
Abstract
Background:
Health literacy proficiency is essential for health care professionals to provide quality patient care. There is limited research exploring health literacy proficiency among undergraduate health science students.
Objectives:
To determine health literacy among health science students in Singapore using the electronic Health Literacy Questionnaire (HLQ).
Design:
A cross-sectional survey using purposive sampling was conducted among undergraduate health science students.
Methodology:
This study hypothesises that health literacy is influenced by gender, and it increases with the level of health science education, attributed to the increased exposure to the health care system and health care education as undergraduates progress through the years of study. Eligible students from the 4-year entry-level programmes of diagnostic radiography, dietetics, occupational therapy, physiotherapy, radiation therapy and speech and language therapy, aged from 21 to 50, were invited. Exclusion criteria were students who were no longer studying due to dropping out or having immediately graduated from these programmes and students in the accelerated programmes whose studies would be completed in less than 4 years.
Results:
In total, 111 respondents (72 females and 37 males) completed surveys (response rate, 7.7%) returned from physiotherapy (n = 69), occupational therapy (n = 25), diagnostic radiography (n = 12) and dietetics (n = 5), with nil from radiation therapy and speech and language therapy. All participants were English literate. Female participants demonstrated higher HLQ with a mean total score of 30.67 (standard deviation (SD) = 0.61) versus male participants 29.83 (SD = 0.53). Year 2, 3 and 4 students generally scored higher than Year 1 across all nine HLQ scales. Overall, dietetics students had the highest total score on the HLQ, while the diagnostic radiography students had the lowest scores for all the nine HLQ scales.
Conclusion:
This study established the health literacy level of health science students in Singapore. Gender and years of study influenced health literacy levels, supporting the hypothesis.
Plain Language Summary
Background:
Health care professionals need to understand health information well to provide good patient care. There is little research on how well health science students understand health information.
Objectives:
This study aims to determine how well health science students in Singapore understand health information using a questionnaire known as the Health Literacy Questionnaire (HLQ).
Design:
The study surveyed health science students.
Methodology:
The study explored if the understanding of health information is influenced by gender and increases with more years of health science education. This is because students get more exposure to the health care system and education as they continue their studies. Students from various health science programmes aged 21 to 50 were invited to participate. Students who had dropped out or just graduated and were in accelerated programmes were excluded.
Results:
The survey was completed by 111 students (72 females and 37 males) from physiotherapy, occupational therapy, diagnostic radiography and dietetics. No students from radiation therapy and speech and language therapy participated. All participants could read and write in English. Female participants scored higher on the questionnaire than male participants. Students scored higher in their second, third and fourth years than in their first year of study. Dietetics students scored the highest overall, while diagnostic radiography scored the lowest.
Conclusion:
This study reported the level of understanding of health information among health science students in Singapore. The level of understanding was influenced by gender and years of study.
Key messages
• Establishing the health literacy level of health science students in Singapore is important.
• Senior students tend to have better health literacy compared with junior students.
• Navigating the health care system and obtaining support from health care providers are areas where students can benefit from health literacy education.
• Educational materials should be optimised to address potential health literacy deficits and ensure high literacy levels upon graduation.
Keywords
Background
Health literacy comprises social and cognitive skills influencing motivation and the ability to access, comprehend and utilise health information to maintain and promote good health. 1 It is multifaceted and involves numerous competencies and skills, such as assessing health information and navigating the health care system. 2 Poor health literacy determinants include inadequate education, learning impairments, age-related cognitive deterioration and the concept of regular practice for maintaining proficiency. 3 Factors, including education level, discipline of studies, age, gender and mastery of languages, influence health literacy.4 –6 At the same time, ethnicity, occupation and income can affect health information availability, causing population disparity in health literacy. 7 The rise of chronic diseases within developed countries such as Singapore 8 has raised the importance of structured long-term care, in which its efficacy largely depends on one’s health literacy. 7 Individuals lacking health literacy will find specific health tasks challenging as they struggle to obtain and comprehend health information, reducing their engagement in preventive health practices. 9 With poor management on an individual level, the resultant economic ramifications on the health care system increase. 10 Aligning with the health master plan of 2017 by the Ministry of Health Singapore of going beyond health care to health, 11 individuals must be equipped with adequate levels of health literacy, which reduces the burden of health care costs on both individual and government levels.
