
Abstract
Background
Despite the recognized importance of postnatal care, utilization of postnatal care services remains markedly low in Ethiopia, particularly in rural areas.
Objective
This study aims to identify the multilevel determinants of postnatal care (PNC) service utilization among rural women in Ethiopia using a multilevel analysis of secondary data from the Ethiopian Demographic and Health Survey (EDHS-2019).
Methods
This study utilized secondary data from the 2019 EDHS. The study population included 2,900 (weighted sample) of 15-49 years women residing in rural areas of Ethiopia who had experienced at least one birth. The data were analyzed using Stata version 17 software. A multilevel mixed-effects logistic regression model was employed to identity the independent determinants by using adjusted odds ratio with 95% CI (p-value <0.05). Model diagnostics were done to assess the goodness-of-fit and validity of the regression model by AIC, BIC, ICC and the log-likelihood ratio test.
Results
Among 2,900 women, only 283 (9.7%) sought postnatal care (PNC) services within the first six weeks after delivery. Several determinants of PNC service utilization at the individual level were identified, including being in the middle wealth index (AOR=1.48[1.04, 2.14]), having fewer than four antenatal care visits (AOR=2.17[1.66, 2.82]), having an institutional delivery (AOR=1.42[1.08, 1.89]), delivering via cesarean section (AOR= 1.60[1.01, 2.57]), having a third birth order (AOR=1.54[1.09, 2.19]), having a birth order of four or more (AOR=1.77[1.18, 2.69]) and being informed about family planning methods (AOR=3.67[1.51, 9.39]).
Conclusions
The findings of this study showed that in rural Ethiopia, socio-economic, maternal and health facility-related factors are significant determinants of PNC service utilization. Therefore, addressing individual-level factors such as socio-economic status, ANC attendance, delivery location, birth order, and awareness of family planning methods is essential to enhance the uptake of PNC services in these areas.
Introduction
Postnatal care (PNC) service utilization is a critical aspect of maternal and child health, particularly in rural areas of Ethiopia. Postnatal care (PNC) is a vital intervention to improve maternal and child health outcomes, especially in the first 42 days after delivery.1–3 However, PNC service utilization remains low in Ethiopia, despite the efforts of the government and its partners to increase access and quality of maternal and child health services.2,4–6
Evidence over the past few decades has shown a gradual increase in the utilization of postnatal care (PNC) services globally, reflecting growing awareness of the importance of maternal health in the postpartum period. In Ethiopia, however, the Ethiopian Demographic and Health Survey (DHS) of 2016 reported that only 17% of women received PNC within the recommended timeframe, which is within the first 42 days after delivery.2,3,7 This figure is far below the target for optimal PNC utilization, highlighting a significant gap between the recommended guidelines for postnatal care and the actual uptake of services.2–7
This discrepancy is particularly pronounced in rural areas, where access to healthcare facilities and trained professionals remains limited. Factors such as long distances to health centers, financial constraints, lack of transportation, and limited awareness about the benefits of timely postnatal care contribute to low utilization rates.3–7 Moreover, cultural practices and perceptions about maternal health may also influence women’s decisions to seek care after delivery, often leading to delays or complete avoidance of PNC services. The low utilization rate of PNC within the recommended timeframe underscores the need for targeted interventions aimed at increasing accessibility and awareness, as well as addressing socio-economic and logistical barriers, particularly in underserved rural regions.3,5,7
Several factors have been identified as influencing PNC utilization in rural Ethiopia, including obstetric, health service-related, and region of residence.2,4,5,8 Additionally, the previous study highlighted the need for a comprehensive intervention package to improve PNC coverage, taking into account the perspectives of women and the acceptability and feasibility of PNC services. 4
While some studies have identified determinants of PNC utilization, there is a lack of comprehensive, multilevel analyses specifically focused on rural areas and the unique determinants affecting PNC service utilization among this population. Therefore, this study aimed to fill this gap by conducting a multilevel analysis of the determinants of PNC service utilization among women of reproductive age in rural Ethiopia.
