
Abstract
Background:
Suboptimal complementary feeding practice during the first 2 years of life are key determinants of malnutrition in children and have a negative impact on a child’s growth, health, and development.
Objective:
To assess the prevalence of suboptimal complementary feeding practice and associated factors among caregivers of children 6–23 months in Dambi Dollo town.
Methods:
Community-based cross-sectional study was conducted at Dambi Dollo Town from 9 August to 11 October 2023, among 284 caregivers of children aged 6–23 months. Binary logistic regression was used to measure the strength of association between dependent and independent variables using adjusted odds ratio (AOR) and 95% confidence interval (CI). A p-value < 0.05 was considered statistically significant.
Results:
The prevalence of suboptimal complementary feeding among caregivers of children 6–23 months was 65.8%. Findings of multivariable logistic regression analysis indicated that lack of formal education (adjusted odds ratio (AOR) = 4.93, 95% CI = (2.35, 10.34)), lack of attending antenatal care (AOR = 2.47, 95% CI = (1.20, 5.08)), and medium knowledge of child feeding practice (AOR = 0.21, 95% CI = (0.09, 0.47)) were significantly associated with suboptimal complementary feeding practice.
Conclusion:
This study showed that two-thirds of children were poorly provided complementary food which significantly associated with lack of attending antenatal care, lack of formal education, and medium knowledge on infant and young child feeding practice. These results highlight the need for targeted interventions, including strengthening antenatal care services, promoting maternal education, and enhancing community-based nutrition education programs to improve complementary feeding practices and ultimately support better child health and development outcomes.
Plain Language Summary
This study looked at how well caregivers in Dambi Dollo town feed their children aged 6 to 23 months, focusing on complementary feeding, the food given to young children in addition to breast milk. Inappropriate feeding during this critical period can lead to malnutrition and affect a child’s growth and development. The findings of this showed that two out of three children (65.8%) were not getting proper complementary foods. The study found that caregivers who had no formal education, did not attend antenatal care (ANC), or had no sufficient knowledge about child feeding were more likely to feed their children poorly. These findings suggest the need to strengthen ANC services, support maternal education, and improve nutrition education at the community level to help ensure children get the right foods at the right time.
Introduction
The World Health Organization (WHO) defines suboptimal complementary feeding practices as failing to meet the four indicators of feeding. The core complementary feeding indicators of WHO are introduction to solid and soft foods, minimum meal frequency (MMF), minimum diet diversity (MDD), and minimum acceptable diet (MAD) recommended by the WHO. 1
Suboptimal complementary feeding including inappropriate breastfeeding practices has detrimental impact on a child’s growth, health, and development. 2 Globally, few children received nutritionally adequate, diversified, age-appropriate frequency, and timely initiation of complementary food. In the world, evidence showed that 73% of children of 6–23 months received solid, semi-solid, or soft foods at 6–8 months, 52% of mothers fed their children with MMF, and only 29% of children have a diversified diet. 3
The 2019 Ethiopia Mini Demographic Health Survey (EMDHS) report shows that 7% of children under 5 years are wasted, 37% are stunted, and 21% of all children are underweight. 4 Worldwide, above 10% of the disease burden are due to maternal and child under nutrition. 5 Almost half (45%) of all children’s deaths are associated with malnutrition, while children in sub-Saharan Africa are more than 14 times more likely to die before the age of 5 than children in developed countries. 6 Suboptimal complementary feeding practices like poor quality of complementary diet, inappropriate breastfeeding, and micronutrient deficiency had largely contributed to the high morbidity and mortality among infant and child in different countries. 1
The Ethiopian government developed and implemented the infant and young child feeding guideline in 2004 to improve feeding practices. Based on the guideline, infant and young child feeding messages were given at health institution and at the community level. However, most mothers inappropriately fed their children. 7
According to Ethiopian Demographic and Health survey (EDHS) 2019, only 7% of children in Ethiopia age 6–23 months meet the minimum standards with respect to Infant and Young Child feeding (IYCF) practices. 4 Suboptimal feeding practice is a vital factor contributing to inadequate nutrient intake among infants and young children.4,7,8
Different researchers show factors that influence optimal complementary feeding practice are socioeconomic status, educational status, child age, maternity knowledge, and family size. 5 Suboptimal complementary feeding practices directly impact the nutritional status and ultimately survival of children less than 2 years of age. If children do not receive sufficient dietary diversity and meal frequency after 6 months of age, they will become stunted even after optimum breastfeeding. 9 Few studies in Ethiopia showed that complementary feeding practices are inadequate. 8 There are no any published articles on suboptimal complementary feeding in the study area, Dambi Dollo Town. Hence, knowing the level of practices helps to undertake appropriate measures to improve optimal complementary feeding practices that in turn improve nutritional status of children through this essential time of child growth and development. Previous studies have used one or two indicators, but the inconsistent findings make it difficult to conclude suboptimal complementary feeding practice. Hence, four indicators are used in this study to obtain better information on suboptimal complementary feeding practices.
