
Abstract
Objective:
During times of crises, women are at elevated risk for intimate partner violence (IPV), but extant discourse fails to consider how this landscape amplifies disparities for Black women. This study examined the prevalence and associations of COVID-19 pandemic–specific coercive control and COVID-19–related stress among Black women experiencing IPV.
Methods:
Fifty-five Black women reporting past-year IPV participated in a prospective cohort study in 2020 and completed surveys on pandemic-specific coercive control, COVID-19–related stress, and sociodemographic characteristics. A subset of 15 participants completed semi-structured interviews in 2021. We conducted multivariable regression analyses to examine associations between coercive control and stress. We used interpretive phenomenological analysis to contextualize women’s experiences of coercive control and stress during the pandemic.
Results:
In the past 3 months, 76% (42 of 55) of women had a partner blame them for exposing them to COVID-19, 74% (41 of 55) had a partner minimize their pandemic concerns, and 52% (29 of 55) had a partner prevent them from getting a COVID-19 test. A higher average of pandemic-specific coercive control was associated with greater severity of COVID-19–related traumatic stress (b [SE] = 0.033 [0.009]; P = .001) and socioeconomic consequences related to COVID-19 (b [SE] = 0.019 [0.008]; P = .03). We identified 3 superordinate themes that illustrated Black women’s experiences: (1) coercive control, (2) pandemic-driven shifts in relational context, and (3) women’s structural and psychosocial stressors.
Conclusions:
Experiencing coercive control during the pandemic interfered with Black women’s engagement in preventive behaviors, which exacerbated distress. Intersectional public health efforts should address sociostructural and relational factors to prevent coercive control and stress among Black women experiencing IPV.
The social and economic consequences of the COVID-19 pandemic substantially affected the mental and behavioral health of Black women in the United States.1,2 In the early days of the pandemic in the United States, Black people were disproportionately burdened with COVID-19–related hospitalizations and deaths compared with people in other racial and ethnic groups.3-5 In particular, the COVID-19–specific mortality rate was higher among Black women than among both White women and White men. 6 Racial disparities in COVID-19–related hospitalizations and deaths were, in large part, driven by the legacy of structural racism and sexism. 7 Structural racism and sexism contributed to the overrepresentation of Black women in low-wage occupations and essential work industries,8,9 which placed Black women at disproportionate risk of viral exposure. 9 The racial disparity in COVID-19–related outcomes has also contributed to a greater severity of COVID-19 stress among Black people in the United States, 10 especially Black women. 11
State-sanctioned lockdown orders and shelter-in-place policies aimed to curtail transmission of the SARS-CoV-2 virus, 12 but these policies worsened economic self-sufficiency for Black women 9 and placed this population at elevated risk for intimate partner violence (IPV) and stress. First, as companies closed, Black women endured job loss and the highest unemployment rate during the pandemic. 13 Wage loss during the pandemic increased housing insecurity 14 ; Black women experience higher rates of eviction than women in other racial and ethnic groups. 15 Pandemic-driven economic vulnerabilities could financially strain a relationship and result in IPV.16,17 Social theories also suggest that IPV could increase if a male partner becomes unemployed, loses relationship power, and tries to regain power with violence.18,19 In addition to potentially escalating IPV, the lockdown orders also limited women’s ability to leave an abusive relationship. 20 Wage loss and unemployment reduced women’s economic reserves, which further derailed opportunities to leave the relationship. 20
Another consequence of the shelter-in-place policies was the influx of coercive control in relationships.21,22 Coercive control occurs in relationships when a partner uses isolation, exploitation, regulation, and deprivation to make a person be subordinate or dependent.21,22 With structural policies in place, abusive partners had more opportunities to exert coercive tactics to control and wield power in their relationship.16,21,22 The Battered Women’s Justice Project created a list of coercive control tactics related to the pandemic by using the Power and Control Wheel. 23
Coercive control is a serious concern, yet little attention has focused on Black women’s experiences of coercive control during the pandemic and its impact on COVID-19–related stress. The dearth of research addressing the pandemic, coercive control, and stress among Black women clearly delineates an intersectional invisibility. Intersectionality is a theoretical framework postulating that multiple marginalized identities at the micro-level can reflect interlocking systems of privilege and oppression at the macro-level (ie, racism, sexism, classism).24,25 As such, an intersectional invisibility acknowledges that when social discourse ignores the unique experiences of Black women, it can result in harm and inaction. 26 Therefore, the present study sought to assess the prevalence of coercive control and its association with COVID-19–related stress among Black women experiencing IPV and contextualize women’s experiences of coercive control and stress during the pandemic.
