
Abstract
Background:
A high rate of unintended pregnancy is said to be driving population growth, particularly in Sub-Saharan Africa, where approximately half of all pregnancies are unintended, coming too soon or even unwanted. Most of these unintended pregnancies could have been prevented with effective family planning services. There, however, remains an unmet gap between the women’s reproductive intention and their contraceptive behaviour.
Objectives:
This study determined the prevalence of unmet needs for family planning and examined its determinants among women of reproductive age group at a tertiary health facility in Southwest Nigeria.
Design:
This was a hospital-based cross-sectional study.
Methods:
Two hundred eighty-five sexually active women were recruited using a pre-tested, semi-structured, validated, interviewer-administered questionnaire. The questionnaire assessed the respondent’s socio-demographic characteristics, obstetrics and gynaecological history, and contraceptive history. Relevant clinical parameters were measured and recorded. Data were analysed using SPSS version 21. Multivariable logistic regression analysis was done using a 5% significance level to identify the determinants of unmet needs for family planning.
Results:
The prevalence of unmet family planning needs for prevention, spacing and limiting were 28.8%, 33.1% and 38.1%, respectively, with 58.2% overall prevalence of unmet needs. The commonest reason for the non-uptake of contraceptives among those with unmet need was the fear of side effects (66.3%). The odds of having unmet needs for family planning were higher for respondents with four or fewer children (adjusted odds ratio (AOR): 7.731; 95% confidence interval (CI): 28.504–2.907, p = 0.002) and those with one partner (AOR: 2.008; 95% CI: 3.669–1.090, p = 0.025).
Conclusion:
A high rate of unmet family planning needs was found in the study. This requires specific interventions and policies towards increasing contraceptive uptake, such as intensified health education aimed at allaying fears related to the side effects.
Introduction
Unmet family planning (FP) needs refer to the magnitude of sexually active females who desire to halt or defer childbirth but are not employing an effective method to prevent conception.1,2 According to the World Health Organization (WHO) 3 statistics, nearly 21 million young ladies aged 15–19 years get pregnant each year in developing nations, about 49% of which are unintended. Fortunately, when properly used, contraptives reduce unwanted conceptions, high gestation and therefore, maternal death rate. 4
Roughly, 6.8 million unwanted conceptions take place in Nigeria every year. 5 Thus, considerable knowledge of the obstacles to birth control is required to tackle this challenge. 6 In a review by Wulifan et al. 1 among females of child-bearing age in developing nations, they found unsatisfied needs for FP ranging between 20% and 58%. The highest rates of unmet needs were seen in ladies who reside in sub-Saharan Africa. 7 A previous local study by Anate et al. 8 in Southwestern Nigeria reported that only 38.5% of the respondents who required modern FP methods in their first postnatal year actually used one, leaving 61.5% unmet needs.
Factors contributing to unmet needs included poor inter-spousal conversation about the wanted number of progeny and the partner’s resistance to birth control method utilisation.7,9 A study done in sub-Saharan Africa found that there was poor involvement of men in the FP decision. 10 Spousal communication helped in the uptake of FP.9,10 Sufficient evidence exists that family functionality influences contraceptive use in women. 11 Findings by Kao and Manczak 12 imply that young persons’ cultural heritage, parents’ unfavourable position and household relations are important indicators for contraceptive utilisation in youth. In a study by Clark et al. 13 in Jordan, it was noted that intimate spousal aggression (ISA) exaggerated the likelihood of unsatisfied needs for contraception by 87% and 76% in females who wedded before and after the age of 18 years, respectively. A study by Adeleye et al. in Lagos revealed that most responders (56.5%) reported functional family support, while 14.5% reported seriously dysfunctional family support. The participants had statistically significant contraceptive uptake as the majority of them had functional family support. 14
Several other factors have been associated with unmet needs from different studies.15,16 These studies have found that total unmet needs were significantly associated with the number of years at the earliest union, the total of children alive, child death occurrence, educational status of spouse and environment. 16 Partner’s dislike, fearfulness of untoward consequences, spiritual notion and poor access were the principal rationality for not adopting birth control measures in the study by Anthony et al. 17 in South-Eastern Nigeria. These factors must be relentlessly tackled if the country will meet up with the Sustainable Development Goals (SDGs) target 3.7 which aims to ensure universal access to reproductive health services including FP by 2030.18,19