The findings of this study will have remarkable implications for policy and program development in Ethiopia. By understanding and addressing the determinants of PNC service utilization, policymakers, and program implementers can develop targeted interventions to improve PNC coverage and maternal health outcomes in rural Ethiopia. The study will also contribute to the existing literature on PNC service utilization in Ethiopia, particularly in rural areas.
Methods
Study design
In 2019 cross-sectional study was conducted by the Central Statistical Agency (CSA).
Study population and data sources
The national survey was conducted among 8,855 women of reproductive age (15–49 years). 8 The 2019 Ethiopia Mini Demographic and Health Survey (EDHS) is the second EDHS and the fifth DHS implemented in Ethiopia. The Ethiopian Public Health Institute (EPHI) conducted the survey in collaboration with the Central Statistical Agency (CSA) and the Federal Ministry of Health (FMoH), and other partners. The 2019 EDHS generates data for measuring the progress of the health sector goals set under the Growth and Transformation Plan (GTP), which is closely aligned with the Sustainable Development Goals (SDG). The survey was conducted from 21 March 2019 to 28 June 2019 based on a nationally representative sample that provided estimates at the national and regional levels and for urban and rural areas.
Sampling procedure
The sampling frame used for the 2019 EDHS is a frame of all census enumeration areas (EAs) created for the 2019 Ethiopia Population and Housing Census (EPHC) and conducted by the Central Statistical Agency (CSA). The census frame is a complete list of the 149,093 EAs created for the 2019 EPHC. Administratively, Ethiopia is divided into nine geographical regions and two administrative cities. The 2019 EDHS was a population-based cross-sectional study with a two-stage stratified cluster sampling design. Each region was stratified into urban and rural areas, yielding 21 sampling strata. Samples of EAs were selected independently in each stratum in two stages. A household listing operation was carried out in all selected EAs and the resulting lists of households served as a sampling frame for the selection of households. In all selected households’ women aged 15–49 were interviewed using the Woman’s Questionnaire. 8
For this study, women aged 15–49 years who resided in rural Ethiopia, had experienced at least one birth, and had complete data were selected from the mini-EDHS dataset. Finally, a weighted sample of 2,900 women was included to identify determinants of postnatal care utilization.
Definition of term
In this study, the utilization of postnatal care (PNC) services is defined as a woman receiving at least one postnatal care visit within the first six weeks following childbirth, either after being discharged from a healthcare facility or in the case of a home delivery as reported in the EDHS.
Inclusion and exclusion criteria
Women in the reproductive age (15–49 years), resided in rural area, had at least one live birth in the past five years before the survey and had complete data on key variables were included in to the study while women with no recent birth, urban residents, and those with missing or incomplete data were excluded.
Data management and extraction process
Stata version 17 was used for data extracting, processing, and analysis. The weighting of the data was done according to the recommendation from the 2018 Guideline to DHS statistics, and all the statistical analyses were done using the weighted data. Some variables that have many missing values such as awareness of danger sign, counselling during pregnancy were omitted from analysis, after the impact of missing data on the analysis was assessed.
For this study, first relevant individual and community-level variables were identified from the EDHS dataset. Next, the data was filtered to include only women who had experienced at least one birth within the last five years and were residing in rural areas of Ethiopia. The selected variables were then extracted and organized into a separate dataset for analysis. Finally, the completeness and accuracy of the extracted data were thoroughly checked, and any missing or inconsistent values were addressed using appropriate data cleaning techniques to ensure the integrity of the dataset for further analysis.
Framework/model of analysis
This study is based on the multilevel framework that postnatal care (PNC) utilization is influenced by individual and community factors. Individual factors include socio-demographic and obstetric characteristics including age, education, wealth status, antenatal care attendance, place and mode of delivery, birth order and knowledge of family planning and danger signs. Community-level factors include where people live (region and rural–urban setting) that influence access to health services via differences in infrastructure and contextual conditions. The factors influence the use of a multilevel analysis to account for the hierarchical nature of the data.
