
Abstract
Background:
During the first year of the COVID-19 pandemic, more than one-third of US older adults (aged 65 years and older) reported delaying medical care. Delayed health care may exacerbate short- and long-term health changes in older adults. Older adults more likely to delay health care may benefit from targeted follow-up to return these individuals to the health care system.
Objective:
The aim of this study was to describe pre-pandemic sociodemographic, psychological, cognitive, and medical factors associated with delayed health care among US older adults during the COVID-19 pandemic.
Design:
We conducted a secondary analysis of 2905 participants from the National Health and Aging Trends Study (NHATS), a nationally representative, prospective cohort of US older adult Medicare beneficiaries.
Methods:
Pre-pandemic factors were reported at the Round 9 interview (2019). Delayed health care, including medical (e.g. usual doctor) and supplementary (e.g. dental) care, was reported on the COVID-19 questionnaire (2020). We calculated adjusted odds ratios using weighted logistic regression, accounting for the NHATS sampling design.
Results:
Overall, 40% of participants reported delayed care. After adjustment, female participants and those reporting fair (vs good) health were consistently more likely to delay health care while persons with lower income or excellent health were less likely to delay care. Other associations varied by care type.
Conclusion:
Women and those with higher income or fair health before the COVID-19 pandemic were more likely to delay care during the pandemic. Our results may inform targeted outreach to older adults who delayed care during the COVID-19 pandemic, or other disruptions to the health care system, to return these individuals to care and promote better management of their health needs.
Introduction
By 30 June 2020, one-third of US older adults aged 65 years and older reported delaying or avoiding medical care due to concerns over the coronavirus disease-19 (COVID-19) pandemic. 1 Although the pandemic evolved over time, a similar proportion of older adults continued to report delaying care due to COVID through at least January 2021. 2 Care delays were evident through reductions in diagnostic cardiovascular procedures, cancer screenings and treatment, and emergency department visits.3 –8 Outside of the COVID-19 pandemic, older adults tend to have more complicated health needs, including a greater number of prescription medications and multiple chronic conditions, which may require a higher level of physician involvement for health management. 9 Health care delays appear to exacerbate symptoms of existing health conditions, including those associated with heart failure, chronic obstructive pulmonary disorder, and dementia.10 –12 Furthermore, older adults may have underlying “silent” medical conditions (e.g. hypertension) that are likely to go undetected outside of a medical setting, and therefore, may be more vulnerable to short-term and long-term health effects from delayed medical care. 9
Early COVID-19 guidelines encouraged individuals to maintain social distancing and avoid high-risk behaviors, which may have extended to the avoidance of health care settings.13,14 Cross-sectional studies suggest sociodemographic patterns; those who delayed care during COVID-19 were more likely to be female, non-Hispanic Black or Hispanic, and have higher household income.1,15 –17 Furthermore, a prior longitudinal cohort study of older adults found that those who were female and had poorer self-rated health were more likely to delay care, while those who were Black and older than 70 years were less likely to delay care. 2 Fear of severe acute respiratory syndrome coronavirus 2 (SARS-COV-2) infection has been identified as a barrier to seeking care during the COVID-19 pandemic. 18 Individuals with pre-existing anxiety or depression may be particularly susceptible to fear of the virus and avoid situations perceived as high risk, a hypothesis supported by cross-sectional studies that report associations between concurrent depressive symptoms, anxiety, and delayed medical care during COVID-19 among older adults.16,19,20 In addition, as COVID-19 is more severe in those with certain underlying medical conditions (e.g. obesity, diabetes, and cardiovascular disease), these patients may delay medical care out of concerns about their personal risk following SARS-COV-2 exposure.21,22 Supporting this, cross-sectional studies of delayed care during COVID-19 indicate that patients with higher perceived risk of contracting or dying from COVID-19 and those with more than two pre-existing comorbidities were more likely to delay care.15,16,23
To date, most studies of individual-level factors associated with health care delays during the COVID-19 pandemic used a cross-sectional design. Although other longitudinal cohorts have analyzed care delays among their study participants, all but the National Social Life, Health, and Aging Project (NSLHAP) assessed both the individual characteristics and health care delays during the COVID-19 pandemic and did not use the pre-pandemic data collected from their participants.2,17,20,23 As such, they cannot provide insight into whether the mental health symptoms or comorbidities associated with delays in care pre-dated or were brought on by the pandemic, or eliminate the possibility that the delayed care led to the development of the symptoms or comorbidities (i.e. reverse causation). Furthermore, cross-sectional studies largely identify prevalent factors associated with delayed health care. However, these prevalent factors may not be documented in the patient’s medical record if they developed during the period in which the patient avoided care, and therefore, may be of limited utility to health care providers seeking to identify patients in need of additional outreach to re-establish their relationship with the health care system. Therefore, the purpose of our study was to complement existing work by describing pre-pandemic factors associated with delayed health care among US older adults during the COVID-19 pandemic, using data from the National Health and Aging Trends Study (NHATS).