Over the years, Nigeria has put in place policies and programmes aimed at improving access to and uptake of contraceptives. 19 The Nigerian Government provides FP commodities at no cost, but bureaucratic barriers and an inefficient supply chain, especially at the state and local government levels, impair access by the end-users. These, in addition to several consumer-level factors, affect FP uptake. 19 Recently, in 2021, there was the launch of the Nigeria FP 2030 commitments which envisioned universal, equitable and affordable access to quality FP. One of the aims is to increase FP uptake from the prevailing contraceptive prevalence rate (CPR) of 12% to at least 27% by the year 2030, through increase in evidence-based practices that synchronise with individual preferences and family needs. 18
Despite such policies and efforts by the government and different development partners, the uptake of modern FP methods has remained low.18,19 A national survey in 2018 showed that only 10.5% of women of reproductive age use modern methods of FP. 20 Could this be because the various personal, family and community-related barriers are yet to be adequately addressed? There is thus the need for continuous re-assessment of the various factors associated with unmet FP needs among reproductive women in different regions of the country. The outcomes of such surveys are potentially useful in informing regular review of existing programmes and policies. It is within this context that this index study was conducted to determine the prevalence of unmet FP needs and its association with socio-demographics, reproductive history and family function among females of procreative age bracket in Southwestern Nigeria.
Materials and methods
Study location
The study was carried out in the Family Medicine clinic of a tertiary hospital in Southwest Nigeria. The Family Medicine clinic served as a primary care facility for people aged 15 years and above, with an average of 2000 patients seen during working hours each month, 20% of whom are females of the reproductive age group. 21 The family medicine clinic is run by family physicians, resident doctors and medical officers.
Study design and population
This was a hospital-based cross-sectional study carried out between September and December 2019. The study population were females of the reproductive age group (15–49 years) attending the Family Medicine clinic during the study period.
Selection criteria
All consenting sexually active female patients aged 15–49 years who attended the clinic during the study period were recruited. The estimated population of those eligible for recruitment was about 100 persons per week. However, clients with infertility, unmarried women who were not sexually active, critically ill subjects requiring emergency treatment and subjects with severe cognitive impairments were excluded.
Sample size determination
The sample size was determined using the following formula
22
: n = z
2
(pq) / d2, where n = the sample size, z = a constant at 95% confidence level = 1.96, p = prevalence of unmet needs for FP (21.4%) among antenatal clinic (ANC) patients from a previous study done in Nnewi,
17

The addition of an attrition rate of 10% gave a sample size of 285 subjects.
Sampling technique
A systematic random sampling technique was used to recruit the 285 respondents who fulfilled the inclusion criteria. According to the medical record unit of the family medicine department of the hospital, an average of 100 patients were seen per week and 1200 (sample frame) patients over the 12 weeks that the study was conducted. Using the formula, K = N / n, where k is the sample interval, N is the sample frame (1200) and n represents the minimum sample size of 285. Therefore, K was approximately 4. The first respondent on each clinic day was chosen by simple random sampling, and after that, every fourth respondent was chosen by systematic random sampling until the sample size of 285 was attained. A total of 275 respondents completed the study yielding a response rate of 96.5%. A sticker was placed on each selected folder to avoid its re-sampling at the subsequent visits.
Data collection
Data collection was done using a pre-tested, semi-structured, validated, interviewer-administered questionnaire. The questionnaire was used to elicit information on respondents’ socio-demographic characteristics, obstetrics and gynaecological history, contraceptive section, family history and the reasons for not using contraception. A pretesting of the questionnaire was done at a sister hospital in the same town. Any errors or ambiguities in the questionnaires were corrected before a final version was drawn. However, the standard and validated sections remained unchanged.
