
Abstract
The Pathfinder Service is a collaboration between the Irish National Ambulance Service and Beaumont Hospital, Ireland. It was implemented in 2020 as an alternative to the traditional ambulance response model. An Advanced Paramedic and an Occupational Therapist or Physiotherapist respond to Emergency Medical Services (EMS) calls. The Pathfinder team may treat patients at home or transport them to hospital. Follow-up care is also provided. The aim of this study was to conduct a micro-costing analysis from a health service perspective to assess the difference in EMS costs when provided by Pathfinder compared with the traditional ambulance response.
The Pathfinder cohort was identified from Pathfinder records. A comparable cohort was identified who met Pathfinder inclusion criteria but had emergency department ambulance conveyance. Both cohorts were contacted by telephone, and consenting individuals were interviewed about their contacts with healthcare providers. The analysis compared the cohorts in terms of age, sex and frailty score, the proportion of individuals who used various services, and the volume and cost of services. The seven-day costs were accumulated into major cost groups and total cost, and the difference in mean costs were reported at 2023-€ price level. Patient satisfaction was also recorded.
Data were obtained from 108 patients with Pathfinder dispatch and 89 with traditional ambulance dispatch. The mean cost of the Pathfinder service was €3315 while the mean costs of the traditional ambulance model was €5482. The mean cost difference (€2,167, p < .001) indicates that Pathfinder is cheaper than the traditional ambulance model. Ninety-eight percent of participants were very satisfied or more than satisfied with Pathfinder in comparison with 85% in the traditional ambulance response group.
These results suggest Pathfinder is a service that achieves high patient satisfaction at a lower cost than the traditional ambulance response model.
Introduction
The increasing number of Emergency Medical Services (EMS) calls in Ireland 1 and internationally 2 has challenged Paramedic services, and healthcare systems generally, to innovate in service delivery. Over 46% of EMS calls in Ireland are for people aged 65 and older. 3 This will increase as Ireland has the fastest aging population in Europe, with the number of people aged over 65 projected to double to 1.8 million by 2057 and the number aged over 85 projected to increase by 274% to 389,000.4,5 International evidence asserts that 13–40% of emergency department (ED) attendances may be inappropriate, 6 with the majority of EMS calls being non-emergency calls. 7 A risk of adverse events for older people associated with ED length of stay, including delirium, pressure injuries, functional decline, increased risk of mortality,6,8–11 has led to EMS and hospitals seeking ways to safely treat more people at home rather than conveying them to ED. In Ireland recent National Ambulance Service (NAS) innovations include community paramedicine services, the development of a ‘clinical hub’ in the National Emergency Operations Centre (NEOC), an ED registrar and emergency medicine technician attending low acuity EMS calls 12 and specialist older person services like Pathfinder. 13
Pathfinder is a collaborative project between the Irish Health Service Executive NAS and Beaumont Hospital Occupational Therapy (OT) and Physiotherapy (PT) Departments. In the hospital catchment area statutory ambulance services are provided by the NAS and Dublin Fire Brigade (DFB). In Ireland, when a patient is attended by either ambulance service, following assessment and treatment, the patient will be conveyed to the ED unless they refuse transport. Pathfinder offers an alternative to this traditional ambulance model.
The model has been previously described and evaluated to be a safe alternative to the traditional EMS response.13–15 A thematic analysis of patient feedback from 573 older people and their next-of-kin, who received the Pathfinder service, found that people strongly valued the opportunity to be treated by the service, rather than being transported to the ED. 16 The primary themes identified included the professionalism of the multidisciplinary team, the role of Pathfinder in connecting people with hospital and community services and the lasting effect of the experience on the patient.
Internationally alternative care pathways (ACP) to ED presentation for EMS callers have been developed and are believed to reduce ED conveyance rates and costs across the emergency care sector. 17 Community Paramedic programmes have demonstrated positive outcomes.18,19 Other ACP models include teams with paramedics and OT and/or PT,20–22 nurses working with general practitioners 23 or paramedics 24 and ED doctors working alongside emergency medical technicians. 25 Internationally there is no consensus on which ACP model is preferable 17 and a systematic review concluded more research was needed on the impact of alternative care options. 26 The development of alternative options to the ED for unscheduled care is a policy aim in Ireland.27–29 Research in this field has been identified as a priority by the European Research Agenda for Geriatric Emergency Medicine. 30
There has been limited research into the cost effectiveness of ACP models. A 2009 U.K. study 31 compared the cost effectiveness of an extended skills paramedic practitioner in comparison with usual emergency care. The intervention group cost £140 less per patient. A 2014 Australian study found extended care paramedics can be cost effective if sufficient throughput of appropriate patients is initiated by control room staff. 32 Another U.K. study in which a nurse attended EMS calls alongside a paramedic was also found to be cost effective. 24 A 2024 systematic review of economic evaluations of community paramedicine found that Dixon et al. 31 was the only paper that provided a full economic evaluation. 33 The authors suggested that the impact of this study may be underreported and noted that, as the data set is 20 years old, advancements in paramedic training could yield a greater impact. This review recommended further research into the cost effectiveness of these services. 33
The aim of this study was to conduct a micro-costing analysis to assess the difference in mean costs of EMS provided by Pathfinder in comparison with usual emergency care in Ireland.
