
Abstract
Understanding patient experience is associated with quality, safe, and effective healthcare. However, there is a scarcity of knowledge explaining how patients experience non-conveyance, a setting where individuals receive unscheduled ambulance service response and paramedic-led care that results in a decision to not attend a hospital emergency department (ED). This research project aimed to investigate patients’ experiences of non-conveyance within an Australian ambulance service setting. Constructivist Grounded Theory methods were used to generate and analyse data from in-depth, semi-structured interviews with 21 participants who received paramedic-led healthcare from an Australian ambulance service between August 2020 and October 2021 that resulted in non-conveyance. A substantive theory centred on ‘Restoring self-efficacy’ was generated. It comprises three categorical concepts and their interconnected relationships, explaining how patients experience non-conveyance. ‘
Keywords
Introduction
Non-conveyance describes cases where a call to emergency services results in the dispatch of an ambulance and involves paramedic assessment of at least one person who is subsequently not conveyed to a hospital Emergency Department (ED). The non-conveyance decision may be the patient's autonomous choice contrary to paramedic advice, paramedic recommendation, or jointly agreed.1,2 These cases account for a considerable proportion of responses by emergency ambulance services, and healthcare provided by paramedics.
Rates of non-conveyance vary widely across international settings, reported as ranging between 3.7% and 93.7% for general patient populations.1,3 In Australia, 3,914,327 patients were attended by state ambulance services between 2020 and 2021, with 498,973 (12.7%) of those patients not conveyed to the ED. 4 Cases that are not conveyed require paramedic assessment and examination, risk screening, identification of goals of care, development and implementation of care options, and may also require collaboration with and/or referral to community-based health services such as a General Practitioner (GP).5–11
Research investigating non-conveyance typically reports on patient-safety aspects, or the impacts on emergency health service resources, rather than an understanding of the patient experience of healthcare they received.1,12–18 Outcomes of interest often include mortality rates, re-presentation rates to emergency services, or subjective analysis into the ability of paramedics to make appropriate non-conveyance decisions.1,13,14 These are important metrics, yet little is understood about patients’ perception of the healthcare they received, patient-reported-experience or outcomes, or why some patients re-present to emergency health care within a short timeframe.1,13–15,19,20
Both the World Health Organization (WHO), and the Australian Commission on Safety and Quality in Health Care (ACSQHC), recommend that measures of patient experience should be used to guide, report on, and evaluate quality improvement initiatives in healthcare.21–24 International research, including systematic reviews and a meta-analysis, recommend that patient experience of non-conveyance requires additional investigation.1,14,15,25 Evaluating the patient experience can provide a valuable perspective of what patients themselves find significant from the encounter.26–30 Understanding the patient experience is associated with improvement in delivery of quality, safe, clinically effective healthcare, and beneficial to guide health policy.21,23,29–35
Knowledge generated from exploring patient experience can inform paramedic education, and transform practice to align with community healthcare needs.21,31–33,35,36 The findings should also support the development of patient-reported outcome/experience measures as indicators of quality during out-of-hospital care.23,36–40
This research therefore aimed to investigate the patient experience of non-conveyance, cases where individuals receive an emergency ambulance service response and paramedic-led healthcare, that resulted in a decision to not transport the individual under care to a hospital ED.
Methods
Methodology
Qualitative inquiry using Constructivist Grounded Theory (GTc) methodology was used to explore patients’ experience of non-conveyance. This design was deemed the most appropriate; it allows an inductive approach to the interpretation and understanding of lived experience of healthcare in this context through the patients’ perspective without preconceived hypotheses.41–44
A qualitative approach provided a platform for patients’ voices to be heard; explaining the how and why of patient experience that quantitative methods are unable to uncover. 45 Grounded theory (GT) methods are useful when generation of theory is the desired outcome, little is known about the topic of interest, the research question is open-ended, and inherent social processes are embedded in the situation being investigated.46,47
Constructivism was adopted as the underpinning philosophy to this project. This philosophy proposes that reality is a subjective construction by individuals who develop meaning based on their interpretation of experiences gained through social interactions.48–50 It acknowledges that multiple, subjective realities exist; opposing the positivist and postpositivist assertion there exists a singular reality.48,51,52 This paradigm aligns with the phenomenon of investigation, and the lead researcher's relativist ontological and interpretivist epistemological assumptions.
Charmaz's constructivist version of GT embraces the position of the researcher as being a co-constructor of data; rather than as an objective collector. 53 Their experience and knowledge are valued as this promotes enhanced sensitivity towards concepts of relevance to the topic of investigation. Use of this expertise during data generation and analysis encourages insightful theoretical interpretation.46,47,53–55
Position of the lead researcher
The lead researcher (RK) conceptualised this research project, formed its design, conducted data generation, analysis, and theory generation; under supervision of all co-authors. Knowledge was generated through interaction between this researcher and participants to co-create understanding. 52 Raising awareness of the researcher's preconceptions is therefore necessary to demonstrate transparency of how knowledge has been generated.47,49,51
RK is an experienced senior paramedic, clinical educator in both vocational and tertiary education, they also provide peer support to paramedic colleagues. Their current role as an extended scope paramedic involves attending to patients who may benefit from referral to health services other than ED. This has provided them an established knowledge of the clinician's perspective of non-conveyance. RK's experiences, and own evolving role perception, evoked professional curiosity about how patients experience emergency ambulance service care that results in non-conveyance. Beliefs formed during this role include that by understanding the patient experience using rigorous research, some existing rhetoric and dogma evident amongst paramedic practice regarding non-conveyance, may be challenged.
RK's position is that of a White, European immigrant, from a working-class background who currently benefits from job security, good health, and unrestricted access to public and private healthcare. They acknowledge these factors, and other complex life experiences, could impart some associated subconscious biases into the research.