Assessment of the family function of the participants
The family function was measured using the Family Adaptability, Partnership, Growth, Affection and Resolve (Family APGAR) scale. 23 Family APGAR is a five-item validated measure of family functioning with subjects having the options of answering with ‘hardly ever’, ‘sometimes’ or ‘almost always’ based on their frequency of feeling satisfied with each parameter been assessed. ‘Hardly ever’ received a score of 0, ‘sometimes’ a score of 1 and ‘almost always’ a score of 2. Hence, a total score of 0–10 was obtainable, with higher scores indicating greater satisfaction with family functioning. A score of ⩽6 implied the presence of perceived family dysfunction, while 7–10 was taken as a functional family. 23
Body mass index
A Hana® stadiometer was used to measure each respondent’s weight (in kilogrammes) and height (in centimetres). The weights were taken in light clothing with shoes off, while heights were measured with the subjects in an upright standing position without shoes or headgear. The readings were recorded to the nearest 0.5 kg and 0.1 cm, respectively. Body mass index (BMI) was calculated from the formula: weight (kg) / height (m2). Women with a BMI of ⩾ 30 kg/m2 were classified as obese.
Blood pressure
The blood pressure was measured using a mercury sphygmomanometer and a stethoscope on all the subjects’ right and left arms in a sitting position after 5–15 min of rest. 24 The onset of the first tapping sound (Korotkoff I) was taken as the systolic pressure. In contrast, the point of complete disappearance of the sound (Korotkoff V) was taken as the diastolic pressure of each subject. The blood pressure of each subject was measured in two different positions on two different occasions at least 5–15 min apart, and the average value was used for each of the subjects. 24
Study variables
The primary outcome variable in this study was whether a woman had an unmet need for FP or otherwise. Sexually active females who intended to prevent, delay or stop/limit conception but had not been using any modern contraceptive method were regarded as having an unmet need for FP.25–27 This variable was categorised as shown in Table 1.

The modern methods of contraception were categorised as follows: pill, intrauterine device (IUD), injection, diaphragm, condom (male or female), sterilisation (male or female), implant or foam/jelly. This variable will be dichotomised into two – whether a woman utilised modern FP or not, and coded 1 or 0, assigned respectively. The definition of the usage of contraceptive methods was limited to modern methods because of the high failure rates of traditional methods.
The independent variables included the subjects’ health status, age, literacy, parity, last inter-pregnancy interval, place of residence (urban vs rural), religion, marital status, number of surviving children, obstetric history, anthropometric and clinical parameters.
Data analysis
Data were entered into Excel on the author’s personal computer and subsequently uploaded and analysed using Statistical Package for Social Sciences (SPSS) software, version 21 (SPSS, Chicago, IL, USA). Descriptive statistics (either as percentages for the categorical variables or mean for the continuous variables) were calculated as appropriate. Bivariate analysis was performed to examine the association between unmet needs for FP and each selected predictor. The strength of association was estimated using Pearson’s chi-square. For all variables, all p values were two-tailed, and values < 0.05 were considered to be statistically significant. All variables with significant differences (p < 0.05) were selected and included in a multivariable logistic regression analysis to identify independent determinants of unmet FP needs with the results presented as odds ratio (OR) and corresponding 95% confidence interval (CI).
Ethical clearance, considerations and consent
Ethical approval was obtained from the institution’s Ethical Review Committee with protocol number: ERC/2017/08/05. Informed written consent was obtained from each respondent before recruiting them into the study. Also, assurance was given to each respondent on the highest possible level of confidentiality, privacy and anonymity. Names and other means of identification were coded. Unidentified hard copies of questionnaires were kept safely with the Researcher under lock. The statement of their right to withdraw from the study at any point in time without any prejudice was documented in the patient information sheet provided for them.
Results
A total of 275 respondents had complete responses and were included in the final analysis, yielding a 96.5% response rate.
