contexts. Using three complex TCIM examples briefly introduced in the previous article—a product (turmeric), a practice (acupuncture), and a practitioner group (birthworkers)—this work shows how a particular therapeutic approach may, under distinct circumstances, fall within the boundaries of multiple TCIM types. This illustration highlights how the typology’s categories are permeable and dynamic, rather than closed and fixed—and how contextual factors within health systems are essential considerations in the typology’s application.
Keywords
Preamble
This is the third article in a four-part series that presents the conceptual foundations (article 1) 1 of an operational typology of the diverse field of Traditional, Complementary, and Integrative Medicine (TCIM) (article 2), 2 along with a detailed discussion of the typology’s applications (articles 3 and 4). 3 Operational typologies offer theoretically informed classification systems for making sense of complex domains using a series of “ideal types.” The sixfold typology presented in the previous article 2 is theoretically built upon a detailed analysis of TCIM-related definitions from the World Health Organization (WHO), which continues to call for TCIM knowledges, practitioners, practices, and products to be better incorporated within national health systems worldwide. The current article offers a more detailed account of how to use the typology as a classification tool, with reference to its first five types, and three key examples illustrated across them. These examples, of a TCIM product (turmeric), practice (acupuncture), and practitioner group (birthworkers), both illustrate TCIM field’s complexity and show how the typology may be used to bring clarity to that complexity. The final article in the series discusses in greater depth the sixth type—Integrative Therapeutics—advancing a conceptual model for understanding the interface between different TCIM approaches, as well as Biomedicine, 1 within and across communities and health systems.
Overview: Applying an Operational Typology of TCIM
The TCIM field is complex, encompassing a diverse set of ethnomedical and nonethnomedical therapeutic systems, knowledges, practices, products, and devices that fall outside of the boundaries of Biomedicine’s standard of care in particular contexts. In two previous articles,1,2 the author has introduced an operational typology of TCIM: a classification system offering conceptual tools to delineate between TCIM therapeutics of various kinds according to their primary characteristics. The typology’s six categories, shown in Figure 1 and summarized in Table 1 (along with their subtypes), are: (A) Orally Transmitted Ethnomedical Systems and Practices, (B) Codified Ethnomedical Systems and Practices, (C) Non-Ethnomedical Whole Systems, (D) Complementary Therapeutics, (E) Community-Based Therapeutics, and (F) Integrative Therapeutics. The typology is meant for use by a wide range of knowledge users—including educators and trainees, researchers, health care practitioners, decision makers, and community members—who may use the typology to better differentiate between the ranges of TCIM approaches relevant to their work. Whether in pedagogy, policy making, program planning, research design, or clinical interactions, a clear understanding of the TCIM approaches at play, and a common language with which to communicate about them, is essential.
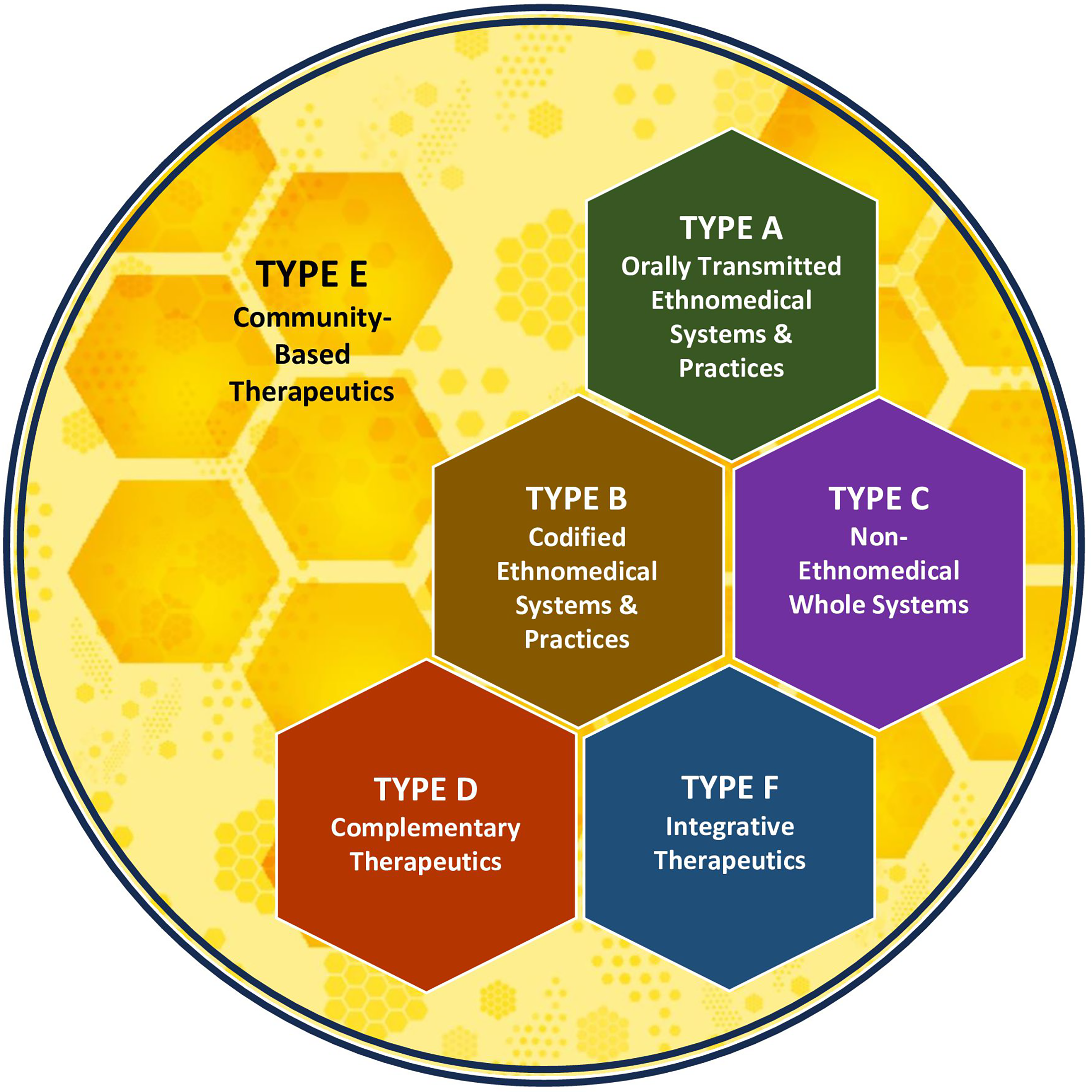
This figure provides a graphical overview of the six primary types in an operational typology of Traditional, Complementary, and Integrative Medicine.