Methods
Setting
Pathfinder is dispatched by the NEOC and responds to EMS calls that are deemed to be low acuity (not immediately life-threatening or time sensitive) for people aged 65 years or older. The NEOC identifies calls for Pathfinder through several methods: using agreed Advanced Medical Priority Dispatch System (AMPDS) codes, 34 by filtering low acuity calls at its Clinical Hub desk, or indirectly via on-scene crew referral (any AMPDS code deemed suitable for Pathfinder by on-scene crew). Pathfinder operates two teams: the ‘Rapid Response Team’ (an Advanced Paramedic (AP) and an OT or a PT (operating Monday to Friday 08:00–20:00) and a ‘Follow-Up Team’ (an OT and a PT). Pathfinder has been operational in the Beaumont Hospital catchment area since May 2020. In 2023, the Pathfinder team responded to 611 calls. Where deemed safe, Pathfinder treats EMS callers at home rather than transporting them to the ED. A description of the interventions provided and the background of the staff is provided in the supplemental material.
Study design
The design of this cost analysis was a service review of a prospective cohort of consecutive patients attended by Pathfinder. A similar cohort of patients who fulfilled the criteria to receive the Pathfinder service, but who instead received traditional EMS care and were conveyed to the Beaumont Hospital ED were identified as a comparison group. In Ireland all EMS calls have traditionally been transported to ED, unless the patient declines transport to ED. For example, in a review of NAS patients who were attended by an emergency ambulance from December 2019 to February 2020, over 96% were transported to a hospital facility. 35
Data on the two cohorts were obtained from NAS, DFB, the Pathfinder team, and the ED using a bottom-up approach. In addition, approximately seven days after the initial call, data collectors contacted patients by phone and asked them to respond to a series of questions related to their use of healthcare resources since the initial emergency call and their satisfaction with the EMS response. Costs were calculated within seven days after the EMS call as Pathfinder and Beaumont Hospital ED routinely collate seven-day outcomes for patients they have cared for. Furthermore it has been suggested seven-day outcomes are more appropriate as a measure of effective care than a longer 30 day period. 36
The analysis compared the measures of resource use and costs for the two cohorts to describe the cost difference and variation in resource use. Our expectation was that the Pathfinder cohort would use fewer resources and be associated with fewer costs than the usual EMS response cohort.
Participants
Patients who received the Pathfinder service were the main study group. Data were collected about the date and time of the emergency call, and decisions made on-site by the team and referrals completed. A comparison group of similar patients to whom an emergency ambulance was dispatched to convey the patient to Beaumont ED was identified to match the Pathfinder group in terms of sex, age, geographical area, time of call (i.e. the patient attended on a day or time when Pathfinder was operational) and AMPDS triage category. 34 Pathfinder could not respond to the comparison cohort of calls as they were tasked to another call at the time.
Patients who had already been assessed by a GP or Specialist Medical Team and where hospital attendance was required, or nursing home residents outside of urinary catheter issues were excluded from the comparison group as they do not meet the inclusion criteria for Pathfinder.
The Pathfinder team requested patient permission for a health care professional data collector from Beaumont Hospital to make a telephone call to request verbal consent to take part in the interview. An information leaflet was left with the patient where appropriate (Appendix 2 in the Supplemental Material). To identify potential patients for the comparison group, the data collectors used the Beaumont ED IT-system to screen for patients who met the criteria for Pathfinder.
Data collection
Data were collected for patients to whom Pathfinder was dispatched and to whom a traditional ambulance response was dispatched during May to October 2023 (Figure 1). An electronic data-capturing tool was developed using the SmartSurvey system (Appendix 1 and 2 in the Supplementary Material). The development of the tool included a series of discussions between members of the study group supplemented with information provided by other service providers (in particular regarding laboratory and imaging services) and subsequent adjustments and editing. The pilot testing included several rounds to secure a valid and consistent data collection process.
