
Abstract
Studies in North American and European cities since the 2000s have found that living in compact cities led to health gains for urban residents, although the benefits can be small and nuanced. Studies in China have shown mixed results, and higher urban density can be associated with adverse health outcomes due to heavier air pollution and overcrowding in Chinese cities. This paper examines the relationship between urban compactness and the self-rated health of older adults in 278 Chinese prefectural and up-level cities based on China’s 2010 census. We use a composite urban compact index incorporating population density, land use, and transportation patterns—salient characteristics according to the compact city and health literature. Our results show that living in compact cities in China is associated with significant statistical gain in self-evaluations of health for older adults, controlling for demographic, socioeconomic, and environmental variables, but the extents of the benefit vary among cities in Eastern, Central, and Western Regions of China, confirming the nonlinear relationship suggested by other studies on individual Chinese cities. The research calls for greater attention to the role of compact cities in supporting the healthy aging processes for older adults in urban China and the potential damage to their physical and mental well-being due to rapidly declining urban compactness in recent decades. The model also identifies other distinctive contributing factors for the self-rated health of older adults in three geographical zones and policy implications.
Introduction
As the majority of the world’s population lives in cities, the impact of urban built environments on people’s health becomes a prominent public policy concern (Barton, 2005; Giles-Corti et al., 2016). In North America and Europe, compact urban designs are thought to foster sustainable, just, and healthy cities (Newton et al., 2019). Researchers since the 2000s have argued that compact cities bring health benefits since higher density, mixed land uses, walkable streets, and accessible transit could improve the mental and physical health of residents by encouraging physical activities, including walking and cycling (Koohsari et al., 2019; Stevenson et al., 2016; Vojnovic et al., 2006), enhancing community belongings and social supports (Mouratidis, 2018; Xiao et al., 2020), and equalizing access to urban services (Ewing et al., 2003; World Health Organization & UN-Habitat, 2016), among others. Many empirical studies report small but statistically significant gains in health among residents in dense neighborhoods, although debates continue regarding the strength and conditions of such findings (Ewing et al., 2003, 2014; Hamidi and Ewing, 2020; Stevenson et al., 2016). The health benefits of compact cities are particularly prominent for older adults. The concept of healthy aging promoted by the World Health Organization (WHO, 2021) recognizes the neighborhood built environment as the critical facilitator for the inclusiveness, safety, and security of old adults (p. 171). Characteristics of compact cities, such as access to public facilities and transit, road connectivity, land use variety, and green spaces, are all parts of building aging-friendly macro environments (Chen et al., 2022).
Relatively little systematic research, however, has been conducted on the health impacts of the built environment in the Global South, where the urban characteristics are markedly heterogeneous and fast-changing, with little consensus on the direction of the relationship. Studies in China, for example, have yielded mixed results with findings of health penalties of dense urban living. Chinese cities have been undergoing rapid urbanization since the1990s. Its urban densities are declining but still higher than its Western counterparts in the 2010s. Chinese central cities also have more salient environmental pollution and overcrowding issues. While the streets are often choked with cars, car ownership per capita is still much lower than the Western norms; thus, the lifestyle health risks associated with driving are not as prevalent. These and other characteristics complicate the positive link between health and compactness found in the West.
Studies on older adults in urban China, while growing in disciplines such as public health and sociology, remain less visible in urban policy discussions. Tsinghua-Lancet Commission (Yang et al., 2018) reports that slightly over half of China’s 60+ population live in urban areas, and their self-rated physical and mental health has dropped between 2001 and 2013 despite the rising standard of living and longevity (p. 2154). The report attributes the drop to growing healthcare needs and costs, and dwindling family support in smaller families, even with the increasing state financial commitment, but does not explore the roles of the built environment. This is especially regrettable as older adults are the most intensive users of neighborhood facilities and services (WHO, 2021). They are also most vulnerable to changes in mobility infrastructure and neighborhood forms, two areas undergoing tremendous transformations in China since 2000. Studies on aging within individual Chinese cities have found evidence that the compact built environment benefits the physical and mental health of older adults, even though such benefits may not be linear with the rising density (Chen et al., 2022; Lang et al., 2019; Liu et al., 2021; Lu, Xiao and Ye 2017; Sun and Yin, 2018).
This paper is the first to provide a national-level assessment of the extent to which the compactness of China cities is related to the health of their older residents. We create a compactness index to measure population density, land use diversity, street connectivity, and transit accessibility with the latest available Chinese official statistics. We use self-rated health (SRH) of individuals 60 years and older as the indicator for the health status, drawing from a 10% sample of China’s 2010 census. SRH has been extensively used in the public health field, and many studies have found that it is one of the most important indicators of health conditions (Liu et al., 2019; Meng et al., 2014; Wu et al., 2013). Our modeling of SRH also incorporates demographic, economic, housing, air pollution, and urban amenity indicators that studies of aging have found important to SRH. Controlling all these variables, our results show that compactness in cities has a statistically significant association with older adults’ SRH nationally, with even stronger effects in the Central and Western Regions. We also identify other key contributing factors in SRH in different regions in China.
As populations in Chinese cities are aging, this research provides strong pieces of evidence that policymakers should re-evaluate the urban planning policies that, in the past few decades, have led to a significant reduction of urban compactness, which may undermine the supportive environment that Chinese cities used to provide for healthy aging of their older adults. It is entirely possible that the changes in compactness may have contributed to the declining physical and mental health cited in the Tsinghua-Lancet Commission Report. As other densely populated and rapidly changing Asian cities face similar challenges of expanding urban forms and population aging, the link between compact cities and older adults’ health has to be elevated to more prominence in public and policy discussion.
Compact cities and health: The West and China
Ewing et al. (2003) first measured the impacts of urban forms on health outcomes by creating a “county sprawl index” based on 448 US counties and 83 metropolitan areas. They found that residents of sprawl counties are likely to walk less, weigh more, and have more health issues. In the years since, there has been considerable research in urban planning and public health literature on the health consequences of the built environment as they exacerbate or mitigate the health problems of modern living (Ewing et al., 2014; Hamidi and Ewing, 2020).
Compact cities offer several spatial attributes such as higher residential density (Frank et al., 2004), mixed land uses (Van Cauwenberg et al., 2011), pedestrian-friendly street system (Marshall et al., 2014), and accessible public transit (Adorno et al., 2018). Figure 1 summarizes the pathways of compact cities that may positively influence health. First, compact cities facilitate a physically active lifestyle. With better-connected streets, the availability of sidewalks, more mixed land uses, and accessible recreational facilities, residents in compact cities are more inclined to walk, cycle, or use public transit, away from relying on automobiles (Ewing and Cervero, 2017; Frank et al., 2004; Stevenson et al., 2016; Koohsari et al., 2019; Vojnovic et al., 2006). Second, urban compactness encourages social interactions at the neighborhood level in denser communities, improving community belonging, socialization, and thus mental health (Mouratidis, 2018; Xiao et al., 2020). Third, compact cities enhance access to urban services for disadvantaged social groups, such as low-income residents and older adults, with shorter distances to travel to services (Burton, 2001; Ewing et al., 2003).