Methods
Study Overview
From November 2020 through June 2021, we recruited Black women in the United States experiencing IPV through flyers on social media nationally to participate in a 2-phase sequential explanatory mixed-methods study (QUANT QUAL). In the first phase, the research team asked participants to complete prospective cohort surveys that explored time-varying relationships between sociostructural stressors and physiological measures of stress. In the second phase, research team members conducted semi-structured interviews to elicit personal narratives of women’s experiences with IPV during the pandemic. Our mixed-methods analysis aimed to explain the quantitative results on coercive control and stress with our qualitative findings.
We considered women to be eligible if they (1) self-identified as a Black or African American cisgender female; (2) were aged 18-44 years; (3) had reported at least 1 incident of physical, sexual, or psychological IPV with a male partner in the past year; and (4) engaged in sexual activity with a male partner in the past 6 months. We screened participants for eligibility either on the telephone with a research team member or through a self-administered online survey. Eighty-nine participants were eligible, of whom 55 (62%) completed the baseline and follow-up surveys, 6 (7%) did not complete their baseline survey, 17 (19%) did not complete a pre-enrollment safety assessment, and 11 (12%) did not complete consent forms.
We obtained informed consent from 55 participants who completed baseline and 1-month follow-up surveys administered through Qualtrics. Each survey, which took about 40 minutes to complete, captured data on sociostructural stressors and mental health; the 1-month follow-up asked additional questions about resource utilization, technology use, and acceptability of wearable devices. After completing the follow-up survey, research team members invited participants to take part in a semi-structured interview; 15 participants agreed to participate. The research team developed the interview guide after a preliminary analysis of the baseline data. The interview guide contained questions about pandemic effects on women’s health, finances, and relationships. After each interview, the research team created analytical memos, and the interview debriefings occurred at weekly meetings. Interviews, which lasted about 60 minutes, were audio-recorded by a research team member, and a HIPAA-compliant company transcribed the interviews.
At the end of both the baseline and follow-up surveys, research team members remunerated participants with $55 and provided a list of community resources (eg, health clinics, domestic violence agencies). At the end of the interview, research team members remunerated participants with $25.
Ethics Approval and Consent to Participate
The ethics committees at Yale University (HIC#2000027381) and Johns Hopkins Bloomberg School of Public Health (institutional review board #13147) approved all experimental protocols and approved the procedures for verbal consent. The research team performed all methods according to the relevant guidelines and regulations and obtained verbal consent from all participants, who were informed that they could withdraw at any time. Verbal consent was appropriate for this study because sensitive information was collected, and the collection of a signature might have increased the risk for participants.
Quantitative Measures and Analysis
Coercive control during COVID-19
The research team developed a 25-item scale in the online survey that measured coercive control in the past 3 months. The research team used (1) the COVID-19 Coercive Control Wheel by the Battered Women’s Justice Project 23 and (2) the Revised Conflict Tactics Scale (CTS2) to create the 25-item scale. 27 To create the content for the scale, the research team extracted information from the COVID-19 Coercive Control Wheel (eg, screaming and yelling about COVID-19). 23 To develop the response options for the scale, the research team used the same response options from the CTS2 (ie, never, once, twice, 3-5 times, 6-10 times, 11-20 times, and >20 times in the past 6 months). 27 The research team created a scale that would assess coercive control perpetrated by a romantic and/or sexual partner. The research team recoded the responses according to the guidance in Straus and Douglas 28 (ie, 3-5 = 4; 6-10 = 8; 10-20 = 15; >20 = 25). Afterward, the research team summed all responses to create a total score; higher scores indicated greater coercive control during the pandemic. Cronbach α was 0.91.
COVID-19–related stress
The research team administered an online survey containing 2 subscales from the 36-item COVID Stress Scale, 29 which assessed COVID-19–related stress in the past week. The scale has 5 subscales 29 ; however, we used the fears about economic consequences and traumatic stress symptoms subscales. The response options for the scale ranged from 0 (never) to 4 (almost always). The research team summed all responses to create a total score for each subscale; higher scores indicated more stress related to the pandemic. Cronbach α for fears was 0.90 and for traumatic stress was 0.90.