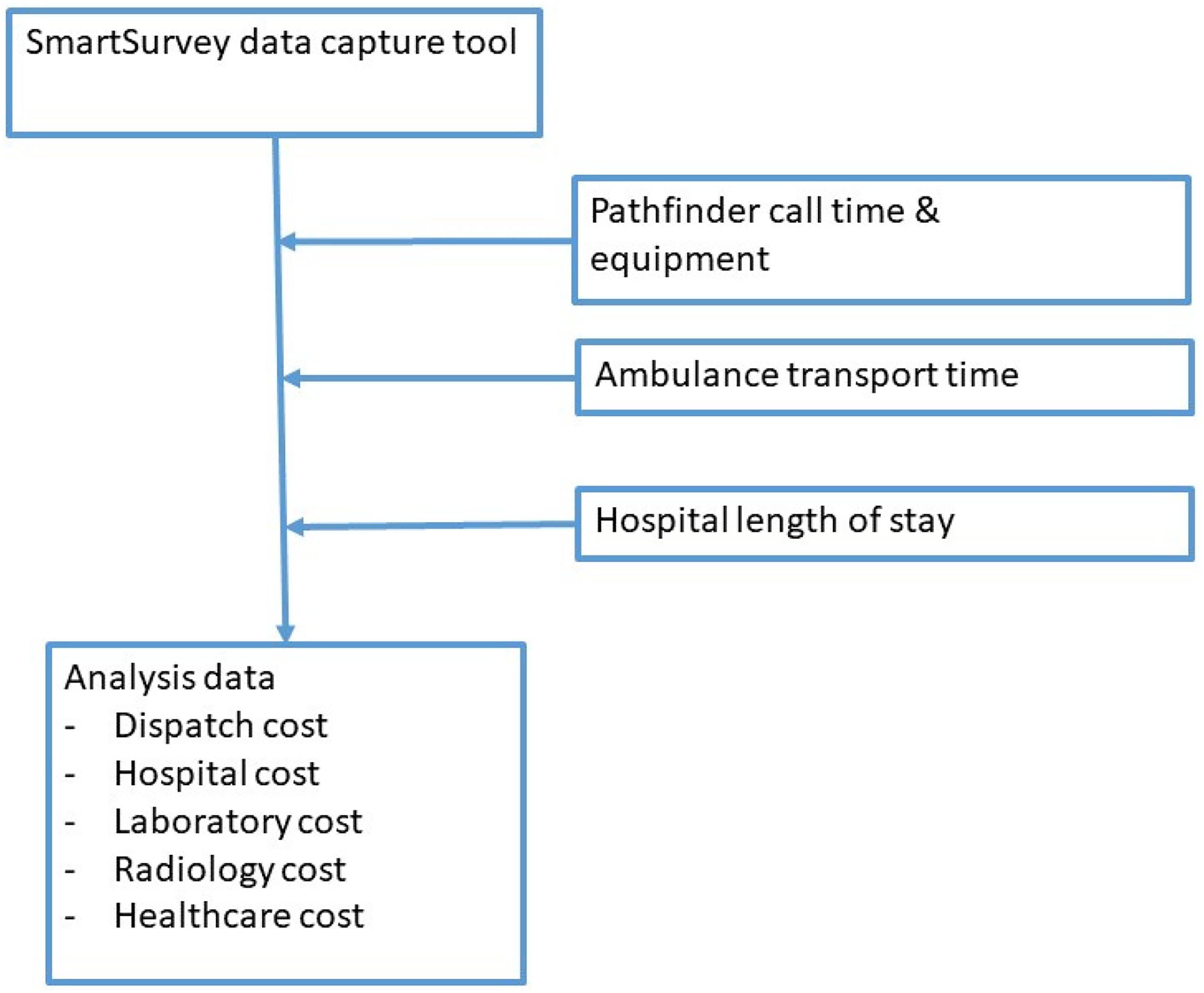
Sources of data material.
The tool captured information about individual patients (age and sex, Rockwood clinical frailty score, 37 dispatch code), date and time for the initial call, medical records from the Pathfinder team (outcome, call interval, repeat calls, provided equipment), medical records from the hospital (admission as inpatient, laboratory and radiology services provided), services provided within seven days after the initial call (ED contacts, hospital outpatient contacts, hospital admissions), patient consent to take part in interview (outcome after initial call, repeat visits by Pathfinder team, repeat EMS calls), use of other healthcare services within seven days after the initial call (number and duration of 20 different services), and patient satisfaction with the response received after the EMS call.
The Pathfinder total call interval was recorded as the duration from dispatch to ready for next assignment. If the patient had additional follow-up interventions with the Pathfinder crew, the number of contacts and total follow-up intervention time were recorded. The following data was collected from Pathfinder and ambulance service records: patient age, outcome following initial contact, whether the Pathfinder team provided support following discharge after ED presentation, and whether the Pathfinder team made referrals to other healthcare providers. This data set also included information on whether different types of equipment were provided to patients as part of the Pathfinder response. The ambulance transport interval was obtained for the ambulance and Pathfinder patients who were conveyed to Beaumont ED. The transport interval was missing for ten pathfinder patients and missing values were replaced with the mean transport interval for ED patients with a valid transport interval.
Validation and adjustment to data
During initial analysis, it was identified that 11 patients in the comparison group were nursing home residents. As nursing home residents are not in the primary target group for the Pathfinder service, the records for these patients were excluded from the analysis. Length of stay data was coded incorrectly for some of the admitted patients. An additional data collection was conducted to obtain comparable measures of length of stay for all hospitalised participants in the study.
Unit costs
Unit costs were developed for each included resource item at 2023-€ price level. The development of unit cost complied with the guidelines issued by the Health Information Quality Authority (HIQA). 38
Table 1 shows the calculation of unit costs of the initial Pathfinder visit and the traditional ambulance response. The unit cost was calculated as a cost per dispatch and a cost per hour. The total cost consists of vehicle and special equipment required, staff costs, and consumables. Most of the costs were considered as fixed costs, i.e. independent of the number of dispatches. The costs related to fuel and clinical consumables are variable costs and depend on the number of dispatches. The cost of the Pathfinder vehicle including special equipment was assumed at €110,000 while the cost of an ambulance was assumed at €220,000. The vehicles were assumed depreciated over five years, while the special equipment was depreciated over three years. The equivalent annual cost was estimated assuming a discount rate of 4% per year.