Overview of Types and Subtypes in an Operational Typology of Traditional, Complementary, and Integrative Medicine
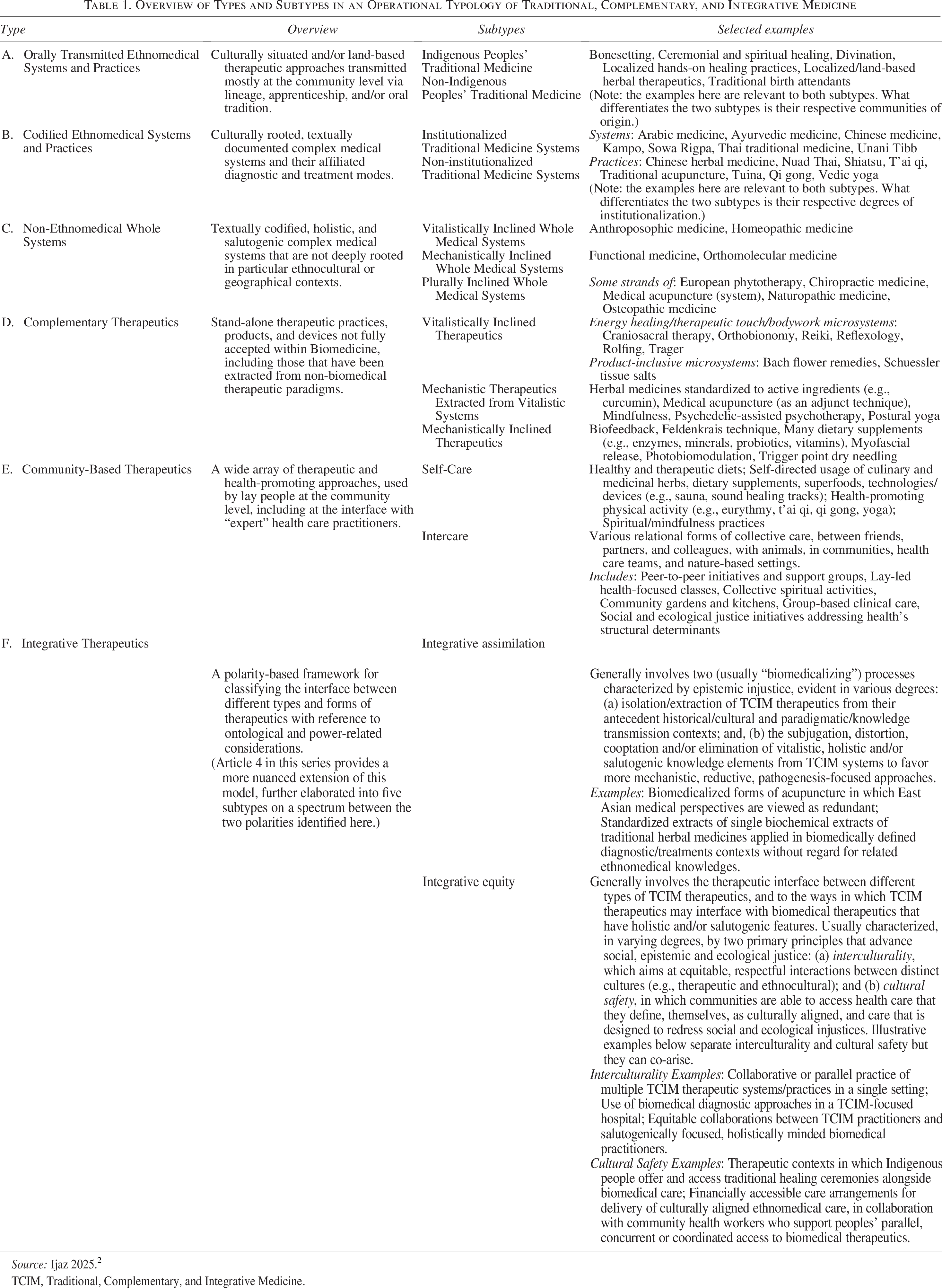
Source: Ijaz 2025. 2
TCIM, Traditional, Complementary, and Integrative Medicine.
The TCIM typology, designed to be used across global contexts, is “built with reference to four primary conceptual domains, which reflect the theoretical underpinnings of the WHO’s TCIM-focused definitions, and related critical social science scholarship.” 2 These four domains are: (1) Historical Factors, (2) Paradigmatic and Cultural Features, (3) Knowledge Transmission Modes, and (4) Health Systems Contexts. The second article in this series makes explicit how the first three of these domains inform the typology’s design. 2 The importance of the fourth domain, Health Systems Contexts, which addresses the “structural considerations that inform the ways in which health care is delivered and received around the world”, 2 is addressed in more detail in the current and next articles. 3
This domain, Health Systems Contexts, is important because it takes into account the diverse systems, settings, and cultures of health and health care that are evident globally—and the roles that TCIM therapeutics may play across these contexts. It is important because a form of care constituted as TCIM in one context (e.g., midwifery, particular dietary supplements) may have become part of Biomedicine in another. It is also important because the particular forms of TCIM that are culturally sanctioned and practiced within communities and health care facilities in a particular bioregion, village, town or city, health care governance authority, country, or region will vary notably. Finally, it is important because the ways in which TCIM therapeutics will interface with one another, and with biomedical care, take many different forms, reflecting a range of power dynamics that influence how people and communities deliver, experience, and receive care within larger ecosystems.