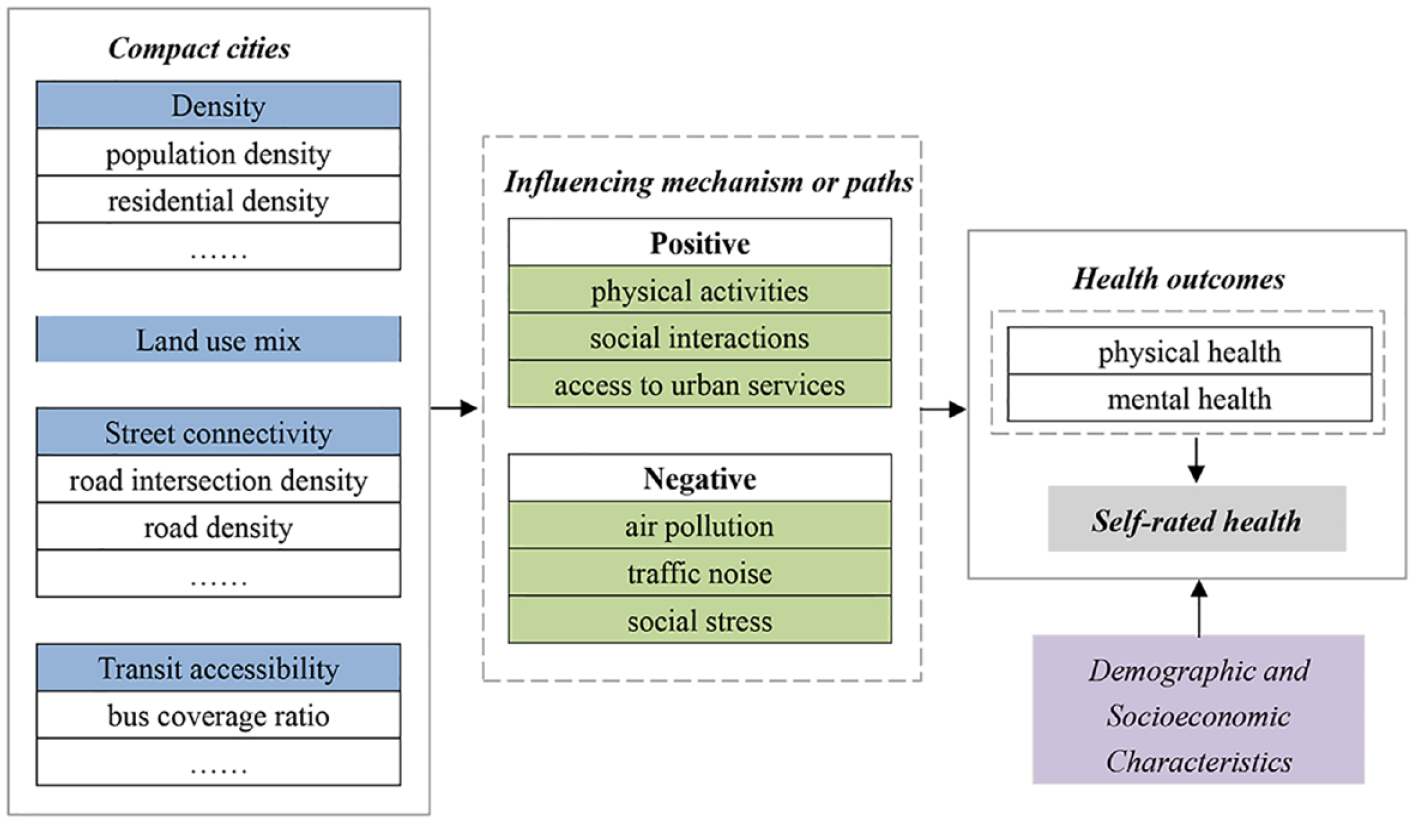
Conceptual framework of compact city and health.
Empirical evidence on compact cities is not always one way, however. Compact living may lead to adverse health outcomes due to more exposure to air pollution, traffic noise, and social stress (Ihlebæk et al., 2021; Lederbogen et al., 2011; Schweitzer and Zhou, 2010). Racial segregation and economic and social disparities between cities and suburbs can become major intervening factors (Galea and Vlahov, 2005; Yang, 2008). Overall, while many studies in the US and Europe support the conclusion that compact cities are associated with gains in physical and mental health, they also underscore that the effects are nuanced and conditional. Population density alone is insufficient to generate health benefits; socioeconomic conditions, land-use patterns, walker-friendly street layouts, and environmental pollutants are crucial intervening factors. The research designs and data across studies are so heterogeneous that some scholars found it hard to reconcile the findings (Feng et al., 2010; Truong and Ma, 2006).
Studies in cities of the Global South found far less clear a link between health and compactness. Chinese cities had a higher population density than commonly found in North America and Europe in 2010, even if that density has declined more dramatically than both high-income and low-income Asian cities since the 1990s (Table 1). Chinese cities also have less automobile ownership/per capita than Western cities, thus driving-related health risks are not the main driver for health challenges, as overcrowding and lack of green spaces may plague the population more. Qin et al. (2020), for example, found that higher residential density was associated with less walking among urban adults in Nanjing. Xu et al. (2010) found higher density is linked with a higher portion of overweight adolescents. Sun and Yin (2018) suggested a “U”-type curve between population density and obesity, so higher population density may be associated with lower obesity only to a certain point, after which the denser population may be associated with higher obesity.
Comparison of urban densities in global cities, 1995 and 2010.