Assumptions and calculation of unit cost for pathfinder and ambulance dispatches.
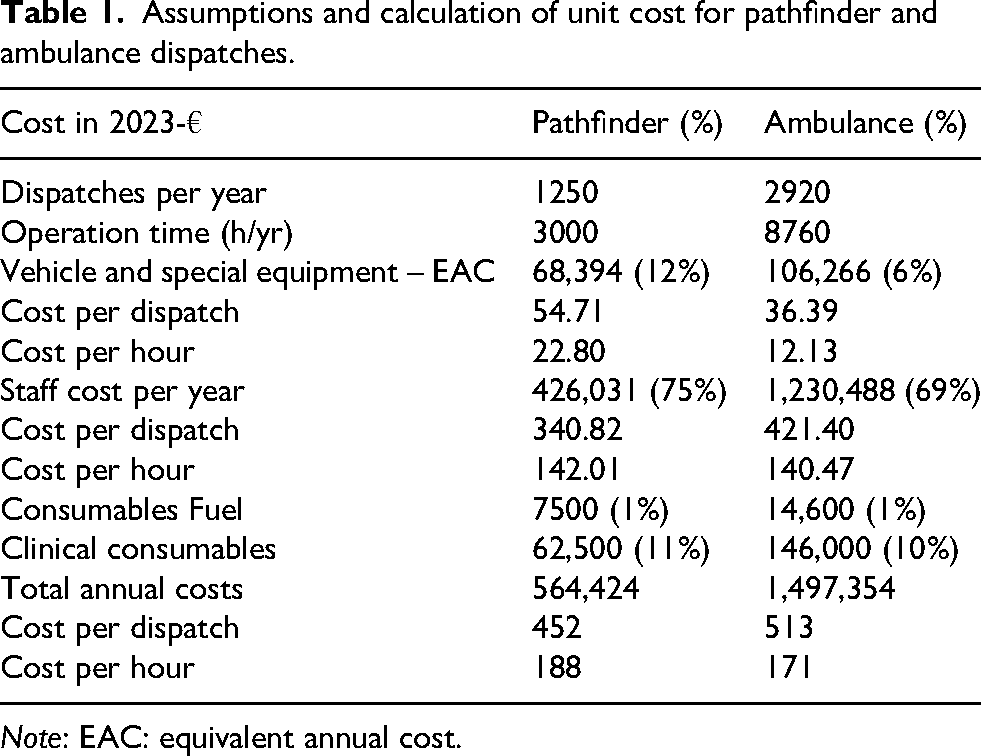
Note: EAC: equivalent annual cost.
The staff cost was assumed as the mid-range full-time gross pay for an Advanced Paramedic, a Paramedic and a Therapist working at Senior or Clinical Specialist grade. The annual working hours were assumed to be 1755 h, of which 77.5% were directly related to the services provided. Consumables included fuel and clinical consumables and was based on expert assessment that the fuel consumption of Pathfinder and the Ambulance was 10 and 12 litres per 100 km. The unit cost of clinical consumables per dispatch was assumed similar for the Pathfinder and traditional Ambulance (€50). With these assumptions, the cost model estimated the annual total costs at €564,424 for the Pathfinder and €1,497,354 for the traditional ambulance. Staff costs accounted for 75% and 82% of the total annual cost. The vehicle and special equipment cost accounted for 12% and 7%, which reflects that the operation time is assumed to be different for the two vehicles. The Pathfinder vehicle was assumed to be in use 250 days per year at 12 h per day, from 08:00 to 20:00 h daily (3000 h per year) or five dispatches per day (1250 dispatches per year). The ambulance vehicle was assumed to be in use 365 days per year at 24 h per day (8760 h per year) or eight dispatches per day (2920 dispatches per year). With these assumptions, the hourly cost for Pathfinder was €188 per service hour versus €171 per service hour for the traditional ambulance. The hourly cost is relatively similar, although this relates to the assumption of 12 h daily service time five days a week for the Pathfinder and 24 h daily service time seven days a week for the traditional ambulance. The cost per dispatch for Pathfinder was €452 versus €513 for the traditional ambulance. If mean daily dispatches was changed from five to three times per day for Pathfinder (750 dispatches per year) and from eight to five times per day for the traditional ambulance (1825 dispatches per year), the mean dispatch cost for Pathfinder was estimated at €715 and €878 for the traditional ambulance. The unit cost of Pathfinder follow-up interventions assumed that the intervention was provided by one therapist.
The unit cost of the equipment provided by the Pathfinder team is presented in Supplemental Table S1.
The use of radiology services was identified in collaboration with staff from the Beaumont Radiology Department as shown in Supplemental Table S2. The six types of services included standard X-ray, CT scan with and without contrast, MRI scan with and without contrast and ultrasound scan. Staff from the Radiology department made an expert assessment of the type of staff and the mean time required for each service. Five different staff categories were identified, and their annual full-time salary was obtained and converted to hourly costs assuming 1755 annual work hours and 78% of the worktime allocated to patient services. Guidelines for economic evaluation of health technologies in Ireland issued by the HIQA recommend that 40% overhead is added to the staff costs. 38 In addition to staff cost, expert assessment was obtained for the consumables and equipment related to each service. The consumables related to specific tests while the equipment cost was calculated based on the purchase cost, 10-year depreciation and the annual number of services provided by the equipment.