A common concern of grounded theorists is maintaining an appropriate balance between applying theoretical sensitivity whilst mitigating against the subconscious forcing of data. 47 To preserve the participants’ perspective, active processes of reflexivity were conducted from conception of the research. These involved the researcher acknowledging their own contextual assumptions, then considering how these may influence the data. 55 Memos specific to reflexivity were maintained throughout the research, during which the researcher challenged themselves with questions regarding the cognitive processes of decision-making they performed with regard to design, data generation, coding analysis, and theory development. The methods of constant comparison during analysis further enhanced reflexivity by considering multiple alternative perspectives to interpret participants’ meaning.
Trustworthiness is demonstrated through the transparency of how methodological congruence, and the researcher's interpretations, led to generation of conceptual categories that formed into the substantive theory. 56 A chain of evidence describing the coding processes is provided within the results section. An audit trail was maintained throughout conception, design and analysis of this research that includes memo-writing regarding analysis, decision-making, coding development, and theory development.
This article adheres to the Standards for Reporting Qualitative Research (SRQR). 57
Setting
Participants were residents of New South Wales (NSW) who received a response from paramedics employed by NSW Ambulance, an Australian jurisdictional ambulance service. This setting was selected as it represents one of the largest ambulance services in Australia.
NSW Ambulance provides clinical care, rescue and retrieval services, serving a population of 8,172,500 residents over a region of 801,1050 km2, including metropolitan, urban, and rural settings. 4 Emergency ambulance calls are processed through a medical priority dispatch system that determines case urgency and priority. Some calls may receive secondary triage, a system whereby a clinician undertakes further assessment to determine the most suitable response, which may include direction to alternate healthcare rather than dispatch of an ambulance resource. Standard response to a call requiring an ambulance involves two paramedic clinicians operating in accordance with clinical practice guidelines that describe their scope of practice.7,58 Paramedics in this setting are able to follow guidelines that allow them a level of autonomy to not convey patients who are assessed as not requiring ED attendance.
Recruitment and sampling
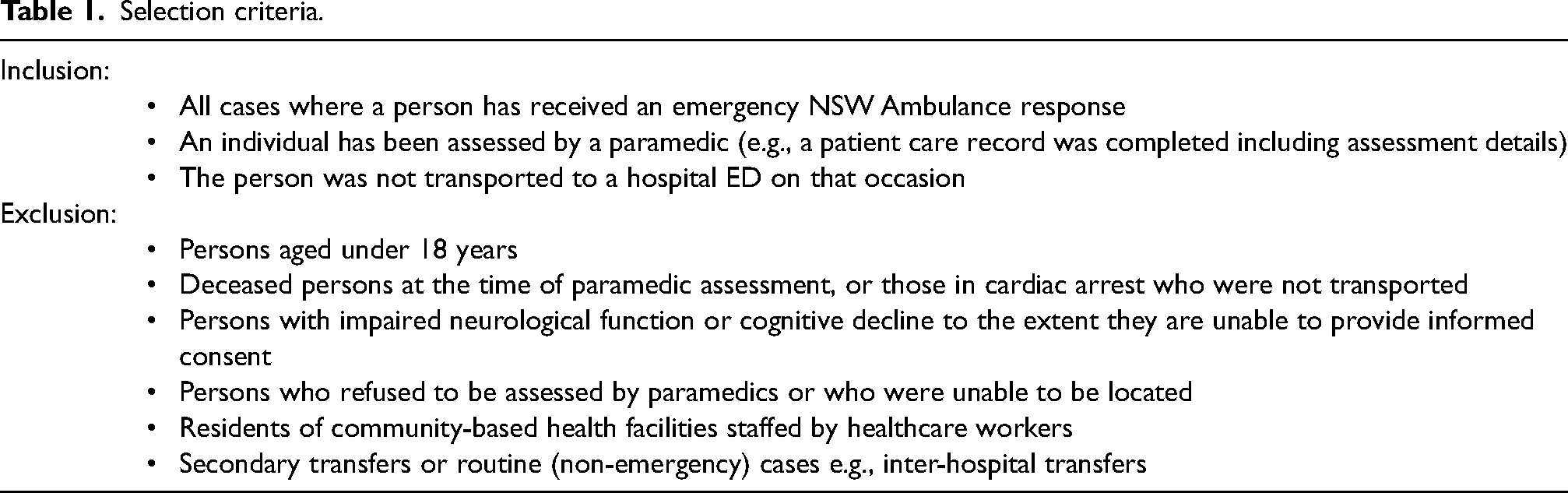
Purposeful sampling was used to recruit participants with recent experience of non-conveyance during a 15-month period between 01 August 2020 and 31 October 2021. Eligible participants were identified from clinical records accessed by an employee of NSW Ambulance using the criteria in table 1.
Selection criteria.
NSW Ambulance dispatched invitation letters sequentially to allow concurrent data generation and analysis from participants with recency of experience. Participants enrolled by returning a consent form directly to the research team by mail, or online via use of a QR code. During the recruitment period NSW Ambulance attended 956,095 people, of which 129,649 (13.5%) people were assessed and not conveyed. From these, 682 persons who met recruitment criteria were invited to participate.
Recruitment continued until theoretical saturation had been achieved; a level whereby sufficient explanation of core theoretical concepts and their relationships was established.47,59 To achieve this level of saturation, theoretical sampling, a key element of grounded theory methods, was used. Theoretical sampling allows the researcher to follow new lines of enquiry, and sources of data that may be of significance to theory generation, during data generation and analysis.46,47 Theoretical sampling took the form of exploring new avenues of data through use of additional, modified, and probing questions asked of participants.
Data generation – semi-structured interviews and analysis
Data was generated using in-depth, semi-structured interviews. These were conducted via telephone between a single researcher (RK) individually with each of the 21 participants. Rapport was first established, then a standard open question was asked of each of the participants: Researcher:
“Please tell me about your experience during the time the ambulance and paramedics attended you and you were not taken to hospital. Please take as much time as necessary, I’m interested in your story.”