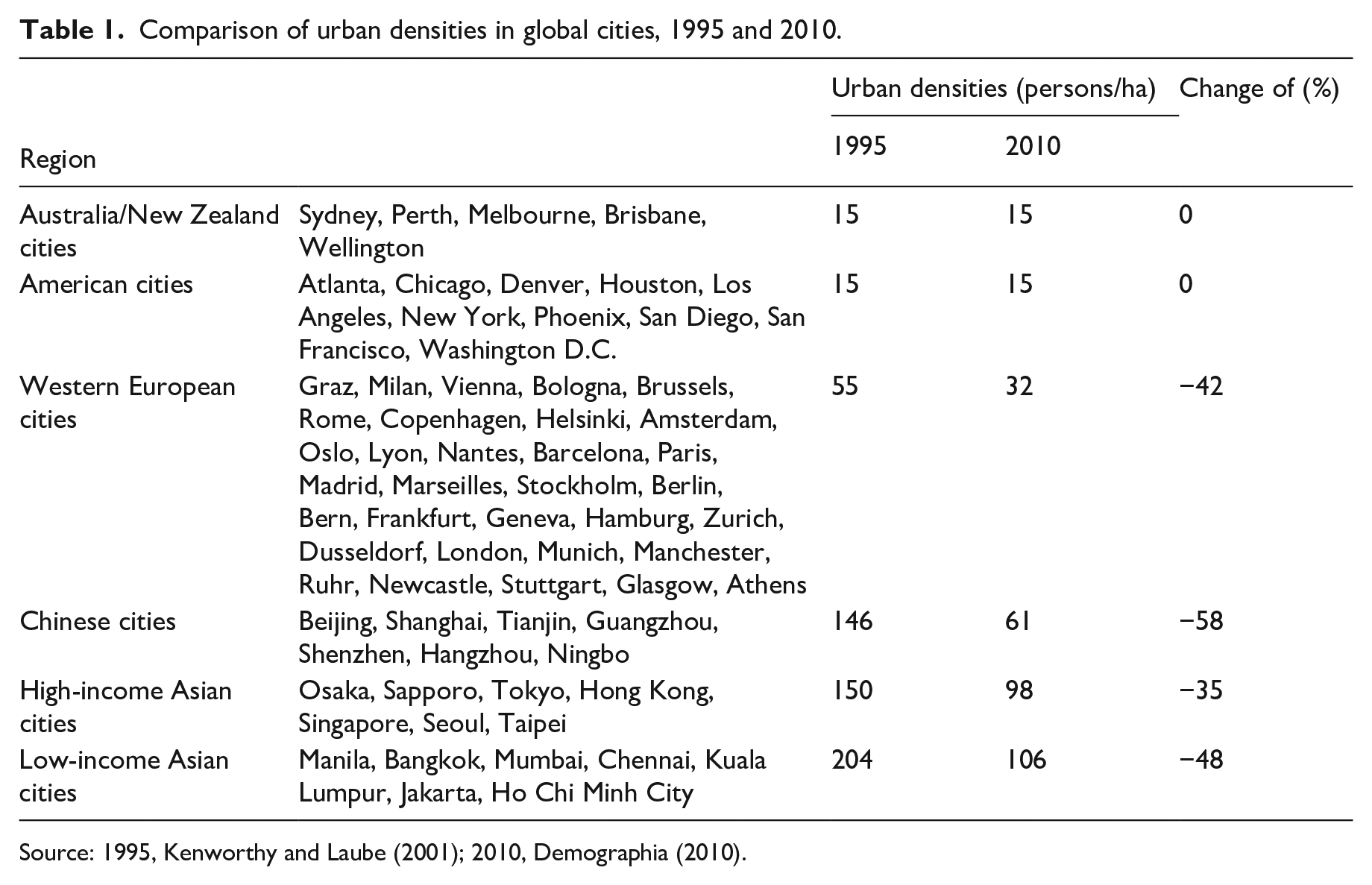
Source: 1995, Kenworthy and Laube (2001); 2010, Demographia (2010).
The distribution of air pollution and other toxins, which are more prominent in China, also contribute to the adverse effect on health in Chinese cities (Chen et al., 2008; Long et al., 2014a; Xie et al.,’s 2019; Yang et al., 2018). Xie et al.’s (2019) work on the city of Wuhan in China shows that stroke clusters are concentrated in the densely populated urban core of Wuhan, close to old industrial districts. It concludes that population and building density are among the risk factors for stroke since crowded neighborhoods have heightened exposure to industrial pollution, air pollution, and other environmental toxins. Residents also suffered from aging housing stock and less access to green and institutional land use. Su et al.’s (2016) study on Shenzhen also indicates that proximity to industrial land use may increase cancer risk, mortality, and low birth weight. Yet, unlike Wuhan, industrial zones in Shenzhen are in the periphery, not the dense core. This suggests that the heterogeneity of urban layouts and different stage of development make it hard to generalize urban density and distribution of toxins, hence the health impact.
Declining compactness and healthy aging of older adults
Despite debates regarding the health effects of the built environment-, there is a strong global policy consensus on the role of compact urban living for the health of older adults. WHO (2021) advocates the concept of healthy aging, which emphasizes the interplay between the built environment and older people’s functional abilities. Environmental attributes such as shorter distances and travel time plus easier terrain allow older adults to walk or use public transit to places of services and parks, and therefore constitute aging-friendly environments (Ko and Yeung, 2018; Liu et al., 2021). US CDC suggests that a safe and secure pedestrian environment and near-destinations to routing services allow older adults to remain independent, active, and engaged. 1 A growing volume of works in various urban contexts confirms the role of the compact built environment in supporting the physical and mental health of older adults, their quality of life and reducing the duration that they have to be placed at caring facilities (Burton, 2012; Cerin et al., 2016; Dujardin et al., 2014; Van Hoof et al., 2018).
Chinese cities used to be relatively compact by the global standard, and population aging has only started to become a policy issue in the past decade, so how the changing urban forms may have implications on older adults have not received much attention so far. Since the 1990s, China’s urban residential densities have declined sharply, driven by the imperatives of urban land development and supported by the growing urban middle class. Table 1 shows the steeper decline of urban density in China than in other Asian cities, driven by historical, political, social, and economic forces. Besides the rise of automobiles, China’s land finance models also generate intrinsic drivers for urban land expansion (Hsing, 2010; Lin, 2014; Wu, 2016; Zhou, 2015). Municipal governments favor moving residents from densely populated urban cores to the periphery to generate housing demands, as the government heavily depends on the land conversion fees from developing land from rural to urban uses. China’s emerging urban middle class also favors lower density as they perceive Western cities of lower residential density as hallmarks of higher quality of life and private automobile use as the status symbol of prestige and modernity (Deng and Huang, 2004).
Unfortunately, the trend toward less compactness is occurring without much consideration for the lives of older adults. Chinese older adults, more so than those in developed countries, are heavily dependent on walking and public transit to access essential and recreational services in their daily lives since China’s automobile age only arrived in the 1990s. 2 A small number of growing studies in Chinese cities have found significant links between the built environment and the health of older adults, but such links are nonlinear, especially in ultra-dense cities. Liu et al. (2019), using China’s 2005 census, found that counties having higher population density are associated with higher older adults SRH, although the study includes both rural and urban counties, so the positive effects of density may be attributed to a higher standard of living in cities rather than compactness, and the 2005 data are dated. Research on individual cities using ethnographical or quantitative analysis methods in Beijing (Dong and Qin, 2017; Li et al., 2022; Yu and Rosenberg, 2020) and Nanjing (Wu et al., 2019) all suggests that compact built environments promote positive physical activities, social interactions, access to daily service, and emotional belonging. Studies in Hong Kong have been particularly prolific and reveal the nonlinear relationships between the physical and mental health of older adults, and the urban compactness measured by population density, street connectivity, and land use diversity (Chen et al., 2022; Guo et al., 2021; Lang et al., 2019; Liu et al., 2021; Lu et al., 2017). Hong Kong researchers have found that very high population and street density, and mixed land uses could increase the hazards and noise for older adults and reduce their ability to engage in physical activities. Hong Kong, however, has an exceptionally high residential density compared to other Chinese cities. Most critically, governed by “the One Country-Two system” Constitution, Hong Kong does not subscribe to the land finance models of mainland China, so it has not undergone rapid urban peripheral expansion and massive housing construction like other mainland cities. There is an urgent need to understand how the compactness of heterogenous and rapidly changing Chinese cities can impact the health of older adults.
Methodology and data
Study coverage and units of analysis
Our study took the city as the basic unit of analysis. Mainland China has a total of 287 cities from the prefectural level and up. We excluded nine of them due to a lack of necessary data on compactness and other socioeconomic and environmental variables, so 278 cities remain (Figure 2a). We used the Chinese 2010 census, which is the most complete, authoritative, and up-to-date with city-level population by age group. We draw from the census and other urban statistics around 2010 to calculate other compactness indicators. Beyond the national analysis, we divide the cities into three geographical zones (the Eastern Region, Central Region, and Western Region) based on classification by the Chinese National Bureau of Statistics (Figure 2b). The Eastern Region is the most developed and wealthiest part of China, with the highest urban density. The Western Region is the least developed but also has the highest heterogeneities, with some highly prosperous cities such as Chengdu and Xi’an and many least developed cities and persistent outmigration. The Central Region is in the middle on most accounts. By 2010, the Central Region was in the midst of accelerated industrialization and is often the destination of polluting industries relocating from the Eastern Region. If the relationship between the compactness and health of older adults is nonlinear, we may see differences in regions with different levels of urban compactness.