Data processing and analysis
Model diagnostics was conducted to assess the goodness-of-fit and validity of the regression model. In the beginning, a null model (a random intercept only model by excluding all other explanatory variables) was fitted to test whether or not grouping variable (region of residence) has an effect on PNC utilization at individual level. The result showed that there is variability between regions and was decided for the multilevel logistic regression model for analysis. Multicollinearity among continuous variables was assessed using variance inflation factors (VIF), and variables with VIF values greater than 10 were excluded. For final fitted multilevel logistic regression model, the lowest value of AIC, BIC was considered. Additionally, ICC and the log-likelihood ratio test was tested to assess model fitness.
The 2019 Mini Ethiopian Demographic and Health Survey was a two-stage stratified cluster sampling design that followed a hierarchical sampling technique where women are nested in households, the households are nested in enumeration areas, the enumeration areas are nested in the types of places of residence and the types of places of residence is nested in the regions. A multilevel logistic regression analysis was employed to identify independent determinants of PNC utilization, accounting for the hierarchical structure of the data (individuals nested within communities). First, bivariable mixed-effects logistic regression analyses was done to assess the association between the independent variables and the dependent variable of the study. The overall categorical variables with a p-value <0.25 in bivariable analysis were included in the final model of the Multilevel logistic regression model in which odds ratio with 95% confidence intervals were estimated to identify the independent variables of postnatal check-ups. P-values less than 0.05 were employed to declare statistical significance. Fixed effect and random effects were calculated to assess the individual and regional variations respectively.