The unit costs for other healthcare services were mainly based on expert assessment. Some resources, e.g. GP services, hospital bed days, ED and outpatient visits have a cost determined by the Health Care Pricing Office (€920 per hospital night). 39 The unit cost for the majority of services was determined based on the staff salary, the mean time of patient contact and if relevant, additional staff time, e.g. planning and documentation, cost of transport and facilities. Hourly staff costs were calculated using the HIQA model using the mid-range salary for the main service provider. 38 The contact time and additional time are assumed to be the time used for an average patient contact.
Analysis
Descriptive analysis of both patient cohorts was performed. Standard statistical tests (chi-squared or t-tests) were used to identify statistically significant differences. The reported use of healthcare resources was analysed for individual patients in the two cohorts. The real resource use has been presented in full detail in Appendix 4 in the Supplemental Material to provide a full picture of the collected data material. By multiplying the real resource use with the defined unit price and accumulating the costs for the two cohorts, the mean costs per patient were presented. In addition, the proportion of patients who used the service and the mean use of services for the users was calculated. The mean cost is presented for all the patients included in the two cohorts.
This service evaluation was registered with Beaumont Hospital Quality and Safety Department. Data used were part of the patient record and part of routine data recording. This data is used to improve service quality. It is the policy of the Beaumont Hospital Ethics (Medical Research) Committee that service evaluations notified to the Beaumont Hospital Quality and Safety Department do not require research ethics committee approval.
Results
During the data-capturing period from 30th March 2023 until 12th October 2023, 208 participants were included. Eleven patients from the comparison group were excluded as they did not meet the criteria for Pathfinder referral. The characteristics of participants are shown in Table 2.
Characteristics of participants.
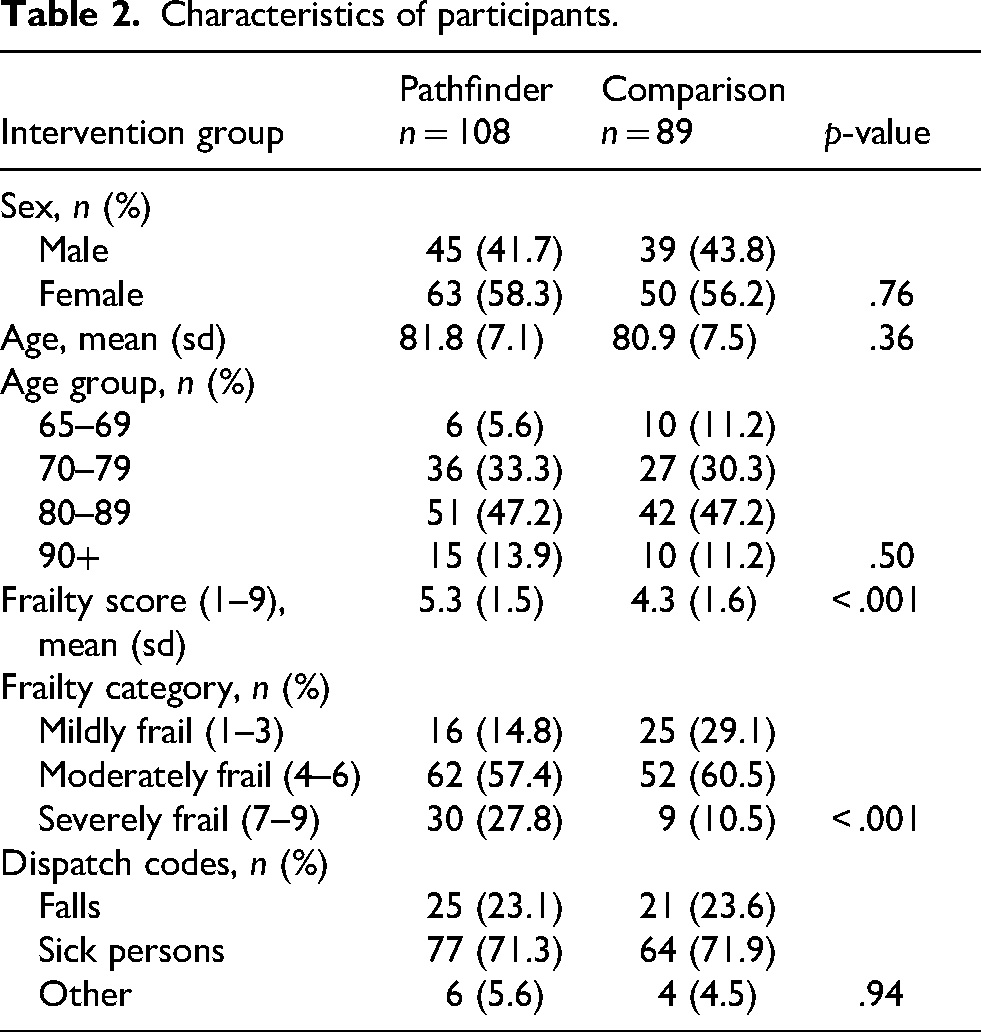
We attempted to recruit 240 participants and recruited 197 participants (response rate, 82%). The cohorts were well-matched for age (mean: 81.8 vs 80.9 years, p = .36) and sex (58% vs 56% female, p = .76). However, Pathfinder patients had significantly higher Frailty Scores (mean: 5.3 vs 4.3, p < .001), suggesting greater overall vulnerability in this group. There was no statistically significant difference in the type of dispatch codes between the two groups (p = .943). Twenty-three percent of the calls related to falls, 72% to sick persons and 5% to other reasons.