Once the interview commenced, participants were encouraged to recollect their experience with use of open-ended questions, supported by an interview guide.
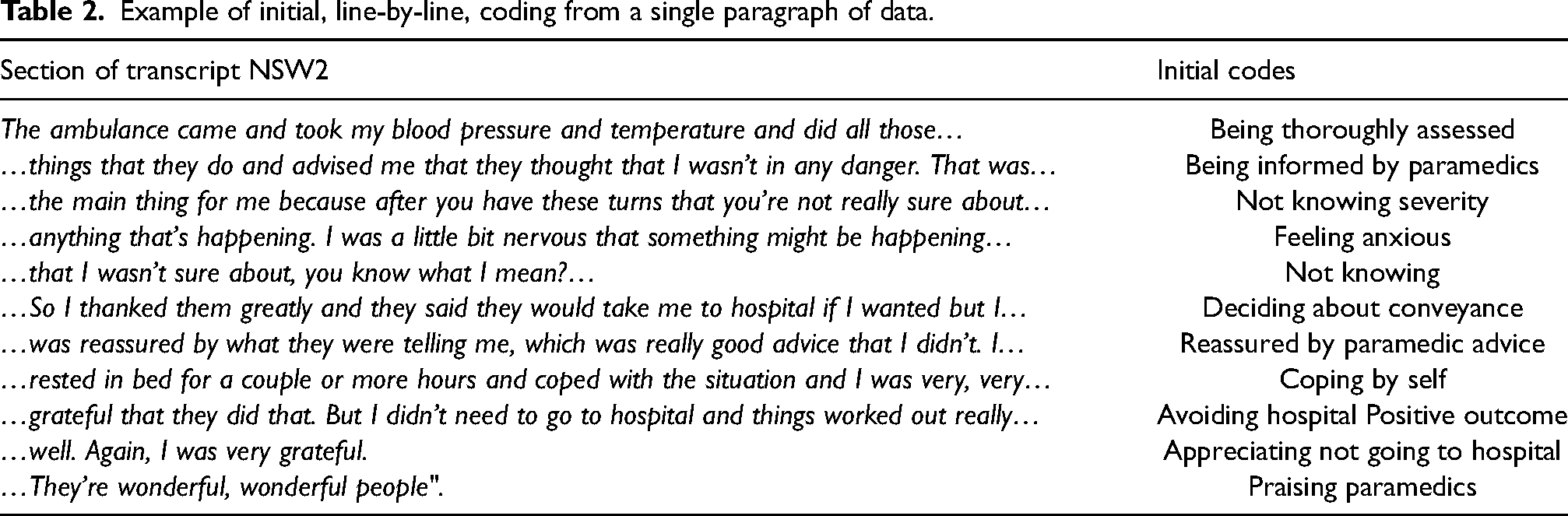
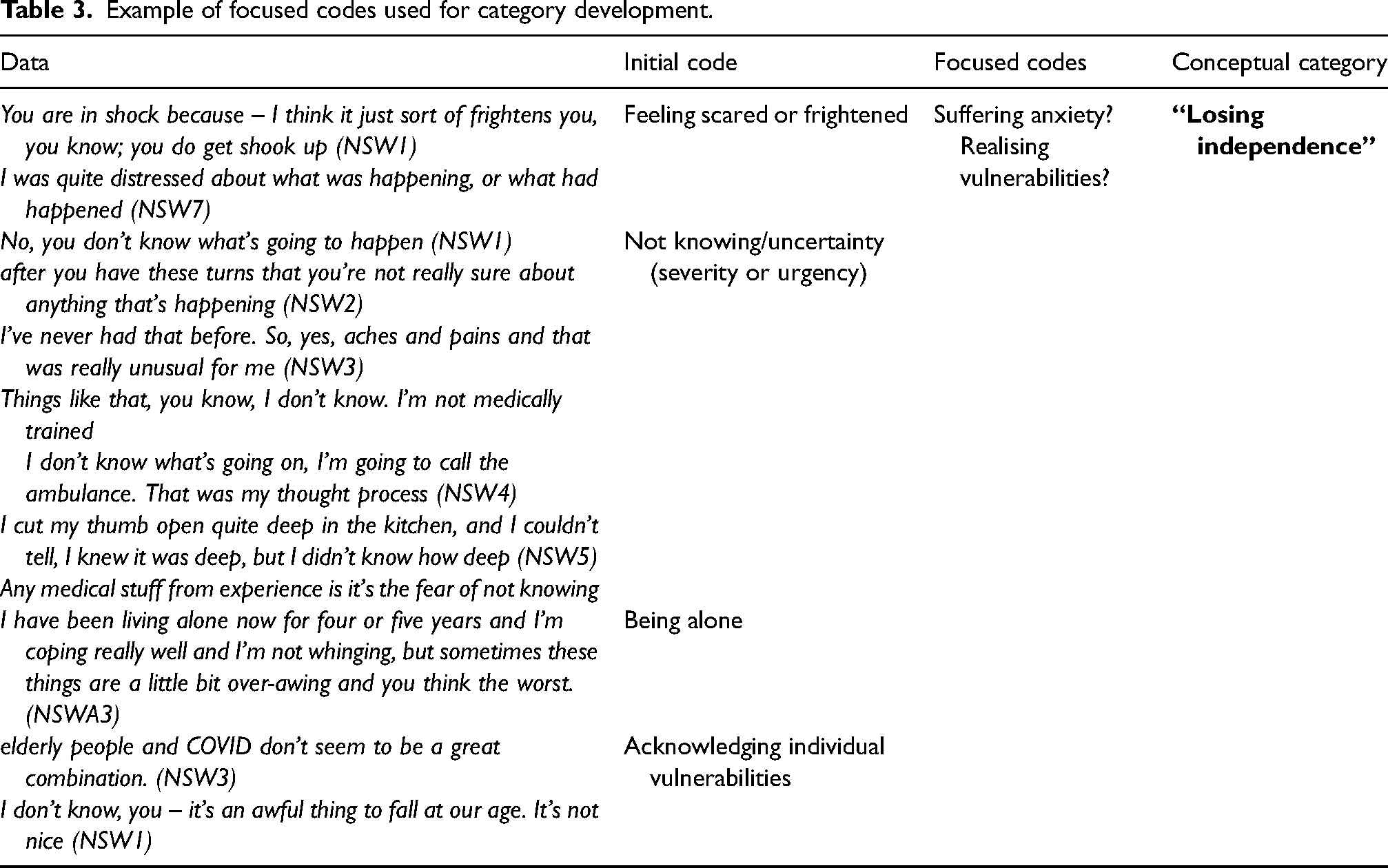
Interviews were digitally recorded, professionally transcribed, then de-identified prior to analysis. Methods essential to grounded theory were employed throughout the research.46,47,60 Generation of data occurred concurrently with analysis; an iterative process of initial, line-by-line (example Table 2), focused (example Table 3 & Fig 1), and advanced coding were applied throughout the analysis process, working back and forth constantly comparing existing and new data. Charmaz's approach to coding with ‘gerunds’, the noun form of a verb, was used to help detect what actions and processes were occurring. 