Methods
Study design and sample
This secondary analysis used data collected by NHATS, a nationally representative, prospective cohort of Medicare beneficiaries (including those enrolled in both traditional Medicare and Medicare Advantage plans) aged 65 years and older living in the contiguous United States. NHATS was established in 2008 to study the aging US population with the aim of reducing disability and improving quality of life at older ages. The first cohort of NHATS participants was recruited in 2011 and the sample was replenished in 2015. All members listed in the Medicare enrollment file were eligible for inclusion and selected using the three-stage NHATS complex probability sampling design. The complex probability sampling selected 95 counties from the contiguous US, from which 655 zip codes were sampled. Within these zip codes, 8245 individuals were enrolled as part of the 2011 cohort and an additional 4182 were recruited during the 2015 sample replenishment, for a total sample size of 12,427. Black beneficiaries and those aged 80 years and older were intentionally oversampled. NHATS targeted a sample size of 8500 participants at both Round 1 and after the Round 5 replenishment to ensure adequate sample size for analyses of activities of daily living over time, by age group and race/ethnicity. Additional details regarding NHATS sample design and selection are described elsewhere. 24 NHATS is sponsored by the National Institute on Aging (Grant No. NIA U01AG032947) through a cooperative agreement with the Johns Hopkins Bloomberg School of Public Health.20 –22 NHATS data collection was approved by the Johns Hopkins Bloomberg School of Public Health Institutional Review Board and respondents provided signed informed consent prior to enrollment. 25 This analysis uses only publicly available, de-identified data and was determined by the George Washington University Milken Institute School of Public Health student oversight review process to be not human subjects research (Reference No. 1750).
From 2011 to 2020, NHATS completed 10 rounds of annual data collection with either the sample person or a proxy, if the sample person was unable to complete the interview themselves. Rounds 1–4 were completed with the 2011 sample and Rounds 5–10 included both the remaining 2011 cohort members not lost to follow-up or deceased and the 2015 replenishment sample. In addition to the 10 data collection rounds, conducted in-person (Rounds 1–9) or by phone (Round 10, due to COVID-related restrictions), a self-administered COVID-19 questionnaire was mailed to all participants who completed a Round 10 sample person or proxy interview (N = 3961).
This analysis used data from the Round 9 in-person interview, conducted from May to October 2019 with either the sample person or a proxy, to define pre-COVID factors. All participants who completed a Round 10 interview (May–October 2020) were invited to complete the COVID-19 supplementary questionnaire by mail. The COVID-19 questionnaires were distributed between May and October 2020 and returned questionnaires were accepted from May 2020 through January 2021 to ensure adequate follow-up time for all eligible participants to complete the questionnaire. Most COVID-19 questionnaires were completed in July and August 2020 and were used to ascertain whether persons delayed care during the pandemic. 26 Of the 3961 participants eligible for the COVID-19 questionnaire, 3257 returned a completed questionnaire (unweighted response rate: 82.2%). All data collection materials are available at https://www.nhats.org/researcher/nhats.
As this was a secondary analysis, the analytical sample size was determined based on the available data. Respondents were eligible for inclusion in this analysis if they completed both the Round 9 interview and COVID-19 questionnaire. Participants were excluded if they were missing data for any of the covariates reported at the Round 9 interview or did not complete the delayed care question on the COVID-19 questionnaire. Identification of the sample is described in Figure 1. Restriction to the eligible participants was achieved using the domain statement in the SAS survey procedures. The final eligible sample size was 2905.

Flowchart of eligible study respondents.
Dependent variables
Delayed health care during the COVID-19 pandemic was measured on the self-administered COVID-19 supplementary questionnaire and represents delays over the first ~10 months of the pandemic (through January 2021). Respondents were asked “During the COVID-19 outbreak, has there ever been a time when you needed or had planned to see a doctor or other health care provider but put off getting care?” (Yes/No). Participants who responded “Yes” were asked what type of care was delayed (usual doctor, specialist, vision, hearing, dentist or hygienist, surgery, physical therapy, mental health care, emergency or urgent care, medication, or other). NHATS adapted these delayed care questions from the Health and Retirement Study COVID telephone module. 26
To assess whether associations differ by health care discipline, we classified delays in care into three categories: any health care, medical care, or supplementary care. Delaying any health care was based on the respondent’s yes/no answer to putting off any needed or planned care from a doctor or other health care provider. Delayed medical care was defined as delaying usual doctor, specialist, surgery, emergency or urgent care, laboratory, medication-related, or other visits. Delayed supplementary care was defined as delayed vision, hearing, dental, physical therapy, or mental health care visits.