Sociodemographic characteristics
Participants self-reported the following sociodemographic characteristics: age (in years); marital status (never married, married, divorced, widowed, separated); highest level of formal education completed (≤9th grade, 10th grade, 11th grade, finished high school, some college, finished college, some graduate school, and finished graduate school), sexual orientation (heterosexual, bisexual, gay or lesbian, prefer to self-describe), and employment (full-time, part-time, unemployed, not in workforce).
During the analysis phase, the research team calculated descriptive statistics (eg, means, frequencies) and correlations among continuous variables. Some responses were not selected by participants (eg, widowed); as a result, the research team did not include those responses in the final analysis. The research team also conducted linear regressions to examine associations between coercive control and COVID-19–related stress, while controlling for covariates. One response was missing for marital status, and responses were replaced with the mean value. The research team conducted all analyses in 2023 by using SPSS version 27 (IBM Corporation).
Qualitative Data Analysis
Research team members coded and analyzed semi-structured interviews into superordinate and subordinate themes by using an interpretative phenomenological approach. Interpretative phenomenological analysis aims to examine personal lived experiences and assess the meaning of the experience from participants. 30 An interdisciplinary team of 5 coders, including the interviewer (M.K.) and the principal investigators (PIs; T.C.W., T.K.), read and reread the transcripts multiple times before open coding a small subset of 2 interviews. The coders discussed, aggregated, and condensed codes in an iterative process to develop a codebook. The coders finalized the codebook on the basis of these discussions. Next, 3 coders coded the remaining transcripts using the finalized codebook. PIs and coders had discussions about inconsistencies in code application and interpretation and confirming and disconfirming cases. The PIs settled any discrepancies in code application. In the analysis phase, a PI met with the coding team to develop and summarize superordinate and subordinate themes and also discussed how participants might be interpreting these experiences. The PIs also extracted illustrative quotes for each of them based on participants’ reports of marital status and stress levels. PIs also extracted data on marital status and stress levels from the surveys. Specifically, the follow-up survey asked participants to answer the question: “How stressed are you about getting COVID-19?”; response options were “not at all stressed,” “slightly stressed,” “moderately stressed,” “very stressed,” and “extremely stressed.” These response options were mirrored from a study on stress and cortisol among women. 31 The coders coded all qualitative data, and the PIs analyzed the codes in 2023 by using Dedoose version 4.5 (Dedoose). The first author developed a convergent joint display to integrate quantitative and qualitative findings. The research team assigned pseudonyms to protect participants’ confidentiality.
We used 4 criteria of trustworthiness for our qualitative analysis: credibility, transferability, dependability, and confirmability.32,33 To increase credibility and dependability, we had prolonged engagement in the data (ie, multiple transcript reviews, intensive coding), conducted peer debriefings (ie, qualitative guidance from scholars who identified as Black women as well as scholars who have experienced IPV), and managed data triangulation (ie, interviews and surveys assessing similar constructs). To enhance transferability, the research team used purposive sampling to focus on key informants. To enhance confirmability, the PIs provided a thorough description of the research process.
Results
The study included 55 cohort participants and 15 interview participants (Table 1). The mean age of all participants was 29 (range, 20-42) years. Most participants had finished college (n = 27; 49.1%) or attended graduate school (n = 8; 14.5%), identified as heterosexual (n = 51; 92.7%), were employed full-time (n = 34; 61.8%), and were married (n = 29; 52.7%).
Characteristics of Black women experiencing intimate partner violence during the COVID-19 pandemic who participated in cohort surveys and semi-structured interviews, United States, 2020-2021

Values are number (percentage) unless otherwise indicated.
Data on marital status were missing for 1 participant.
Other categories were offered, but no one self-identified in these additional categories.
Coercive control was highly prevalent during the pandemic (Figure). The most prevalent coercive control behavior reported by participants was being monitored (87.3%), followed by being sworn at (83.6%), their partner spending money excessively (81.8%), their partner expecting sexual acts because of COVID-19–related circumstances (76.4%), and blaming them for COVID-19 exposure (76.4%).