Health care professionals are touch points of communication regarding health literacy to patients. Health care professionals help influence and shape the formation of good health behaviours through patient education when interacting with one another.12,13 Therefore, health care professionals need reasonable levels of health literacy to advocate for good health practices and behaviours.14,15 Support is needed for patients with low health literacy to help them gather and comprehend information. A prior study examined the relationship between health care providers’ level of health literacy, awareness of health literacy, attitudes towards promoting health literacy and strategies for addressing low health literacy among patients. 16 The findings highlight deficiencies in health literacy, particularly concerning the health literacy levels of providers, their awareness of health literacy and their ability to manage patients with low health literacy. These results underscore the necessity for devising strategies to enhance the collaborative efforts of providers within the health care system and to advocate for health literacy. Possible strategies may include the implementation of recommended tools and techniques for effective health communication.
Health science students represent the future of health care professionals and will champion and act as exemplars advocating for healthy lifestyles. 13 Health science students are hence exposed to information on health care as part of their curriculum and are, therefore, assumed to be highly health literate to meet the health literacy needs of their future patients. A study explored the experience of undergraduate nursing students in caring for patients with low health literacy by identifying behavioural cues and adopting strategies to increase health knowledge or self-care skills. The results of this study suggest that it would be beneficial for educators to incorporate health literacy into the undergraduate curriculum as a critical component of patient education. They could also focus on objectively assessing health literacy, evaluating patient education materials and promoting patient empowerment. This approach would ensure that students are exposed to health literacy-related content and have opportunities to apply this knowledge as they progress through their entry-level training. 17 Unfortunately, current literature on health literacy among undergraduates in health science programmes reported suboptimal health literacy among health science students across various disciplines, health care systems and countries,1,15,18 –23 despite the importance. Health science programmes in Singapore incorporate the principle of health literacy into their curriculum; this includes understanding and evaluating health information and navigating the local health care system. These elements are embedded universally within the first 2 years of entry-level training. 24 However, there is a lack of research conducted to assess the level of health literacy among health science students in Singapore. It is unclear whether the health literacy levels among health science students in Singapore will mirror the earlier findings. Understanding the health literacy levels of health science students and addressing potential gaps can offer a means to produce health-literate health care professionals capable of effectively managing the health care needs of patients. Therefore, this raises a need for a local study to identify possible health literacy shortcomings among health science students and understand the nuances within the health and education systems that may explain such findings.
Objectives
This study aimed to determine health literacy among health science students in Singapore using the Health Literacy Questionnaire (HLQ). The study hypothesises that health literacy is influenced by gender, and it increases with the level of health science education, attributed to the increased exposure to the health care system and health care education as undergraduates progress through the years of study. Demographic factors involving years of study, course of study and gender would determine their association with HLQ scores.
Design
Following the checklist for reporting of survey studies (CROSS) guidelines, 25 this purposive sampling cross-sectional study recruited undergraduate health science students in Singapore. Data collection was performed between February 2022 and January 2023. This study surveyed participants with HLQ electronically.
Ethical considerations
Ethical approval was granted by the University Institutional Review Board (approval number 2022027). The electronic dissemination of the HLQ enabled obtaining consent before the participants could proceed to answer the HLQ. The option ‘I consent to participate in this survey’ would bring on the HLQ for the entire survey activity, while the option ‘I do not consent to participate in this survey’ would indicate that no consent was given and participation defaulted. No financial reimbursement was offered to participants. The questionnaires were coded to ensure the confidentiality of the information (pseudonymised data). The electronic data were stored in a password-encrypted computer file, and only the research team had access to the questionnaire database. Once the legally required retention period has passed, the data will be destroyed as per legal requirements.
