
Abstract
Introduction:
Sick leave documentation is a routine component of emergency visits but remains understudied in obstetrics and gynecology emergency room settings. Understanding the factors associated with sick leave issuance can inform better resource allocation and highlight opportunities for integration into primary healthcare services, particularly in the context of women’s health. The purpose of this study was to evaluate the trends, features, and associated factors of sick leave issued in the obstetrics and gynecology emergency room at a major teaching hospital in Saudi Arabia.
Methods:
This record-based retrospective epidemiological study was conducted on all obstetrics and gynecology emergency room visits of females aged ⩽60 years between January and December 2022 at a Saudi teaching hospital. Sociodemographic, clinical, and operational variables were extracted. Logistic regression was used to identify predictors of sick leave issuance.
Results:
Of the 8743 visits, 7.61% resulted in sick leave. Older age, non-Saudi nationality, musculoskeletal and gynecological complaints, the autumn season, and morning visits were significantly associated with higher odds of sick leave. Among those issued with sick leave, only 4.36% received more than 3 days, which were mostly associated with hospital admission, the winter season, and longer emergency room stays.
Conclusion:
A sick leave is often requested for non-urgent complaints that can be managed in the primary healthcare settings. From a public health standpoint, integrating sick leave documentation and women’s health services into primary healthcare may reduce unnecessary emergency room visits, optimize healthcare delivery, and support national healthcare transformation goals.
Keywords
Introduction
Sick leave is a legally recognized patient right that provides workers with time off to recover from illness, based on physician certification. In some clinical situations, sick leave may be a crucial part of medical management to allow patients the necessary duration for physical and psychological recovery. To balance patient well-being, workforce needs, and healthcare system integrity, healthcare providers must prescribe sick leave only when it is medically required to avoid any ethical, legal, or economic consequences associated with unnecessary issuance.1,2
Emergency rooms (ERs), including obstetrics and gynecology (OB-GYN) ERs, are frontline settings where patients often present with acute symptoms, ranging from menstrual disorders and early pregnancy symptoms to OB-GYN emergencies. These conditions can significantly impair daily and work functioning, even when inpatient care is not indicated.3,4 In such settings, sick leave issuance is often based on clinical judgment rather than standardized protocols. In general ER practice, clinicians report that sick leaves are a frequent order, often linked to viral illnesses or mild gastrointestinal disorders, and that guidance about duration is highly variable. 5 However, patterns of sick leave issuance in OB-GYN ER settings, where specific clinical and demographic factors may influence decisions differently, are underreported, especially in Middle Eastern countries.
In Saudi Arabia, research on sick leave has primarily focused on general healthcare worker absenteeism and administrative sick leave patterns. A study in Riyadh reported frequent sick leave requests among younger staff, nurses, hospital assistants, and housekeepers, often due to upper respiratory tract infections, and identified flu vaccination as a protective factor. 6 Despite the significance of sick leave as a healthcare and workforce concern, little is known regarding the clinical and temporal patterns of sick leave issuance from OB-GYN ER services in Saudi Arabia. Understanding these trends is critical for developing institutional policies that promote appropriate sick leave utilization and continuity of care.
Therefore, this study aimed to assess the trends, frequency, characteristics, and determinants of sick leave issuance in the OB-GYN ER of a large teaching hospital in Saudi Arabia. Moreover, to determine factors associated with prolonged sick leave duration. By understanding these patterns within the broader context of women’s health, this study aimed to inform institutional policies, promote continuity of care, and guide effective integration with primary healthcare (PHC) systems.
Methodology
Ethical statement
This study was approved by the Institutional Review Board of Imam Abdulrahman Bin Faisal University (IRB-2022-01-443). The requirement for written informed consent was waived, as the study was based on anonymized, retrospective data.
Study design and setting
This record-based retrospective epidemiological study was conducted at a large teaching hospital in Saudi Arabia. The study focused on the OB-GYN ER, which is staffed by a multidisciplinary team including consultants, residents, and rotating medical trainees, as well as other healthcare providers such as nurses. The facility is equipped with an examination room, three observation beds, pharmacy and radiology services, and the capacity to admit patients if necessary. Females presenting with obstetric or gynecological complaints, as well as pregnant females with medical conditions, are assessed in the OB-GYN ER through direct walk-ins, referrals from PHC, or transfers from the adult ER, reflecting its broader role in providing initial evaluation and issuing sick leave when needed.
