
Abstract
Background:
Chronic rhinosinusitis (CRS) is among the most common upper airway inflammatory disorders. Conventional cigarette smoking has been significantly associated with CRS. However, little is known about the association between e-cigarette use and CRS.
Objectives:
To examine the prevalence and patterns of electronic cigarette use among patients with CRS and its association with disease severity.
Design:
This cross-sectional study was conducted at King Saud University Medical City, Saudi Arabia, between January 2023 and December 2024.
Methods:
Patients diagnosed with CRS using computed tomography (CT) scans were interviewed regarding the use of electronic cigarettes after obtaining informed consent. Disease severity was assessed using the Sino-Nasal Outcome Test (SNOT-22) and the Lund–Mackay score. Statistical analysis was performed using SPSS software, with a p-value <0.05 indicating significance.
Results:
A total of 300 patients with CRS were interviewed. The SNOT-22 showed moderate to severe symptom impact, and CT scans revealed severe disease. Electronic cigarette use was reported by 11% of patients (lifetime use), and 4.7% used such cigarettes in the past month. Electronic cigarette use was associated with age, gender, employment status, traditional smoking, nasal septum deviation, and reduced concentration. However, no significant association was found between e-cigarette use and disease severity.
Conclusion:
Frequency of electronic cigarette use is high among patients with CRS. However, e-cigarettes use did not influence the disease severity. Larger longitudinal studies are needed to confirm these findings.
Plain language summary
Chronic rhinosinusitis (CRS) is a long-lasting inflammation of the sinuses that causes symptoms like nasal congestion, facial pressure, and reduced sense of smell. It’s a common condition affecting many people worldwide. Traditional cigarette smoking has been linked to worsening sinus problems, but researchers don’t know much about how using electronic cigarettes (e-cigarettes or vapes) might affect CRS.
This study was done at King Saud University Medical City in Saudi Arabia between January 2023 and December 2024. It included 300 patients diagnosed with CRS using CT scans. They were asked if they used e-cigarettes and how often. The researchers also measured how severe their sinus symptoms were using special scoring systems.
The study found that:
• About 11% of CRS patients had tried e-cigarettes at some point, and nearly 5% had used them in the past month.
• People who used e-cigarettes were more likely to be younger, male, employed, traditional smokers, have a deviated nasal septum, and report trouble concentrating.
• However, using e-cigarettes was not linked to how severe their sinus symptoms were.
In conclusion, while e-cigarette use is relatively common among people with chronic sinus problems, it doesn’t appear to make the condition worse. The researchers recommend larger, long-term studies to better understand how e-cigarette might affect sinus health over time.
Keywords
Introduction
Electronic cigarettes (e-cigarettes) are battery-powered devices that deliver nicotine by heating a solution to produce a vapor (aerosol) inhaled by the user. The solution used in e-cigarettes (e-liquid or e-solution) typically contains nicotine, artificial flavors, solvent carriers (such as vegetable glycerin and propylene glycol), and water. 1 Although e-cigarettes have been promoted as healthier alternatives to traditional tobacco cigarettes, findings in the literature remain controversial.2,3
Chronic rhinosinusitis (CRS) is among the most common upper airway inflammatory disorders. 4 CRS is characterized by the presence of two or more symptoms for over 12 weeks. The first symptom includes nasal congestion, blockage, or nasal discharge (anterior discharge or posterior nasal drip), while the second symptom includes facial pressure/pain or olfactory dysfunction. 5 Diagnosis of CRS is confirmed by nasal endoscopy or imaging studies such as computed tomography (CT) scans. 6 In addition to chronic symptoms, patients with CRS may experience acute exacerbations.
In Saudi Arabia, CRS affects 22.5% of the general population, 7 imposing a substantial socioeconomic burden and significantly affecting quality of life. 8 The term “CRS” encompasses a variety of disorders for which the exact pathophysiology remains incompletely understood. It is believed that interaction between host factors (e.g., genetics) and environmental factors (e.g., allergens and pathogens) alter immune function, initiating CRS. 6
Exposure to dust, animals, and toxic gases, as well as regular cigarette smoking, has been significantly associated with CRS.9,10 However, little is known about the association between e-cigarette use and CRS. A nationwide study in South Korea reported significantly higher odds of CRS among e-cigarette users compared to non-users, suggesting that e-cigarette use may increase the risk of CRS. 11
Since its invention in 2003, e-cigarettes have gained popularity across age groups and demographics. The incidence of e-cigarette use was observed to triple yearly among previous smokers and non-smokers.12,13 A national survey conducted in Saudi Arabia by Algabbani et al. reported e-cigarette use in 2.2% of the general population. 14 While e-cigarettes are marketed as a healthier alternative to conventional smoking, significant levels of toxins and carcinogens, including organic compounds and metals, have been detected in e-cigarette vapor. These include toxins and carcinogens not found in conventional cigarettes. Moreover, potentially hazardous fine and ultrafine particles were detected indoors after e-cigarette use.15,16
The health effects of e-cigarette use remain under investigation. Reported adverse outcomes include tachycardia and increased systolic blood pressure after vaping, acute lipoid pneumonia, asthma exacerbations, and otological and sinonasal issues such as vestibular dysfunction, hearing loss, sinusitis, and allergic rhinitis.17–21 Additionally, neurological effects, including seizures, have been observed even in previously healthy individuals. 20
Tobacco use in Saudi Arabia remains a major public health challenge. According to the Global Burden of Disease 2023 study, smoking accounts for nearly 6% of all deaths and approximately 4% of disability-adjusted life years in the country. 22 National surveys further estimate that approximately one in five Saudi adults are current smokers. 23 These figures highlight the considerable health and economic impact of smoking-related diseases in Saudi Arabia and underscore the importance of evaluating alternative nicotine products such as e-cigarettes. Moreover, nationally representative surveys provide insight into the prevalence of e-cigarette use in Saudi Arabia. The 2019 Global Adult Tobacco Survey (GATS) reported that 0.8% of Saudi adults were current e-cigarette users (1.1% males; 0.4% females). 23 Similarly, the 2022 Global Youth Tobacco Survey found that 5.4% of adolescents aged 13–15 years were current users and 14.4% had ever used e-cigarettes.24,25 These findings highlight the growing concern of e-cigarette use among both adults and youth in Saudi Arabia.