Independent variables
Independent variables were chosen to represent factors previously linked to care delays, and included sociodemographic, psychological health, cognitive health, and medical conditions.21,22 NHATS uses validated instruments to assess anxiety (Generalized Anxiety Disorder 2-item (GAD-2) scale), depressive symptoms (Patient Health Questionnaire 2-item scale), and dementia (NHATS dementia classification).27 –29 The remaining questions are similar to those used in multiple other settings (e.g. age, gender, and self-rated health status), including the Health Retirement Study and the NSLHAP.2,17
Sociodemographic variables
Age, gender, race/ethnicity, census division, living in a metropolitan area, marital status, income, and self-rated health status were based on the Round 9 interview. Age was categorized as 65–74, 75–79, 80–84, 85–89, and >90 years. Fewer than 1% of participants were 65–69 years old at the time of the Round 9 interview and were combined with the 70- to 74-year-old category. Gender (female or male) and race/ethnicity (non-Hispanic White, non-Hispanic Black, Hispanic, or other) were self-reported at enrollment. Marital status (married or living with a partner or not married or living with a partner) and health status (excellent, very good, good, fair, or poor) were self-reported at the Round 9 interview. Census division was classified by NHATS based on the participant’s address at the Round 9 interview and categorized into four regions: North, Midwest, South, and West. Metropolitan area was derived by NHATS by linking the participant’s address at Round 9 to the 2013 Urban–Rural Continuum Codes from the US Department of Agriculture Economic Research Service and categorized as living in either a metropolitan or non-metropolitan area. 30 NHATS imputed five income values for the 31% of the sample who did not provide an exact value for income. We categorized the first imputed value into income quartiles (<US$18,000, US$18,000–US$35,000, US$35,000–US$68,000, and >US$68,000).
Pre-pandemic psychological and cognitive health
Anxiety symptoms, depressive symptoms, and dementia were measured at the Round 9 interview using validated instruments.27 –29 Anxiety symptoms were assessed using the GAD-2 scale and scored on a scale from 0 to 6 points. 27 A score of 3 or higher on the GAD-2 was classified as consistent with the presence of anxiety symptoms. 27 Depressive symptoms were assessed using the Patient Health Questionnaire 2-item (PHQ-2) scale and also scored from 0 to 6 points. 28 A score of 3 or higher on the PHQ-2 indicated the presence of depressive symptoms. 28
To assess probable or possible dementia, we used the NHATS dementia classification method. 29 Dementia classification was based on at least one of the following: (1) report of a dementia diagnosis from a health care provider, (2) a score of 2 or greater on the Eight-Item Informant Interview to Differentiate Aging and Dementia (AD8) indicating probable dementia, or (3) performance at or below 1.5 (possible) or 2 (probable) standard deviations from the mean participant scores on cognitive tests of memory, orientation, and executive function.
Pre-pandemic medical history
We considered eight pre-pandemic medical conditions associated with more severe COVID-19 outcomes and reported at the Round 9 interview: high blood pressure/hypertension, heart attack/myocardial infarction, heart disease (e.g. angina, congestive heart failure), stroke, obesity, diabetes, cancer, and lung disease (e.g. emphysema, asthma, and chronic bronchitis).21,22 For obesity, we calculated body mass index (BMI) from self-reported height and weight. Respondents with a BMI ⩾ 30 kg/m2 were considered to have obesity. For the other seven health conditions, we considered the respondent to have a history of that condition if a doctor’s diagnosis was self- or proxy-reported during any of the pre-COVID interviews. We also assessed whether the presence of multiple comorbidities was associated with delayed medical care and classified participants into having 0–1 versus 2 or more conditions of interest.
Statistical analysis
We performed univariate analyses to derive frequencies for each factor of interest. Bivariate analyses were conducted to determine the unadjusted associations between each factor and the delayed care outcomes. Separate multivariate logistic regression models were used to quantify the association between each factor and the three delayed care outcomes, adjusting for the presence of all other characteristics. All analyses were performed in SAS Version 9.4 (SAS Institute, Cary, NC). We used the SAS complex survey procedures, and the sample weights provided by NHATS with the COVID-19 questionnaire data, to account for the complex survey design of NHATS. Probability of selection into the NHATS cohort differs by race/ethnicity and age, with intentional oversampling of beneficiaries who are Black or older than 80 years of age, and participants are sampled using geographic stratification and clustering. Use of the analytic weights is necessary to account for this differential probability of selection and generate nationally representative estimates of Medicare beneficiaries.
Results
The unweighted and weighted sample characteristics are shown in Table 1. The weighted sample was 55% female, 80% non-Hispanic White, and 67% had at least two pre-pandemic comorbidities. Delayed care during the first ~10 months of the COVID-19 pandemic was common: 40.2% delayed any type of health care, 30.9% delayed medical care, and 29.2% delayed supplementary care.
Pre-pandemic characteristics of included NHATS respondents (unweighted N = 2905).