Objectives
This study aimed to assess the prevalence of suboptimal complementary feeding practices and associated factors by using the four key child feeding indicators to obtain a more comprehensive understanding among caregivers of children aged 6–23 months in Dambi Dollo town, Ethiopia.
Methods
Study design
A cross-sectional quantitative study was conducted from 9 August to 11 October 2023.
Study setting
The study was carried out in Dambi Dollo Town, Kellem Wallega Zone, Oromia Region, Ethiopia. Dambi Dollo is found at the distance of 652 km from Addis Ababa, the capital city of Ethiopia. The latitude of Dambi Dollo is approximately 8.5°N and the longitude is 34.8◦E. Dambi Dollo has 4 kebeles with a total population of 52,245, where males constitute 25,990. The town has one general hospital, one health center, and four health posts. Its temperature typically varies from 54°F to 84°F and is rarely below 51°F or above 90°F.
Study population
The source population were all caregivers of children aged 6–23 months, and in the study population, the caregivers were randomly selected.
Sample size determination
A total of 284 sample sizes are calculated using a single population proportion formula, assuming a 50% prevalence of suboptimal complementary feeding practices among children aged 6–23 months in the study area. As a source population was 1102, a correction formula was applied and a 10% non-response rate was considered.
Sampling procedure
This study included all four kebeles of Dambi Dollo town. A sample frame was created using the registered birth dates of the last child from family folders obtained through the kebele urban health extension workers. House-to-house visits were conducted with the corresponding household identification number, and proportional allocation was applied to each kebele. Simple random sampling was used to select participants, and mothers with children aged 6–23 months were then chosen using systematic random sampling.
Inclusion and exclusion criteria
The caregivers who had children 6–23 months were included in the study, while caregivers who were unable to communicate were excluded from the study.
Data collection procedure
Structured and pretested questionnaires were used to collect data on sociodemographic characteristics, dietary practice, health and related characteristics, and maternal knowledge. Based on the WHO guidelines, dietary data were collected by using a 24-h recall method. Caretakers were asked to recall all food items given to their child in the past 24 h before the day of survey.
In this study, suboptimal complementary feeding practice was defined as the failure to meet one or more of the four criteria outlined by the WHO. These criteria include the untimely introduction of complementary feeding, inadequate meal frequency based on the child’s age and breastfeeding status, insufficient dietary diversity, and the failure to achieve an MAD.1,10
Minimum dietary diversity was defined as the proportion of children 6–23 months of age who received foods from five or more food groups from eight food groups: (1) grains, roots, and tubers; (2) legumes and nuts; (3) dairy products; (4) flesh foods; (5) eggs; (6) vitamin A-rich fruits and vegetables; (7) other fruit and vegetables; and (8) breast milk.
A proportion of children aged 6–23 months who received minimum of 3 meals within the last 24 hours were considered as the children who achieved the MMF.