Furthermore, emerging data from Saudi Arabia reinforce the local respiratory impact of e-cigarette use. A recent cross-sectional survey among university students in Madinah found that current e-cigarette users had over twice the odds of self-reported respiratory symptoms (AOR = 2.26; 95% CI: 1.14–4.51), and ever users showed similarly elevated odds (AOR = 2.32; 95% CI: 1.21–4.46), compared to never users, adjusting for confounders including tobacco smoking. 26 Additionally, a national cross-sectional study (Sept 2022–Aug 2023; n = 447) linked e-cigarette use frequency with fatigue, breathlessness, shortness of breath, and particularly asthma-related symptoms (p < 0.05), underscoring respiratory concerns associated with vaping in the Saudi context. 27
To our knowledge, no previous research has investigated e-cigarette use in relation to CRS in Saudi Arabia. Therefore, this study aimed to (1) determine the prevalence and patterns of e-cigarette use among patients with CRS in a tertiary hospital setting, and (2) explore its association with disease severity.
Methods
This cross-sectional study was conducted at King Saud University Medical City in Riyadh, Saudi Arabia, for 24 months from January 2023 to December 2024. The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement. 28 Patients presenting to the otolaryngology clinic with CRS, confirmed by CT scans, were consecutively enrolled. Patients under 18 and those with missing CT scans or Sino-Nasal Outcome Test (SNOT-22) data were excluded.
Inclusion criteria:
Adult patients (⩾18 years) diagnosed with CRS according to EPOS 2020 criteria (symptoms persisting >12 weeks plus confirmatory CT scan findings).
Patients with available SNOT-22 scores and/or Lund–Mackay CT scores.
Patients attending the otolaryngology clinics during the study period (January 2023–December 2024).
Exclusion criteria:
Patients with acute rhinosinusitis, sinonasal tumors, cystic fibrosis, immunodeficiency, or systemic inflammatory conditions (e.g., granulomatosis with polyangiitis, sarcoidosis).
Patients with incomplete clinical or imaging data.
Patients who declined to provide informed consent.
A structured questionnaire was used to gather the following data:
Patient demographics: Age, gender, nationality, level of education, and employment status.
Medical history: Physical activity, aspirin allergy, comorbidities (diabetes mellitus, hypertension, and asthma), immunodeficiency disorders, diagnosis of nasal septum deviation, previous sinonasal surgery, and environmental/occupational exposure to strong odors.
SNOT-22 score: This standardized questionnaire evaluates 22 sinonasal symptoms divided into five categories: nasal complaints, ear or facial discomfort, psychological distress, sleep disturbance, and quality of life. Symptoms are scored from 0 to 5 (0 = no problem; 5 = as bad as it can be). Total scores: 0–10 (minimal impact), 11–40 (mild to moderate impact), 41–70 (moderate to severe impact), 71–110 (severe impact). A validated Arabic version of the questionnaire was used for this study.
29
Lund–Mackay score: This radiological scoring system evaluates sinus inflammation and obstruction using CT scans. Opacification of the frontal, maxillary, anterior/posterior ethmoid, and sphenoid sinuses is scored bilaterally: 0 = no opacification, 1 = partial opacification, 2 = total opacification. Osteomeatal complex obstruction: 0 = no obstruction, 2 = occluded. Disease severity: 0–3 (mild), 4–12 (moderate), 13–24 (severe disease).
30
E-cigarette use: Assessed lifetimes and past-month use, duration of use prior to CRS diagnosis, and use among family members.
Conventional cigarette smoking habits: Included lifetime and past-month tobacco use, duration before CRS diagnosis, smoking ⩾100 cigarettes in a lifetime, and duration of smoking cessation (if applicable).