The TCIM typology presented in this series has a primary (and somewhat unusual) design feature that allows it to be flexibly applied with reference to the important considerations raised above. As explained in the second article in this series, 2 many operational typologies are based on “Eurocentric intellectual logics” that imagine typological categories as discrete, mutually exclusive, fixed boxes. However, this TCIM typology is designed to have “permeable and interconnected” categories, reflecting the blurring of discrete categories that is often evident in “epistemologies of the South” (from which many TCIM therapeutic approaches originate). This design approach recognizes that particular therapeutic systems, knowledges, and practices may dynamically occupy multiple spaces within the typology—at different temporal moments, in distinct contexts, and in the various forms they take. 2
It may be tempting to try to use the TCIM typology to unequivocally classify a specific TCIM approach within a specific type or subtype. But this is not the typology’s purpose and does not reflect the reality of therapeutics around the world or through history. Of course, as a classification tool, the typology is designed to help situate particular TCIM approaches within specific types and subtypes within particular contexts, at particular moments in time, and for particular purposes. However, users are invited to resist the temptation to intellectually “crystallize” or “universalize” their classification efforts as though these were uncontestable or unchanging. They are not.
Like culture, like language, the world of therapeutics is constantly changing, hybridizing, transforming, and transmuting. No doubt many typology users may find themselves in a position in which their work—for example, a research project, or a policy undertaking—requires that they (provisionally) treat particular TCIM approaches as static, fixed entities. This in itself is not a problem—and producing classifications for such applications is a major part of the typology’s intended purpose. However, to adhere to the spirit of the typology’s design, users would best keep in mind that when they use the typology in this way, that in another context, the classifications that seem to make sense in one setting or temporal moment may not always or necessarily apply.
With these considerations in mind, this article walks readers through some illustrative examples of how the typology may be appropriately applied. These examples—referring to a TCIM practice (acupuncture), product (turmeric), and practitioner group (birthworkers)—were initially introduced in the previous article with respect to Type F, integrative therapeutics. Here, however, the emphasis is on showing how each of the aforementioned may—under different circumstances—be classified under all of the typology’s first five types (A through E). The purpose of these examples is to reinforce to readers that it is essential to consider the specific context of a use of a particular TCIM approach, along with its paradigmatic features, to classify it appropriately using this typology.
Using the TCIM Typology’s Classification Model
The operational typology presented in the second article in this series 2 provides a detailed overview of six “ideal types” into which TCIM therapeutic approaches (whether alone or in combination) may be classified (see Fig. 1 and Table 1). Each of those types includes at least two (and in some cases three) subtypes, which identify and disambiguate functionally distinct subcategories within the larger type. The first four categories, Types A through D, elaborated further in the subsection Applying types A through D: Practices, practitioners, and products, may be contemplated as a “bundle” united by their emphasis on elements of TCIM care typically linked to the construct of “expert” (rather than community-based) usage in particular therapeutic domains, communities, or health-related (eco)systems. Types E and F are qualitatively different from Types A through D in that they refer to broader “spheres” of care. In other words, whereas Types A through D substantially refer to care delivered one-on-one or in small groups, Types E and F, by contrast, more broadly encompass forms of health-related care offered, experienced, and shared at the level of the individual or group, within communities or health care settings, and/or across health (eco)systems more broadly. Yet, Types E and F remain deeply interconnected with the first four and, as discussed in the subsections Applying Type E: Community-Based Therapeutics (Type E) and the next article (Type F), 3 respectively, cannot be appropriately understood without close reference to them.
Before turning to a more detailed account of how the typology’s classification model may be tangibly applied, readers may note that the typology’s graphical representations show both a vertical and horizontal structure and a multilayered dimensionality. In Figure 1, one may observe from top to bottom a progressively increasing alignment with biomedical epistemic premises and evidentiary norms, as well as an increasing adherence to professionalization norms (i.e., standardization, institutionalization, professional regulation) rooted in 19th-century Europe. From bottom to top, one may conversely observe an increasing commitment to retaining therapeutic knowledges and practices within the “commons” or public domain rather than engaging them within capitalistic intellectual property claims (including those affiliated with product patents as well as professional licensure), an increasing alignment with vitalistic (rather than mechanistic) epistemic premises, as well, in some cases, as a heightened attention to matters of spirituality. Horizontally in the typology’s second “tier”, one sees structural similarities between two different types (B and C) of complex medical systems (ethnomedical and nonethnomedical), which demonstrate a higher degree of textual codification, internal standardization, and institutionalization than those approaches in the top tier.
Applying Types A through D: Practices, practitioners, and products
In its 2014–2023 Traditional Medicine Strategy, the WHO draws attention to three elements of TCIM that warrant careful consideration with reference to health systems contexts: “products, practices and practitioners.” 8 This work’s typology, in addition to having the capacity to classify diverse TCIM systems and microsystems, is useful for classifying forms of TCIM across all three of these health systems-relevant elements. Before turning to some illustrative cases that will support typology users in better using the classification system, some brief notes about the typology’s first four types are warranted. As detailed in the previous article, each of these types has distinct associated historical factors, paradigmatic and cultural features, and knowledge transmission modes. That said, the four also have characteristics in common with one another.