MAD is a composite indicator of minimum dietary diversity and MMF. When a child meets both the MDD and the MMF, it is coded as the MAD. 8
In this study, mothers’ knowledge of infant and young child feeding practices was assessed using nine questions covering key areas, including food preparation (diversity, processing, cooking, and mixing), feeding techniques, hygiene practices (holding and storing), timing of complementary feeding, and feeding frequency. Based on their responses, mothers were categorized as having high knowledge (score ⩾7), medium knowledge (score 4–6), or low knowledge (score <4).
Data quality control and management
Training sessions were held for data collectors and supervisors to ensure the reliability and validity of the data collection process. These sessions covered interviewing techniques, questionnaire understanding, and consistency. Supervisors were trained to oversee quality control. The questionnaire was pretested on 5% of the sample a week before data collection in a neighboring woreda. The pretest helped identify issues such as ambiguous wording, and based on feedback, necessary modifications were made to improve clarity and flow, ensuring the final version was both reliable and valid for the study.
Data analysis
The collected data were checked for its completeness and edited before entry into computer. Then, the questionnaire was coded, and data were entered to EpiData version 4.6 and exported to SPSS version 27 computer software for analysis. Descriptive statistics such as frequencies, numerical summary measures, text, graphs, and tables are used to describe the outcome variable against all relevant independent variables. Binary logistic regression was used to see the association between dependent and independent variables. Variables having a p-value < 0.25 in binary logistic regression were transferred to multivariable logistic regression. In this study, a p-value < 0.25 was used in bivariable analysis to avoid excluding potentially important variables. A p-value < 0.05 was considered as statistically significant; adjusted odds ratio (AOR) and 95% confidence interval (CI) were used to interpret findings. The fitness of the model was tested by the Hosmer–Lemeshow goodness-of-fit test, and accordingly, the model was found to be fit with (p = 0.432). Multicollinearity between independent variables was checked by using the variance inflation factor (VIF) and was found to be 2, indicating the absence of significant collinearity among independent variables.