Patients were interviewed by the authors to complete the questionnaire. Informed consent was obtained from all participants, ensuring their right to accept or decline participation in this study without affecting their healthcare. Patient-related documents were secured in a locked file, accessible only to the principal investigator and co-investigators. The Institutional Review Board of King Saud University granted ethical approval for this study.
Statistical methods
The sample size was calculated based on the following parameters: an expected prevalence of 10.5% for e-cigarette use among Saudi adults, as reported by AlHumaidan et al., 31 a 95% confidence level, 5% margin of error, and a design effect of 2 due to the non-random sampling method used. A minimum sample size of 288 participants was required to obtain valid results.
Data were analyzed using the Statistical Package for Social Sciences (SPSS) software (version 26) developed by IBM. Categorical variables were presented as counts and percentages, while continuous variables were described using mean ± standard deviation or median (interquartile range). Associations between e-cigarette use and demographic or clinical variables were examined using chi-square tests (or Fisher’s exact tests, where appropriate) for categorical variables and the Mann–Whitney U test for continuous variables. Binary logistic regression analysis was used to examine independent predictors of e-cigarette use. E-cigarette use (yes/no) was considered the dependent variable while demographic, behavioral, environmental and clinical variables were entered into the model. Odds ratios (ORs) with 95% confidence intervals (CIs) were calculated and the level of statistical significance was considered at p < 0.05.
Results
Participant characteristics
Three hundred patients with CRS participated in this study. The average age of participants was 41
Demographic and clinical characteristics of the study participants.

SD: standard deviation; PhD: Doctor of Philosophy; HTN: hypertension; DM: diabetes mellitus.
Percentages are shown in parentheses.
A diagnosis of nasal septum deviation was established in 71% of participants. Most of the patients had undergone previous sinus surgery (74%). About 19% reported environmental or occupational exposure to strong odors, 8.3% were allergic to aspirin, 29.7% were asthmatic, 8.3% had hypertension (HTN), 14% had diabetes mellitus (DM), and 3% were diagnosed with immunodeficiency disorder (Table 1).
CRS symptoms and imaging
SNOT-22
The median total SNOT-22 score was 43.5 (24.3–61.8), indicating a moderate to severe impact on patients’ lives. The most commonly reported severe or worst possible symptoms were: nasal blockage (46%), need to blow the nose (42%), decreased sense of smell/taste (41%), postnasal discharge (35%), and waking up tired (35%).