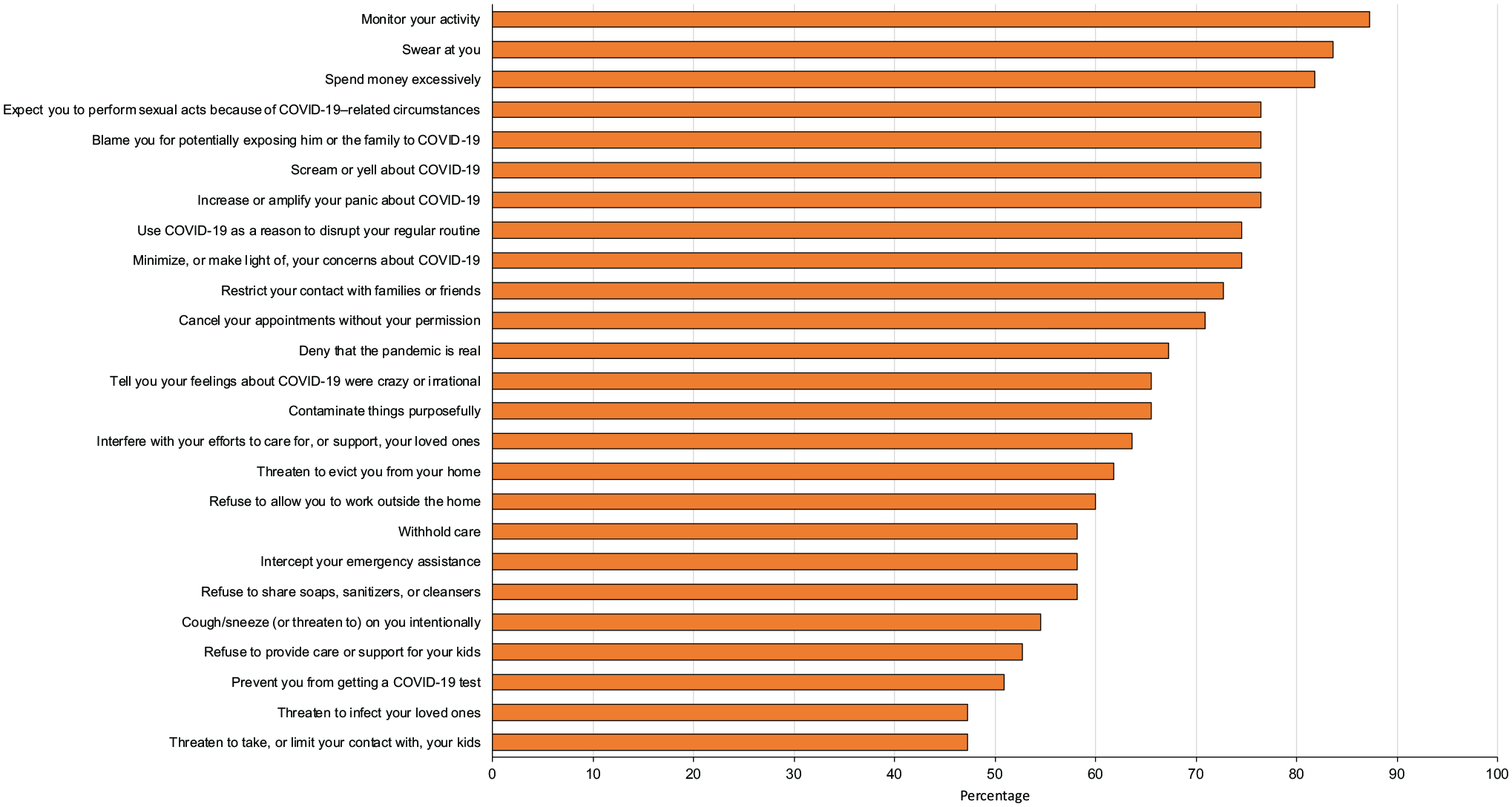
Prevalence of coercive control reported during the COVID-19 pandemic among Black women experiencing intimate partner violence in the United States, 2020-2021.
Coercive control was positively correlated with COVID-19–related traumatic stress (r = 0.54; P < .001) and COVID-19–related socioeconomic consequences (r = 0.44; P < .001).
Adjusted linear regressions indicated a positive association between coercive control and COVID-19–related traumatic stress (b = 0.033; SE = .009; P = .001) and COVID-19–related socioeconomic consequences (b = 0.019; SE = 0.008; P = .03; R2 = 30.2%) (Table 2).