Table 2 shows the socio-demographic characteristics of the respondents. The mean age of the respondents was 29.71 ± 8.06 years (range: 17–49). Most respondents (104, 36.5%) were aged 15–24 years, currently married (137, 48.1%), Christians (245, 85.9%) and were Yoruba (249, 87.4%). The majority of the respondents (260, 91.2%) resided in an urban area. Half of the respondents, 143 (50.2%), had tertiary education. Most participants (185, 64.9%) were unemployed, while respondents who earned less than 18,000 Naira per month were 147 (51.6%).
Socio-demographic characteristics of respondents.

Single.
Separated/divorced/widow.
Ijaw/Itshekiri/Igede.
Students, full-time house wives, subsistent farmers.
Reasons for non-uptake of contraceptives
Among the respondents with an unmet need for FP, the reasons for the non-uptake of contraceptives are shown in Table 3. These include fear of side effects (107, 66.3%), husbands’ disapproval (13.8%) and 16 (8.8%) related to religious grounds.
Reasons for unmet family planning needs.

Multiple responses.
Mother-in-law disapproval, infrequent sex.
Prevalence of unmet needs for FP
Table 4 shows the proportions and categories of unmet needs for FP. The respondents with unmet needs were 160 (58.2%). These include those with unmet needs for limiting: 46 (28.8%), spacing: 61 (38.1%) and prevention: 53 (33.1%).
Proportion and categories of respondents with unmet needs for family planning.

Relationship between unmet needs and various factors
Table 5 shows the association between socio-demographic characteristics of the respondents and unmet needs for FP. Parity (χ2 = 15.64; p = 0.001) and level of education (χ2 = 5.87; p = 0.042) were statistically significantly associated with unmet FP needs. Whereas, respondents’ age, marital status and income had no statistically significant relationship with the unmet need for FP (p > 0.05).
Relationship between social-demographic characteristics and unmet family planning needs.

The association between unmet needs for FP and Obstetrics factors is shown in Table 6. The number of respondents’ partner(s) (χ2 = 4.76; p = 0.029) and the current number of children of respondents (χ2 = 15.08; p < 0.001) had a statistically significant association with unmet FP needs. However, the number of sexual activities per month, unplanned pregnancies dysmenorrhoea and heavy bleeding were not statistically significantly related to unmet FP needs.
Obstetrical and gynaecological factors and unmet family planning needs.

Significant at 95% confidence level.
Table 7 highlights the relationship between unmet FP needs and family-oriented factors as well as clinical parameters. None of the variables was statistically significantly associated with unmet FP needs (p > 0.05).
Relationship between family-oriented factors, clinical parameters and unmet family planning need.

Family APGAR: Family Adaptability, Partnership, Growth, Affection and Resolve; FP#: family planning; BMI: body mass index; BP: blood pressure.
Independent predictors of unmet needs
The result of the multivariable logistic regression analysis is displayed in Table 8. It shows the significant predictors of unmet FP needs among the respondents. Those with four or fewer children were about eight times more likely to have unmet needs than respondents with five or more children (adjusted odds ratio (AOR): 7.731; 95% CI: 28.504–2.907, p = 0.002). Also, the odds of having unmet needs among respondents who had one partner was two times, the odds among those with two or more partners (AOR: 2.008; 95% CI: 3.669–1.090, p = 0.025).
Significant independent predictors of unmet needs.