Conversely, the symptoms with the highest proportion of “no problem” responses included ear pain (53%), cough (49%), facial pain or pressure (47%), sadness (45%), dizziness (44%), and embarrassment (44%). Other items, such as ear fullness (42%), reduced concentration (39%), and reduced productivity (38%), were also reported as non-problematic (Figure 1).
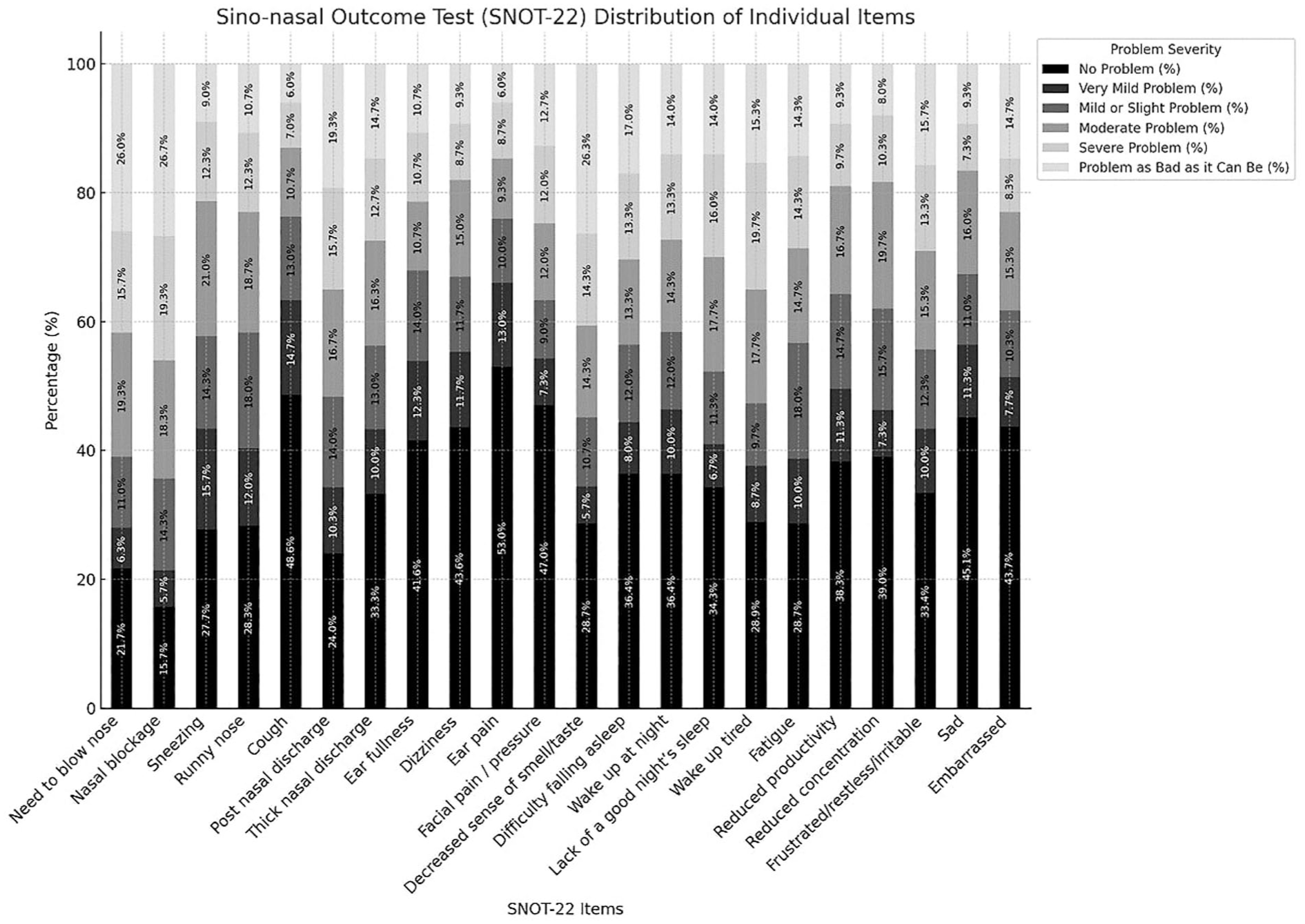
Distribution of Sino-Nasal Outcome Test (SNOT-22) individual items and total scores as a stacked bar chart.
Lund–Mackay score
The mean total score was 13 (9–18), indicating severe disease (reported in 232 patients). Opacification was most commonly observed in the ethmoid sinuses (left anterior ethmoid sinus: 92%; right anterior ethmoid sinus: 90%; right posterior ethmoid sinus: 89%; and left posterior ethmoid sinus: 88%). CT scans revealed opacification in other sinuses as well (maxillary sinuses: 86% (right) and 83% (left); frontal sinuses: 71% (right) and 66% (left); and sphenoid sinuses: 70% (right) and 66% (left)).
Osteomeatal complexes were occluded in most patients’ CT scans: 72.4% in left osteomeatal complex and 69.0% in the right osteomeatal occlusion (Figure 2).

Lund–Mackay score distribution for disease severity among participants.
Electronic cigarette and conventional cigarette use
Among CRS patients, 11% reported a history of e-cigarette use, 43% of them had used e-cigarettes in the past month, while most of them (76%) reported using e-cigarette for 1 year before the CRS diagnosis. Additionally, 17% of participants reported e-cigarette use by a family member (Table 2).
Prevalence of electronic cigarette and conventional cigarette use among participants.

CRS: chronic rhinosinusitis; e-cigarette: electronic cigarette.
Data are presented as counts (n) and percentages (%).
Conventional cigarette smoking was reported by 18% of the participants, with 40% smoking in the past month. The majority (87%) reported smoking over 100 cigarettes in their lifetime with most of them (76%) smoking for more than 2 years before CRS diagnosis. Approximately 18% of conventional cigarette smokers had quit smoking, with 53% having quit for 1 year (Table 2).
Factors associated with e-cigarette use
E-cigarette users were significantly younger than non-users (p < 0.0001). E-cigarette use was also more common among males (p < 0.0001), and those who were employed (p = 0.001). However, nationality and educational level were not significantly associated with e-cigarette use.
Regarding medical history, nasal septum deviation was significantly associated with e-cigarette use (p = 0.008). However, no significant associations were found with physical activity, aspirin allergy, immunodeficiency disorders, previous sinonasal surgery, and environmental/occupational exposure to strong odors (Table 3). No association of these variables was observed even when the effect of potential confounders that is, comorbidities (asthma, DM, and HTN), and prior sinus surgery was controlled (p > 0.05) (Table 3).
Factors associated with electronic cigarette (e-cigarette) use.