Adjusted associations between coercive control and COVID-19 stress among Black women experiencing intimate partner violence who participated in a prospective cohort study, United States, 2020-2021

Multivariable associations were tested with linear regression; differences were determined by the Wald χ2 test, with P < .05 considered significant.
The PIs identified 3 superordinate qualitative themes that illustrated the experiences of Black women who experienced IPV during the pandemic: (1) coercive control, (2) pandemic-driven shifts in relational context and dynamics that lead to these coercive acts, and (3) their contributions to women’s stress (Table 3).
Representative qualitative quotes by theme among Black women who experienced intimate partner violence (IPV) during the COVID-19 pandemic and participated in semi-structured interviews, United States, 2020-2021
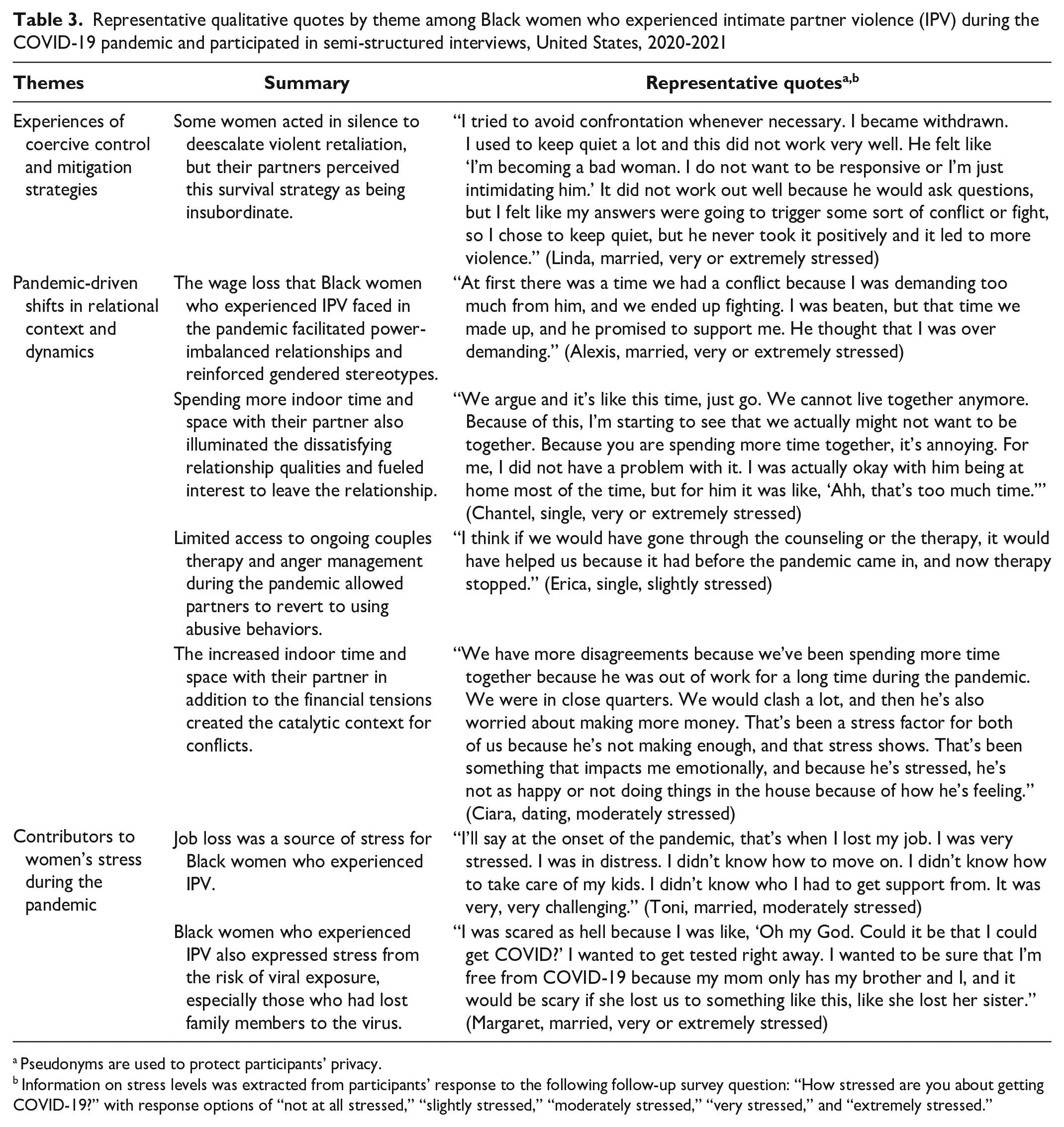
Pseudonyms are used to protect participants’ privacy.