Ethical considerations
The data for this study were obtained from the 2019 EDHS archive data (https://dhsprogram.com/publications/index.cfm) following an appropriate request and with official permission. The EDHS data were collected following all the necessary ethical procedures in accordance with the relevant guidelines and regulations. The DHS program is authorized to distribute, free of charge for legitimate academic research.
Results
Socio-economic characteristics of 15-49-year-old women living in rural areas of Ethiopia and experienced at least one birth (n=2900).

Obstetric characteristics of 15-49-year-old women living in rural areas of Ethiopia (n=2900).
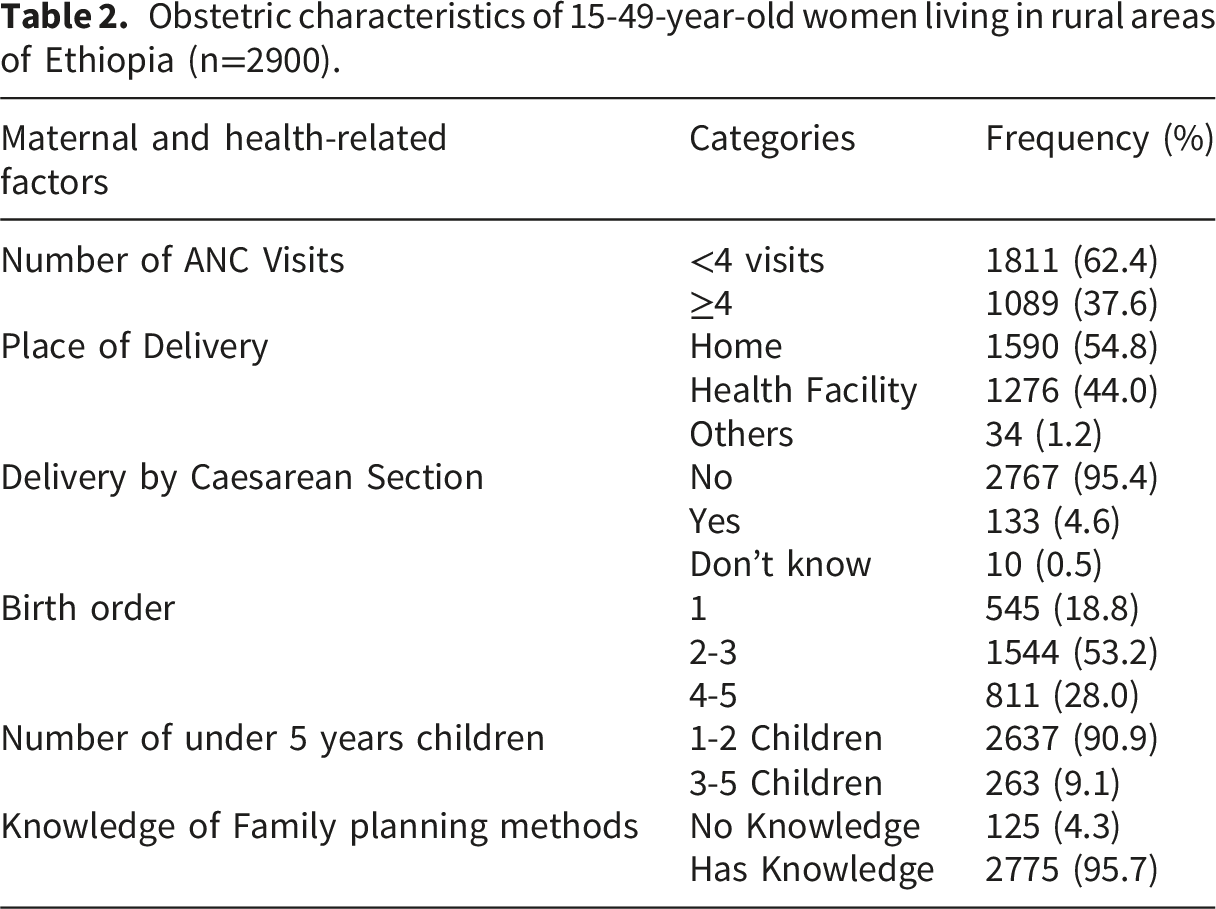
The study indicates that the overall utilization of PNC services among women aged 15-49 in rural Ethiopia is 283 (9.7%). This utilization rate specifically refers to PNC services accessed within the first six weeks (42 days) of delivery after discharge or home delivery (Figure 1). Postnatal care service utilization of 15-49-year-old women in rural Ethiopia.
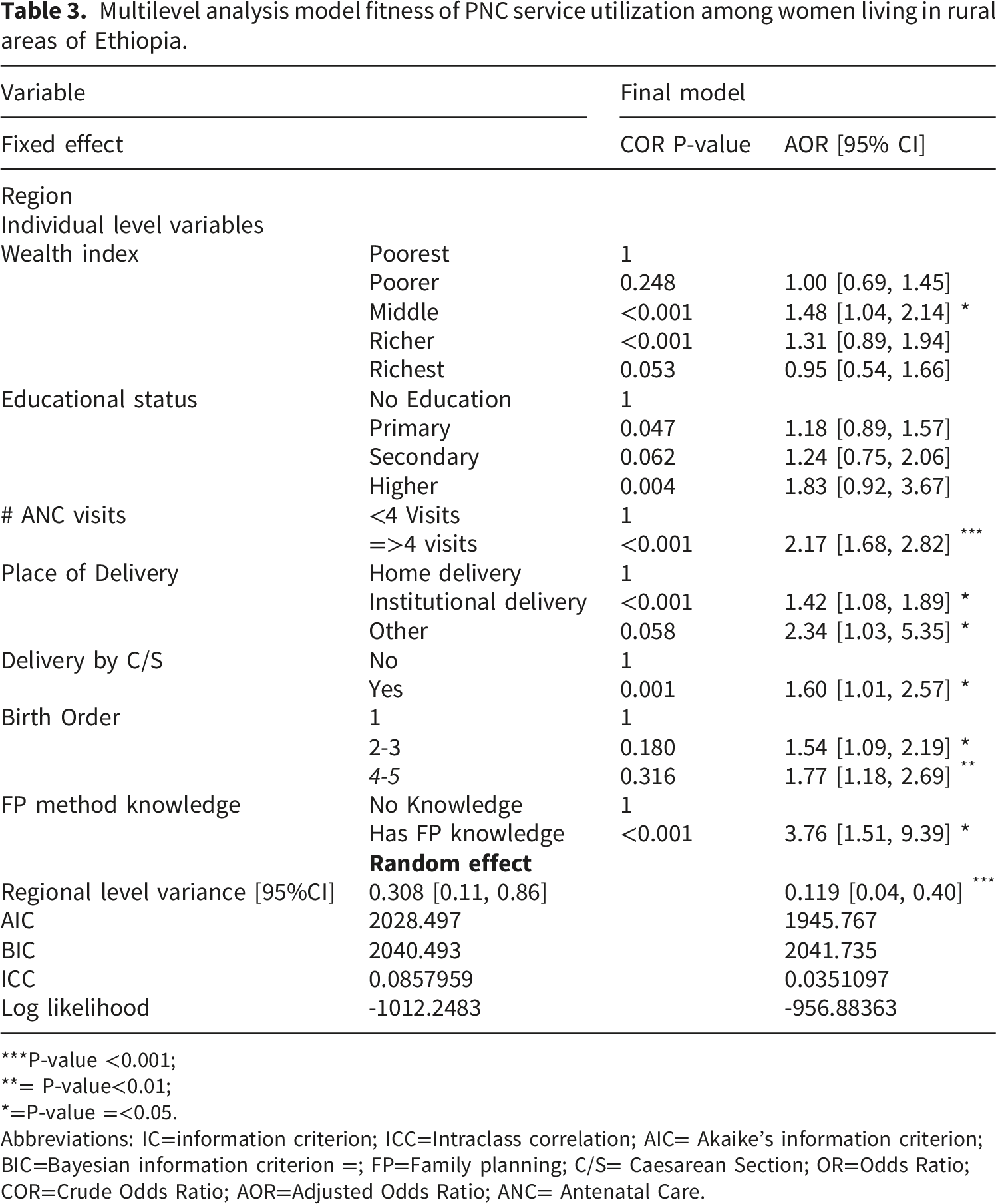
In this study, a multilevel logistic regression analysis was conducted to assess the fitness of the model for predicting PNC (Postnatal Care) service utilization using region as a grouping variable. The random intercept (Model 1/null model) log-likelihood ratio test strongly favored multilevel logistic regression analysis, with a P-value of less than 0.001. This indicates that there is sufficient variability among the eleven regions in rural areas of Ethiopia, suggesting the appropriateness of the multilevel approach. Given