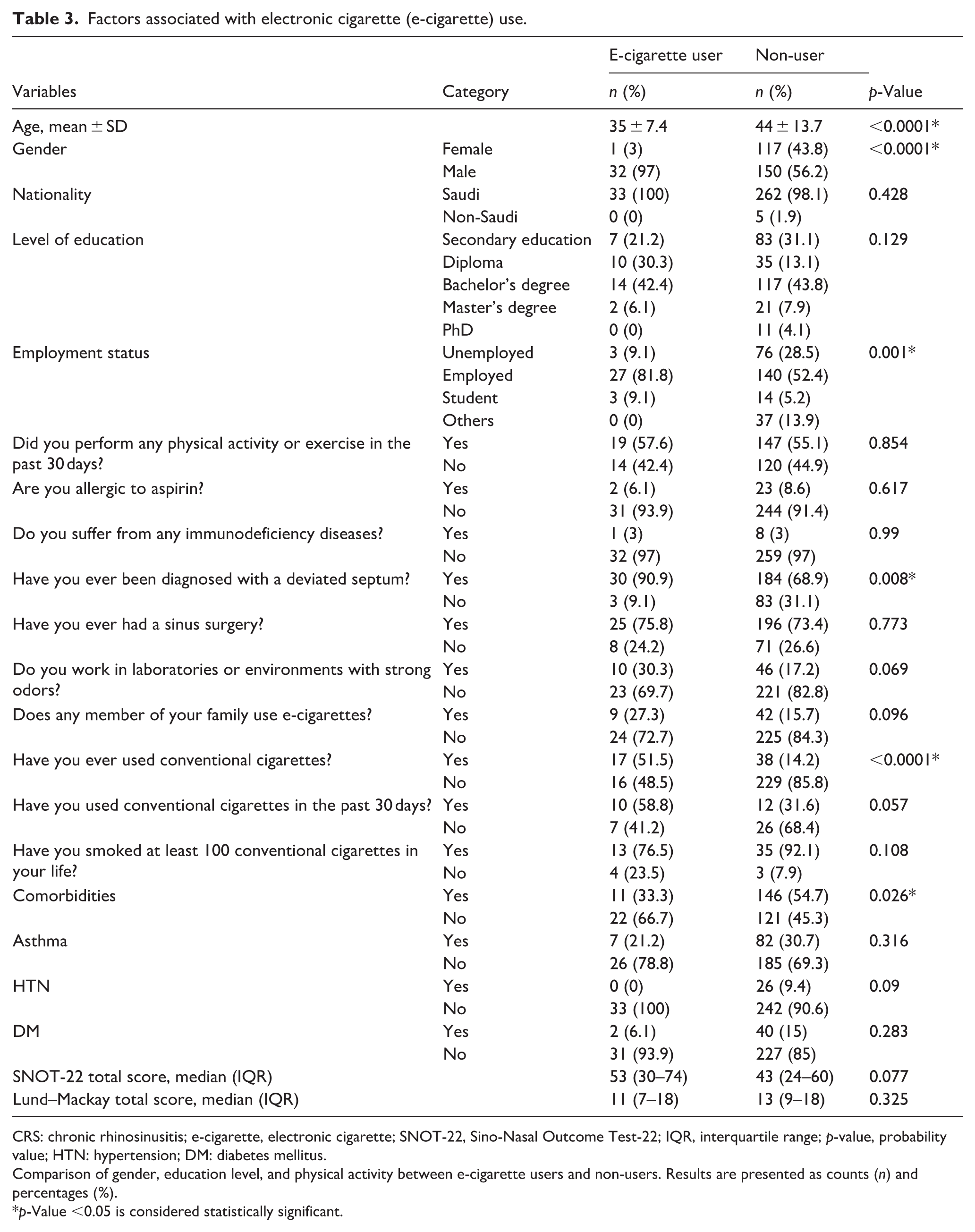
CRS: chronic rhinosinusitis; e-cigarette, electronic cigarette; SNOT-22, Sino-Nasal Outcome Test-22; IQR, interquartile range; p-value, probability value; HTN: hypertension; DM: diabetes mellitus.
Comparison of gender, education level, and physical activity between e-cigarette users and non-users. Results are presented as counts (n) and percentages (%).
p-Value <0.05 is considered statistically significant.
A significant association was found between e-cigarette and conventional cigarette use (p < 0.0001), with 52% of e-cigarette users also smoking conventional cigarettes. However, smoking in the past month or smoking⩾100 cigarettes in a lifetime was not significantly associated with e-cigarette use. Similarly, having a family member who used e-cigarettes was not significantly associated with e-cigarette use (Table 3).
No significant association was detected between e-cigarette use and the Lund–Mackay score. While a higher SNOT-22 total score was observed among e-cigarette users, this association was not statistically significant (Table 3). Among individual SNOT-22 items, only reduced concentration showed a significant association with e-cigarette use (p = 0.02) (Figure 3).