Methodology
Survey instrument
The HLQ was formulated considering both the patient’s and professional’s viewpoints via a method known as concept mapping. 2 With the initial question of ‘What does a person need to be able to understand, get and use the health information and services they need?’ that guided the process and followed by the incorporation of qualitative and quantitative elements. The HLQ conceptual model comprises nine distinct constructs (scales) encompassing various aspects to allow for dimension-specific evaluation. The skills range from comprehending and critically evaluating health information to actively interacting with health care providers and navigating the health care system. With established validity and reliability, the HLQ has proven highly relevant to diverse stakeholders and exhibits robust and reproducible psychometric properties. 2 The total scores from all the scales illustrate the complete multidimensional health literacy profile. The self-administered HLQ identifies health literacy strengths and shortcomings of individuals, facilitating dimension-specific intervention plans. The HLQ can be administered in multiple forms: phone-based, paper and pencil, mailed survey, face-to-face and computer-based.26 –29 It is a 44-item tool comprising nine scales representing the nine aspects of health literacy: 2
Feeling understood and supported by health care providers;
Having sufficient information to manage my health;
Actively managing my health;
Social support for health;
Appraisal of health information;
Ability to actively engage with health providers;
Navigating the health care system;
Ability to find good health information;
Understanding health information well enough to know what to do.
The HLQ is split into two parts. Part 1 consists of HLQ Scales 1–5 and utilises a 4-point Likert-type scale. Part 1 responses are scored 1–4 to indicate the participants’ level of agreeability: with 1 = strongly disagree; 2 = disagree; 3 = agree and 4 = strongly agree. Part 2 consists of HLQ Scales 6–9, utilising a 5-point Likert-type scale. Part 2 responses are scored 1–5, which indicate participants’ self-reported capability: 1 = cannot do; 2 = very difficult; 3 = quite difficult; 4 = quite easy and 5 = very easy. Each scale score is based on the mean of their item scores, with higher scores indicating higher strength in the respective health literacy aspects. The HLQ scoring is performed separately for each scale and summed to the total score, with no categorical scoring or cut-off points.
Overall, the HLQ has excellent psychometric properties. The content validity of HLQ has been verified in more than 20 countries in Europe and Asia across various settings and has good reliability, with a Cronbach’s alpha of 0.8. 30 This survey used the original English HLQ in its unmodified form.
Survey population
Undergraduate health science students aged 21–50 were recruited from the university for this survey. Eligible students from the 4-year entry-level programmes of diagnostic radiography, dietetics, occupational therapy, physiotherapy, radiation therapy, and speech and language therapy were invited to participate via student email groups, cohort group chats on messaging platforms and the circulation of participant recruitment posters for dissemination. Exclusion criteria were students who were no longer studying due to dropping out or having immediately graduated from these programmes and students in the accelerated programmes whose studies would be completed in less than 4 years. A minimum sample size of 91 was targeted based on the sample size calculation with a 95% confidence level, 50% population proportion with an estimated population size of 1430 (estimated total health science students’ number in the local university) and a margin of error of 10%.
Data collection and management
The HLQ and a simple demographic survey were disseminated via a link using the online survey platform QualtricsXM. The demographic data obtained included participants’ age, gender, language literacy, course of study and year of study. The survey link was disseminated as part of the study invitation, accompanied by a recruitment message and a poster summarising the study information. Participants were advised to complete the survey in one sitting, although the ‘save’ function was available in the event of survey fatigue. Participants were required to submit the last four of the nine alphanumeric characters of their National Registration Identity Card number as their anonymised personal identifier. Participants could resume the survey via this four-letter code and assess and/or resume the questionnaire whenever they preferred. These four alphanumeric characters also served to prevent duplicate submissions.