Study population and sampling
All OB-GYN ER visits by females aged 60 years or younger between January 1 and December 31, 2022, were eligible for inclusion. Patients over 60 years of age were excluded, as they are generally retired and are not given sick leave. Visits with missing data were also excluded. As this was a retrospective study including all eligible OB-GYN ER visits during the 1-year period, no a priori sample size calculation was performed. Instead, the sample size was determined by the complete coverage of available encounters.
Data collection and variables
A structured electronic data collection tool was developed for this study to extract sociodemographic, clinical, and operational information from the medical records. The study variables were predefined by the investigators, guided by prior literature, the study objectives, and the availability of data within the electronic medical records.6–9 Content validity of the data collection tool was established through consensus among the research team, which comprised four senior consultants with expertise in family medicine, OB-GYN, women’s health, and public health. The collected data included patient age, nationality, triage level (according to the Canadian Triage and Acuity Scale), date and time of visit, presenting complaint, shift, outcome status, length of stay (LoS) in the OB-GYN ER, and whether a sick leave was issued, including the number of days granted (Supplementary Table 1). 10
Statistical analysis
The first outcome of this article was whether an OB-GYN ER patient visit had been issued with a sick leave (yes/no), and a secondary outcome based on a subgroup analysis was the duration of sick leaves in days (⩽3 vs >3 days). Seasons were classified as winter (December, January, February), spring (March, April, May), summer (June, July, August), and autumn (September, October, November), and nationality was divided into Saudi or non-Saudi. The three shifts that the patient arrived at the OB-GYN ER were morning (8:00 am–16:00 pm), evening (16:00 pm–00:00 am), and night (00:00 am–8:00 am).