Overall, Types A, B, and C characterize complex medical systems distinct from Biomedicine (along with their affiliated core practices). Types A and B both address ethnomedical systems, but are differentiated by their respective primary associated modes of knowledge transmission (i.e., oral [type A] vs. textual [type B]). Types B and C, in turn, similarly include textually transmitted complex medical systems, with the two types differentiated by their predominant connectedness with ethnomedical lineages (type B) or not (type C). Type D is qualitatively different from the first three types (in that it does not address complex medical systems), but it is not entirely distinct from those types either. While Type D primarily characterizes standalone therapeutic products, practices, and devices used primarily as clinical adjuncts delinked from complex systems, it also includes therapeutic ‘microsystems'. Such microsystems share some characteristics with the complex systems of Types A through C, but have a narrower, more circumscribed focus on a specific bodily or health-related domain rather than on health care more broadly. Furthermore, many Type D therapeutics have historical antecedents in Types A, B, and C systems, but have been separated from their antecedent epistemologies and cultural contexts of origin and subsequently reframed in biomedicalizing terms.
The previous article in this series provides detailed examples of each of the four aforementioned Types (and their subtypes), 2 as does Table 1. Readers are, however, reminded that what ultimately determines the appropriate typological classification of a particular TCIM approach or element are its characteristic features in a particular context. Thus, the examples provided may not universally hold across all contexts. To support readers in applying the typology as a classification tool in their work, the following series of questions (listed below, and depicted, with color-coding, in Fig. 2) will prove helpful:
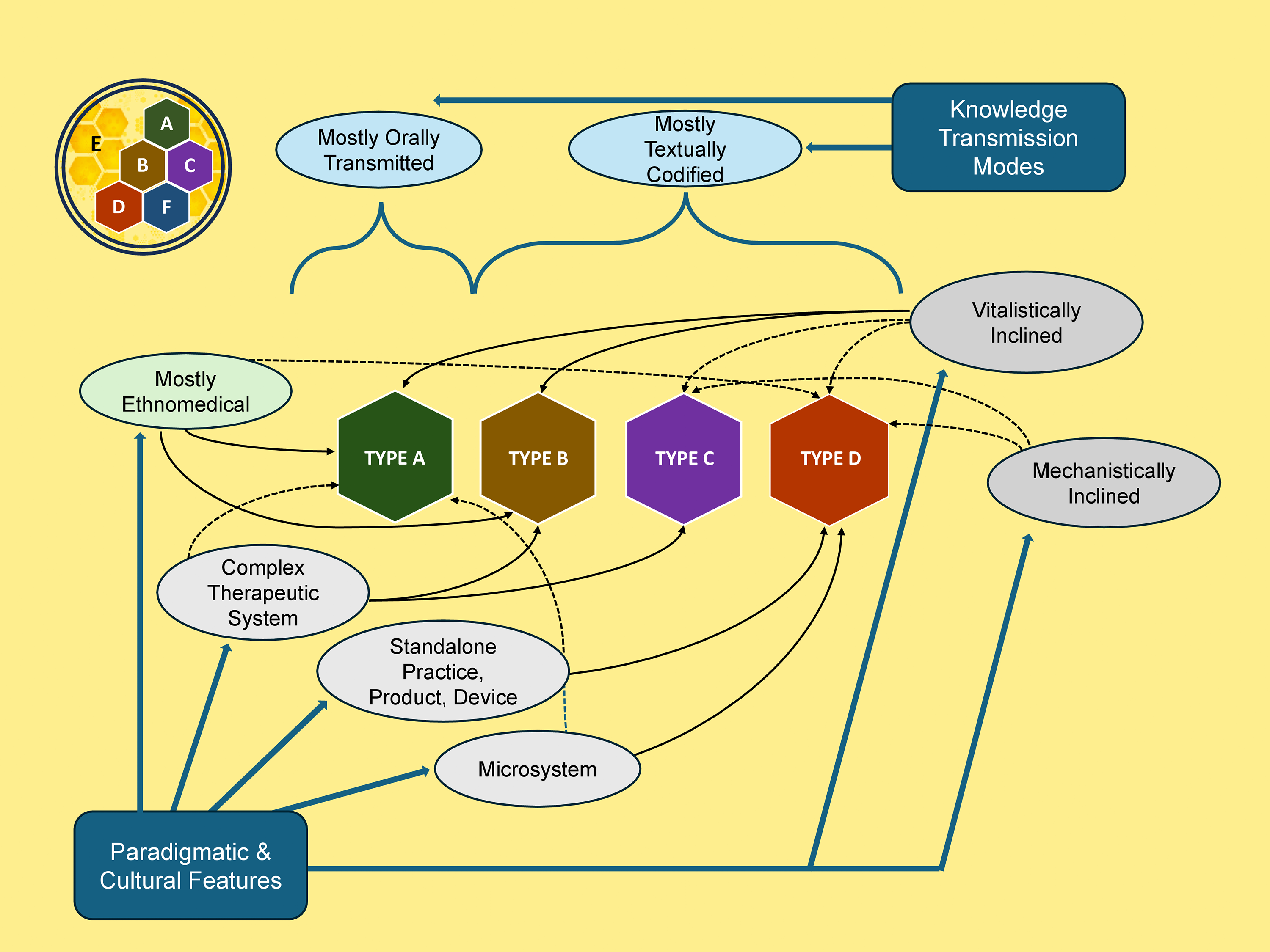
Flowchart for applying an operational typology of Traditional, Complementary, and Integrative Medicine. Type A: Orally Transmitted Ethnomedical Systems & Practices. Type B: Codified Ethnomedical Systems & Practices. Type C: Non-Ethnomedical Whole System. Type D: Complementary Therapeutics. Type E: Community-Based Therapeutics. Type F: Integrative Therapeutics.
[Blue]: Is the TCIM approach or element mostly orally transmitted or mostly codified in textual sources?
[Green]: Is the TCIM approach or element predominantly ethnomedical in origin?
[White]: Is the TCIM approach or element (or is it being practiced within the boundaries of) a complete “whole” medical system, or is it instead a microsystem, stand-alone practice, product, or device?
[Gray]: Is it rooted in and/or practiced from a vitalistic or mechanistic paradigmatic standpoint, or both?