Information on stress levels was extracted from participants’ response to the following follow-up survey question: “How stressed are you about getting COVID-19?” with response options of “not at all stressed,” “slightly stressed,” “moderately stressed,” “very stressed,” and “extremely stressed.”
Experiences of Coercive Control and Mitigation Strategies During the Pandemic
Black participants who experienced coercive control reported experiencing isolation, intimidation, and exertion of male privilege. One participant shared this: I was on my phone and he snatched it from me to confirm what I was doing and see if I was talking to another man. I was talking to my girlfriends, but he kept scrolling through my messages. That was disturbing. It was invading my privacy. I asked him to give me my phone back. He said, ‘No, I cannot give it to you.’ He threw it down and the phone cracked. (Chantel, single, very or extremely stressed)
Partners also used minimizing, denying, and blaming tactics. Abusive partners would blame Black women for spreading COVID-19: “I’ve been blamed for a lot of things during the pandemic. He tends to make it like it’s my fault. He has accused me of the virus” (Bianca, married, moderately stressed). State-sanctioned measures to control the pandemic shifted power dynamics, and partners used COVID-19 for control. Some partners minimized IPV survivors’ pandemic concerns: He would not think it was serious to keep a mask on when he was around his friends because he felt like it was not real. I’m like, “Whether you feel like this is real or not, you got to come back to your family. You need to protect yourself while you’re out there.” He felt like I was being dramatic and this is a fake virus. We had lots of arguments about that. (Ciara, dating, moderately stressed)
Abusive partners denied and minimized Black women’s concerns about the pandemic, which made them feel unsafe and uncertain about their risk of viral exposure.
Pandemic-Driven Shifts in Relational Context and Dynamics
Black women who experienced IPV discussed how pandemic-related sociostructural factors affected their relationship. Black survivors noted that they experienced wage loss because of the influx of underemployment and unemployment during the pandemic. One participant said, The negative part is when I lost my job, I did not have any income. I was in debt to him. When you’re depending on a man, they become violent. While they would give the finances, they feel like you’re misusing money and you feel like things are not going well. . . . I asked for money, and he felt that I’m misusing the money. We quarreled, and he slapped me. (Monica, married, very or extremely stressed)
The pandemic facilitated economic dependence but also constrained Black women’s responses to violence. For example, 1 participant shared, The minute you’re not able to support yourself and you’re dependent on somebody else, you become vulnerable. When somebody shouts at you, you’re not able to shout back. When you have your own finances, able to support yourself, it’s easy to ignore that person and move on because, at the end of the day, you’re able to support yourself. The moment that you’re not able to support yourself, you’re at the mercy of that person. (Kori, married, very or extremely stressed)
The relationship power became unbalanced because the partner had more power due to his finances.
Contributors to Women’s Stress During the Pandemic
Coercive control contributed to Black women’s stress during the pandemic. For example, Kori (married, very or extremely stressed) said, “It’s kind of stressing because you do not feel free. You feel under pressure. You’re being controlled. You’re being monitored.”
Black women who experienced IPV in this study also experienced stress from employment and workplace settings. While trying to find employment during the pandemic, survivors discussed sociostructural stressors. Monica shared the following: It’s not easy because of racism and discrimination. A Black woman works twice as hard as the White woman to survive. Racism is very common, and you’re discriminated in workplaces. Once you’re discriminated, you do not get those jobs, so your income becomes lower. Managing your finances becomes a very big burden, and it affects you mentally. Sometimes, you get a job, and then the work environment is unfriendly because of discrimination and racism. You feel uncomfortable working, and you prefer not to work because you’re stressed. (Married, very or extremely stressed)
Black women who experienced IPV also experienced discrimination during the pandemic while searching for employment.
Integrated Results
The quantitative and qualitative findings were integrated in a convergent joint display (Table 4).