Statistical analysis
Duplicate and incomplete survey entries were excluded from the analysis. Microsoft Excel was used for data tabulation and mean calculation based on the template and formulas provided by the HLQ User Package. IBM SPSS (version 29) was used in the statistical analysis of the data. Data distribution normality was determined using the Shapiro–Wilk test. Descriptive statistics, mean scores and standard deviations (SDs) were generated for the HLQ scores. The Mann–Whitney U-test analysed gender comparisons and the Kruskal–Wallis test for other nonparametric demographic categories. Statistical significance was defined as a p < 0.05 and examining 95% confidence intervals. Cohen’s d effect size was calculated to indicate the magnitude of difference between groups.
Results
Demographic of participants
Initially, 166 surveys were returned. However, 55 were excluded due to incomplete and missing information. In total, 111 completed survey entries were used for data analysis, indicating a 7.7% response rate and an 8.94% error margin with a confidence level of 95% out of 1430 students at the end of the collection period (Figure 1). Table 1 details the demographic breakdown of participants. The age of the participants ranged from 21 to 48. Of all the years of study, Year 3 students had the highest number of participants at 48.6% (n = 54), followed by Year 4 students at 28.9% (32). Year 1 and 2 students formed 11.7% (n = 13) and 10.8% (n = 12) of participants, respectively. More than half the participants identified themselves as female, making up 64.3% (n = 72) of the participants. The course distribution of participants was skewed towards physiotherapy students, with physiotherapy students forming 62.2% (n = 69) of participants, while 22.5% (n = 25) were occupational therapy students, and 10.8% (n = 12) were diagnostic radiography students. Only five responses from dietetics (4.5%) and nil returned from the radiation therapy and speech and language therapy students. All participants were literate in English, with 88.3% (n = 98) understanding a second language.

Survey participant recruitment flowchart.
Demographic data of participants (n = 111).

HLQ
Female participants scored higher in eight of the nine scales of HLQ with a total score of 30.67 (SD = 0.61), while male participants scored higher only in Scale 3 ‘Actively managing my health’ and reported with a total score of 29.83 (SD = 0.53).
The mean scores from each HLQ scale stratified by years of studies are presented in Table 2, while Table 3 presents the mean scores from each HLQ scale stratified by programme. As a whole (Table 2), on Scales 1–5, where responses were based upon a 4-point Likert-type scale, participants broadly agreed with statements corresponding to Scale 4 ‘Social support for health’ with a score of 3.06 (SD) 0.54 but rated Scale 1 ‘Feeling understood and supported by health care providers’ the lowest at 2.73 (SD = 0.43). For Scales 6–9, where responses were based on a 5-point Likert-type scale, the highest scores were detected in Scale 9 ‘Understanding health information well enough to know what to do’ at 4.10 (SD = 0.36). The lowest reported scores in these scales were found in Scale 7 ‘Navigating the health care system’ at 3.75 (SD = 0.46). In general, scores were primarily clustered around 3 on Scales 1–5, signifying that participants ‘Agree’ with statements within the questionnaire and felt that tasks on Scales 6 to 9 were ‘Quite easy’ to perform as all the activities were rated with scores >3.75. Few participants obtained the highest and lowest possible scores in this study, which may indicate an absence of a floor or ceiling effect.
Health literacy scores across years of study.

HLQ: health literacy questionnaire; SD: standard deviation; CI: confidence interval; M: mean.
For Scales 1–5, scores ranged from 1 to 4. For Scales 6–9, scores ranged from 1 to 5.
Health literacy scores across allied health programmes.

HLQ: health literacy questionnaire; SD: standard deviation; CI: confidence interval; M: mean.
For Scales 1–5, scores ranged from 1 to 4. For Scales 6–9, scores ranged from 1 to 5.