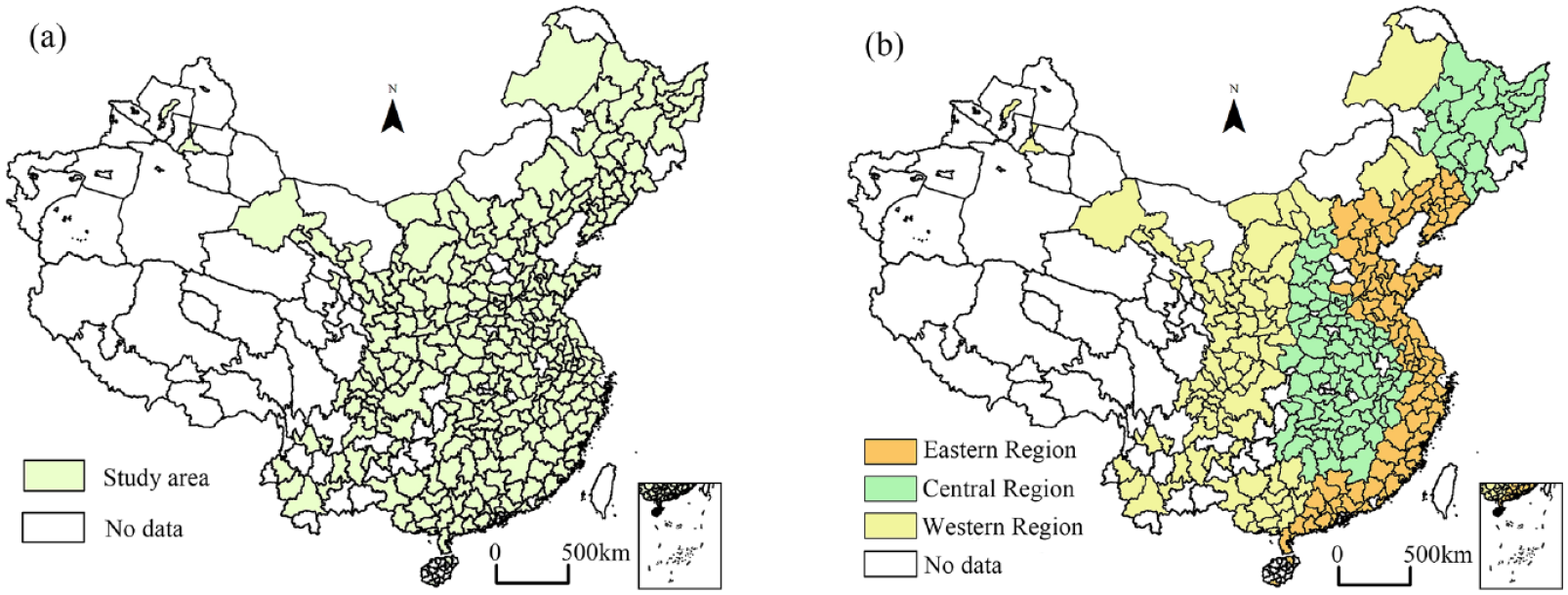
Study coverage and units of analysis.
Dependent variable: SRH%
Publicly available national health statistics at the city level are limited in China. Our SRH is derived from the question of a 10% sample in the 2010 Chinese census for individuals aged 60 years and older: “How was your health in the past month?” Four options are given: good (健康), fair (基本健康), poor but able to care for themselves(不健康,但可以自理), and needing assisted living (无法自理). The last category is problematic for this study of the interactions between built environment and health because this population is highly unlikely to venture outside the home, so their inclusion in the data can distort the pattern for the rest of the older adults. We decided to try two groups of estimation using the full sample to maintain the census representativeness and a subsample with self-care older adults, which takes out those needing assisted living to focus on those interacting intensively with the built environment. The SRH% of a city is the share of that self-rated good and fair health in either the full sample or the self-care older adults. The higher SRH% in a city, the higher proportion of older adults who believe that they are in good or fair health. SRH is a subjective measure, so it runs the risk of over/under-estimation of self-health by individuals. However, various studies have found it as a valuable health indicator. Wu et al. (2013) suggest that it is consistent with objective health measures in China. Meng et al. (2014) argue that SRH reduces recall and the investigative bias of objective indicators and is a good indicator of both disease status and self-care functions of older adults. SRH% is also the only nationally consistent indicator, making it appropriate to compare nationally.
Urban compactness index (UCI)
Similar to compact city literature, we also use population density, land use mix, street connectivity, and transit accessibility as our compactness measures (Ewing et al., 2014; Fan et al., 2019; Tsai, 2005). Studies of aging in mainland China and Hong Kong have found various components of compactness such as street connectivity (Wu et al., 2019), mixed land use, shorter distance to transit and neighborhood services (Chen et al., 2022; Lang et al., 2019; Li et al., 2022; Liu et al., 2021; Guo et al 2021) are important factors for the health of older adults. Table 2 summarizes our calculations of each indicator of the urban compact index (UCI), and we explain it below.
List of variables used on the urban compactness index.