the hierarchical nature of the data, only region was used as a community-level variable. Several individual-level candidate predictor variables were considered for multilevel analysis, including wealth index, educational status, number of ANC visits, place of delivery, delivery by cesarean section, birth order, and knowledge of family planning methods. From these variables, six were found to have a significant association with PNC service utilization.
The study findings revealed that women in the middle wealth index category were 1.48 times more likely to utilize PNC services compared to women in the poorest wealth index category (AOR=1.48, [1.04, 2.14]). Additionally, women who had four or more ANC visits were 2.17 times more likely to utilize PNC services compared to those with fewer than four ANC visits (AOR=2.17, [1.68, 2.82]), highlighting the number of ANC visits as the strongest predictor.
Regarding the place of delivery, women who gave birth at a health institution were 1.42 times more likely to utilize PNC services compared to those who gave birth at home (AOR=1.42[1.08, 1.89]). Women who gave birth by cesarean section were 1.6 times more likely to utilize PNC services compared to those who gave birth without cesarean section (AOR=1.60 [1.01, 2.57]) as well. Additionally, women with a child in the second or third birth order were 1.54 times more likely to use PNC services compared to those with a firstborn child (AOR = 1.54 [1.10, 2.19]). Similarly, women with a child in the fourth birth order or higher were 1.77 times more likely to utilize PNC services compared to those with a firstborn child (AOR=1.77 [1.18, 2.69]). Furthermore, women who reported knowing about family planning methods were 3.76 times more likely to utilize PNC services compared to those who lacked this knowledge (AOR = 3.67 [1.51, 9.40]).