These four questions, taken together, will assist the user in discerning where to position a given therapeutic system or element across Types A through D. At times, however, classifications may not be straightforward, owing to context-specific factors within a particular community or health system, and to the hybridizations of therapeutic approaches that continue to take place over time. Sometimes, an approach may straddle more than one category. Or, what may appear at the surface to be a single therapeutic product, practice, or practitioner community may occupy multiple types and/or subtypes depending on contextual factors. The sections that follow illustrate, with reference to globally important examples of TCIM products, practices, and practitioners, how the answers to the four aforementioned questions will support typological classification efforts. Furthermore, the same three cases are again explored with reference to Type E, Community-Based Therapeutics.
Case 1 (products): Turmeric
Turmeric (Curcuma longa) has a multimillennial history of culinary, spiritual, and ethnomedical applications across South and East Asia. 9 The plant’s famed rhizome has also, in various forms, entered the treatment toolkits of a range of nonethnomedical practitioner groups in recent decades. Here, the typology’s first four Types permit a nuanced (though provisional) differentiation of turmeric’s diverse applications and forms as a TCIM product.
Under Type A, Orally-Transmitted Ethnomedical Systems and Practice, one may find diverse therapeutic and spiritually focused preparations of the rhizome (whether fresh or dried, alone or in combination with other ingredients, for topical or internal usage) offered by traditional and Indigenous healers based on vitalistic family and community knowledge lineages.
Classified under Type B, Codified Ethnomedical Systems and Practices, one may find a similar span of turmeric usages, for a wide range of health conditions, perhaps extended to include some industrially produced concentrates of the whole rhizome. These might be variously but, from a paradigmatic standpoint, vitalistically applied with reference to textually documented diagnostic and therapeutic parameters, within such ethnomedical systems as Ayurvedic, Chinese, Siddha, and Unani medicine.
The same rhizome, in some of the same forms as described above but increasingly frequently in commercially prepared forms, might be recommended by practitioners of some non-ethnomedical whole systems such as naturopathic or functional medicine (Type C). More vitalistically inclined clinicians may be more likely to use the whole (dried, or occasionally fresh) rhizome or extracts of the whole plant in pill form, either for particular ‘energetic’ applications or with reference to biomedical diagnoses. Such applications might be informed by traditional ethnomedical as well as biomedical evidentiary indications. Practitioners more mechanistically inclined may be more likely to use commercial turmeric extracts over the dried plant powder, may show a preference to extracts of the rhizome standardized to include specific proportions of particular biochemical constituents (e.g., curcumin) or isolated extracts (plant-based or synthetic) of curcumin alone. On the whole, one might expect these mechanistic usages to refer to particular biomedical diagnostic categories (e.g., rheumatoid arthritis) and/or peer-reviewed research evidence.
Under Type D’s second subtype (Complementary Therapeutics: Mechanistic Therapeutics Extracted from Vitalistic Systems), one may find commercially prepared forms of turmeric (including but not limited to standardized and isolated extracts), and to a lesser degree, the dried powdered rhizome, used as an adjunct treatment, often with reference to biomedical diagnostic categories or peer-reviewed research evidence.
Case 2 (practices): Acupuncture
According to WHO survey data, acupuncture is the “most common form of [TCIM] practice” reported around the world, reported to be used in 85% of member states. 10 However, as a TCIM practice, there is no singular ‘acupuncture’. As with turmeric, different forms of acupuncture may be classified in each of Types A through D, and across multiple subtypes.
Under Type A, Orally-Transmitted Ethnomedical Systems and Practice, one may find (predominantly vitalistic) forms of acupuncture that continue to be primarily orally transmitted (whether, for example, as an element of the Mesoamerican Indigenous medicine system of the Mayan People on the Yucatán peninsula 11 [subtype 1, Indigenous Peoples’ Traditional Medicine], or through ethnomedical family lineages in Eastern Asia [subtype 2, Non-Indigenous Peoples’ Traditional Medicine]. 12
Better classified under Type B, Codified Ethnomedical Systems and Practices, would be (predominantly vitalistic) forms of acupuncture practised as part of a codified ethnomedical system such as traditional Chinese medicine (TCM), traditional Korean medicine, or Kampo medicine, whether inside or outside of East Asia.
Within Type C, Non-Ethnomedical Whole Systems, one may find acupuncture being practiced within a plurally inclined, non-ethnomedical system, whether vitalistically or mechanistically, as one among multiple therapeutic modes or as a system’s primary therapeutic approach. In Canada, for example, acupuncture is taught at professional schools of naturopathic medicine (with reference to both East Asian and biomedical concepts), and statutorily included within that occupation’s practice scope in multiple provinces. However, owing to the epistemic diversity within the naturopathic occupation, 13 clinicians may variously engage the practice with reference to vitalistic and/or mechanistic principles. Then, there is the ‘medical acupuncture’ system developed by medical doctor Joseph Wong,14–16 predicated upon biomedical (‘neuroanatomical’) concepts, but also explicitly informed by (vitalistic, ethnomedical) theoretical and practical elements from TCM. Wong himself vitalistically indicated that “the great concepts of TCM are still the most important parts of acupuncture.” 14 However, there may be many biomedical clinicians (to whom Wong’s work was primarily directed) who use Wong’s technical indications to perform acupuncture predominantly from a mechanistic ('neuroanatomical') standpoint, despite Wong’s own “emphasi[s] that no one should practice acupuncture without a good understanding of TCM.” 14
Furthermore, there are forms of acupuncture (typically practiced from a mechanistically inclined stance) that might be best classified under Type D, Complementary Therapeutics. Many such practices have been extracted from East Asian ethnomedical traditions (Subtype: Mechanistic Therapeutics Extracted from Vitalistic Systems) and are employed as an adjunct therapeutic approach by biomedical clinicians (e.g., physicians, chiropractors, physical therapists), often to treat musculoskeletal pain. There are also various acupuncture microsystems (e.g., auriculotherapy), some with antecedents or counterparts in vitalistic Type B systems, used to treat a limited range of conditions (e.g., addictions). Except when used within the context of a Type B system (in which case they might best be classed there), these microsystems and devices, used as adjunct modalities in clinical practice, might be categorized as Type D therapeutics. Finally, some mechanistic forms of acupuncture (like Trigger Point Dry Needling developed by biomedical physician Simons et al., 17 used primarily for musculoskeletal conditions) are rooted in biomedical (rather than ethnomedical) therapeutic innovations (e.g., injections using hypodermic needles) but later adopted acupuncture’s filiform needles. These practices might be classed under Type D, as Mechanistically Inclined Therapeutics.