Dietetics (n = 5) and physiotherapy (n = 69) students scored higher on HLQ total scores, while diagnostic radiography (n = 12) scored the lowest (Table 3). Among the courses of study, dietetics students obtained the highest mean scores for seven scales except for Scale 2 ‘Having sufficient information to manage my health’ and Scale 4 ‘Social support for health’.
Difference between course of study and course year
The Cohen’s d effect size and the pairwise asymptotic significance values from a two-sided test are displayed in Tables 4 and 5. These values represented the relationship between gender, the course of study and the course year. The Cohen’s d effect size was determined to measure the extent of the difference between genders, depicting the influence of gender on health literacy.
Differences between gender and course of health science study in HLQ expressed as Cohen’s d effect size and p values of pairwise asymptotic significance.

p value set as <0.05. *denotes p < 0.05.
Differences between years of health science study in HLQ expressed as Cohen’s d effect size and p values of pairwise asymptotic significance.
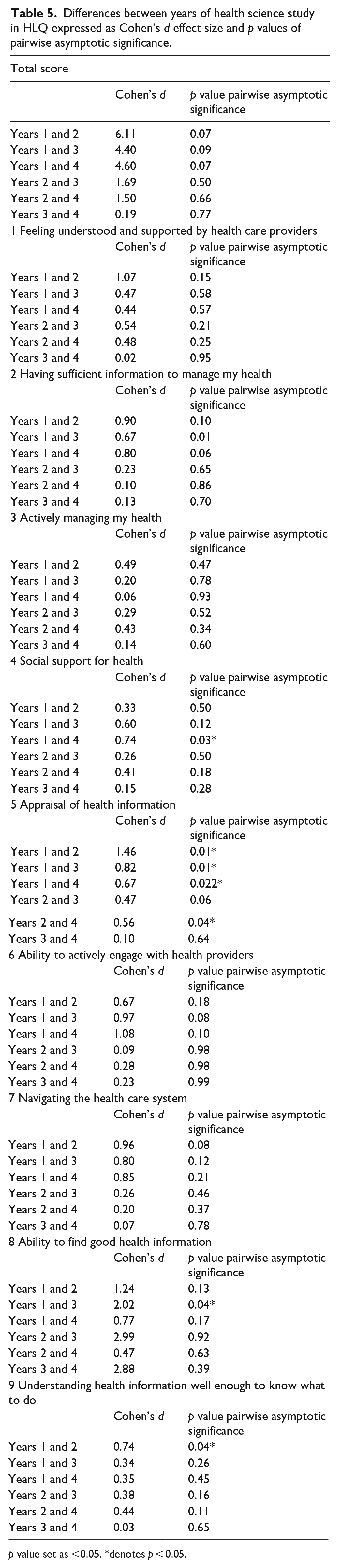
p value set as <0.05. *denotes p < 0.05.
The tabulated magnitude of difference showed a large effect size between HLQ total scores across the four health science programmes (Table 4) and observed a medium-to-large effect size in five of the nine scales. It is evident that Scale 4 ‘Social support for health’, Scale 7 ‘Navigating the health care system’ and Scale 9 ‘Understanding health information well enough to know what to do’ observed trivial to small effect size across all courses of study. A similar trend is observed in Table 5, with a large effect size on the total score across all course years, except for the comparison between Year 3 and Year 4, which showed only a trivial effect size. There are medium-to-large effect sizes on five of the nine scales between Year 1 and Year 2, 3 and 4 comparisons, while only small-to-medium effect sizes are observed on the same scales between the Year 2 and Year 3 and 4 comparisons. Notably, the magnitude of difference in the eight scales determined a trivial effect size in all the nine scales except Scale 8 ‘Ability to find good health information’.