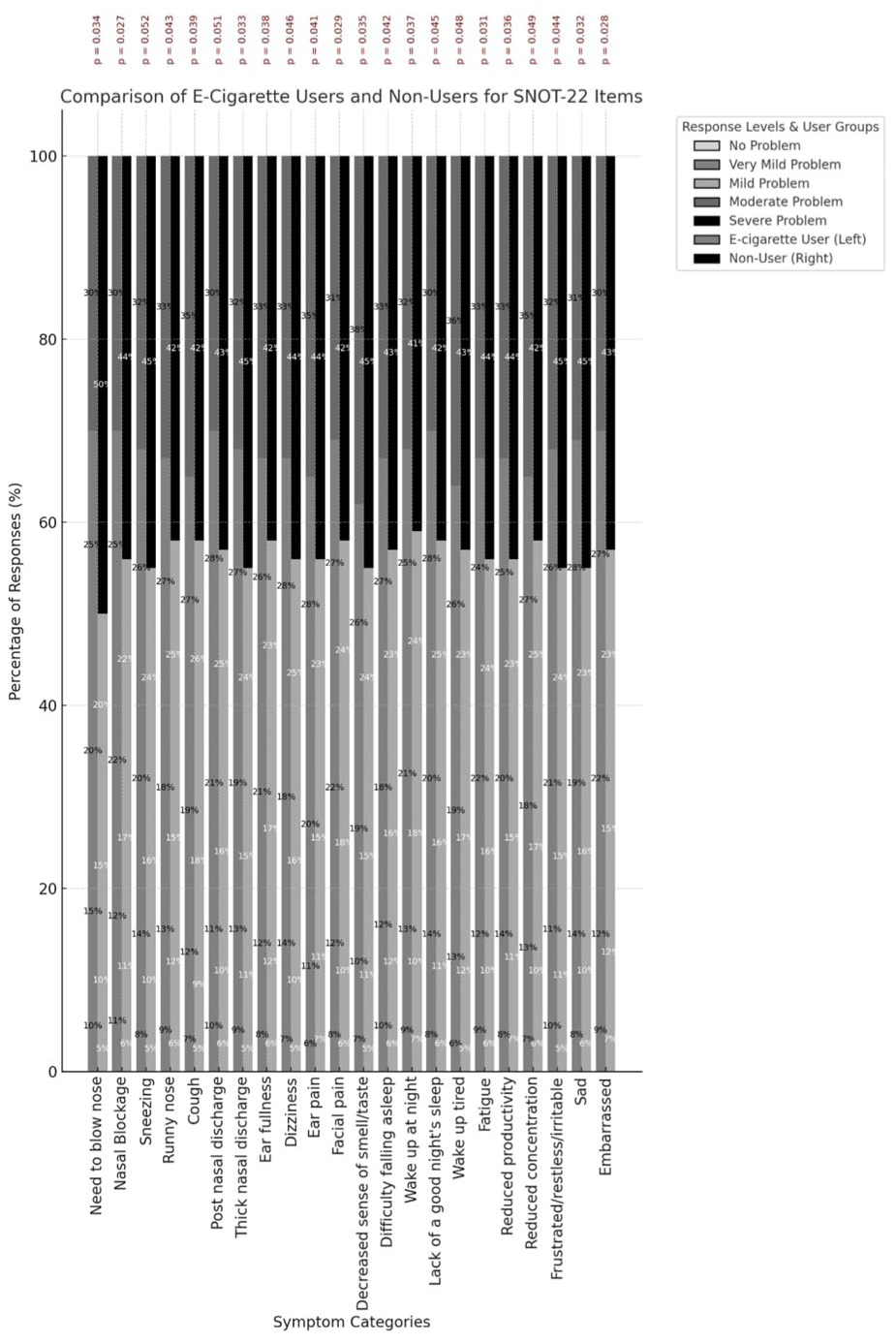
Association between electronic cigarette (e-cigarettes) use and Sino-Nasal Outcome Test (SNOT-22) items.
Factors associated with E-cigarette use
The binary logistic regression model, which is indicated in Table 4, was used to identify the independent predictors of e-cigarette use in the study sample to ensure that the effects of confounders were considered. It showed that the lifetime use of conventional cigarettes was significantly linked to a lower chance of e-cigarette use (B = −1.919, OR = 0.147, 95% CI: 0.064–0.335, p = 0.001) so that those with a lifetime history of conventional cigarette use had an approximately 85% lower chance of using e-cigarettes than never-smokers. Similarly, deviated nasal septum diagnosis was correlated with reduced e-cigarette dependence odds (B = −1.550, OR = 0.212, 95% confidence interval: 0.060–0.749, p = 0.016), indicating an almost 79% reduced probability with such a diagnosis. Conversely, the female participants had statistically significant propensity of use of e-cigarettes when compared to males (B = 0.942, OR = 2.565, 95% trust interval: 1.019–6.457, p = 0.046). The age showed a positive correlation with the use of e-cigarettes, and every year of age increase increased the odds by about 3.5% (B = 0.034, OR = 1.035, 95% CI: 1.005–1.066, p = 0.024). There were no statistically significant correlations with the presence of a family member who uses e-cigarettes (B = −0.787, OR = 0.455, 95% CI: 0.178–1.218, p = 0.100) or work in an environment with strong or pungent odors (B = −0.725, OR = 0.484, 95% CI: 0.193–1.218, p = 0.123). An overall effect of these findings is that a previous traditional smoking background with structural nasal mechanisms may lessen the risk of entering into the e-cigarette smoking habit, but female gender and age seem to augment the tendency of this habit. The exposure to strong odors in the environment and the family smoking of e-cigarettes did not have a statistically significant impact on individual patterns of use in this cohort.
Binary logistic regression analysis of factors associated with the outcome variable.

OR: odds ratio; CI: confidence interval.
All variables were entered simultaneously using the Enter method. A p-value <0.05 was considered statistically significant.