47 NVIVO software was used as a data management tool to store, label, document memos, and link codes with memos. 61
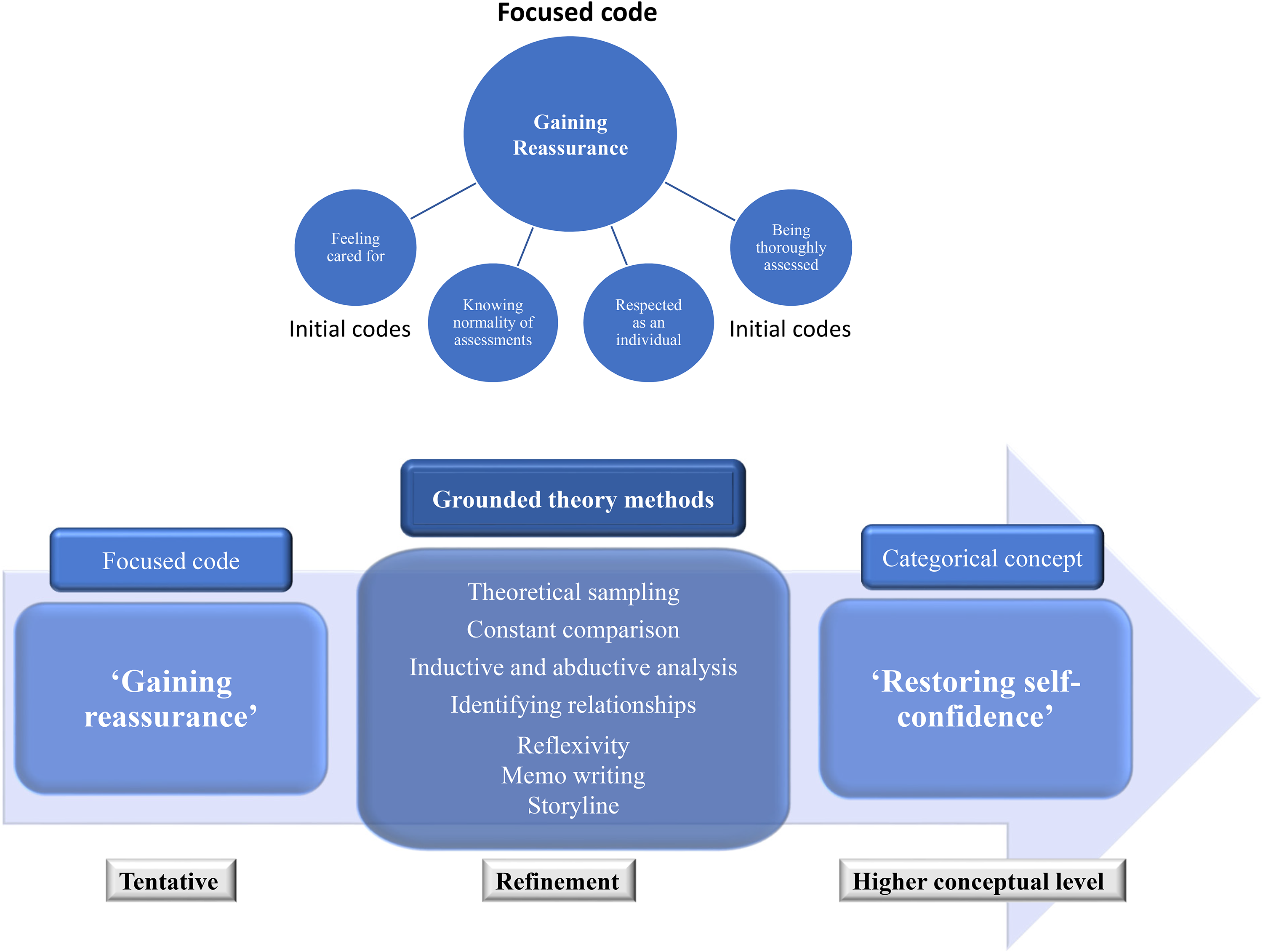
Diagrammatic representation of focused coding.
Example of initial, line-by-line, coding from a single paragraph of data.
Example of focused codes used for category development.
For consistency purposes, the lead researcher individually conducted all data generation and coding analysis to quarantine the generation of theory from external influences. A chain of evidence is provided below to provide transparency of the lead researcher's analysis and interpretation that led to the construction of the substantive theory.