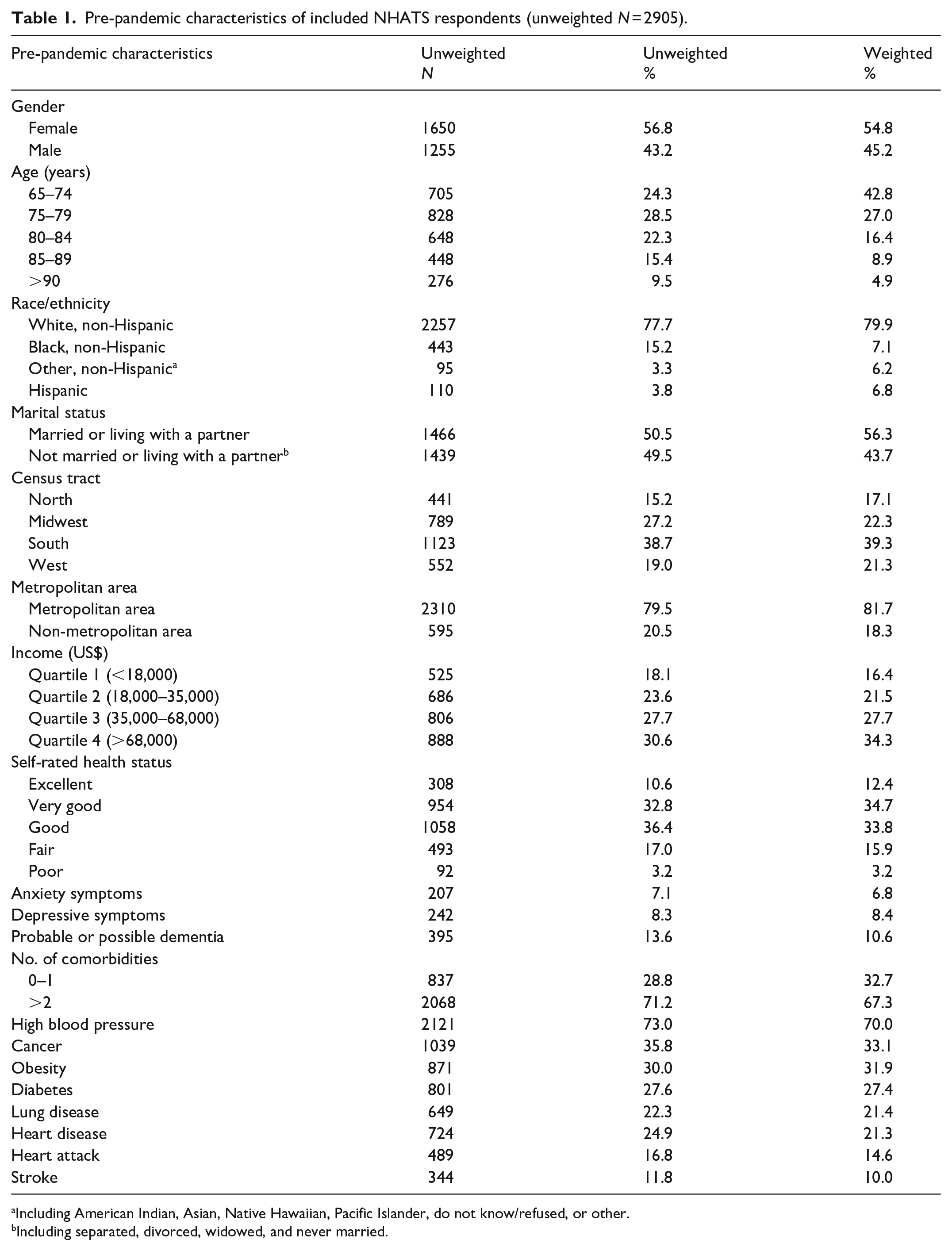
Including American Indian, Asian, Native Hawaiian, Pacific Islander, do not know/refused, or other.
Including separated, divorced, widowed, and never married.
Delayed any type of health care
Unadjusted and adjusted associations between pre-pandemic characteristics and delay in any health care type are provided in Table 2. After adjustment, respondents were more likely to delay any health care if they were female (adjusted odds ratio (aOR) = 1.69, 95% confidence interval (CI): 1.39, 2.04) or reported fair health status (vs good health status—aOR = 1.90, 95% CI: 1.34, 2.68) prior to the COVID-19 pandemic. Respondents were less likely to delay health care if they reported excellent health status (vs good—aOR = 0.73, 95% CI: 0.54, 0.98), lower income (Quartile 1 (Q1) vs Q4: aOR = 0.47, 95% CI: 0.29, 0.76; Q2 vs Q4: aOR = 0.51, 95% CI: 0.36, 0.76; Q3 vs Q4: aOR = 0.58, 95% CI: 0.44, 0.75), or depressive symptoms (aOR = 0.58, 95% CI: 0.38, 0.91), after adjusting for all other characteristics.