Discussion
Data collection
To our knowledge, this is a pioneering effort to establish health literacy in health science students in Singapore. This investigation encompassed 111 participants, all enrolled in entry-level health science programmes locally. Notably, this number surpasses the minimum sample size requirement of 91. Regrettably, the data set, which includes only 9 participants who can speak one language, 98 who are bilingual and 4 who can speak three languages, is highly skewed. In line with the nature of entry-level undergraduate degrees, the majority of the participants in this study fell within the 20–29 age group (n = 98), with smaller representations from the 30–39 (n = 9) and 40–49 (n = 4) age groups. This imbalance could lead to significant errors in statistical analysis and potentially result in inaccurate reporting. Therefore, the researchers are cognizant of this unequal distribution across groups and have chosen not to examine the impact of age and language proficiency on health literacy.
Health literacy and gender
Our results support our hypothesis that gender influences health literacy. Female participants in this study attained higher scores in eight of the nine scales, except Scale 3 and the total HLQ score. The finding is consistent with several similar reports on health science or university students.1,6,19,27,31 –33 On the contrary, male participants achieved better ratings on Scale 3 ‘Actively managing my health’. Despite differing from previous reports, such a trend could be explained by the results of a recent National Population Health Survey (2020), 34 which reported that more Singaporean males exercised regularly than females and had a higher proportion of sufficient muscle strengthening. 34 This is likely due to the yearly obligation to pass their individual physical proficiency test upon completing their national service, an active requirement by male reservist men in this study’s age bracket. 35 Monetary incentives to maintain fitness levels are also given out should these individuals achieve higher levels of physical fitness, serving as motivation.
Health literacy and years of health science study
Year 2, 3 and 4 students generally achieved higher scores than Year 1 across all nine HLQ scales, with an exception observed on Scale 8 ‘Ability to find good health information’, where Year 3 students (3.03; SD = 0.37) scored lower than Year 1 (3.72; SD = 0.31) (Table 2). Interestingly, Year 2 students scored higher than Years 3 and 4 on seven of the nine HLQ scales, except for Scales 4 and 6 ‘Social support for health’ and ‘Ability to actively engage with health providers’, respectively.
Furthermore, Year 2 achieved the highest in total score among all students. This observed pattern is also evident in Table 5, where the comparison of the effect size shows a substantial difference between Year 1 versus Years 2, 3 and 4 and Year 2 versus Years 3 and 4. Our findings differ from other studies conducted among medical and health science students in China and India as significant differences were observed throughout all 3 years of education, showing a positive trend of greater health literacy with longer education.36,37 The jump in scores from Year 1 to Year 2, followed by a broadly consistent health literacy score for subsequent years, may have come about from the structure of the health science curriculums in the Singapore programmes. In Year 1, students are exposed to nondiscipline-specific modules such as health systems in Singapore. 24 There is then a shift in curriculum focus towards clinical competencies through clinical placement. Clinical placement may occur at different times depending on the students’ programmes. Some programmes may start at the tail-end of their first years and increase frequency towards their third and fourth years. The clinical placement allows students to bridge the gap between theoretical knowledge and patient care. This change in focus away from health systems education and community outreach programmes could explain the stagnation of health literacy scores in senior years. Following the same logic, this also explains the rationale that Year 3 and 4 students obtained better scores in Scales 4 and 6, with the exposure during the clinical placement. The immersive clinical placement enhances confidence in exploring ‘Social support for health’ and ‘ability to actively engage with health providers’.
In addition, the disparity in scores between students from Year 2, Year 3 and Year 4 narrowed in five out of the nine HLQ scales (Table 5). Furthermore, marginal score differences are more apparent between Year 3 and Year 4; all scales demonstrated trivial effect size except for Scale 8 ‘Ability to find good health information’, the only scale with a large effect size (Cohen’s d = 2.88). Depicting the consistent trend of higher HLQ scores as compared with the freshmen.