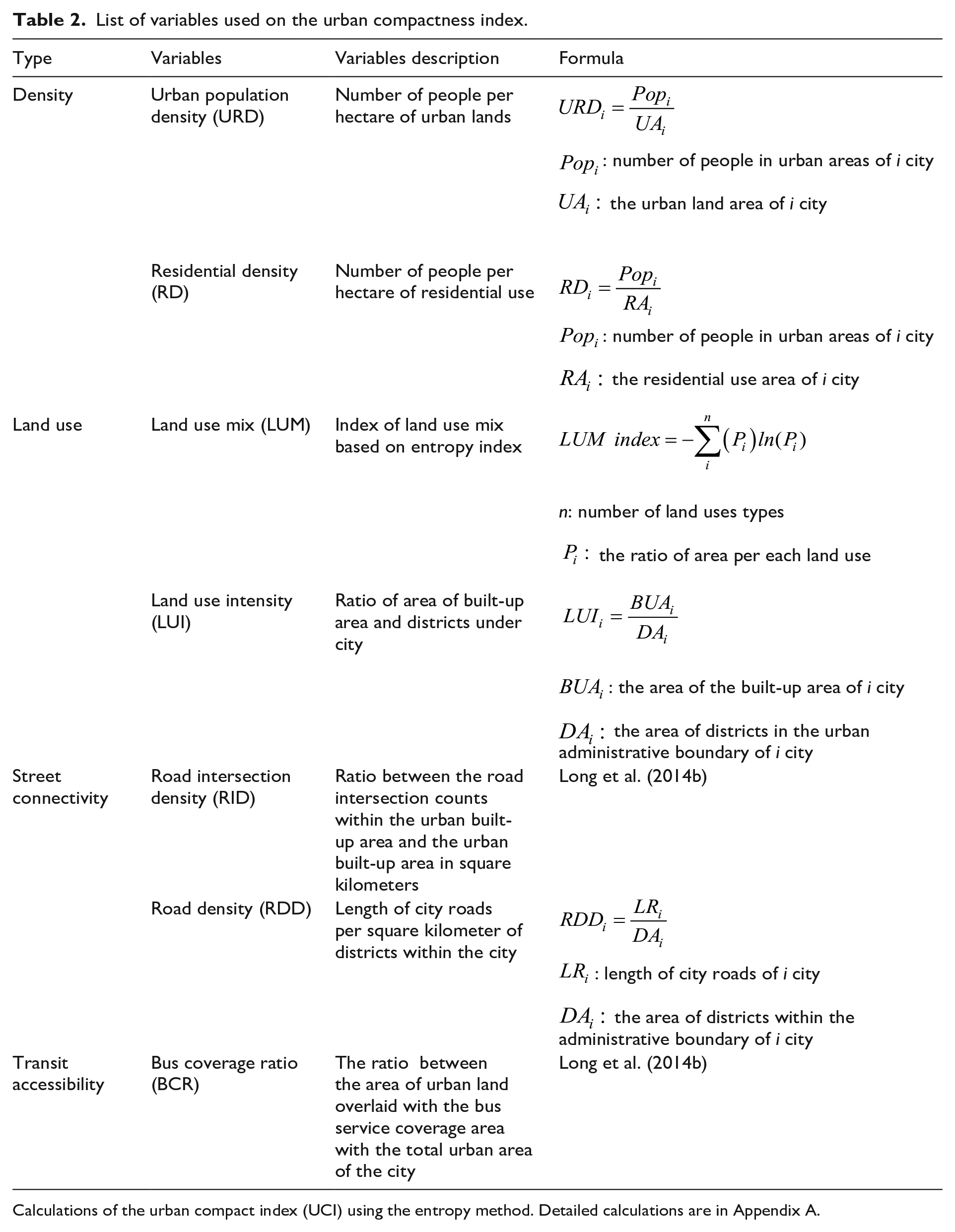
Calculations of the urban compact index (UCI) using the entropy method. Detailed calculations are in Appendix A.
To combine the seven factors into a single UCI, we use the entropy weight method, 6 which has been widely used to evaluate urban compactness/sprawl (Abdullahi and Pradhan, 2017; Shi et al., 2016; Tan and Lu, 2019). The value of the UCI is between 0 and 1; a higher UCI indicates higher compactness.
Other controlling variables
Studies on aging suggest the following demographic, socioeconomic, and environmental variables at the city level contribute to older adults’ health. All variables’ definitions and sources are presented in Table 3 and explained below.
Description of variables, data sources, and variance inflation factors (VIF).
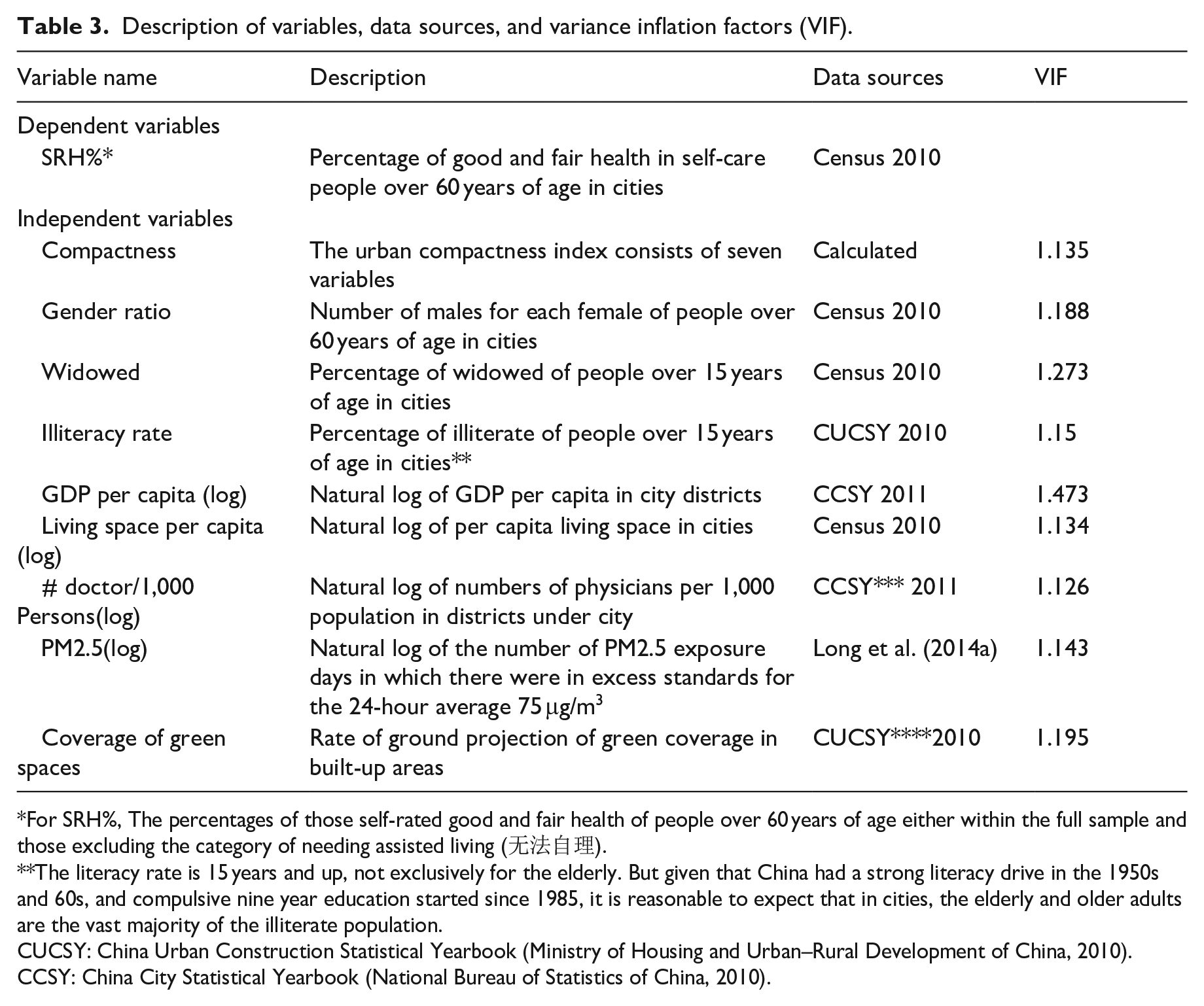
For SRH%, The percentages of those self-rated good and fair health of people over 60 years of age either within the full sample and those excluding the category of needing assisted living (无法自理).
The literacy rate is 15 years and up, not exclusively for the elderly. But given that China had a strong literacy drive in the 1950s and 60s, and compulsive nine year education started since 1985, it is reasonable to expect that in cities, the elderly and older adults are the vast majority of the illiterate population.
CUCSY: China Urban Construction Statistical Yearbook (Ministry of Housing and Urban–Rural Development of China, 2010).
CCSY: China City Statistical Yearbook (National Bureau of Statistics of China, 2010).