Associations between pre-pandemic sociodemographic, psychological/cognitive health, and medical history with delayed health care among US Medicare beneficiaries during the COVID-19 pandemic.
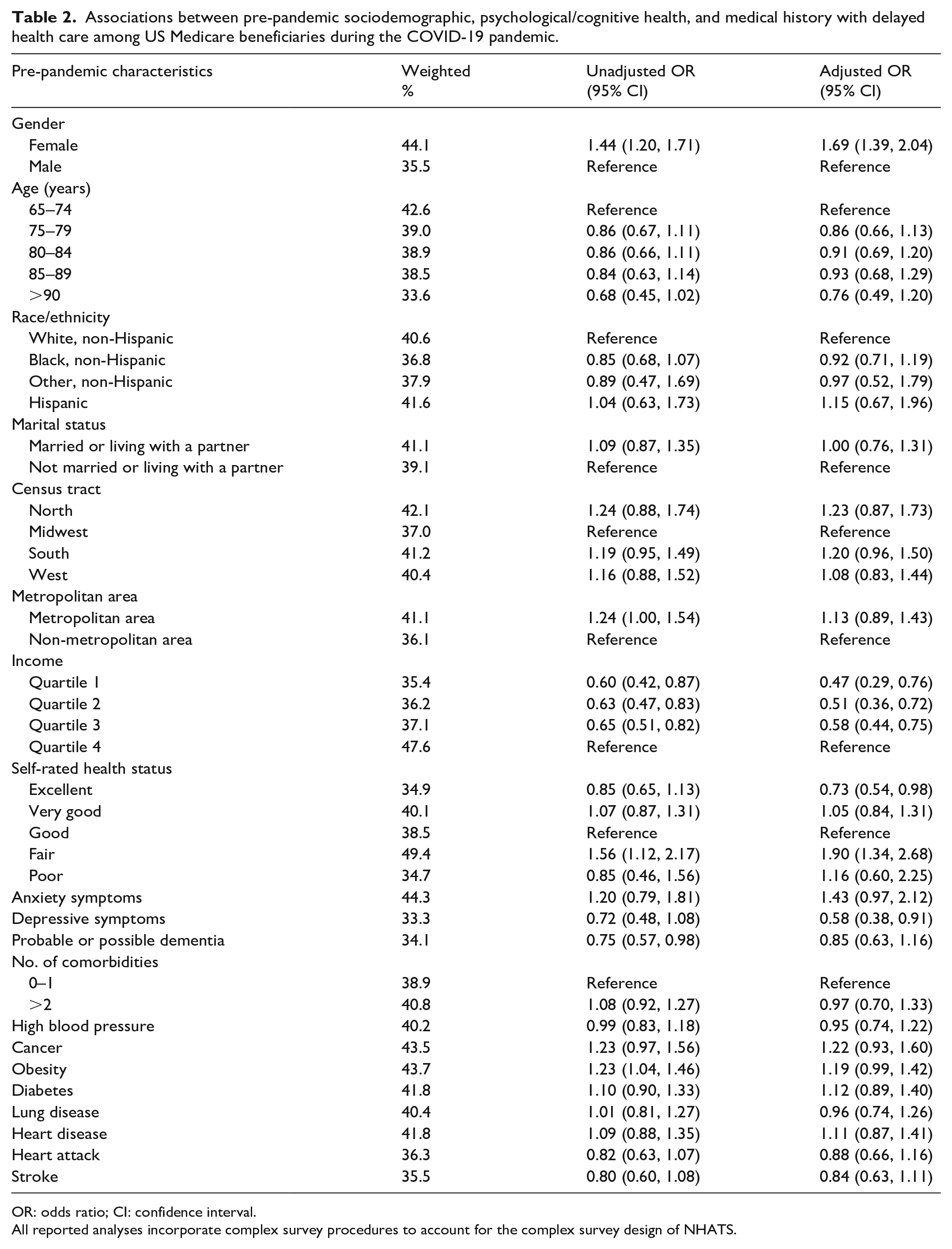
OR: odds ratio; CI: confidence interval.
All reported analyses incorporate complex survey procedures to account for the complex survey design of NHATS.
Delayed medical care
Unadjusted and adjusted associations between pre-pandemic characteristics and delay in medical care are provided in Table 3. Respondents were more likely to delay medical care if they were female (aOR = 1.41, 95% CI: 1.16, 1.72), reported fair health status (vs good—aOR = 1.62, 95% CI: 1.13, 2.34), had anxiety symptoms (aOR = 1.58, 95% CI: 1.06, 2.36), or diabetes (aOR = 1.27, 95% CI: 1.02, 1.57) prior to the pandemic. Those who were less likely to delay health care were lower income (Q2 vs Q4: aOR = 0.63, 95% CI: 0.46, 0.88; Q3 vs Q4: aOR = 0.73, 95% CI: 0.55, 0.96) or reported excellent health status (vs good—aOR = 0.71, 95% CI: 0.52, 0.97) prior to the pandemic.