During initial coding each line of data, rather than full sentences or paragraphs, was coded (labelled) to summarise its meaning. ‘Fracturing’ the data this way encouraged analysis to challenge assumptions, be open to all theoretical directions, reduce the likelihood of imposing the researcher's assumptions, and understand the participants’ view more closely.46,47,62
Focused coding was conducted once data had been generated from interview number 12. Codes of significance were identified, synthesised, analysed and conceptualised into tentative categories based on theoretic or conceptual similarity, then further refined using grounded theory methods (see Figure 1). 63 This stage provided freedom to compare these tentative categories with large batches of data to test if they explained what was occurring without making premature commitment. 47
Three main conceptual categories were constructed. Analysis using focused coding refined the developing concepts of ‘Suffering anxiety’ into the main category of ‘Losing independence’ that captured all variations of patient experience of this concept. The initial focused code of ‘Gaining reassurance’ was refined into ‘Restoring self-confidence’ through more abstract analysis (Figure 1). A third, separate category of ‘Self-management’ was constructed that corresponded with how participants continued to cope with their ongoing symptoms, or circumstances, once paramedics had departed.
To complete the final advanced coding analytic memos, conceptual categories, and social processes and their interconnected relationships were collectively weaved together at a greater conceptual level. Diagrammatic representations of the evolving theory were also created to encourage higher conceptual analysis. Finally, storyline, a form of narrative explanation, was used to both refine and present the substantive theory.45,47,64
Ethical consideration
Ethical approval was granted by the South Eastern Sydney Local Health District (SES LHD) Human Research Ethics Committee (2019/ETH00116), from the setting in which the project was conducted, NSW Ambulance (2019/STE00203), and by the research institute overseeing this project, the University of the Sunshine Coast Office of Research (project S201456).
Results
Participants
A total of 21 participants were interviewed and provided detailed accounts of their experience. Although 22 consent forms were received by the research team, of these, 1 person was unable to be contacted to arrange an interview, and therefore excluded from the study. Recruitment ceased when theoretical saturation was acknowledged; the final three interviews revealed no new theoretical concepts, nor added anything of further relevance to the research aims.47,65 Duration of interviews ranged from 22 to 72 min with a mean of 38 min. Age ranged from 35 to 79 years with a mean age of 60 years. All participants were asked their gender, 17 responded as female and 4 as male.
Table 4, ‘Participant characteristics’, demonstrates the broad range of participant-reported events that instigated a call to the emergency ambulance services. Two participants received pharmacological intervention, with a further two receiving first aid (wound dressing, and joint strapping). Participants’ postcodes were converted to regional status using the ‘Modified Monash Model’ (MMM) to identify remoteness of location and de-identify this data. 66
Participant characteristics.
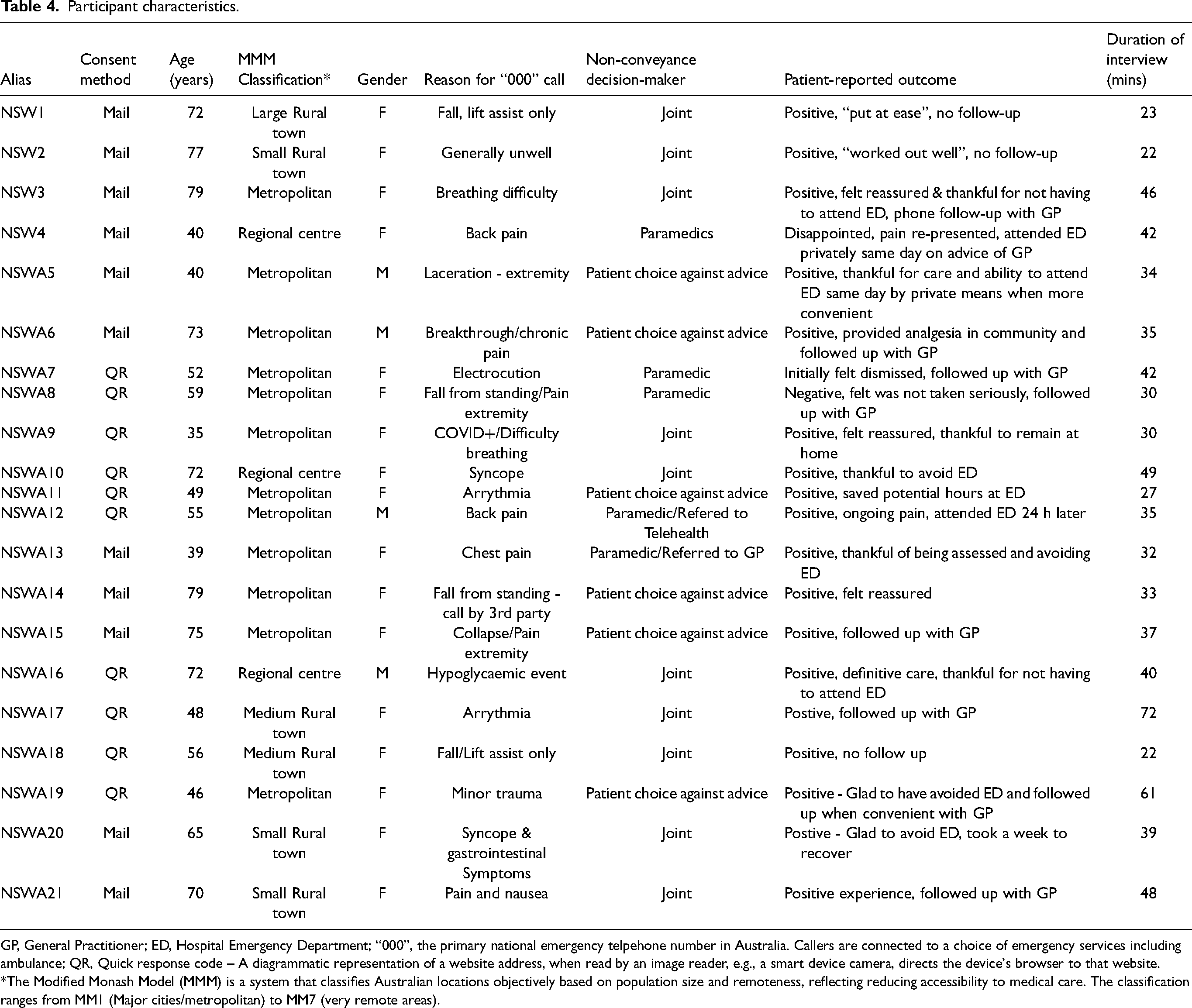
GP, General Practitioner; ED, Hospital Emergency Department; “000”, the primary national emergency telpehone number in Australia. Callers are connected to a choice of emergency services including ambulance; QR, Quick response code – A diagrammatic representation of a website address, when read by an image reader, e.g., a smart device camera, directs the device's browser to that website.