Multilevel analysis model fitness of PNC service utilization among women living in rural areas of Ethiopia.
***P-value <0.001;
**= P-value<0.01;
*=P-value =<0.05.
Abbreviations: IC=information criterion; ICC=Intraclass correlation; AIC= Akaike’s information criterion; BIC=Bayesian information criterion =; FP=Family planning; C/S= Caesarean Section; OR=Odds Ratio; COR=Crude Odds Ratio; AOR=Adjusted Odds Ratio; ANC= Antenatal Care.
Discussion
The study found that the utilization of postnatal care (PNC) services among women aged 15-49 years within six weeks of delivery in Ethiopia was 9.7%. This finding is consistent with a similar study conducted in Tigray, which reported an 8% utilization rate. 9 The similarity in these findings may be due to shared socio-demographic factors across regions.
Understanding both individual and community-level characteristics of rural women in Ethiopia is essential for designing targeted interventions to improve maternal and child health during the postnatal period. By using a multilevel mixed-effects model, this study was able to identify key determinants of PNC service utilization at both the individual and regional levels, providing valuable insights for developing more effective health interventions in rural areas. The findings of this study indicate that women in the middle wealth index category were more likely to utilize PNC services after discharge or home delivery compared to those in the poorest wealth index category. This is consistent with previous research, including a study conducted in four Sub-Saharan African countries, which found that women from middle-income families were more likely to use PNC services.10,11 The greater utilization among women in the middle wealth index category may be attributed to factors such as improved access to healthcare, better financial stability, and greater ability to afford transportation or healthcare fees. In contrast, women in the poorest wealth category may face significant barriers, such as financial constraints, limited access to healthcare facilities, and other socio-economic challenges, which hinder their ability to seek timely postnatal care.8,10,11
The findings of this study show that women who had four or more antenatal care (ANC) visits were more likely to utilize postnatal care (PNC) services compared to those with fewer than four ANC visits. This result aligns with a study conducted in Malawi, which also found a positive association between the number of ANC visits and PNC utilization.12,13 The similarity in these findings may be due to comparable patterns in healthcare utilization among the study populations. Women who attend more ANC visits are likely to be more engaged with the healthcare system, which increases their awareness of the importance of postnatal care and may also provide them with the necessary information and resources to access PNC services after delivery. This highlights the critical role of comprehensive antenatal care in promoting timely and appropriate postnatal care utilization.
This study found that women who gave birth at a health institution were more likely to utilize postnatal care (PNC) services, a finding that is consistent with a previous study conducted in Debremarkos. 14 However, this result contrasts with a study done in Ethiopia), which reported a weaker association between place of birth and PNC utilization in Ethiopia. The discrepancy in findings may be due to differences in how place of birth was considered in the analysis. In contrast, the current study focused on individual-level factors, which may better capture the direct influence of institutional delivery on PNC service use. This highlights the importance of considering the level at which variables are analyzed when assessing health service utilization patterns.
The study also found that women who gave birth via cesarean section were more likely to utilize postnatal care (PNC) services, which is consistent with a previous study conducted in Ethiopia.8,9,14 However, the association observed in this study is stronger compared to studies conducted in Malawi in 2019 and in northern Ethiopia. This difference may be attributed to methodological variations, such as smaller sample sizes in the latter studies, which may have limited their ability to detect a true effect. Smaller sample sizes can lead to less precise estimates, making it harder to identify significant associations. Therefore, the larger sample size in the current study may provide a more accurate representation of the relationship between cesarean section delivery and PNC utilization.