Case 3 (practitioners): Birth workers
Finally, the case of birth workers provides a salient example of how TCIM practitioners who, at first glance, appear to work in a similar domain may more accurately be categorized across multiple Types. Traditional birth attendants and Indigenous midwives trained primarily through community and family lineages might best be classified under Type A. By contrast, clinicians practicing ethnomedical forms of midwifery within a licensed profession (such as in Thailand, where traditional midwifery forms one element of the state-regulated system of Thai traditional medicine, which relies on institutional training programs), might be better classified under Type B. Elsewhere, one may see occupations of midwifery predicated on biomedical knowledges but also informed by contemporary feminist epistemologies and variously influenced, in practice, by ethnomedical birth work. In some countries (such as the United States), some midwives (and in particular, nurse–midwives) have become established members of national health systems, practice from a predominantly biomedical standpoint, and would thus not be constituted as TCIM practitioners (and fall outside of this typology’s scope). Conversely, also in the United States, there exist in some states licensed “direct-entry” midwives who “do not carry nursing credentials” but are statutorily authorized to “attend births outside of hospital settings.” 18 Because their work falls substantially outside of Biomedicine’s boundaries, the latter midwives might be understood as TCIM practitioners, working within a mechanistically inclined Type D system.
Synthetic considerations
Overall, it is thus clear that no TCIM system or microsystem, practice, product, or practitioner community should be statically or unequivocally classified within a particular Type or subtype without careful examination of its distinct and contextual characteristics. This point has important implications for research and governance. Indeed, the nuances described above make evident how research undertakings (e.g., systematic reviews) that group together diverse forms of what might appear, at its face, to be a singular TCIM approach (e.g., turmeric, acupuncture, midwifery), may fall short in adhering to rigorous conceptual standards in scholarship. Similarly, decision makers might do well to attend carefully to the distinctions between different forms of related TCIM approaches in designing and evaluating policy interventions and frameworks. Certainly, these issues and their ramifications warrant additional investigation, which falls beyond the current article’s scope. Nevertheless, the typology’s utility in pointing to the distinctive features of distinct TCIM approaches may serve as a conceptual basis for such work.
Applying Type E: Community-Based Therapeutics
As explained in the previous article, Type E, Community-Based Therapeutics, is the broadest and most inclusive category in this typology, “encompass[ing] but extend[ing] beyond the other types, a zone of interface between the other types, and ultimately as an overarching backdrop within which the other types are housed.” Furthermore, Type E “represents a domain of health democratization, illustrating lay people’s autonomous capacity to engage, with and/or without “expert” inputs, the therapeutic knowledges and practices that address their needs and preferences.” This may include forms of health-seeking ‘Self-Care’ (Type E’s first subtype), as well as the ‘Intercare’ (the second subtype) that takes place between and among people, synergistically with other living organisms, and across health systems and ecosystems more broadly. As Figure 3 shows, the knowledge, practices, and interactions that permeate Community-Based Therapeutics flow in a multidirectional manner between and within all other TCIM types.

The fluid interface of Community-Based Therapeutics in an operational typology of Traditional, Complementary, and Integrative Medicine.
Critically, the spheres of ‘expert’ care described in Types A through D are symbiotically infused with and shaped by the broader community-based contexts in which they are offered. What people do to care for their health alone and together in their homes and communities, in relation to the ecosystems with which they interface, and how they specifically go about doing these things in culturally specified ways, represents an integral dimension of health systems. What is considered acceptable and healthful in a particular community or culture, and how people view life and understand and work to create health, fundamentally informs what kinds of ‘expert’ care people will seek out, accept, and adhere to, even under dire circumstances.
Ethnomedical traditions, which arise transparently from cultural and land-based contexts, make visible the uncontestable relations between health care, culture, and ecosystems. But these relations are also evident for all forms of ‘expert’ care, including Biomedicine, which (as discussed in the previous articles)1,2 is, like all complex medical systems, historically and culturally situated. In turn, the ‘expert’ care offered within communities and health care institutions infuses the communities themselves, in fluid and reciprocating ways. Unfortunately, however, these points are too often ignored by health system decision makers. This has been explicitly recognized by the Lancet Commission on Culture and Health, which finds that “the systematic neglect of culture in health [is] the single biggest barrier to advancement of the highest attainable standard of health worldwide.” 19
Furthermore, the hybridization of knowledges and practices that takes place across the Community Based Therapeutics type should not be overlooked. Within their homes and communities, lay people may elect to draw on multiple different therapeutic knowledge systems (and practices) to address their health- and wellness-related needs in ways that suit them. This may take place in ways that do not align singularly with the constructs of any one therapeutic or cultural system. This has been elsewhere described as “a citizenry actively combining medical knowledge bases and building plural health care traditions.” 20 In turn, as this same citizenry interfaces with health care practitioners and health care institutions serving their communities, these hybrid therapeutics become further complexified. Here, the issues of power addressed more explicitly in Type F, Integrative Therapeutics, become more evident.