Associations between pre-pandemic sociodemographic, psychological/ cognitive health, and medical history with delayed medical care (usual doctor, specialists, emergency or urgent care, surgery, laboratory or screening tests, medication-related visits) among US Medicare Beneficiaries during the COVID-19 pandemic.

OR: odds ratio; CI: confidence interval.
All reported analyses incorporate complex survey procedures to account for the complex survey design of NHATS.
Delayed supplementary health care
Unadjusted and adjusted associations between pre-pandemic characteristics and delay in supplemental care are provided in Table 4. Respondents who delayed supplementary health care were more likely to be female (aOR = 1.85, 95% CI: 1.51, 2.27), live in a metropolitan area (aOR = 1.36, 95% CI: 1.02, 1.81), report fair health status (vs good—aOR = 1.79, 95% CI: 1.18, 2.71), and report a history of cancer (aOR = 1.37, 95% CI: 1.11, 1.68). Delaying supplementary health care was less likely among those with excellent health status (vs good—aOR = 0.67, 95% CI: 0.47, 0.96), lower income (Q1 vs Q4: aOR = 0.41, 95% CI: 0.26, 0.65; Q2 vs Q4: aOR = 0.44, 95% CI: 0.31, 0.63; Q3 vs Q4: aOR = 0.56, 95% CI: 0.43, 0.74), depressive symptoms (aOR = 0.46, 95% CI: 0.29, 0.74), or history of stroke (aOR = 0.67, 95% CI: 0.48, 0.94) prior to the pandemic.
Associations between pre-pandemic sociodemographic, psychological/cognitive health, and medical history with delayed supplementary health care (dental, vision, hearing, physical therapy, and mental health) among US Medicare Beneficiaries during the COVID-19 pandemic.
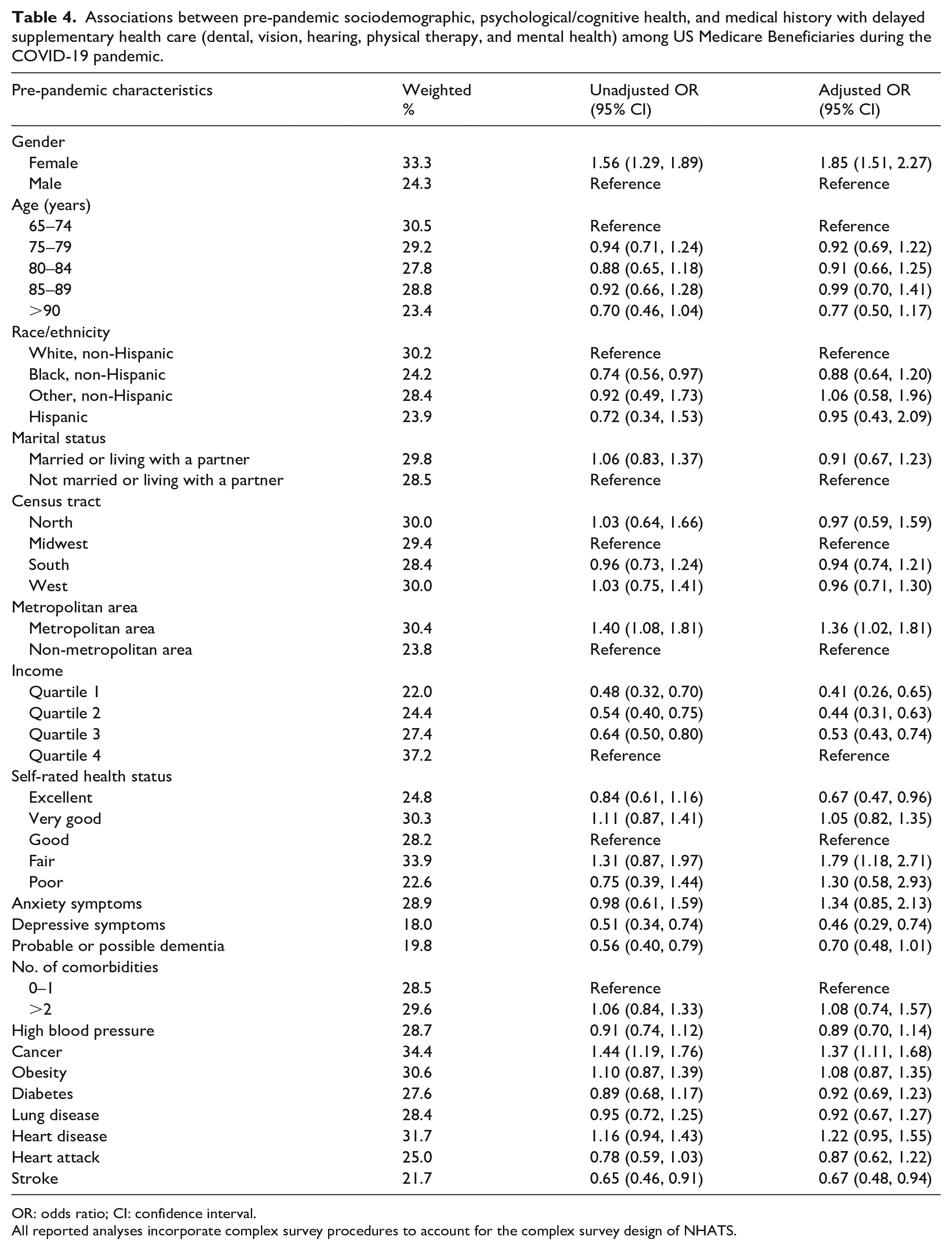
OR: odds ratio; CI: confidence interval.