Discussion
CRS is one of the most common upper airway inflammatory disorders, yet data on its association with e-cigarette use remain limited. This study explored e-cigarette use among CRS patients presenting to a tertiary care hospital in Saudi Arabia. Most CRS patients were male and in their 40s—findings consistent with earlier studies.32,33 CRS had a moderate to severe impact on patient’s lives, as shown by the SNOT-22 scores, with nasal blockage, need to blow the nose, reduced sense of smell/taste, postnasal discharge, and waking up tired being the most commonly reported severe symptoms. Lund–Mackay scores revealed severe disease, predominantly affecting the ethmoid sinuses and the osteomeatal complexes.
In this study, 11% of patients with CRS reported a history of e-cigarette use, and 4.7% had used them in the past month. This prevalence is higher than 2.2% reported in the general Saudi population, 14 aligning with findings by Rha et al. in South Korea, where higher odds of CRS were observed among e-cigarette users. 11 While these results suggest a potential association, data remain limited to draw definitive conclusions.
Our study found no significant association between e-cigarette use and CRS symptom severity (SNOT-22 total score) or disease severity (Lund–Mackay score). However, reduced concentration, a specific symptom in the SNOT-22 assessment, showed a significant association with e-cigarette use. These results suggest that while e-cigarettes may not exacerbate CRS severity in a clinically measurable way, they could still impact specific symptoms. This result aligns with the hypothesis that e-cigarette use may contribute to CRS initiation but not necessarily its progression. Future studies examining the duration and quantity of e-cigarette use are needed to explore this relationship further.
As this was a cross-sectional study, no causal inferences can be drawn regarding the relationship between e-cigarette use and CRS. While we found no association with overall CRS severity, e-cigarette use was linked to specific symptoms such as reduced concentration. These findings should be considered hypothesis-generating. Future prospective cohort studies and mechanistic investigations are needed to determine whether e-cigarette use plays a causal role in the initiation or progression of CRS.
E-cigarette users in our study were more likely to be younger males, consistent with findings by Rha et al. and Al Humaidan et al.11,31
In this study, 18% of patients with CRS reported conventional cigarette use, with 7.3% having smoked in the past month. The prevalence of conventional cigarette use exceeded that of e-cigarettes; concurrent use of both products was also observed, consistent with previous studies.11,34 This dual use may be considered as the CRS patients’ attempt to quit smoking or their perception of e-cigarettes as a less harmful alternative, as reported in Saudi Arabia, where nearly 49% of e-cigarette users failed to quit smoking. 35
The pathogenesis of CRS involves mucociliary dysfunction, anatomic variation, genetic predisposition, and environmental exposures like allergens and pathogens.8,36,37 E-cigarette vapor has been shown to disrupt nasal epithelial integrity through oxidative stress and cytotoxicity, leading to mucosal inflammation.38,39 This disruption may impair mucociliary clearance, which is crucial for eliminating pathogens and debris, resulting in prolonged inflammation and CRS development. 40 Emerging mechanistic evidence further supports this hypothesis. A recent experimental study demonstrated that e-cigarette vapor can directly penetrate the sinonasal cavities, 41 suggesting that the upper airway mucosa is directly exposed to aerosolized particles and chemicals during vaping. This observation provides biological plausibility for a potential causal relationship between vaping and CRS, although longitudinal human studies are still needed to confirm this association.
Additionally, e-cigarette exposure has been associated with immune suppression and increased pathogen virulence, which may further contribute to CRS initiation or exacerbation.42,43 Studies have reported reduced cytokine expression essential for early immune responses and decreased gene activity in immune regulation. Concurrently, bacterial colonization in the upper airway may become more virulent, exhibiting resistance to antimicrobial peptides. 42 These mechanisms offer plausible explanations for our findings, particularly the observed associations between e-cigarette use and CRS symptoms such as reduced concentration. However, further studies are needed to confirm these pathways in human populations.
Most studies examining the impact of e-cigarette use on the upper airway are limited to in vitro or animal studies, which may not fully reflect outcomes in humans. Human data, particularly on the association between e-cigarette use and CRS, remain scarce. To our knowledge, this is the first study in Saudi Arabia to investigate e-cigarette use among patients with CRS, using an objective diagnosis via CT scans and a sufficient sample size.
Our findings have important clinical and public health implications in Saudi Arabia. The prevalence of e-cigarette use among CRS patients in this cohort was higher than estimates in the general Saudi population, suggesting that e-cigarette use may be emerging as a relevant exposure in this patient group. Clinically, otolaryngologists should consider screening for e-cigarette use during patient evaluations, as it may contribute to symptom burden and comorbidities, even if not directly linked to disease severity. From a public health perspective, the increasing uptake of e-cigarettes among Saudi youth and young adults underscores the need for awareness campaigns and preventive strategies targeting e-cigarette use. Policymakers should recognize e-cigarette use as a potential risk factor for respiratory morbidity, alongside conventional smoking, and integrate it into national tobacco control initiatives.