Demographic and socioeconomic variables
All demographics are for the population 60 years and older. In 2010, the 60 and older Chinese population were born before 1950, so their childhood and youth were spent during China’s devastating wars before the 1950s, and political upheavals, education disruption, and poverty between 1949 and 1980. By 2010, they were almost all retired, with China’s mandatory retirement age being 60 for men and 55 for women. Many were taking care of grandchildren.
Gender ratio: measuring any differences in the gender ratio of older adults
Existing studies in China show that gender can affect SRH, as older women tend to have poorer SRH than men, even if women live longer (Dong et al., 2016). It may have to do with women’s caretaking roles, which make them more perceptive of health issues than men, and also that men may be more reluctant to admit or discuss illness as masculine norms value independence and physical prowess (Read and Gorman, 2010).
Widowed: measuring the differences among cities in shares of the windowed population
Losing of a spouse is one of the most serious health threats. Krochalk et al. (2008) found that among those aged 60+, widowhood had a negative effect on SRH for over four years. Given that this cohort of Chinese older adults rarely divorce (Weber, 2019), widowhood is the most likely cause of losing spouses.
Illiteracy: measures the percentage of illiterate population 15 years and up
Education level affects how people access, absorb, and assess information for health (Spuling et al., 2017). We use illiteracy to reflect the education level of the urban population, as illiteracy would severely inhibit accessing and applying basic health information. While the measurement is not exclusive to older adults, it is reasonable to expect that older adults are the main body of the illiterate population in cities (Table 3 notes)
GDP/Per capita (log): measuring the city’s economic development level
Economic prosperity raises standards of living, which brings better nutrition, sanitation, housing, and urban and health services, even as it may also introduce pollution and a less active lifestyle.
Living space/per capita (log): measuring the average housing space among the cities
It is calculated by the total square meters of housing in the city divided by the population of urban statistical areas. More spacious accommodation improves the SRH of residents (Gibson et al., 2011). Crowded cities may lead to decreasing privacy and mental “overload” (Fuller-Thomson et al., 2000), thus negatively affecting SRH%.
Doctors per 1,000 persons (log): indicating the medical provisioning in a city
Research in the West and in China has found that the availability of healthcare professionals could increase the early diagnosis of serious diseases such as cancer (McLafferty and Wang, 2009) and increase life expectancy (Luo et al., 2016). We used the number of doctors rather than the number of hospitals or clinics to indicate the healthcare provision because of the great variations in capacities among such hospitals and clinics. Large hospitals rather than clinics are the most common place for the Chinese to seek care.
Environmental variables
We selected two common environmental factors that are known to affect the health status of urban residents.
Exposure to PM2
5(log) 5: measuring days of exposure to the dangerous air pollution level in a city.
Environmental pollution is the leading health challenge for Chinese cities (Fan et al., 2022; Ju et al., 2022; Yang et al., 2018; Yao et al., 2022). PM2.5 is particularly dangerous because it is small enough to penetrate deeply into the lungs. We use the data collected by Long’s et al. (2014a) team on the number of days that the level of PM2.5 in a city exceeded the national daily standard of 75 μg/m3 within a 24-hour period.
Green space: measuring green space coverage in cities
Studies from China and elsewhere have recognized the critical role of green space for the mental and physical health of urban residents (Liu et al., 2017; Xie et al., 2019), especially for older adults to relax, socialize, and exercise (Ji et al., 2019; Zhou et al., 2020, 2022; Zhu et al., 2020). The coverage of green spaces in a city is calculated as the percentage of total green coverage (by ground projection) in the built-up area.
Analysis and results: National and regional level
Before conducting the regression, the variance inflation factors (VIF) test was carried out to detect multicollinearity. The result is presented in Table 3, which shows that all the variables have VIF values less than 10, indicating that the independent variables in the model are not highly correlated to each other.
Table 4 summarizes the descriptive statistics of SRH% and UCI at the national level and by regions and ANOVA test results of different groups. It shows that over 91% of self-care older adults rated their health as good or fair. ANOVA test results indicated that there are statistically significant differences among regions of SRH% and UCI (p < 0.001). SRH% and UCI are the highest in the most developed Eastern Region, followed by the Central Region and the Western Region.
Descriptive statistics and ANOVA test among different groups of SRH% and Compactness (UCI) in the models.
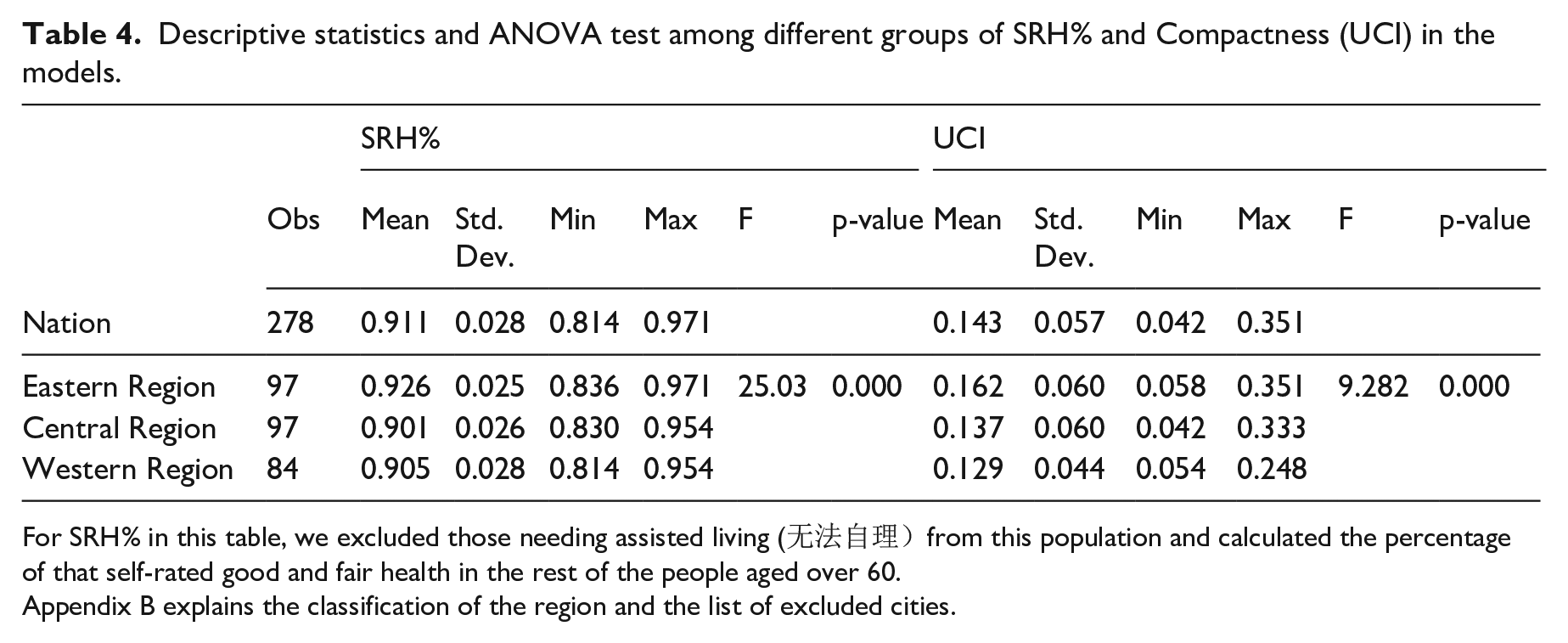
For SRH% in this table, we excluded those needing assisted living (无法自理)from this population and calculated the percentage of that self-rated good and fair health in the rest of the people aged over 60.