All data were described by either mean ± standard deviation or median and interquartile range, depending on the normality of the continuous variables’ distribution. Categorical variables were described as frequencies and percentages. Bivariate analyses were performed by t-tests, Mann–Whitney U tests, and chi-squared tests to derive p values of associations, with the significance level set at <0.05. Binary logistic regression models were used to derive unadjusted and adjusted odds ratios (ORs) and 95% confidence intervals (CIs). The adjusted model included age, nationality, triage level, outcome status, presenting complaint, season of visit, shift, and LoS. These variables were selected a priori based on prior literature, study objectives, and clinical plausibility. Stata Statistical Software version 15 was used to conduct statistical analysis. 11
Results
A total of 8743 visits were included in the study. The mean age of patients was 30.84 ± 7.49 years. Of the total number of visits, 14.74% were for non-Saudi nationals. Triage level IV was the highest recorded level at 71.82%, followed by triage level III (Table 1).
Obstetrics and gynecology emergency room visit characteristics according to sick leave orders between January and December 2022.
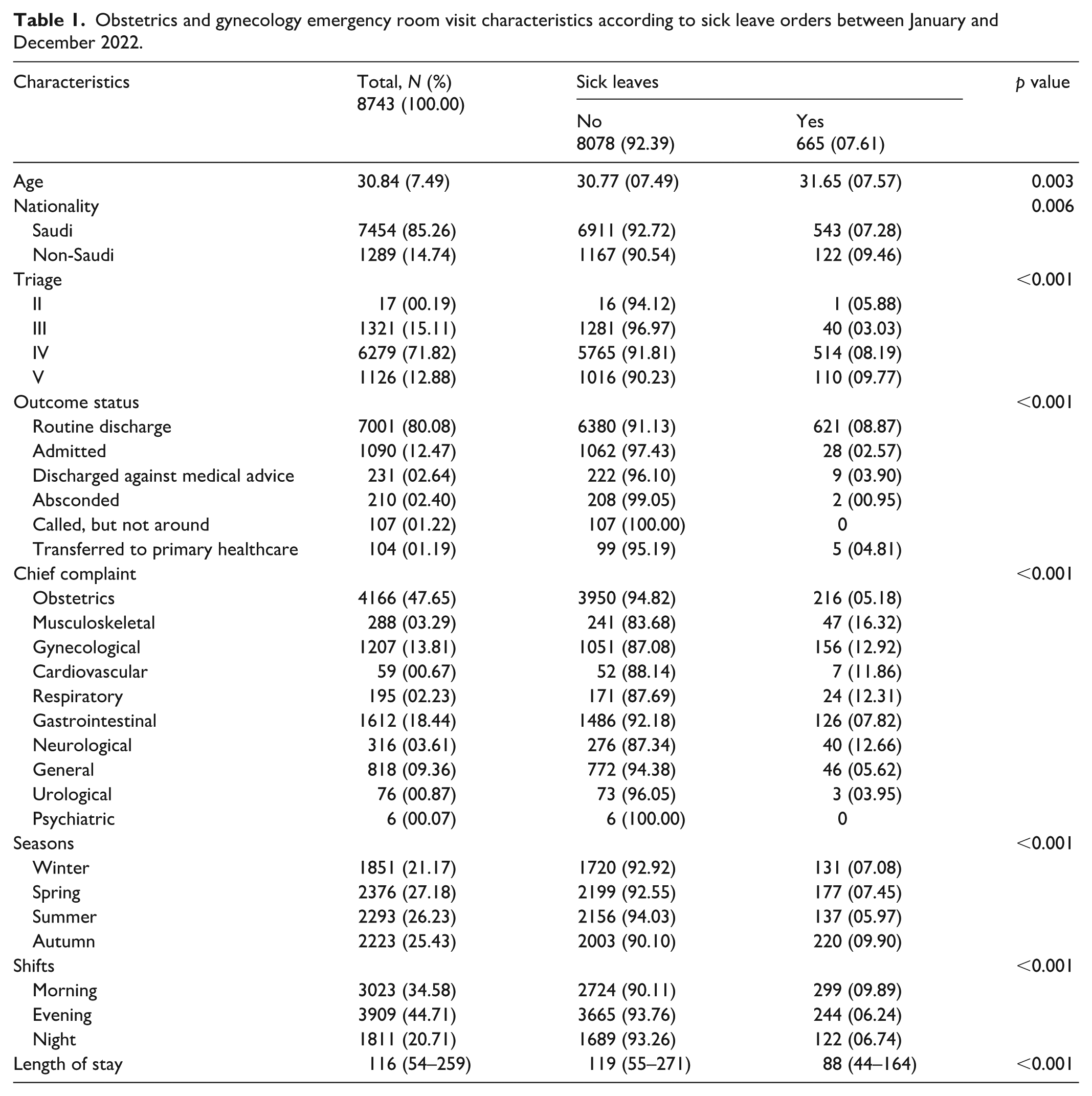
OB-GYN ER visit characteristics and their associations with sick leaves
Table 1 shows the bivariate associations between sick leaves issued and visit characteristics. Sick leaves were issued to 7.61% of the 8743 visits recorded during the study period. A higher percentage of patient visits with sick leaves were found in non-Saudis compared to Saudis (p = 0.006). They were also recorded mostly for patient visits belonging to triage level V and least for triage level III (9.77% and 3.03%, respectively). Patient visits with issued sick leaves were mostly for musculoskeletal complaints, followed by gynecological complaints (16.32% and 12.92%, respectively). With regards to seasons, sick leaves were mostly requested during autumn and least requested during the summer (9.90% and 5.97%, respectively). Visits occurring during the morning shift had the highest percentage of sick leave requests. Also, visits with issued sick leaves had a shorter median LoS compared to those without (88 vs 119 min, respectively).
Prevalence of sick leaves per month
Figure 1 plots the prevalence of sick leaves per month during the study period between January and December 2022. July visits had the lowest recorded sick leaves at around 4.50% of all visits during that month. Whereas requests for sick leave had gradually increased after July and had peaked during the month of October.