*The Modified Monash Model (MMM) is a system that classifies Australian locations objectively based on population size and remoteness, reflecting reducing accessibility to medical care. The classification ranges from MM1 (Major cities/metropolitan) to MM7 (very remote areas).
Main categorical concepts
A substantive theory centred on ‘Restoring self-efficacy’ was generated. This theory comprises three main categorical concepts and their interconnected relationships that explains how patients experience their journey through the phenomenon of non-conveyance. ‘
The core conceptual category is described in detail as this was central to patient experience.
Restoring self-confidence
The categorical concept of ‘Restoring self-confidence’ appeared early in data with frequency, and strength of sentiment. It represents underlying processes of how patients experienced non-conveyance, therefore was recognised as having great significance to the research question. Restoration of confidence weaved through experience, connecting different stages of the patients’ journey through this phenomenon, needing, seeking and gaining confidence. Patient experience had moved from negative emotions to positive ones, moving from a sense of vulnerability, to feeling sufficiently confident to manage in their own environment without transport to a hospital ED. Concerns that led to an emergency ambulance being requested had been resolved through a process resulting in a non-conveyance outcome.
The data provided strong evidence that the pivotal point of non-conveyance decision balanced on patient interpretation of their interactions with the attending paramedics. Participants often described an amount of relief connected with the arrival of paramedics, further being ‘put at ease’ through experiencing combined positive professional and compassionate interaction with paramedics. Levels of professionalism and compassionate care displayed by paramedics were significant factors influencing the level of trust patients placed in them and their care. Professional care was experienced when the paramedics demonstrated clinical competence by validating patients’ individual concerns, performed a thorough clinical assessment, used technical equipment, and through verbal and non-verbal communication reinforced, or exceeded, the expected level of clinical knowledge.
Compassionate care was experienced when the paramedic was perceived to acknowledge, understand and act with empathy upon the individual's circumstances and unique vulnerabilities through behaviour and verbal communication that demonstrated genuine empathy. Being provided choice of whether the patient wanted to attend ED was valued and reinforced a sense of self-confidence. When this care coincided with normality of clinical findings, it positively influenced patients’ confidence in their own ability to manage their circumstances when deciding about conveyance to hospital or remaining in the community. “…not when you're out of your – you're out of your comfort zone anyway because you’ve got something weird happening that you're not sure of and then you get some horrible person that would make you feel not very good at all. But when….they give you confidence in yourself I think it can become, it's not mind over matter but when you feel that you're being well looked after and you're being told what has happened it does mentally make you feel better which I think also then goes to physical as well..” NSWA10, Syncope
The ‘restoring self-efficacy’ theory of non-conveyance
The substantive theory of non-conveyance is presented in diagrammatic form (Figure 2), then explained using storyline; a mechanism that provides narrative explanation of the concepts, categories and their interrelationships in a format contextually rich to paramedicine.45,67
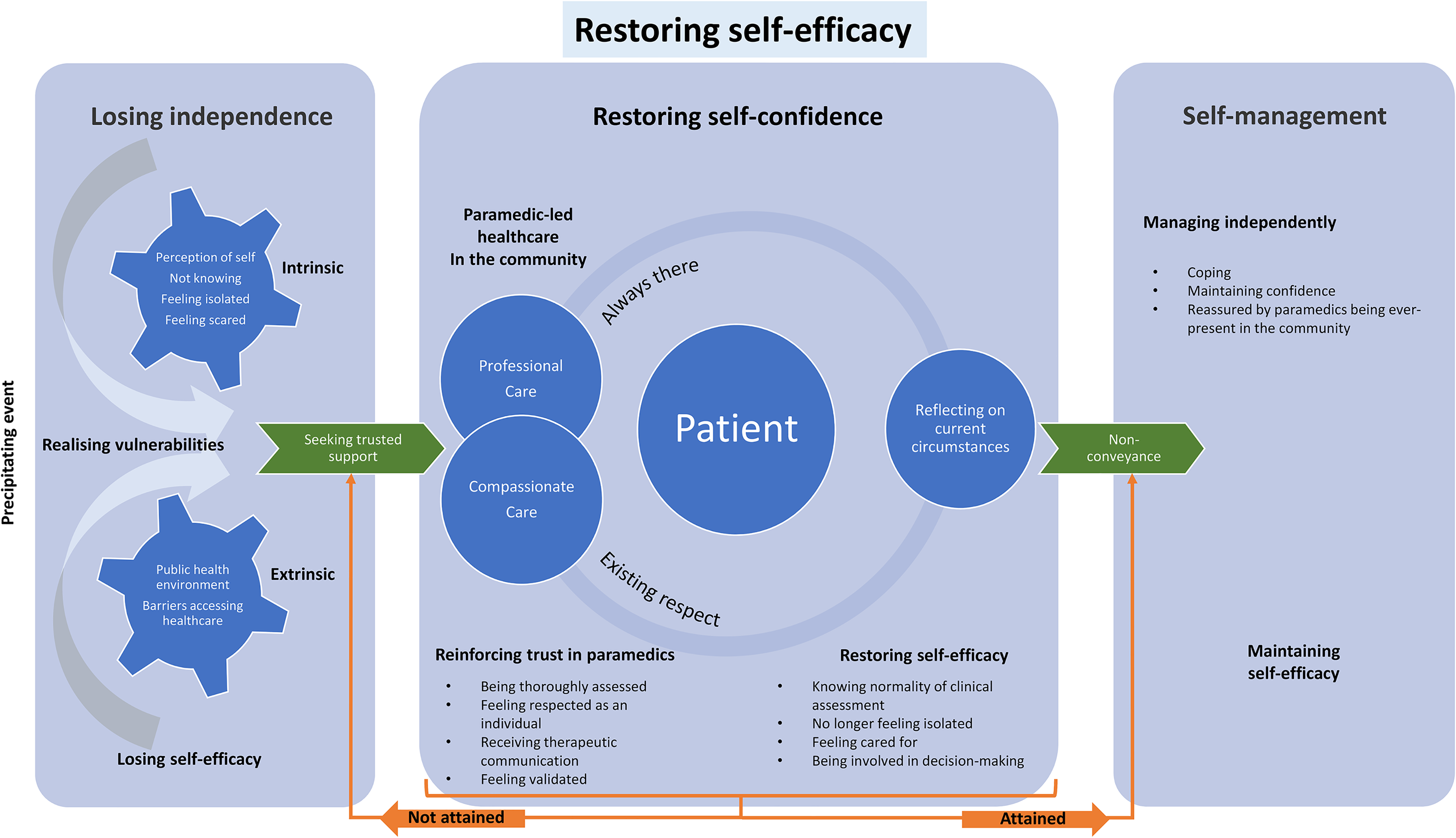
Diagrammatic representation of ‘Restoring self-efficacy’, a substantive theory explaining patient experience of non-conveyance.