Appendix B explains the classification of the region and the list of excluded cities.
Table 5 presents the ordinary least squares (OLS) estimation for the multiple regression model of the 278 cities. The models (1, 3, 5, 7) are based on the subsample of self-care older adults, and models (2, 4, 6, 8) are based on the full sample, including those who need assisted living. The results of the two samples are largely consistent, except that green space is no longer significant in models 2 and 6, even if it is significant in models 1 and 5. Given the overwhelming consensus globally and in China on the role of green space in promoting the health of older adults, we believe that the culprit for the contradictory findings between the two models is the inclusion of the population needing assisted living. There is no reason to believe that green space would not be a significant factor for SRH nationally or in any of the regions. We thus believe our subsample estimation captures more accurately the interactions between the older adults and the built environment, even at the possible risk of losing certain population representativeness. Our analysis will thus focus on models 1, 3, 5, and 7. Since the two sets of models are largely consistent except for the green space variable, we will not discuss models 2, 4, 6, and 8 to avoid redundancy.
Regression estimates of the nation and regions.
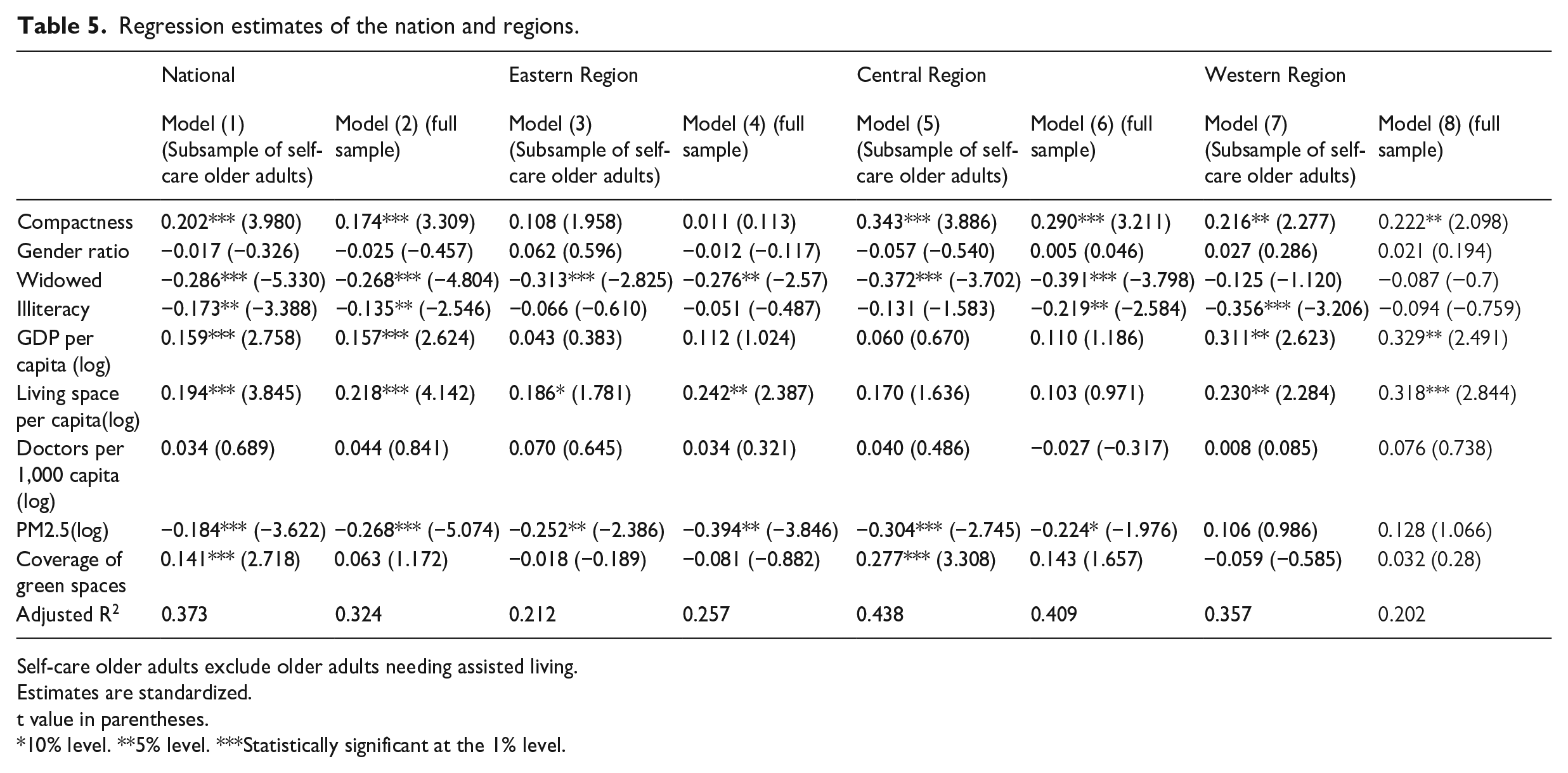
Self-care older adults exclude older adults needing assisted living.
Estimates are standardized.
t value in parentheses.
10% level. **5% level. ***Statistically significant at the 1% level.
National level
The results show that UCI, percentage of widowed, illiteracy rate, GDP per capita (log), per capita living space (log), number of doctors/1000 persons (log), exposures of PM2.5 (log), and coverage of green spaces are all significant at 1% level or lower for SRH%. In other words, cities may have a higher proportion of older adults feeling healthy if the cities were more compact, wealthier, provided more spacious accommodation, had less exposure to pollution, had more green space coverage, and also less portion of older adults in the city are widowed and illiterate. The UCI is significant at below the 0.001 level (p = 0.000), indicating a robust positive association between compact cities and the health of older adults.
The gender ratio is not significant in SRH%. One possible explanation is that the gender discrepancies in SRH disappear for those 85 and up (Carmel and Bernstein, 2003), which leads to mixed results when considering all older adult age groups. The model also fails to show a significant relationship between the number of doctors and SRH%. While the existing research shows prevision of doctors affects the treatment of illness, more doctors do not necessarily help SRH.
Regional level
We run our model separately for cities of Eastern, Central, and Western Regions with declining levels of economic development. Table 4 shows that UCI and SRH% decline from the Eastern to the Western Region, correlating to the economic development levels. Interestingly, our model of each region reveals major differences in contributing factors in the variation of SRH%. Results of the model (5) and model (7) based on self-care older adults in Table 5 show that UCIs are significantly positively correlated with SRH% in the Central Region (p = 0.000) and in the Western Region (p = 0.026), with the coefficients of 0.343 in the Central Region and 0.216 in Western Region, both higher than the national model (0.202), suggesting compactness in the Central and Western regions is associated with more benefits in SRH% than the national average. UCI in the model (3) is not significant among cities in the Eastern Region. Since the Eastern Region already has the highest UCI, our results further confirm that the relationship between UCI and SRH% is not linear, and even higher compactness in Eastern Region would not reward higher SRH of older adults. As in the case nationally, the statistical associations between UCI and SRH% in the full sample-based regional models (models 4, 6, and 8) are largely consistent with the self-care older adults-based model with the exception of the green space in the Central Region, discussed earlier (Table 5).