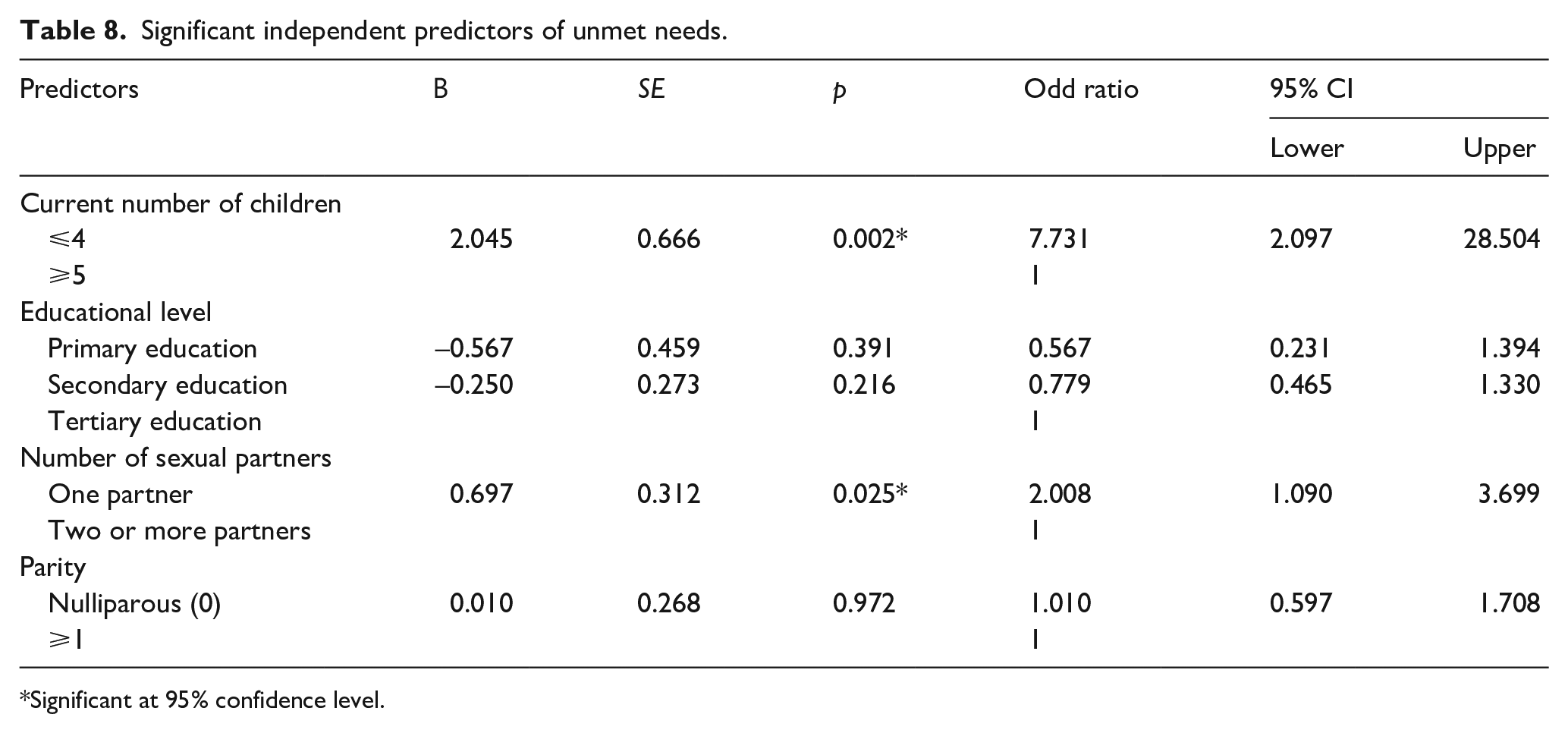
Significant at 95% confidence level.
Discussion
The study determined the prevalence of unmet needs for FP and its determinants among women of reproductive age groups in Southwestern Nigeria. This is important because unmet needs for FP have remained a significant indicator for monitoring the progress towards the reduction of maternal mortality worldwide. 27
Prevalence of unmet needs for FP
The prevalence of unmet needs for FP in this study was 58.2%. This finding was higher than the results found in other studies. For instance, Bhattathiry and Ethirajan 28 reported a 39% prevalence of unmet needs. A related study by Ajong et al. 2 found the unmet needs for FP to be 20.4% while Anthony et al. 17 reported 21.4% unmet needs. The reason for the low level of unmet needs in the other studies as compared to this study might be because their respondents were married women who were recruited from the ANC and might have sufficient knowledge and counselling from repeated ANC, thereby increasing their contraceptive uptake and reducing their unmet needs.
In this study, the respondents using FP for spacing (48.4%) were relatively higher than those using it for limiting (12.7%), which was similar to that reported by Anthony et al. with 15.2% and 6.2% of respondents using it for spacing and limiting, respectively.