Storyline
Losing independence
Constructs of what instigates an emergency ambulance being requested are dynamic, complex and unique to a patient's individual circumstances. Patients who experience the phenomenon of non-conveyance have suffered unscheduled adverse events in the community that results in them eventually losing confidence to manage independently.
When considering resolution, they assess their situation, reflecting on both intrinsic and extrinsic factors, forcing them to realise their circumstantial vulnerabilities. They recollect memories of recent, or previous health experiences to help them make sense of what is happening. Intrinsic factors include perception of self, not knowing (the clinical urgency or severity of the concern), and feeling isolated. They suffer emotions such as feeling scared and vulnerable. “When you live by yourself - I lost my husband six years ago and I'm by myself and I'm coping really well and I'm not whinging, but sometimes these things are a little bit over-awing and you think the worst. You think, oh gosh, what's going to happen to me? NSW2, generally unwell
External factors, such as those created by living in a pandemic environment, may escalate a sense of anxiety; in addition, perceived limited access to health services further narrows potential of self-resolution, and may generate frustration. “So it's like you needed that reassurance because the paramedics were the only people that were willing to give you that reassurance in person. Because the GPs didn’t want a bar of you and even the COVID doctors, it was just all via Telehealth”
NSW9, Covid+/Difficulty breathing
Where a patient is uncertain regarding the clinical urgency, or severity, of symptoms; or where they are unable to resolve concerns themselves, (or with support of trusted associates), assistance is sought from trusted external health provider such as community-based healthcare or telehealth support. “Any medical stuff from experience is it's the fear of not knowing, having been through what I’ve gone through, and having initial tests, and then having scans, then having to wait a week for the outcome, it's horrible, and it's that fear of not knowing what it is. Even when you know what it is, at least then, then you can deal with it…” NSW12, Back pain
If actual or perceived barriers exist to accessing healthcare, uncertainty remains, or the situation is considered an emergency, health-seeking behaviour progresses to a request for emergency ambulance services. “So you just needed a means of knowing that you're okay” NSW9, Covid+/Difficulty breathing
“It just didn't and it got worse and I thought, I better call an - never having done this - I better call an ambulance before it's too late and I can't call an ambulance.” NSW3, Breathing difficulty
Restoring self-confidence
Having an existing societal concept that ambulance services are there just for emergencies causes some patients to deliberate whether their situation necessitates this level of health service. Where their vulnerabilities are significant, or they feel no other option exists, the ambulance service is recognised as always being ‘there’, always available; and this provides a sense of reassurance.