Ethical considerations
Prior to data collection, ethical approval was obtained from the Ethical Review Board of Dambi Dollo University, with the ethical clearance code IHRPGC/735/17. A formal letter of permission was also provided by the zonal administration to the Dambi Dollo Town Health Office. Finally, verbal consent was obtained from each study participant during data collection after the objectives of the study were clearly explained. Participants were assured of confidentiality, anonymity, and the voluntary nature of their participation.
Results
More than three-fourths of mothers (77.8%) were 24–29 years, with a mean age of 26.93. All mothers (100%) were married, and more than half 176 (62%) of mothers attended primary school (grade = 1–8). A large proportion (58.5%) of caregivers were housewives. More than three-fourths (77.4%) of children were living with a family size of 4–6 (Table 1).
Sociodemographic characteristics of caregivers of children 6–23 months in Dambi Dollo Town, 2023.

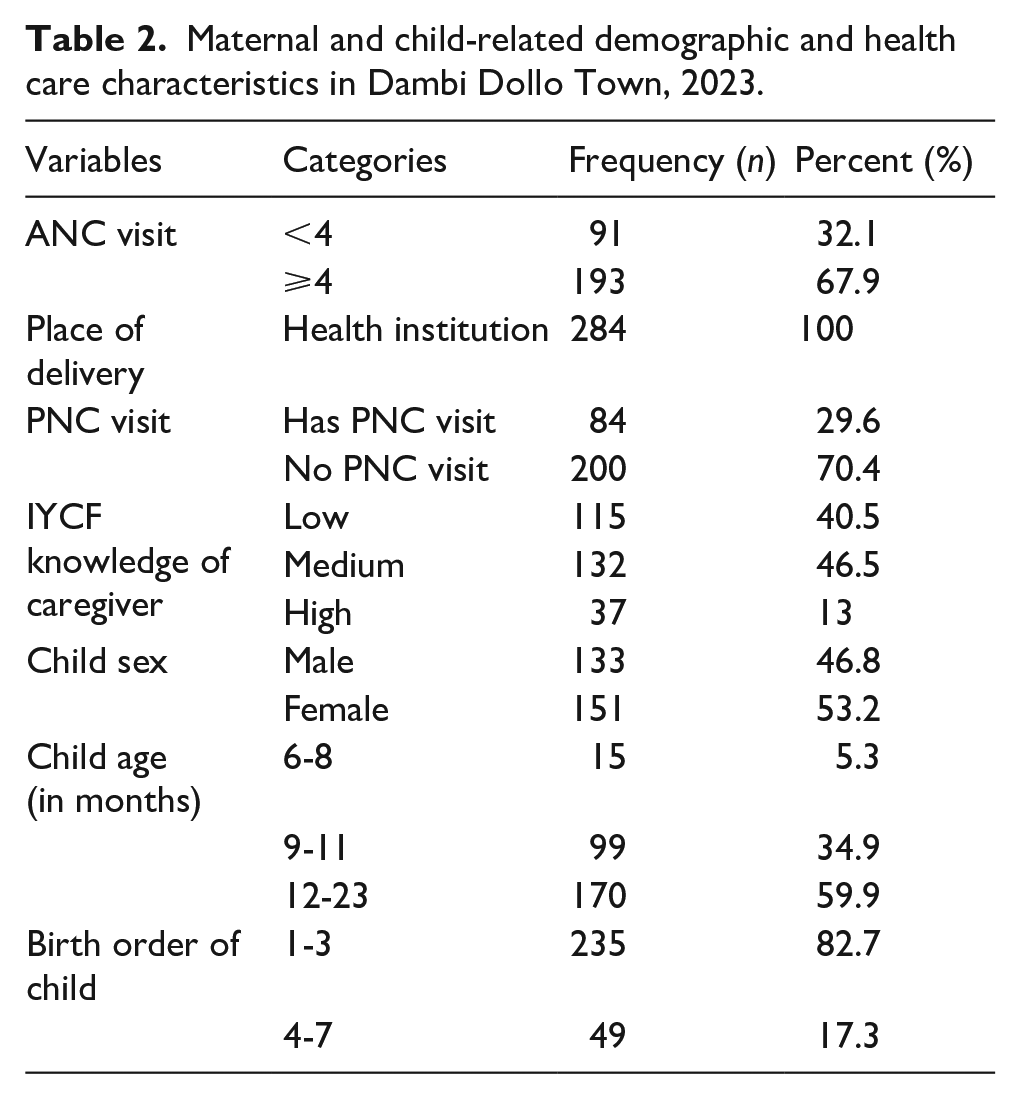
All caregivers (100%) have attended ANC for the index child, in which 193 (67.9%) had attended greater than or equal to four. All the study participants gave birth at a health facility. Only 84 (29.6%) of caregivers attended postnatal care (PNC). More than half (59.9%) of children were 12–23 months old (Table 2).
Maternal and child-related demographic and health care characteristics in Dambi Dollo Town, 2023.
Child feeding practices
Findings of this study indicated that one-third (65.8%) of caregivers did not achieve optimal complementary feeding (Figure 1).

Complimentary feeding practices of children aged 6–23 months in Dambi Dollo Town, 2023.
Out of 284 caregivers, 181 (63.7%) have introduced complementary feeding at <6 months of child age. Findings of this study showed that 34.5% of caregivers provided their children ⩾5 food groups within the last 24 h and 102 (35.9%) children have received the MAD (Table 3).
Child feeding practices among caregivers of children 6–23 months in Dambi Dollo Town, 2023.