Health literacy and course of health science study
Comparing different health science programmes in Singapore, there seems to be a trend for diagnostic radiography students having significantly lower health literacy based on total scores and several scales (Scales 3, 5, 6 and 8). According to current literature, no study has explicitly examined diagnostic radiography students’ health literacy. Based on this study, no apparent attributing factors could be drawn from this observation. Compared with other health care professions, it could be noted that dietitians, occupational therapists and physiotherapists do have significantly greater contact time with patients.38 –41 Increased contact time with patients increases the opportunities for health promotion,42,43 which relies on one’s health literacy. Physiotherapy students are trained to promote health and well-being, and physiotherapists can change patient behaviour by role-modelling. Through role-modelling, firsthand experiences also allow physiotherapists to develop approaches to support their patients better. This may explain significantly higher scores for Scale 3 ‘Actively managing my health’ in physiotherapy students. Dieticians must assess nutritional health information sources before recommending them to patients and be able to evaluate health information well.43,44 This could explain dietetics students achieving higher scores on Scale 5 ‘Appraisal of health information’.
However, it is crucial to recognise that patients with lower health literacy may struggle with reading and understanding written preparation documents. This is significant, particularly in the field of radiation sciences, where the ability to adhere to preparation guidelines for diagnostic imaging procedures is crucial. 45 It has been proposed that those with limited health literacy often come less prepared for diagnostic examinations, leading to lower-quality diagnostic results. Medical radiation technologists have a vital role in educating patients about medical imaging examinations and assisting them in adequately preparing for these procedures. 46 Consequently, the findings of this study serve to bolster efforts aimed at improving the health literacy of diagnostic radiography students now that such a gap has been identified.
Strengths and limitations
The primary strengths of this study include the prospective cross-sectional participant recruitment and the utilisation of a validated instrument for evaluating health literacy. However, several limitations of this study should be acknowledged. There is an 8.94% margin of error with the final sample size obtained in this survey, and the sample size of 111 participants was relatively small. Furthermore, the significant skewness of the data set precludes the possibility of analysing the impact of age and spoken languages as factors influencing health literacy in this study that targeted entry-level undergraduate health science students. We also recognise that this purposive sample may overrepresent physiotherapy students. Participation in the survey was voluntary, and some individuals may have opted out due to their self-perceived higher or lower health literacy levels. In addition, the self-administered version of HLQ was the primary instrument used in this study. Consequently, individuals with lower literacy levels may have chosen not to return the questionnaire for similar reasons. However, using the HLQ to gauge the health literacy of various student groups proved feasible and practical. The individual scale scores offered a detailed and action-oriented overview of the health literacy strengths and weaknesses among the different student groups.
Conclusion
This report attempts to establish the health literacy level of health science students in Singapore. The results support the hypothesis that health literacy is influenced by gender, and it increases with the level of health science education. This trend is attributed to the increased exposure to the health care system and health care education as undergraduates progress through the years of study. Students would benefit from having health literacy education earlier. Therefore, it is imperative to optimise educational materials throughout the courses to address potential health literacy deficits, ensuring that students have a high level of health literacy upon graduation.
Supplemental Material
sj-docx-1-map-10.1177_27550834231222382 – Supplemental material for Cross-sectional survey of health literacy among health science students in Singapore
Supplemental material, sj-docx-1-map-10.1177_27550834231222382 for Cross-sectional survey of health literacy among health science students in Singapore by Kenrick Y Cheong, Syed Munauwwar B Syed Mahmud, Nicole W Chng, Geralyn J Kwek, Clement C Yan and Meredith T Yeung in The Journal of Medicine Access
Supplemental Material
sj-pdf-2-map-10.1177_27550834231222382 – Supplemental material for Cross-sectional survey of health literacy among health science students in Singapore
Supplemental material, sj-pdf-2-map-10.1177_27550834231222382 for Cross-sectional survey of health literacy among health science students in Singapore by Kenrick Y Cheong, Syed Munauwwar B Syed Mahmud, Nicole W Chng, Geralyn J Kwek, Clement C Yan and Meredith T Yeung in The Journal of Medicine Access
Footnotes
Acknowledgements
The authors thank the Health and Social Sciences Cluster of the Singapore Institute of Technology for the support and all subjects who participated in the study.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.