All reported analyses incorporate complex survey procedures to account for the complex survey design of NHATS.
Discussion
Our study examined the associations between pre-pandemic characteristics of US older adults and health care delays during the COVID-19 pandemic. We found that, during the first ~10 months of the COVID-19 pandemic, female participants and those reporting fair health status were consistently more likely to delay health care, including both medical care and supplementary care, while those with lower income and excellent health status were consistently less likely to delay care.
Other associations varied by the type of care delayed. Persons with anxiety symptoms were more likely to delay medical care, but this association was not observed with supplementary care. In contrast, those with a prior cancer diagnosis and those living in a metropolitan area were more likely to delay supplementary care, while those with depressive symptoms or prior stroke were less likely to delay supplementary care, but these associations were not observed with medical care. Finally, multimorbidity and most health conditions associated with more severe COVID-19 were not independently associated with increased delays in any health care, medical care, or supplementary care.
A prior study conducted in the NSLHAP also analyzed longitudinal data. Our study confirms their findings that female respondents and those with poorer self-rated health were more likely to delay health care. The NSLHAP analysis differs from our own in that multimorbidity was associated with increased likelihood of delayed care, where we found no association. This discrepancy may be at least partially explained by the inclusion of different comorbidities in our two studies. For example, we included obesity, but not dementia, in our multimorbidity measure, whereas the NSLHAP analysis included arthritis and dementia, but not obesity, in the comorbidity count. Our findings further build on the work conducted by this study due to our inclusion of validated mental health assessments (vs self-rated mental health). 2
Other than the NSLHAP analysis, however, most prior studies of individual-level factors associated with delayed care among older adults during the COVID-19 pandemic used a cross-sectional design to analyze surveys collected during the COVID-19 pandemic.16,17,20,31,32 Our results complement these other reports, as our design ensures that pandemic-related delayed care did not induce the characteristics of interest. Moreover, two were conducted in the Netherlands;16,20 thus, our study expands our understanding of the US experience, given expected differences due to differing health care systems and COVID-19 infection rates across countries. For example, the Netherlands relies on general practitioner (GP) referrals to seek specialist care, while this primary care “gatekeeper” system is not used in the United States. 16 This intermediary role of the GP could play an important role in access to care and continuity of care in the Netherlands that would not factor into US health care decisions. Furthermore, by June 2020, the United States had nearly double the infection rate of the Netherlands (5925 vs 2786 cases per million), which could, in turn, affect residents’ perception of and behavior surrounding the risk of COVID-19 infection in the respective countries. 33
In the Rotterdam study, Health and Retirement Study, and a prior NHATS study, female sex and lower self-rated health status were positively associated with care delays, similar to our own findings.16,31 However, the Rotterdam study found that depressive symptoms were associated with increased care delays, the cross-sectional NHATS study observed no association, and we observed that those with depressive symptoms reported pre-COVID were less likely to delay care.16,31 Depressive symptoms significantly increased in prevalence during the pandemic. 34 The differences across studies analyzing depressive symptoms reported before versus during the pandemic suggest that onset of depressive symptoms during COVID-19, possibly resulting from the COVID-19 pandemic itself, may drive the increased likelihood of delaying care observed in the Rotterdam study, whereas pre-existing depressive symptoms do not prompt the same choice to delay care.
Among US and Canadian adults, belief in one’s robust personal health was identified as the strongest predictor of disregarding social distancing. 35 If social distancing beliefs extend to health care environments, which may be perceived as particularly high risk, this may explain our observation that those with excellent pre-pandemic self-rated health were less likely to delay care while those with fair self-rated health were more likely to delay care, compared to those rating their health as “good.” The same study found that female sex was a strong predictor of excessive avoidance of readily available and open services during the COVID-19 pandemic, which aligns with our observation that female sex is associated with health care delays. 35 Furthermore, patients with a history of stroke were less likely to delay supplementary care, while patients with a history of cancer were more likely to delay supplementary care, although neither of these associations were observed with medical care. Cancer patients may view themselves as especially high risk for COVID-19 and determine that the benefits of supplementary care do not outweigh the risk of COVID-19. 36 In contrast, the decreased likelihood of stroke survivors delaying supplementary care could reflect the value these patients place on ensuring continuous access to these services, such as physical therapy, during stroke recovery. This constellation of findings supports the theory that individual perceptions about the risks from COVID-19 play a role in care delays.