It should be noted that the privileging of ‘expert’ perspectives (and in particular those biomedical) over the voices of ‘patients’ and communities can represent “a form of epistemic injustice.” 21 In such contexts, health-related choices that do not align with biomedical ontologies may be “pathologized” within biomedical health systems and even prosecuted by the state. As Gray and Brunger show, issues of culture (rather than ‘clinical’ considerations alone) typically underpin such complex medicolegal cases. 22 Drawing on the emancipatory critical pedagogical principles of Paulo Freire, which call for the “flattening of hierarchies” between distinct knowledges, Thomas and colleagues have argued that shared decision-making may be deployed as a strategy for advancing epistemic justice in health care contexts. 21 However, shared decision-making is not always implemented in a manner that prevents epistemic injustice, which optimally requires attention to “culture, justice and power” on the part of health care professionals. Nevertheless, some countries (such as Brazil, with its National Policy on Popular Education in Health) have made advances in designing policies in which community-based, “popular health practices” such as “reiki therapy, auriculotherapy, massage therapy, meditation, [I]ndigenous and traditional medicine practices, among others,” have been incorporated into public health care systems. 23
With reference to the same three cases (turmeric, acupuncture, birth workers) discussed in the subsection Applying Types A through D: Practices, practitioners, and products, the place of Type E, Community-Based Therapeutics (and its two subtypes, Self-Care, and Intercare), within health systems becomes evident.
Case 1 (products): Turmeric
Turmeric (Curcuma longa) is a plant whose diverse usages vividly illustrate the blurred boundaries between what constitutes “medicine” as compared with “food”; turmeric, of course, is both. In addition to the range of “expert” therapeutic applications described in a previous section, turmeric is widely used, all over the world, as a culinary spice and as a home remedy alike. Given that governments around the world do not generally classify turmeric as a restricted medicinal substance, turmeric is widely accessible, in various forms, across consumer marketplaces.
Whether as a deliberate form of therapeutic self-care (including preventive efforts) and/or as a matter of culinary preference, turmeric is an ingredient used to season meals in countless households across the globe each day. This includes meals in communities where turmeric represents a long-standing, culturally specified ingredient, and in meals prepared by “cultural outsiders.” In many (or perhaps most) cases, more than one household member might partake in such meals, reinforcing the collective nature of Community-Based Care, constituted in this typology as ‘Intercare.’ Consumed in various culinary forms, turmeric’s effects may best be understood as ‘salutogenic’ (i.e., health-promoting, preventive, and palliative) rather than strictly ‘pathogenic’ (meant exclusively to ‘cure’ ailments), although the former category is inclusive of the latter.
Turmeric markets around the world represent a multibillion-dollar industry. That industry showed notable signs of growth in response to the COVID-19 pandemic, during which turmeric’s therapeutic attributes made the plant (whether as a culinary spice or as a dietary supplement product) increasingly sought-after around the world.24,25 During that pandemic, in India, the largest global turmeric producer, 25 the government agency (“Ministry of AYUSH”) responsible for traditional medicine issued a National Clinical Management Protocol based on Ayurveda and Yoga for Management of COVID-19. 26 This protocol, which included self-care measures to support immunity within the general public, recommended nightly consumption of “Golden Milk”, a culturally familiar preparation of milk with turmeric powder, as well as a preventive “gargle” of “warm water…with a pinch of turmeric and salt.” 26 Here, one sees how, in the sphere of Community-Based Care, large-scale institutional interventions may interface with Self-Care and Intercare at the household level.
Survey-based data collected in 2020 by India’s Ministry of AYUSH, involving over 700,000 participants, showed that “turmeric milk” was one of the most commonly used community-based TCIM therapeutic interventions across the country during the pandemic. 27 As the authors of that study note, many TCIM measures used by members of the public in India are “either traditional formulations with centuries of use in the maintenance of health or home remedies and are an integral part of Indian culture and cuisine…passed on from generation to generation.” In some cases, such Community-Based Care measures are “used across India irrespective of sociocultural, religious, and geographical differences.” Elsewhere, however, as in one Ethiopian study, turmeric was not among the most commonly used medicinal plants preventively consumed by members of the public during the COVID-19 pandemic. Rather, illustrating the culturally specified, highly local nature of Community-Based Care, it was garlic, ginger, garden cress, and a plant locally known as “Damakase” that were predominantly used, in most cases harvested from “the home garden.” 28
Case 2 (practices): Acupuncture
Unlike turmeric, which is widely accessible for use by members of the public across many global marketplaces, acupuncture is a practice that, in many jurisdictions, is restricted by law to use by statutorily licensed health care professionals. Regardless of its legal status, acupuncture is often offered as a one-on-one private treatment. Here, the importance of the practitioner–patient relationship, as a form of Intercare with therapeutic implications, should not be underemphasized. As with many TCIM therapeutics, the sphere of the practitioner–patient interface is being increasingly documented in clinical research with reference to the concept of “nonspecific effects.” 29 Such ‘nonspecific effects’ refer to the range of therapeutic impacts of acupuncture care that extend beyond the ‘specific’ effects of the needles inserted. But importantly, acupuncture is also a practice with iterations beyond one-on-one private treatments that provide further indications as to how Community-Based Care may be understood within health systems contexts.