Saudi Arabia has made considerable strides in expanding cessation services across the Kingdom. The Ministry of Health currently operates hundreds of fixed smoking cessation clinics (SCCs) and mobile units, complemented by a national 937-service hotline and mobile applications that connect users to counseling and pharmacologic support. These services offer free medical consultations, behavioral therapy, and follow-up care. Awareness and use of these services remain moderate: according to the 2019 GATS, 60% of tobacco users were aware of fixed SCCs, 26% knew about mobile clinics, but only 9% had actually visited an SCC. Recent evaluations also report high levels of patient satisfaction with cessation services. In the context of rising e-cigarette use among patients with CRS, these infrastructure and public health resources could be leveraged to integrate cessation support (including for vaping) into otolaryngology and respiratory clinics, enhancing preventive care and reducing potential complications associated with both traditional and electronic nicotine product use.44,45
However, our study has some limitations. The cross-sectional design does not establish causal inference, and CRS subtypes (e.g., with or without nasal polyps) were not analyzed separately. These represent distinct endotypes with different inflammatory mechanisms, and it is plausible that e-cigarette exposure could differentially affect the two subgroups. Future studies should stratify CRS patients accordingly to better elucidate these potential differences. Another limitation is that while we captured lifetime, recent, and duration of e-cigarette use, we did not assess intensity of use (e.g., daily frequency or nicotine concentration), which may influence disease outcomes. Recall bias is also possible, as data on e-cigarette and cigarette use were based on self-report. Additionally, the hospital-based nature of our sample may limit generalizability to the broader Saudi population. Furthermore, the association between e-cigarette use and the duration or intensity of exposure was not explored. Also, the absence of a control group precludes definitive conclusions about the risk of CRS attributable to e-cigarette use. Nevertheless, our findings provide initial descriptive evidence in a Saudi cohort and underscore the need for future longitudinal and case-control studies to clarify causal relationships. Despite these limitations, this study provides an important knowledge base and highlights the need for further investigation. Future longitudinal studies with larger cohorts should examine e-cigarette use as a potential factor in CRS initiation and symptom progression.
Results of multivariate logistic regression analysis identified several independent predictors of e-cigarette use among CRS patients after statistical adjustment for potential confounding factors. Female gender was independently associated with increased odds of e-cigarette use, although males showed a higher prevalence in unadjusted analyses, highlighting the importance of conducting multivariable analysis. Age also showed a positive association with e-cigarette use, with increasing age leading to a slightly higher likelihood of use. Conversely, a history of traditional cigarette use was associated with a significant decrease in the odds of using e-cigarettes, suggesting that e-cigarette use in this sample may reflect a different behavioral pattern, and not necessarily a direct alternative to traditional smoking. In addition, patients diagnosed with a deviated nasal septum were less likely to use e-cigarettes, possibly due to intolerance to aerosol inhalation due to structural changes in the upper respiratory tract. No statistically significant associations were observed between e-cigarette use and either environmental exposure to strong odors or a family member’s use of e-cigarettes. Overall, these findings suggest that e-cigarette use among CRS patients is influenced by demographic, behavioral, and anatomical factors and should be interpreted with caution given the cross-sectional nature of the study.
Conclusion
This study found that patients with CRS presenting to King Saud University Medical City had severe disease on sinus CT scans and a moderate to severe impact on their quality of life, as measured by the SNOT-22 score. E-cigarette use was significantly associated with younger age, male gender, employment status, regular smoking, and nasal septum deviation but not with disease severity or overall symptom intensity. E-cigarette use was also associated with reduced concentration. Further long-term research on a larger scale is required to support our findings and investigate further associations over time.
Supplemental Material
sj-doc-1-taj-10.1177_27558428261421699 – Supplemental material for Electronic cigarette use among patients with chronic rhinosinusitis: A cross-sectional hospital-based study in Saudi Arabia
Supplemental material, sj-doc-1-taj-10.1177_27558428261421699 for Electronic cigarette use among patients with chronic rhinosinusitis: A cross-sectional hospital-based study in Saudi Arabia by Ahlam H. Alamri, Mohammed A. Alwahibi, Ali M. Almatri, Saleh H. Alawaji, Abdulrahman M. Mokhatar, Ibrahim M. Alotaibi, Nawaf H. Alzaben and Ahmad S. Alroqi in Therapeutic Advances in Chronic Disease
Footnotes
Acknowledgements
We also like to thank Editage for English language editing.
ORCID iDs
Ethical considerations
This study was approved by the Ethics Committee of King Saud University (Ref. No. 24/1493/IRB) on August 11, 2024. Before enrollment, all participants provided verbal informed consent, recorded in an independent witness’s presence. The research adhered to ethical principles outlined by the Institutional Review Board of King Saud University.
Consent to participate
Verbal informed consent was obtained from all participants prior to enrollment. The ethics committee approved the use of verbal consent instead of written consent due to the observational nature of the study and minimal risk involved. Verbal consent was documented by the research team in case report forms at the time of data collection.
Author contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability Statement
Data sharing is not applicable to this article.
Supplemental material
Supplemental Material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.