An individual’s available resources to adapt to a disruption in care may also influence their willingness to delay health care. We observed a significant association between history of diabetes diagnosis and delayed medical care. Unlike the other conditions we analyzed (e.g. cancer, heart disease), patients with diabetes may be able to regulate their condition from home, using a combination of monitoring devices, self-reporting glucose metrics to a health care provider, medications, and diet. 37 It is possible that this level of autonomy, combined with access to telemedicine and medication delivery services, led these individuals to delay care if they perceived the benefit of a health care visit to be less than the risk of contracting COVID. 38 In contrast, we observed lower-income older adults were consistently less likely to delay health care. All patients included in this study were enrolled in Medicare and would have access to health care services covered by Medicare, regardless of income. However, low-income older adults are less likely to own a smartphone or tablet, and less likely to have access to their health records or provider electronically.39 –41 Older adults who lack these resources may have felt less equipped to manage their health needs in the absence of a health care appointment and were therefore, less likely to delay or put off care.
Our study is subject to limitations. Due to sample size, we were unable to examine each health care type individually, which could mask some of the effects if one type of care, such as mental health care, saw a substantial increase in patients while other specialties in the same category (e.g. dental or vision providers) saw decreases. Furthermore, all variables were self- or proxy-reported and may be subject to misclassification or recall bias. However, all independent variables were reported prior to the COVID-19 pandemic, and thus we expect any misclassification to be non-differential. Except for imputed income, all variables are available as categorical variables in the NHATS publicly available dataset, which limited our ability to treat these variables (e.g. age) as continuous. Our study only looks at delayed health care reported at a single time point during the first 10 months of the COVID-19 pandemic. Although the pandemic evolved over the course of the study period and beyond, this evolution reflects the real-world changes in patient behavior and health care systems we might expect after a major disruption to health care. However, we cannot establish the duration of time care was delayed nor the impact in later stages of the pandemic, which represent areas for future research. Unlike other studies, we were unable to stratify by provider versus patient-initiated delays or disability status, which makes comparison to other studies more difficult.20,32 Finally, although we observed delays in health care among older adults during the COVID-19 pandemic, the long-term effects on morbidity and mortality remain unknown and represent another important area of future research.
Our study also has strengths. NHATS is a nationally representative study, and thus our findings are generalizable to the US Medicare population, which covers approximately 96% of US older adults. In addition, all predictors were measured in the pre-pandemic, Round 9 interview, which minimizes the possibility of reverse causation and provides a novel perspective on predictors of delayed care. Cross-sectional studies identify prevalent patient factors that may play a role in their avoidance of health care. Although patient health may be affected by the event that precipitated the care disruption, if the patient has avoided care thus far, the avoidance may create a gap in the patient record and the provider will lack up-to-date information regarding the patient’s health. Identifying pre-pandemic factors that are associated with delayed health care acknowledges this gap and supports health care providers leveraging the patient’s existing medical record to return the patient to the health care system.
Our study suggests important topics for future research, especially into the factors influencing the individual’s decision-making. The reasons why care was delayed, the influence of one’s resources (e.g. technology skills and access), and the value placed on continuing different types of care may all play a significant role in preventing delayed health care during crisis. Further exploring these factors may help identify preventive systems and strategies the health care system could develop to prepare in the event of another disruption.
Delaying health care could worsen existing health conditions, miss opportunities to detect developing conditions, and impact the timing and use of interventions. 20 As older adults tend to experience a higher burden of chronic medical conditions, which subsequently impact disability and quality of life, early intervention through routine care may be critical in slowing the progression of these conditions and preserving function and health as individuals age. Minimizing disruptions in care and ensuring timely follow-up and retention of older adult patients is therefore important, especially to reduce the possibility of health disparities exacerbated by missed care. The results of this study describe patient factors associated with delayed health care during COVID-19 and may help providers leverage patient records to ensure these individuals return to the health care system and receive missed services. Furthermore, these factors may identify groups that could benefit from interventions, such as telemedicine tutorials, aimed at preparing individuals to cope with disruptions in health care access. Our results may also justify targeting outreach efforts to specific groups in the event of another public health crisis such as COVID-19, especially to reach these groups early and minimize unnecessary delays in care.
Conclusion
Delayed care was common during the COVID-19 pandemic. The results of our study indicate that women and those reporting fair pre-pandemic self-rated health status were more likely to delay health care, including medical care and supplementary care, while those who were lower income, report excellent health, or have a history of stroke pre-pandemic were less likely to delay care. Associations with other predictors varied across the type of care delayed and indicate that the likelihood of delaying different types of health care may vary by patient characteristics.