Prehospital care costs
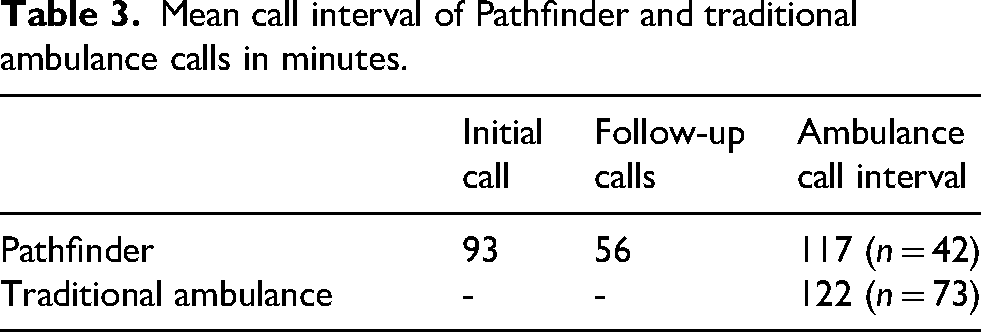
Of the 108 Pathfinder dispatches, 45 (42%) resulted in conveyance to the ED. The remaining patients were either discharged after treatment (26 (24%)) or were referred to other health care providers for treatment at home (37 (34%)). The mean call interval for the 108 initial Pathfinder dispatches was 93 min (SD 40, median 89, min 7, max 251) as shown in Table 3. During the seven days after the initial EMS call, the mean number of follow-up interventions was 2.6 (SD 2.6, median 2). The mean duration of the follow-up interventions was 56 min (SD 74, median 50, min 15, max 330). The mean interval duration of the traditional ambulance was 122 min.
Mean call interval of Pathfinder and traditional ambulance calls in minutes.
Costs
Table 4 outlines the mean cost per patient in the Pathfinder and comparison groups. The mean cost of a Pathfinder patient was €3315 and €5482 for the comparison group patient. The mean cost of conveyance with Pathfinder was €199 more costly than the traditional ambulance response. The mean hospital cost was €2166 lower (p = .001), the laboratory cost was €116 lower (p < .001), and the radiology cost €64 lower (p = .003). There was no statistically significant difference in downstream healthcare costs.
Mean cost per patient (€).
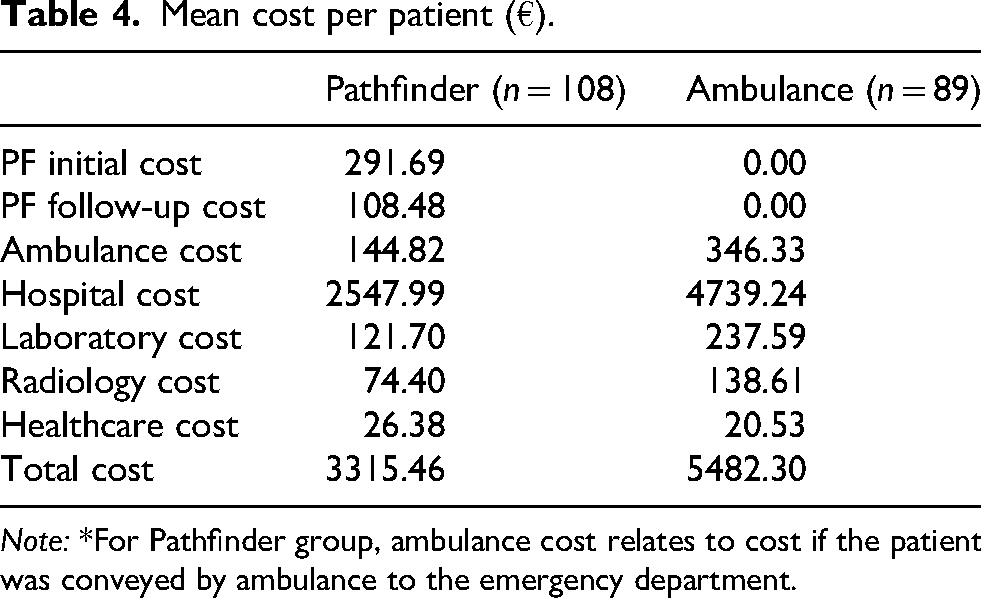
Note: *For Pathfinder group, ambulance cost relates to cost if the patient was conveyed by ambulance to the emergency department.