Other controlling variables show differential impacts across the regions. For example, widowed is the most significant variable in the Eastern Region and Central Region, so spousal support is a crucial factor for the SRH% of older adults. Cities in these two regions are more developed and have a higher prevalence of small families. Many older adults are empty nesters with young people seeking better opportunities outside their hometowns and even abroad. Small family sizes make losing a spouse particularly devastating for the SRH of older adults. The same variable is not significant in the Western Region cities which suggests that in China’s least developed region, either a larger number of children and/or extended families are still more prevalent and can offset the effects of the loss of a spouse. GDP per capita and literacy rate are significant variables only in the Western Region, reflecting the poor socioeconomic development in this region has adverse relationship with the health of older adults although the gap in GDP between the Eastern and Central regions does not matter. Living space per capita is significant in the Eastern Region as these are China’s most crowded cities with the highest housing prices, so living space negatively relate to SRH. It is also significant in the Western Region even though population density is the lowest. This may be explained by the fact that Western Region has many old and less developed cities where small and old homes continue to be common. In contrast, housing is relatively plentiful in cities in the Central Region, which have been undergoing a housing boom since the 2000s, so the variable does not have a significant impact on SRH. PM2.5 has a significant impact on SRH% in the Eastern and Central regions, but not in the less industrialized Western Regions. This variable registers the highest coefficient and significant level in the Central Region. Since 2000, the Central Region is undergoing accelerated industrialization and often receives the relocated pollution industry from the Eastern Region. Pollution is rather a salient factor for SRH%. We also want to note that the coefficients of PM2.5 are substantially higher in the full sample models, suggesting that PM2.5 may be associated with heavier SRH loss with the population needing assisted living, possibly because this population is older than the rest sample. Coverage of green space is highly significant only in the Central Region, even though it is significant in the national model. Urban amenity development in the Central Region lags behind the Eastern Region and its population density is higher than the Western Region, so it is especially an important factor for SRH%. Two variables not showing significance at the national level (gender ratio and the number of doctors/1000 persons) still do not register significance in the regional subgroups.
Discussion
While studies in the Chinese general urban population have not found a clear positive link between health and urban compactness due to pollution and overcrowding, our research offers strong evidence that compact cities are associated with health benefits of older adult residents. The level of association is robust at the national level but more prominent in Central and Western regions. This finding thus substantiates the research conclusions globally and in China that compact urban environments can support the healthy aging of older adults. To a higher degree than residents in North America and Europe, Chinese older adults heavily depended on walking and public transit for mobility in their entire life. They also have strong attachments to their immediate neighborhoods (Chen et al., 2022; Ko and Yeung, 2018; Li et al., 2022; Liu et al., 2021; Wu et al., 2019). Compact urban design with its short blocks, mixed land use, and dense transit services allow older adults to engage in more variety of activities more efficiently, such as shopping, picking up grandchildren, exercising, visiting doctors, socializing, and recreation in urban parks. More socializing opportunities have been shown to improve older adults’ mental health (Xiao et al., 2020). Declining urban compactness would limit the range and activities they can participate independently as it requires further distance to travel, less frequent or more extended bus services, and fewer opportunities for routine social interactions. Without alternatives of easily accessible and affordable transportation arrangements, lower UCI in Chinese cities could lead older adults to be less independent, suffering more confinement at home, and even social isolation. Given how Chinese urban compactness has been declining and the large size of Chinese urban older adults living in these cities, we believe great attention needs to be paid to this association.
We acknowledge that this research has limitations. First, we rely on the SRH as the health indicator, which can be affected by people’s biased perception of their health. If national data are available, it would be valuable to examine the relationship between health indicators such as the share of the population with obesity, hypertension, and diabetes and study these associations with urban compactness. While such “objective” indicators also have limitations in reflecting the overall physical and mental health of the population, they could complement SRH-based studies. Second, additional longitudinal research to examine the dynamic link between Chines urban compactness and SRH would be desirable to move beyond our cross-sectional study. It may help to establish whether Chinese SRH has indeed declined with compactness. Third, China’s regional variation goes far beyond the three zones in our study. More fine-grain geographical analyses on regions and different classifications of cities can identify other dimensions of how the urban built environment can affect the health of older adults.
Policy implications
Our finding raises significant concerns that the rapidly changing urban forms may leave large vulnerable populations falling through the cracks. In many Chinese and also other Asian cities, it is the younger middle class driving the urban policies, and their preferences for bigger homes, private automobiles, and auto-oriented infrastructure often define urban planning priorities. In China, additional powerful political and economic forces, such as the urban land finance regime, favor lower-density development. Older adults, though traditionally respected in Chinese culture, have little opportunity to contribute to public discussion of urban design directly, and their heavy reliance on compact cities’ built environment is often neglected or unacknowledged in urban policymaking.
As compactness declines in most Chinese cities through lower residential density, more single-purpose land use, less walking-friendly streets, and less transit coverage, older adults are experiencing more inconvenience, less capacity to be independent, and less socializing and recreational opportunities. Such trends contradict the call of WHO to design the built environment to enhance the functional ability of older adults. As a result, the whole society may pay a heavy price for the declining SRH of older adults because they would require more time and emotional and financial support from family members or the society at large to provide routine services to maintain their health status.
The Chinese government is increasingly committed to promoting sustainable and healthy cities, but the concerns of energy and land savings dominate the discussion on compact cities by far, and those discussions on health are primarily about providing more health services, exercise spaces, and caring facilities. Our work makes it clear that Chinese compact cities have long served the supportive roles of promoting the physical and mental health of older adults and prolonging their independence, for which building more older adults’ homes is a far inferior/expensive substitute. In addition to compactness, our research shows that China should adopt different regional strategies to increase SRH%. In the Eastern Region, cities must provide more social support for the widowed, reduce pollution, and improve housing. In the Central Region, cities need to address family support, reduce pollution, and increase urban amenities such as green space. The Western Region primarily needs more socioeconomic development and to reduce illiteracy, as well as improve housing in old neighborhoods. Overall, this study aims to highlight the synergy of urban compactness, sustainability, and older adults’ health. We hope our findings can help policymakers to revalue, preserve, and promote more compact urban designs in China. We also call for more research on such issues in China and other cities of the Global South, as many such cities are facing or will face similar challenges or urban changes and aging populations.
Footnotes
Appendix A
where
where
Appendix B
Acknowledgements
We thank the editor and anonymous reviewers for their comments and suggestions and Kathryn Kraynik for her editorial assistance.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: We would like to acknowledge China Scholarship Council for supporting Feixiang Sun exchange at Vassar College (No.201908110305).
Notes
Author biographies
Feixiang Sun is postdoctoral researcher in the Data Center, National Academy of Innovation Strategy, China. His research interests include urban and regional innovation, high-tech industry, and urban planning in China.
Yu Zhou is a professor of geography at Vassar college. Her research has been on China’s technological development, and urban sustainability.