In the United States, for example, where professional licensure takes place on a state-by-state basis, some licensed acupuncturists elect to work not within a ‘private room’ context in which each patient is seen individually but in a ‘group’ setting.30,31 Sometimes referred to as ‘Community Acupuncture’ or ‘group acupuncture', such treatment contexts permit cost savings to the patient paying out of pocket for treatments (who may be more able to afford regular treatments at reduced ‘group’ rates). Especially in ‘working class’ communities, in the larger U.S. national context wherein acupuncturists are not generally reimbursed by government insurance plans and the prospect of sustainable livelihood remains tenuous, 18 such group-based treatment models may also offer modest income advantages for practitioners. Furthermore, as Rohleder (founder of the U.S. ‘community acupuncture’ movement) asserts, the group-based setting—in which multiple patients receive care together in a quiet ‘living room’ environment—can confer relational advantages, with the collective ‘Intercare’ context constituting a ‘refuge’ with its own therapeutic benefits.30,31
There are also instances of group-based acupuncture, including but not limited to jurisdictions with acupuncture licensing laws, where it is community members themselves (rather than licensed practitioners alone) who offer forms of acupuncture care. This can involve auricular (ear) acupuncture “microsystems”, such as the “5-needle protocol (5NP),” often used to address “mental health conditions, addictions, pain, and trauma.” 18 In 14 U.S. states, for example, “statutory provisions … permit lay persons with defined training to perform the 5NP, usually under the supervision of a licensed acupuncturist or a medical doctor.” 18 Parallel arrangements are evident across multiple countries, including among Kenyan refugees in Uganda, 32 and among displaced persons in post-earthquake Haitian communities. 33 In such settings, community members working as volunteers may use acupuncture needles, and/or seeds (such as mustard seeds, used in lieu of needles) to deliver auricular treatments to adults and children alike. Across such contexts, such Intercare, offered by community members, supports access to acupuncture care in culturally acceptable ways for considerably larger numbers of community members than might have accessed ‘private room’ care.
Case 3 (practitioners): Birth workers
The previous article, and the subsection Applying types A through D: Practices, practitioners, and products, elaborated multiple iterations of the so-called “expert” birth work in the context of this typology. Birth work, such as acupuncture and many other forms of TCIM, includes many elements of (so-called ‘nonspecific') care that extend far beyond the ‘technical', physical aspects of stewarding the emergence of infants into the world. In the context of community-based midwifery care, “which contrasts with the institutional approach of hospital midwifery”, the heavy demands for “emotional labor” on midwives have been documented as an “invisible load.” 34 In one Australian study, for example, Indigenous midwives were found to be at risk of burnout from their work as both “cultural brokers and carers.”
With this in mind, it may be recognized that partners, family members, pets, and friends also often play a vital role in birthing care. The hands-on and emotional support offered by such community members can contribute immeasurably to the health and well-being of birthing persons and their children. (Such care, of course, can interface with ‘expert’ care in a range of ways, both supportive and, at times, as giving rise to tensions within the care space).
Appreciating the value of community-based birthing care by ‘lay’ persons can help to complicate (and appropriately so) the very notion of ‘expertise.’ Indeed, persons close to a birthing parent will be local experts with indispensable knowledge and honed skills in caring appropriately for that person, whether in terms of their emotional needs, food and beverage preferences, musical tastes, or otherwise. The value of such ‘invisible labor', often but not exclusively offered by women, should not be underestimated.
In several countries, there is an emerging occupation of “birth doulas” who provide “physical, emotional, and informational support” 35 to birthing persons but are not typically constituted as health professionals by the state. Such doulas may, on one hand, fill gaps left by the absence of expert community members and by other expert birthworkers. In some jurisdictions, health authorities have begun to reimburse birth doula care, in particular for low-income persons (who are often members of marginalized communities).18,36
Nevertheless, as Cancelmo indicates, there remain those “who believe that birth should not be connected to the state in any way, and who want to limit the ways birth is medicalized.” 36 Here, questions of expertise are again rendered complex. In a birthing process, who is most qualified to determine what kinds of care are warranted? Within Biomedicine, the notion of ‘shared decision making’ between health ‘professionals’ and ‘patients’ has become increasingly important, but can often be implemented in ways that (sometimes inadvertently) reinforce biomedical paternalism. 37 Much work remains to explore health democratization’s dimensions with reference to the place of Community-Based Care within health systems.
Synthetic considerations
Community-Based Care, both in the form of Self-care and Intercare, is are vital health systems elements that too often escape attention in research and decision making. These forms of care are often highly localized and culturally specified and can interface closely (though often in poorly documented ways) with the care delivered by those designated as health care experts within particular communities. The effects of community members’ own health-related engagements can ultimately not be separated from the effects of ‘expert’ care that more often form the basis for research and governance. All of these forms of care together constitute and shape the landscape of health systems in a particular context, whose hybrid interface raises complex issues related to expertise and power that may be better understood with reference to the final category in the TCIM typology. That final category, Integrative Therapeutics, and its health systems dimensions, are elaborated in greater depth in the final article in this series. 3
Conclusions
This article, the third in a four-part series, has used three key examples—of a TCIM product (turmeric), practice (acupuncture), and practitioner group (birthworkers)—to show how the first five of six ‘ideal types’ in the author’s operational typology of TCIM may be applied to appropriately classify them. These examples are notable in that each of the identified TCIM approaches may fall, under specific circumstances, within each of the typology’s distinct categories. These examples reinforce two key points. First, the typology’s categories are not meant as ‘fixed boxes’ but as permeable categories meant to account for the contextual features of TCIM therapeutics. Second, and related: in using the typology as a classification tool, it is essential to consider not only the paradigmatic, historical, and cultural features of TCIM therapeutics, as well as their knowledge transmission modes, but also their associated health systems contexts, in characterizing them appropriately. The next and final article in the series brings all of these issues together in a synthetic manner to show how these diverse therapeutic approaches may interface with one another within larger health systems.
Footnotes
Acknowledgments
The author is grateful to Anne Taillefer, to readers of the SSRN preprint, and to the respected journal peer reviewers, for their valuable critical feedback and questions on earlier versions of this work. Jenny Jaeckel provided artistic advice and support on Figures 1 and ![]() , which the author deeply appreciates. The author would also be remiss not to recognize the fluffy companionship of my ginger cats, and the compassionate guidance of her community of plant beings, through the many phases of this work’s choreography.
, which the author deeply appreciates. The author would also be remiss not to recognize the fluffy companionship of my ginger cats, and the compassionate guidance of her community of plant beings, through the many phases of this work’s choreography.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.