Patient satisfaction
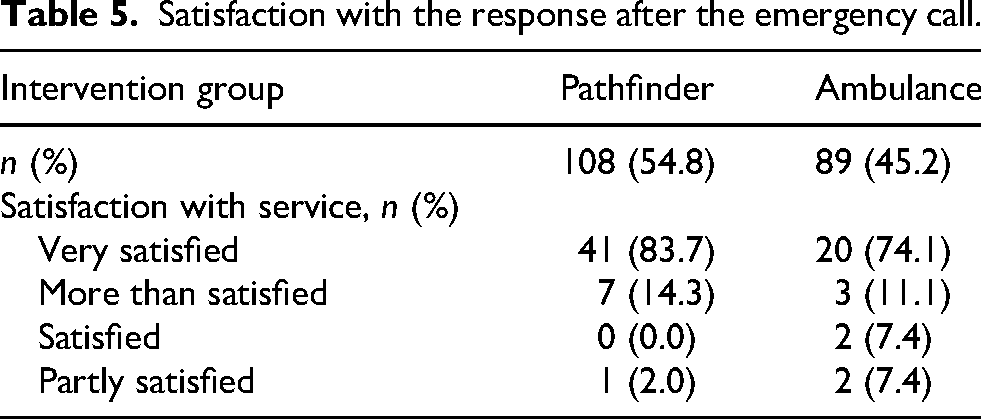
During the telephone interview, participants were asked about their satisfaction with the emergency prehospital service they received. The majority of participants expressed satisfaction with both types of services (Table 5). More participants were very satisfied or more than satisfied with the Pathfinder service in comparison with the traditional ambulance response.
Satisfaction with the response after the emergency call.
Discussion
Based on these results, the Pathfinder model appears to provide a service with which patients were more satisfied, at a lower cost, compared with those who received a traditional ambulance response. This analysis confirms findings from previous evaluations of the Pathfinder model, demonstrating that the service is attractive from several perspectives. This is the first analysis to assess the potential cost savings of the model. Using a micro-costing approach, the seven-day cost for Pathfinder patients was €2167 (39.5%) lower than for patients receiving a traditional ambulance response.
Our finding of lower costs associated with the Pathfinder model is consistent with previous research, with savings attributable to reduced ED attendances, reduced hospital admission and reduced length of stays.31–33 Health systems with high transfer to ED for EMS calls are likely to experience cost savings from developing services like Pathfinder. 31 In Ireland until recently all patients were transported to hospital unless they declined to attend the ED. 27 This may partly explain the significant savings demonstrated in this study.
Other research has reported even greater cost savings. A Canadian team that included an OT in one of its five ACP vehicles reported a 60% saving compared with regular EMS care. 40 Xie et al. 40 costed scene time, capital costs and ED visits and suggested that if healthcare costs beyond the day of the EMS call had been included, the savings might have been even greater.
A major strength of this micro-costing analysis is the detailed account of services provided to individual patients. The use of a phone survey, in addition to screening hospital medical records, ensured comprehensive data collection for patients who did and did not attend hospital. The analysis considered a wide range of health care resources during the seven-day period following the initial EMS call. Another strength of this study is the inclusion of downstream healthcare costs, ensuring that subsequent outcomes associated with the initial decision to treat a patient at home, or transport them to ED, were accounted for. As many investigations in Ireland ordered in community settings are processed in hospitals, the data collectors could obtain this data for people who did not attend the ED also. Another study 28 cited the lack of measurement of costs beyond the initial EMS call as a limitation.
Of the 108 Pathfinder patients, 45 (41.6%) were transported to ED while 63 (58.3%) remained at home. This is consistent with previously published research. 13 Fewer than half of the patients who stayed at home were referred to other healthcare services. Participants were very satisfied or more than satisfied with the Pathfinder service in comparison with the traditional ambulance response, although it should be stated that very few patients were less than satisfied with both services. High patient satisfaction with Pathfinder is also consistent with previous research. 16
The savings from avoiding hospital conveyances are substantial particularly regarding admissions, laboratory tests and radiology diagnostics. Radiology costs were 46% lower for the Pathfinder cohort. Another Irish study has suggested that 40% of radiograph tests may be inappropriate imaging referrals. 41 This may explain why it is possible to manage this cohort of patients with significantly fewer imaging referrals. Use of other non-hospital services was limited, and no significant differences were observed between the two groups of patients.
A major difference in cost per average patient in both cohorts was length of hospital stay. Variation in length of hospital stay costs was further driven by the proportion of admitted patients in the two groups. Only 34% of Pathfinder patients had inpatient days compared to 67% of the traditional ambulance patients. The lower rate of hospital admissions is one of the attractions for the Pathfinder model, and this is clearly reflected in the cost analysis. The overall costs for the average patient, who is dispatched a traditional ambulance response were over 1.6 times more expensive than for the average Pathfinder patient. As demand for EMS services for older people is expected to increase in line with anticipated older person population increases4,5 the need for cost effective services for the State and an ‘age friendly ambulance service’ 3 will also increase.
Limitations
In Ireland, patients attended by an emergency ambulance crew are conveyed to an ED, unless they refuse transport. In other countries, ‘treat-and-discharge’ is a more common option. This more conservative approach may limit the generalisability of our findings. However, one of the primary reasons that the Pathfinder service can ‘treat-and-leave’ patients in the community is their knowledge of and access to onward referral options. Our study demonstrates that, while empowering staff to utilise a ‘treat-and-leave’ approach is more costly for the ambulance service, it is substantially more cost effective for the wider health service.