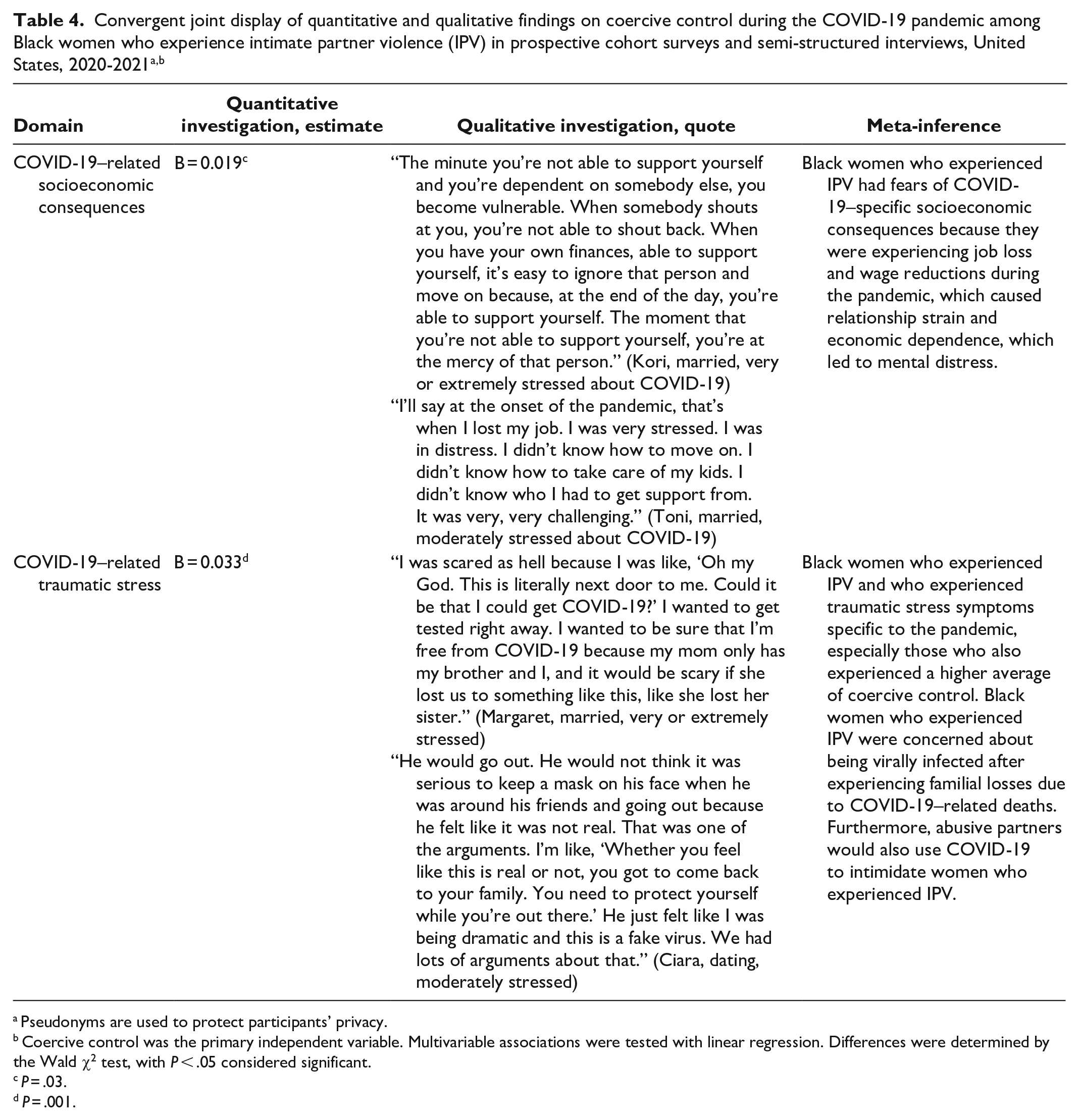
Pseudonyms are used to protect participants’ privacy.
Coercive control was the primary independent variable. Multivariable associations were tested with linear regression. Differences were determined by the Wald χ2 test, with P < .05 considered significant.
P = .03.
P = .001.
Discussion
Overall, Black women who experience IPV represent an intersectional invisibility in discourse addressing IPV and mental health during the COVID-19 pandemic. Using an intersectional lens, our findings illustrate how racism, sexism, and classism uniquely influence Black women’s experiences of IPV and stress during the pandemic.