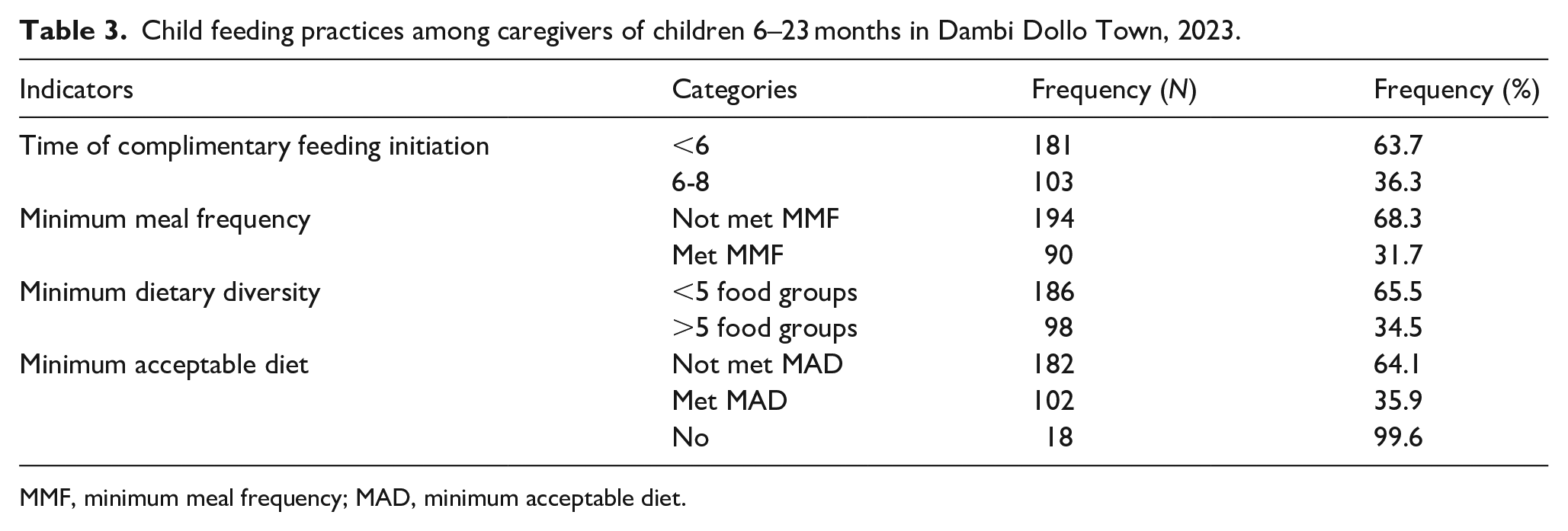
MMF, minimum meal frequency; MAD, minimum acceptable diet.
The most dominant food group given for children was grain products. Low feeding practice was observed on vitamin A-rich fruit and vegetables (20.4%), eggs (20.4%), flesh meat (0.4%), and dairy products (7%) (Figure 2).

Types of food given to children in the preceding 24 h among children aged 6- to 23-month children in Dambi Dollo Town, 2023.
Factors associated with suboptimal complementary feeding practice
In the bivariable analysis, educational status of mother, history of ANC, birth order, number of family members, and knowledge of caregivers on infant and young child feeding practice were found to be associated with suboptimal complementary feeding practice (p < 0.25). Findings of multivariable logistic regression showed that women who had no formal education were 4.8 times more suboptimal complementary feeding than women who attended formal education (AOR = 4.93, 95% CI = (2.35, 10.34)). The odds of suboptimal complementary feeding were 2.5 (AOR = 2.47, 95% CI = (1.20, 5.08)) times higher among caregivers who attended less than four ANC visit as compared with their counterparts. Caregivers who had medium knowledge on IYCF practice were 79.1% (AOR = 0.21, 95% CI = (0.09, 0.47)) less likely practiced suboptimal complementary feeding (Table 4).
Factors associated with suboptimal complimentary feeding practice among caregivers of 6- to 23-month children in Dambi Dollo Town, Western Ethiopia, 2023.

1 = indicate for reference group.
Significant association at p < 0.05; **p < 0.001.
Discussion
The study found that 65.8% of children had suboptimal complementary feeding practices which is higher than the 43.5% (10%) in Northeast Ethiopia but lower than the 87.5% in Southern Ethiopia. 10 In the Oromia region, the prevalence of suboptimal complementary feeding practices was 70%, 4 which is consistent with the national trend. Regional differences may be due to variations in socioeconomic status, education, knowledge, and access to health services.