The costing assumptions applied in this analysis can be challenged. For both services there will be an element of ‘stand-by’ cost, and therefore the full cost may not be allocated to individual patients. Staff cost was estimated using standard guidelines issued by HIQA which are based on annual salaries, assumptions of add-on costs, working hours and proportion of worktime allocated to patient care. The cost model made an explicit assumption of the weekly staffing of the vehicles, and the cost of the vehicle was obtained from local sources. A standard model was then used to estimate the equivalent annual cost, assuming explicit depreciation periods and discount rates. Equivalent annual costs were then divided among the assumed number of conveyances or hours in operation. These costs were used as unit costs for the analysis. All these assumptions have been stated explicitly. Other assumptions may change the mean cost per conveyance or per hour of services.
We are confident that data collection accurately captured seven-day laboratory and imaging investigations for both hospital attending patients and community treated. For patients who remained at home, laboratory work and imaging ordered by GPs would typically have been processed in the hospital and therefore captured by the data collectors. It is possible that a small proportion of patients may have attended private healthcare facilities during the seven-day period and had investigations. These private investigations may not have been fully captured. Collecting costs at a consumer level has been recommended. 22 However, in Ireland, people aged over 70 are entitled to free GP care and therefore private GP use is likely to be low. Nonetheless, it must be acknowledged that for some healthcare utilisation, we have relied on the information provided by patient.
The cost analysis was based on two relatively small samples. Healthcare service costs can vary widely because some patients may use no services while other patients use many. This poses challenges for statistical analysis of mean cost differences. However, by focusing on seven-day costs, we reduced the potential for cost variation. Determining an appropriate follow-up period following an emergency incident is challenging. Seven days was selected because a longer timeframe would be more likely to reflect chronic condition management or unrelated healthcare needs.
As patient recruitment was not randomised, the risk of allocation bias should be mentioned. All emergency calls are triaged using the AMPDS system by non-clinical call takers. The resulting AMPDS code is used to determine which ambulance resource is appropriate, and the resource is allocated by a non-clinical dispatcher. As recommended by recent research guidelines both the intervention and comparison groups consisted of patients from the same AMPDS codes. 33 Call takers and dispatchers work to strict protocols and do not have training or latitude to consider any additional clinical information when dispatching a resource. While the Pathfinder team may refuse calls that they believe are inappropriate, this is an extremely rare occurrence. If the AMPDS code matched and the Pathfinder resource was available in the patient's catchment area, the Pathfinder resource would have been dispatched. Although this does not fully remove the risk of allocation bias, as Pathfinder is essentially dispatched based on an availability rather than a clinical basis, we do not believe there was substantial risk of allocation bias in our study.
Conclusion
The Pathfinder model appears to provide services at a lower cost in comparison with a traditional ambulance response. The magnitude of this difference in overall costs was very substantial with a mean difference of approximately €2167 per patient less per Pathfinder patient in comparison to patients who receive the traditional EMS response. The cost savings are heavily influenced by hospital admissions and associated bed days. Additionally, on average, Pathfinder patients required fewer laboratory and radiology investigations, and their other healthcare costs were similar to patients who were dispatched a traditional ambulance. Participants were very satisfied or more than satisfied with the Pathfinder service. Pathfinder has previously been reported as a safe alternative to ED conveyance for EMS calls and has demonstrated consistently high levels of patient satisfaction. This study now suggests that Pathfinder is also cost saving for the health service.
Supplemental Material
sj-docx-1-pam-10.1177_27536386261417745 - Supplemental material for Cost analysis of the pathfinder service as an alternative to the traditional ambulance response
Supplemental material, sj-docx-1-pam-10.1177_27536386261417745 for Cost analysis of the pathfinder service as an alternative to the traditional ambulance response by Paul Bernard, Siobhan Masterson, Grace Corcoran, Laura Hammond, Laura Hogan, William Howard, Frances Horgan, Lawrence Kenna, Grainne Maher, Louise McGettigan, Grace McKee, Yvonne O’Riordan and Jan Sorensen in Paramedicine
Footnotes
Acknowledgments
The Pathfinder Team would like to acknowledge the excellent organisational support and leadership provided by the joint Beaumont Hospital and NAS Pathfinder Management Forum. The team would also extend special thanks to the DFB for their ongoing close collaboration, as well as and the many other organisations making it possible for the team to deliver this service to older people.
Ethical approval
This service evaluation was registered with Beaumont Hospital Quality and Safety Department. Data used were part of the patient record and part of routine data recording. This data is used to improve service quality. It is the policy of the Beaumont Hospital Ethics (Medical Research) Committee that service evaluations notified to the Beaumont Hospital Quality and Safety Department do not require research ethics committee approval.
Consent to participate
The Pathfinder team requested permission for a healthcare professional data collector from Beaumont Hospital to make a telephone call to the patient to request verbal consent to take part in the interview. An information leaflet was left with the patient where appropriate. At the time of the interview, verbal consent was provided by participants. This was recorded.
Author contribution(s)
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.