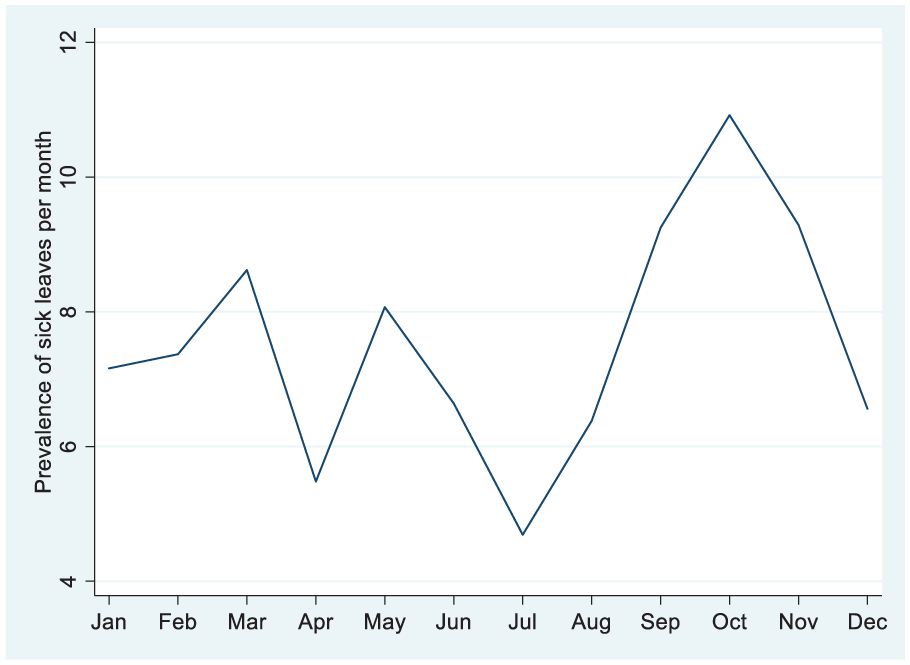
Pattern of sick leaves issued from obstetrics and gynecology emergency room between January and December 2022.
Predictors of sick leaves issued
Table 2 provides the results of univariable and multivariable regression models. Increased age was observed to be a significant predictor of sick leaves (OR = 1.02, 95% CI = 1.01–1.03). Non-Saudi nationals were 30% more likely to receive sick leave (95% CI = 1.04–1.61). Triage level III was associated with a 50% decreased likelihood of sick leaves when compared to triage level IV, and this was highly statistically significant (p < 0.001, 95% CI = 0.35–0.71). With regards to outcome status, all statuses when compared to routine discharge were found to have a lower likelihood of sick leave, and this was more pronounced for patients who had absconded (OR = 0.09, 95% CI = 0.02–0.38). Musculoskeletal complaints had more than a three-fold increased likelihood of sick leave (OR = 3.14, 95% CI = 2.19–4.49), and gynecological, cardiovascular, respiratory, and neurological complaints all had over a two-fold increased likelihood of sick leave compared to obstetrics complaints. With regards to the season of the visit, in comparison with spring visits, visits that had occurred during the summer season had a 26% lower likelihood of sick leave (95% CI = 0.58–0.93), whereas those that had occurred during the autumn season had a 26% increased likelihood (95% CI = 1.01–1.57). Also, for the shift of the visit, visits during the morning shift had a two-fold increased likelihood of sick leaves (OR = 2.00, 95% CI = 1.67–2.41) when compared to evening visits. LoS was observed to have an inverse association (95% CI = 0.98–0.99).
Univariable and multivariable binary logistic regression models of sick leaves issued to obstetrics and gynecology emergency room patients, adjusted for demographic, clinical, and visit-related variables.

CI: confidence interval; OR: odds ratio.
Subgroup analysis of patients with sick leave
Figure 2 shows the distribution of visits issued with sick leave (n = 665) according to the number of days given. Over 50% of sick leaves issued were for only 1 day; this was followed by 2 days (24%). Only one patient visit was issued with 4 and 13 days each (0.15%).

Number of sick leave days issued between January and December 2022 (n = 665).
Of the 665 visits with sick leave, 95.64% had ⩽3 days, whereas 4.36% had over 3 days of sick leave. Table 3 presents the bivariate associations between patient visit characteristics and number of sick leave days. Only outcome status, seasons, and LoS were observed to have a statistically significant association (p < 0.05). For outcome status, a higher percentage of sick leaves over 3 days was observed for the visits that concluded in admission (53.57%). Also, a higher percentage of visits with sick leaves of over 3 days was seen for visits that had occurred during the winter season (11.45%). Patient visits that had sick leave days of over 3 days were found to have a longer LoS than those that had ⩽3 days.
Characteristics of obstetrics and gynecology emergency room patients according to the number of days of sick leave issued.

Discussion
This study highlights critical trends in sick leave orders among females presenting to the OB-GYN ER. It offers a deeper understanding of how various clinical, demographic, and temporal factors influence the issuance of sick leaves. By examining these patterns, the study sheds light on healthcare utilization behaviors and potential inefficiencies in service delivery. These insights can inform strategies to optimize care pathways and enhance integration with PHC services.