This finding showed that more than one-third (36.3%) of caregivers practiced complementary feeding timely. This finding is almost comparable with the study done in Gondar 11 where 36% of mothers or caregivers practiced complementary feeding at 6 months. However, a study done in Jimma showed that 42.9% of the mothers introduced complementary food before 6 months. 12
Complementary foods for children should be made from at least five food groups and nutrient dense. 8 However, in this study, only 34.5% of children met the minimum requirement of five or more from the eight food groups. This finding is similar to studies from five South Asian countries; the dietary diversity reported was less than 50% in all countries except Sri Lanka 71.1%. 13 The current finding is lower than reported in Tanzania, where 38% of children received minimum dietary diversity. 14 This discrepancy might be due to the lack of affordability of these foods or inadequate knowledge of caregivers about the importance of diversity feeding of infants and young children.15 –18
This study also showed that 31.7% of children received MMF. This finding is lower than studies conducted in Dangle, Ethiopia (50.4%), 15 Tanzania (38.6%), 14 and Nigeria (36.6%).16,19 This discrepancy could be a consequence of social, educational, and cultural differences existed between this study and others. This study showed that the prevalence of children who received MAD was low. As MAD takes both MMF and minimum dietary diversity, 8 only 35.9% of the children achieved the MAD. However, this finding is higher to similar studies conducted in northwest Ethiopia, 17 with a national prevalence of 4.1%, 7.3%, and 11.3% during the survey periods of 2011, 2016, and 2019, respectively. 4
Findings of this showed that women who had no formal education were practicing more suboptimal complementary feeding than women who attended formal education. This finding is consistent with the report from Nigeria, 19 Ethiopia,20,21 and India. 22 A possible reason could be mothers who did not attend formal education have no exposure to information on feeding practices. Hence, caretakers could practice suboptimal complementary feeding practices.
Lack of attending ANC was positively associated with suboptimal complementary feeding practices. Caregivers who attended fewer than four ANC visits were more likely to have suboptimal feeding practices compared to those who attended four or more visits. This finding is consistent with a study in Bahir Dar City, Ethiopia. 23 Regular ANC visits offer mothers essential health education on nutrition, feeding schedules, and introducing solid foods, which supports improved feeding practices. Thus, mothers who attend ANC regularly are more likely to adopt healthier complementary feeding practices, underscoring the role of healthcare services in influencing maternal behaviors. Although not significant in this study, other research has shown that PNC attendance also plays a significant role in promoting optimal complementary feeding, likely due to caregivers receiving nutrition counseling on child feeding practices.13,24
Caregivers with moderate knowledge of IYCF practices were less likely to engage in suboptimal complementary feeding. This highlights the importance of understanding key feeding guidelines, such as the appropriate timing and types of complementary foods. Studies from Sidama, 25 southwest Ethiopia, 26 and Pakistan 27 support this finding, showing that caregivers with better IYCF knowledge are more likely to implement optimal feeding practices.
Limitations of the study
The findings of this study have significant implications for the prevention of acute malnutrition. However, the study has several limitations. These include its cross-sectional design, which limits causal inference, and potential selection bias due to recruitment from an urban setting. In addition, the reliance on self-reported data for some explanatory variables may have introduced recall and social desirability biases. As the study was conducted in an urban area, the findings may not be generalizable to rural populations.
Conclusion
The results of this study demonstrated that two-thirds of the children had inadequate complementary feeding, which was significantly associated with lack of prenatal and postnatal care, low maternal education, and limited knowledge of infant and young child feeding practices. To address these gaps, both governmental and non-governmental organizations should strengthen maternal and child nutrition interventions by integrating infant and young child feeding practices counseling into ANC and PNC services, providing targeted training for health workers, and implementing community-based programs to improve maternal education and awareness. These strategies are vital to improving complementary feeding practices and reducing the risk of acute malnutrition among young children.
Footnotes
Acknowledgements
The authors would like to thank Dambi Dollo University for technical support. The authors would also like to thank data collectors and study participants.
Consent for publication
Not applicable.
Author contributions
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was conducted with the technical support of Dambi Dollo University, but there is no financial support. The views presented in the article are those of the author and do not necessarily express the views of Dambi Dollo University.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data set used for this study cannot be shared, and in the future, interested parties may request the approval to access the data by writing to the Dambi Dollo University Institutional Review Board.