In addition, women with second or third-born children were more likely to utilize postnatal care (PNC) services, which contrasts with a study conducted in Malawi. 12 This discrepancy may be due to geographical and temporal differences between the two studies. Variations in healthcare systems, cultural practices, and access to services in different regions could influence maternal health behaviors, including PNC utilization. Furthermore, differences in the time periods of the studies may reflect changes in healthcare policies or interventions, which could also impact utilization patterns.
Moreover, women who were knowledgeable about family planning (FP) methods were more likely to utilize postnatal care (PNC) services compared to those without such knowledge. This finding aligns with a study conducted in Ethiopia,15–17 suggesting that there may be similarities in the study populations and in patterns of health service utilization. Women who are informed about family planning are generally more engaged with the healthcare system, which could increase their likelihood of seeking other health services, including PNC. The shared trends in both studies highlight the importance of health education and awareness in promoting broader utilization of maternal health services.18–24
Study limitations and strengths
The study has some limitations that should be considered when interpreting the findings. Firstly, the data used in the study relies on self-reported health service utilization, which may be subject to recall bias. Secondly, the study is based on cross-sectional data from the mini-EDHS 2019, which limits the ability to establish causal relationships between the predictors and PNC service utilization. Longitudinal studies would provide more robust evidence on the temporal relationship between these factor and PNC utilization. Some important predictors were also excluded due to the large number of missing data.
Despite these limitations, the study also has notable strengths. The use of national survey data and a large sample size enhances the generalizability of the findings at the national and regional levels in Ethiopia. On top of that, the study utilizes advanced analysis techniques (Multilevel analysis) to examine PNC coverage, which contributes to a more comprehensive understanding of the factors influencing PNC service utilization. The findings of this study can guide practitioners and policymakers in developing targeted interventions to increase PNC utilization among rural women. Further research is needed to address the limitations and expand our understanding of the barriers and facilitators of PNC service utilization in different contexts.
The study found low postnatal care (9.7%) utilization in rural part of Ethiopia which indicates a major gap in maternal health services. The key determinants of postnatal care are antenatal care attendance, place and mode of delivery, birth order and family planning knowledge, highlighting the importance of integrated maternal health services and targeted health education. The regional variations also shows the need for context-specific interventions. Generally, strengthening ANC, promoting facility-based delivery, and addressing socioeconomic and geographic barriers are essential to improve PNC utilization and maternal and neonatal health outcomes in rural Ethiopia.
This study can fill a key gap in evidence on postnatal care utilization in the rural part of Ethiopia by providing a multilevel analysis of nationally representative data. Unlike previous studies, it considers both individual and community-level determinants within a hierarchical framework.
Conclusion
In conclusion, this study identifies key factors influencing postnatal care (PNC) utilization in Ethiopia, including socioeconomic status, antenatal care (ANC) visits, place and mode of delivery, birth order, and family planning knowledge. These findings emphasize the need for targeted interventions to overcome barriers to PNC access, especially in rural areas. Improving access to quality ANC, facility-based deliveries, and timely PNC services is essential for better maternal and child health outcomes. Collaboration among policymakers, healthcare providers, and communities is vital to ensuring all women, particularly in rural Ethiopia, have access to essential PNC services, ultimately promoting better health for mothers and children.
Footnotes
Acknowledgements
First, we would like to thank the Heavenly God. Next, we want to thank Jimma University, College of Health Sciences and faculty of Public Health for giving us the chance to develop this manuscript. Lastly, but certainly not least, we would like to thank EDHS data center for their permission and licensing data-extraction for this study.
Ethical considerations
EDHS addressed all ethical issues during the actual data collection. The study participants name was not shared by EDHS data center though it was collected during the primary data collection. The authors extracted (![]() ) and used the data for the purpose of developing this manuscript and didn’t share it to third party.
) and used the data for the purpose of developing this manuscript and didn’t share it to third party.
Author contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.