This study revealed that 7.61% of OB-GYN ER visits were issued with a sick leave. This finding is higher than a previous Saudi study, which reported a sick leave rate of 4.7% for ER visits overall, without a specific focus on OB-GYN cases. 12 Limitations in the available studies with an objective of investigating sick leave prescriptions in the OB-GYN ER settings render comparisons difficult. However, literature confirms that the unique health conditions in the OB-GYN specialty, including issues related to pregnancy, dysmenorrhea, abnormal uterine bleeding, and gynecological emergencies, usually necessitate a more extended recovery period, leading to an increased likelihood of prescribing a sick leave.3,4,7,13
This study identified multiple significant predictors of sick leave issuance among females visiting the OB-GYN ER. Notably, older age was associated with an increased likelihood of receiving a sick leave certificate. This trend aligns with findings from occupational health literature, which suggest that aging is associated with accumulating health issues and increased absenteeism, particularly among females in physically or mentally demanding roles.14,15 Non-Saudi nationality was also linked to higher sick leave issuance. While some studies indicate that local populations often show higher sick absenteeism due to job security and access to leave, in this context, expatriate females may be more likely to seek formal documentation for sick leave due to stricter employer policies or limited access to PHC.16–18 A strong association was found between morning OB-GYN ER visits and sick leave issuance. This likely reflects work-related behaviors; patients presenting to the ER early may seek documentation for an ongoing or missed workday. 19 Similar patterns have been reported in other Saudi studies, where emergency departments frequently serve as entry points for nonurgent care and sick certification.12,16
The type of complaint was a significant determinant with sick leave issuance in the present study. Nonobstetric conditions, such as musculoskeletal, respiratory, cardiovascular, gynecological, and neurological issues, were more than twice as likely to result in sick leave as obstetric cases. This aligns with global data showing that musculoskeletal pain is the leading cause of sickness absenteeism.20–22 Besides, obstetric emergencies typically result in direct admission or acute treatment rather than documentation for temporary work absence. Gynecological complaints were the second most common reason for sick leave issuance in the study. Within this broad category, common presentations such as abnormal uterine bleeding, pelvic pain, and dysmenorrhea were frequently observed and are known to impair daily functioning, which likely explains their association with sick leave. A Spanish study among 1800 females found that 72.6% experience menstrual pain, significantly impacting daily life and work, with over a third considering sick leave. Despite this, only 17.3% actually requested leave, mainly due to fear of professional consequences. 3 Interestingly, higher-acuity triage (level III) was associated with a lower rate of sick leave issuance than less urgent cases in the current study. This reinforces prior observations that many ER visits and issued sick notes were for mild, self-limited conditions that do not warrant inpatient care. 16 Moreover, higher acuity cases mostly result in admission rather than routine discharge and home rest. In agreement with this explanation, visits that concluded with routine discharge status in the study had the highest frequency of sick leave issuance.
In the current study, a clear seasonal trend emerged in sick leave issuance, with the lowest rate in July (~4.5%) and a peak in October. This pattern was confirmed by the regression analysis, which showed that autumn visits had higher odds of sick leave issuance than those in spring, while summer visits showed a decreased odd of sick leave. These trends correlate with global and regional data linking cooler months to increased incidence of respiratory infections and exacerbations of chronic illnesses.23,24 Conversely, the summer period, marked by extreme heat, vacations, and reduced work activities, may lower the demand for ad hoc sick certification. Further research should explore the direct links between seasonal epidemiology and patient sick leave in this context, enabling tailored resource planning and patient education interventions. Interestingly, shorter OB-GYN ER LoS was associated with a higher likelihood of sick leave issuance. This may reflect the rapid assessment and discharge of patients with acute but disruptive symptoms, such as pelvic pain, early pregnancy complications, or dysmenorrhea, who require rest but not prolonged observation. In such cases, clinicians may issue sick leave as a precautionary measure to support recovery despite a brief ER stay or admission to the hospital. Conversely, longer LoS often involves extended monitoring, specialist consultation, or inpatient admission, which may reduce the perceived need for postdischarge sick leave, as rest has already been provided during the OB-GYN ER stay. 8 Another possible explanation could be that these patients usually need hospital admission and had the sick leave orders by the admitting team prior to discharge from the hospital rather than the OB-GYN ER attending physicians. Nonetheless, strengthening PHC integration and ensuring continuity of care may reduce unnecessary sick leave issuance in OB-GYN ER settings by offering timely follow-up, appropriate symptom management, and preventive interventions in a more stable outpatient environment.