Reasons for non-use of modern contraception
In this study, the major reason for not using modern contraception was fear of side effects (66.3%). This was comparable to the findings in the studies by Patil et al. 29 and Bhattathiry and Ethirajan, 28 respectively. Therefore, regular and sustained counselling by the stakeholders is needed to improve modern contraception in the study area. Modern contraception has remained a significant indicator for monitoring the progress towards the reduction of maternal mortality worldwide. 27
Factor associated with unmet needs
Education
The respondents with higher education had a higher prevalence of unmet needs for FP. This was similar to the study by Bhattathiry and Ethirajan 28 in 2014 in Tamil Nadu, India. Education was statistically significant because many of the respondents were educated due to the high level of educational attainment in the Southwestern part of Nigeria where the study was conducted.
Parity
Unmet needs were found to be significantly higher among those who were nulliparous (most likely the unmarried women) and those who were primiparous. The women with higher parity were likely to have had repeated contraceptive counselling during their several ANC visits during each conception coupled with the less sexual drive as they age. This corroborates the finding by Anthony et al. 17
Number of living children
Respondents with four children or less reported a higher level of unmet needs. This factor also emerged as an independent predictor of unmet needs for FP from the multivariable logistic analysis. Women with a higher number of living children were most likely uninterested in more children, hence potentially more open to the use of contraceptives. This was comparable with the study in India by Patil et al. 29 This finding was however contrary to that of Akintade et al. 30 in Lesotho.
Number of sexual partners
This index study found a significant association between the number of sexual partners of respondents and unmet needs for FP. It also showed that respondents with one sexual partner had twice the unmet needs for FP compared with respondents with more than one sexual partner. This is because respondents with a sexual partner were more likely to have a reduced perception of getting pregnant. Hence, they make little or no effort in preventing conception, thereby increasing their chances of getting pregnant and increasing their unmet needs as against respondents with more than one sexual partner who are more conscious of their increased chances of getting pregnant because of their more sexual partners. Hence, they tend to make frantic efforts to prevent getting pregnant, thereby reducing their unmet needs. This is in line with the findings by Letamo et al. 31 in a cross-sectional survey in Botswana.
Limitations of the study
This was a facility-based research; as such, its findings could not be a true reflection of what is obtainable in the community. The information in the study was obtained by self-reporting; therefore, certain information may be withheld or exaggerated by participants as well as the sample size. Furthermore, the result of the logistic regression needs to be interpreted with caution because of the potential impact of the sample size. According to Bujang et al., observational studies logistic regression in the analysis should have a minimum sample size of about 500 to derive the statistics that are close to the true population parameters. It must also be noted that only the variables with significant p values from the bivariate analysis were included in the multivariable regression model. This poses the risk of specification bias because the number of relevant variables must have been inadvertently excluded. Diagnostic tests, such as tests for multicollinearity, were also not done.
Conclusion
A high rate of unmet needs for FP was found in this study and the commonest reason for the non-uptake of contraceptives was the fear of side effects. There is a need for intensification of routine counselling during consultations, public health education and awareness, and regular review of existing policies. The educational outreaches should be tailored towards addressing some of the unfounded fears of the side effects of contraceptives. Furthermore, the effectiveness of current policies needs to be more regularly monitored and evaluated.
Supplemental Material
sj-docx-1-map-10.1177_27550834221115979 – Supplemental material for Unmet needs for family planning and its determinants among women of reproductive age in Ilesha Southwest Nigeria: A cross-sectional study
Supplemental material, sj-docx-1-map-10.1177_27550834221115979 for Unmet needs for family planning and its determinants among women of reproductive age in Ilesha Southwest Nigeria: A cross-sectional study by Murithada Kadiri Uthman, Ibrahim Sebutu Bello, Akinyemi Olaleye Fadugbagbe, Temitope Oluwafemi Olajubu, Waheed Olalekan Ismail and Azeez Oyemomi Ibrahim in The Journal of Medicine Access
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.