The lockdown orders and economic aftermath of the pandemic contributed to the onset of coercive control and exacerbated women’s fears about socioeconomic consequences of the pandemic. The quantitative results showed that more coercive control trended with more fears about the socioeconomic effects of the pandemic. Moreover, in the qualitative findings, Black women who experienced IPV shared that they experienced unemployment and wage loss during the pandemic and, as a result, had to financially rely on their partner. Financial tensions often led to violence in the relationship, and Black women survivors had to self-silence their responses because of the economic dependence. Furthermore, job-seeking Black women who experienced IPV dealt with employment and workplace discrimination during the pandemic. These findings align with evidence on unemployment among Black women during the pandemic 9 in addition to resource theories on violence escalation. 20 The stress from discrimination might be more pronounced during the pandemic given the economic vulnerabilities survivors were navigating. Conversely, an intersectional lens suggests that the economic effects of the pandemic reinforced gender norms because women who experienced IPV felt obliged to suppress their emotions to avoid conflict,34,35 which increased mental distress among Black women.36,37 Employment and workplace discrimination also prevent Black women who experience IPV from accessing high-wage jobs, 9 reinforcing occupation segregation, 37 and reducing their chances of leaving an abusive relationship because of low economic resources. Organizations should develop and implement culturally responsive practices that address the systemic barriers Black women who experience IPV face when leaving abusive relationships and seeking employment.
Experiences of coercive control also trended with more traumatic stress symptoms related to the pandemic, whereas the qualitative findings indicate that isolation, regulation, and exploitation contributed to women’s stress. Consistent with prior research,16,21,22 Black women who experienced IPV experienced isolation, minimizing, blaming, and emotionally abusive tactics from their partner, which included blaming survivors for viral exposure and preventing survivors from using a COVID-19 test. Black women who experienced IPV shared that coercive control made them feel unsafe and increased their concern about being infected during the pandemic. Abusive partners who minimized the importance of preventive behaviors placed women who experienced IPV and their children at risk for viral exposure. On the other hand, an intersectional lens proposes that Black women who experience IPV are at elevated risk for COVID-19 because of the confluence of structural racism, sexism, and pandemic-related coercive control. Consistent with prior research, 9 structural racism and sexism put Black women at disproportionate risk of viral exposure, but having a partner who perpetrates coercive control exacerbates an already disproportionate risk. As a result, shelter-in-place policies are insufficient to prevent COVID-19 transmission and may inadvertently increase viral exposure for Black women who experience IPV because the orders prevented mobility. National leadership should develop alternative strategies to mitigate viral transmission for Black women who experience IPV who are at the intersections of multiple systems of oppression, such as racism and sexism. Similarly, in the event of another outbreak, standardized protocols should be created for survivors needing to leave their relationship safely and access support services.
Limitations
Our findings had several limitations. First, the data did not allow causal inferences. Second, study variables were self-reported; as such, they were susceptible to social desirability bias, and, thus, coercive control might be underreported. Third, while the study was powered for adjusted regressions, our sample precludes complex analyses to assess intracategorical intersectionality with moderation or interaction terms. Fourth, our findings are mainly generalizable to Black women with at least a high school education. To improve external validity, future studies should use different strategies to recruit Black women with less than a high school education. Fifth, this study centered on Black cisgender women’s experiences during the pandemic in the United States. Thus, these findings may not be transferable to Black lesbian, bisexual, and transgender women nor Black women in other countries.
Conclusions
To our knowledge, this is one of the first studies to integrate quantitative and qualitative findings that document and contextualize the experiences of Black women who experience IPV to address how sociostructural risk factors contribute to IPV risk. Future studies and strategies should take an intersectional and equity lens to understand how emergency responses and policies affect IPV among Black women.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: T.C.W. was supported by the National Institute on Minority Health and Health Disparities via K01MD015005 and L32MD016555 and the National Institute on Drug Abuse via R25-DA035692. The funding bodies did not play a role in the design of the study and collection, analysis, or interpretation of data or in writing the article.
Availability of Data and Materials
The data generated and/or analyzed during the study are not publicly available because they contain information that could compromise participant privacy and/or consent. The corresponding author can be contacted for follow-up questions and/or concerns.