A majority (95.64%) of prescribed sick leaves in the present study were limited to 3 days or less, suggesting that most patients experienced relatively short-term health issues. While specific data on sick leave issuance in OB-GYN ER settings is limited, this short duration reflects a conservative and cautious approach that aligns with common clinical and administrative practices, where short-term leave is often deemed sufficient for symptom recovery or social adjustment. Furthermore, over 50% of issued sick leaves were for just 1 day, indicating that many patients faced acute, short-term health issues that resolved quickly. On the other hand, a minority of patients (4.36%) required more than 3 days of sick leave, this result may reflect more complex or severe medical conditions, warranting further investigations or management. The lower percentages of prolonged duration of prescribed sick leave can be attributed to the fact that the issuance of prolonged sick leave is highly conservative in this setting, potentially reflecting either a cautious clinical approach or institutional protocols. Further analyses revealed that visits concluded with admission, visits during the winter season, and visits with a prolonged LoS in the OB-GYN ER were significantly associated with the longer duration of sick leaves. Patients requiring admission usually present with more severe conditions, warranting the immediate issuance of longer rest periods and additional sick leave days by the attending consultant. The winter season may reflect fluctuations in both clinical presentations and service delivery. For instance, certain months may be associated with a rise in pregnancy complications, upper respiratory tract infections, or asthma exacerbations, influencing sick leave issuance. A study from Spain found that cold temperatures increased the risk of sickness absence episodes attributable to infectious and respiratory diseases. 25 A prolonged LoS in the OB-GYN ER may occur due to various factors, including the need for intravenous fluid hydration, additional imaging studies such as computed tomography scans, and the requirement for medical consultations from other specialties such as endocrinology, internal medicine, or surgery. 8 Consequently, visits with a prolonged LoS could necessitate extended sick leave durations.
A key strength of this study is the integration of both clinical and administrative variables, including triage level, presenting complaint, timing, and visit outcome, offering a comprehensive and multidimensional understanding of factors influencing sick leave requests. Furthermore, the inclusion of sick leave duration adds analytical depth, allowing for indirect assessment of the perceived or clinical severity of cases. This study also contributes to the limited literature on the intersection between ER care utilization and occupational health considerations in OB-GYN settings, providing a valuable foundation for health policy and PHC planning. While this study was conducted in Saudi Arabia, its findings contribute both to the local and wider international discourse on healthcare utilization. On the one hand, the results highlight specific contextual factors related to the Saudi healthcare system, such as patterns of OB-GYN ER utilization and the integration of sick leave certification within a PHC setting, which is aligned with the national transformation goals and Saudi Vision 2030. 26 At the same time, many of the observed patterns, including higher sick leave issuance for nonurgent complaints, seasonal variations, and the predominance of short-duration leaves, resonate with global trends reported in the literature. Thus, the study offers insights that may be relevant to other healthcare systems facing similar challenges in balancing OB-GYN ER workload, sick leave issuance, and integration with PHC. Several limitations should be acknowledged. As a retrospective study, causal relationships cannot be established. The reliance on electronic records may introduce information bias due to variations in clinical documentation or coding of complaints. A further limitation is that no prospective sample size calculation was undertaken. However, the use of a complete census of encounters and the high events-per-variable ratio provide reassurance regarding the robustness of the analyses. The generalizability of findings may be limited, as the study was conducted at a single institution with specific administrative and staffing structures. Additionally, nonclinical influences on sick leave issuance, such as patient expectations, employment policies, or physician characteristics, were not addressed in the dataset. Moreover, detailed occupational or employment-related information was not available, preventing assessment of workplace influences on sick leave requests. Finally, the study did not include patient-reported outcomes or qualitative perspectives, which could have provided additional insights into the motivations and expectations behind sick leave utilization. In addition, seasonal and contextual factors may not be generalizable to other countries, where health-seeking behaviors, socioeconomic conditions, and seasonal patterns of illness can differ. Such variations further limit the broader applicability of our findings. Future research should explore these sociocultural and institutional factors through prospective or qualitative methodologies to complement these findings.
Insights into public health and family medicine
The pattern of sick leave issuance in OB-GYN ER settings offers critical insights into both patient needs and system-level inefficiencies. This study highlights that sick leaves are frequently issued for nonemergent complaints such as musculoskeletal and gynecological conditions that can often be appropriately managed in PHC settings. The seasonal and temporal variations, as well as the predominance of short-duration sick leaves, suggest an overreliance on OB-GYN ER services for routine health needs and work documentation.
From a public health and women’s health perspective, these findings indicate an opportunity to improve the integration of occupational health and women’s services into PHC. Equipping family physicians with training to manage common OB-GYN and women’s health complaints and issue sick leaves could reduce unnecessary OB-GYN ER visits and associated system burden. Moreover, clear policies regarding sick leave issuance, coupled with patient education on the appropriate settings for nonurgent care, would enhance healthcare efficiency. Aligning with Saudi Vision 2030, this calls for expanding community-based care, digital sick leave systems, and streamlined referral pathways. By shifting care delivery for mild-to-moderate OB-GYN and women’s health-related conditions from ERs to PHCs, the healthcare system can better serve patients while minimizing costs and enhancing care quality and continuity.
Conclusion
Sick leave was issued in ~7.6% of OB-GYN ER visits, with notable variability by patient demographics, clinical presentation, and visit characteristics. Non-Saudi nationals, older age, and morning shift visits were significantly associated with increased odds of receiving a sick leave. Clinical factors such as musculoskeletal, gynecological, and nonobstetric complaints were strong predictors of sick leave issuance, suggesting that many of these visits may not require specialized OB-GYN ER care and could be redirected to PHC services. Seasonal variations were also observed, with the highest issuance during autumn and the lowest during summer. Interestingly, shorter OB-GYN ER LoS was associated with a higher likelihood of sick leave issuance. Most sick leaves were for a short duration (⩽3 days), though longer durations were more frequent among patients admitted or who had presented during winter. From an epidemiological and public health perspective, these findings underscore the importance of optimizing care pathways and triage protocols while also highlighting opportunities to integrate sick leave services and nonurgent OB-GYN care into PHC settings to reduce OB-GYN ER burden and improve continuity of care.
Supplemental Material
sj-docx-1-smo-10.1177_20503121251384526 – Supplemental material for Sick leave issuance in an obstetrics and gynecology emergency room in Saudi Arabia: Insights for public health and family medicine
Supplemental material, sj-docx-1-smo-10.1177_20503121251384526 for Sick leave issuance in an obstetrics and gynecology emergency room in Saudi Arabia: Insights for public health and family medicine by Nouf A. AlShamlan, Reem S. AlOmar, Nourah H. Al Qahtani, Fatimah S. Badghaish, Rehab F. Alghamdi, Omar Y. Almukhadhib, Nurah Salham Alnuaimi, Assim M. AlAbdulKader, Amani S. AlOtaibi, Abdullah H. Alreedy and Malak A. Al Shammari in SAGE Open Medicine
Supplemental Material
sj-docx-2-smo-10.1177_20503121251384526 – Supplemental material for Sick leave issuance in an obstetrics and gynecology emergency room in Saudi Arabia: Insights for public health and family medicine
Supplemental material, sj-docx-2-smo-10.1177_20503121251384526 for Sick leave issuance in an obstetrics and gynecology emergency room in Saudi Arabia: Insights for public health and family medicine by Nouf A. AlShamlan, Reem S. AlOmar, Nourah H. Al Qahtani, Fatimah S. Badghaish, Rehab F. Alghamdi, Omar Y. Almukhadhib, Nurah Salham Alnuaimi, Assim M. AlAbdulKader, Amani S. AlOtaibi, Abdullah H. Alreedy and Malak A. Al Shammari in SAGE Open Medicine
Footnotes
Acknowledgements
The authors would like to thank the Information Technology Department at King Fahd Hospital of the University for their valuable support in providing the required data for this study.
Ethical considerations
This study was approved by the Institutional Review Board of Imam Abdulrahman Bin Faisal University (IRB-2022-01-443).
Consent to participate
The requirement for written informed consent was waived, as the study was based on anonymized, retrospective data.
Author contributions
N.A.A. and R.S.A. contributed to the study’s conception. N.A.A. and R.S.A. carried out the study design. R.S.A. performed data analysis. N.A.A., R.S.A., and N.H.A. contributed to material preparation, and analysis interpretations. F.S.B., R.F.A., O.Y.A., N.S.A., and A.H.A. collected the data. All authors participated in the writing process and approved the final version of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.