Relief was gained knowing that the decision to call the ambulance has been made, and that someone is coming. Further comfort is gained where there is a short duration until arrival of the ambulance; where a delay occurs, patients justify to themselves that the system has prioritised them accordingly, accepting that other people may have higher priority needs. Uncertainty of how long they take may cause discomfort and anxiety for other patients. A greater sense of relief is gained on arrival of the ambulance crew as patients no longer feel isolated; now present are highly respected, trusted, professionals with knowledge and technical equipment that can answer their uncertainty, determine whether they are suffering a significant illness, or can resolve their concerns. “These two great men arrived with all of this equipment and everything and I started feeling better already” NSW3, Breathing difficulty
While highly respected, there is an element of personal assessment of the paramedics on arrival. Patients make ‘first-appearance’ judgements on whether the paramedic(s) is/are clinically competent or have the capability to assist with their problem. Two powerful, closely interconnected skills – receiving both professional, and compassionate care need to be experienced for the individual to reinforce their trust in paramedics that results in restoration of self-confidence. “they were kind, and they were professional, and they were compassionate. I would – that was all I would expect of them…they deal with so many people, but they did it in a respectful, compassionate, kind manner, and I was most appreciative of that.” NSW15, Collapse/Pain extremity
Professional care is experienced when a person feels thoroughly assessed, technical equipment is used, and verbal and non-verbal communication reinforces, or exceeds, the expected level of clinical competence. “when I saw what they have I went, wow, that's incredible. Like, they just whip out this 12-lead ECG, tested my glucose. The gear was so impressive, and I think that part of me kind of went, oh, that's really good, we're not doing a half/half attempt here. I was really comforted by that…” NSW17, Arrythmia
Compassionate care is experienced when the patient feels they are being respected as an individual experiencing circumstances exposing their unique vulnerabilities that were acted upon with empathy while receiving therapeutic communication. “…when you go to see a specialist…they don’t need to explain whatever they're doing. They know what they're doing so you accept that.. But when it's an ambulance person, the first people there, I think, yes, it helps a lot more when they build your confidence up as well and treat you like a human being not like a patient on the table.” NSWA10, Syncope
“they listened to me which a lot of medical people don’t. So, I was absolutely blown away by them. I have nothing but praise for them…I really found them very, very thorough, very, very professional, very, very caring and just so well-mannered …. NSW6, Breakthrough pain
When patients perceive they have not received professional care, such as inadequate assessment, or feel they are not being taken seriously, they are unable to trust the paramedic. If this is not resolved, the patient does not reach a state of restored self-confidence. Feelings of anxiety and uncertainty continue until the patient has received professional aspects of care. “I’m not saying I wasn’t completely taken seriously but I called the ambulance because I thought I really need to go to hospital and have this tested because I thought it might be something seriously wrong here. But then they said, we don’t think you need to go to hospital. So I was, well you guys know better than I do because you do this all the time, whether I need to go to hospital or not……Yeah. The next day I’m in so much pain that I really do need to do something, I need to go see my GP and get a referral.” NSW8, Fall/pain extremity
Influenced by interpretation of their interaction with paramedics, patients reflect on their current circumstances with a revised perspective. This contributes to the restoration of self-confidence. Patient concerns when considering whether to attend hospital highlight the personal vulnerabilities that led to ambulance services being called in the first place. These causes of concern include perception of being isolated, losing one's individuality and identity, not being listened to, and experiencing lengthy delays at hospital. When their original concerns have been addressed and resolved, through their partnership with paramedics, they switch from uncertainty or belief in the need to attend hospital, to one where they hold restored self-confidence to manage within the community. A strong contributor to this is being advised of the normality of clinical examination and vital signs. “Look, the only thing - it just gave me comfort to know that there wasn’t anything seriously wrong. That partly helped from a head down point of view of maybe relaxing. Now, okay, well, I know what it is, I know what it's not.” NSW12, Back pain
Emotions experienced include sense of relief, reassurance and gratitude. “I suppose one of the biggest things, I think, for most people, I can't speak for other people, of course, but for me, particularly, would be that reassurance” NSW7, Electrocution
“they asked if I wanted to go to hospital. I said no because COVID was out and about. Not that we’d had a lot up here, but I still wasn’t keen on going in to somewhere that people who have COVID are taken. If you don’t have to go into places like that, you don’t exposure yourself unnecessarily.” NSW15, Collapse/Pain extremity
Self-management
Patients demonstrated a change in behaviour as a result of their reconstructed perspective of their circumstances and environment. After the episode of care resulting in non-conveyance, patients still experiencing symptoms continued to self-manage at home. The patient-paramedic partnership has restored self-efficacy, the individual's belief in their own capability to manage their concerns or symptoms in the community. When definitive healthcare has been received from paramedics within the community, this results in less of a need to seek further health advice or use alternative care options. “I was starting to feel a lot better. I didn’t feel myself for about two weeks after that episode. I was really unwell. It took about 10 days to two weeks to feel back to normal and I haven’t had … so I was comfortable with the decision not to go.” NSW21, Pain and nausea
Factors other than the direct paramedic-patient partnership supports restored self-efficacy. Confidence is gained from a realisation that patients are able to receive paramedic care in their community without having to attend ED, further enhanced by a sense of security that emergency ambulance services are ever-present in the community. “If I needed them to come back give them a call and they’d come straight back…that was a confidence thing when they said, okay, well, you’ve decided not to go but if you need us ring up and we will come straight back. You won’t have to wait. Somebody will be there straightaway…” NSW10, Syncope
“It meant comfort like they’re not just driving off into the sunset. You can call us, and you don’t feel bad about calling if you have to.” NSW14, Fall from standing height
Discussion
The aim of this research project was to investigate how patients experience non-conveyance. Adhering to constructivist grounded theory methods, the substantive theory of ‘restoring self-efficacy’ was established; a conceptual model that contributes original, explanatory knowledge relating to patients’ experience of non-conveyance. The results may inform paramedic practice, improvements in patient-centred care, and new models of ambulance service delivery.
A strength of substantive theory is the richness of insight they produce that is contextual to the setting in which they are generated. 47 This theory provides valuable knowledge, grounded in data constructed between patients with expert understanding of the specific phenomenon and an experienced provider of clinical care. By doing so it contributes to narrowing the gap of knowledge that was identified by the scoping literature review associated with this research project. 15 This insight may be useful in supporting patient-centred care in similar healthcare settings.
Central to patients’ experiences was restoration of self-confidence through several interactions and processes that result in their ability to self-manage in the community. This occurs when patients perceive they have received constructs of professional and compassionate healthcare from paramedics for circumstances that do not require urgent conveyance to ED. The theory highlights processes that support this change in patients’ self-efficacy from being unable to manage independently, to having restored self-confidence to manage. The inductive methods used further identified that an entire continuum of care was of relevance. Patient experience is not only a sum of all interactions with the health service; prior experiences and beliefs, events and circumstances preceding healthcare intervention, awaiting care, and once the clinician interaction has ceased, all contributed to overall patient experience in this setting.
Relation to existing research and theory
The influence of receiving both ‘professional and compassionate’ care towards patients’ confidence in the non-conveyance decision are also reflected in similar research in a Dutch setting. 68 Themes identified in research of paramedic-led care in the setting of women's experience of unplanned birth out-of-hospital also revealed the combination of ‘clinical competence’ and ‘bedside manner’ was significant to generating trust in paramedics which in turn led to confidence of the birthing women. 69 There is clearly a need, and value being attributed, to patient-centred, humanistic, and emotional intelligence aspects of paramedic care being provided alongside the technical aspects.15,70–73
The concept of self-efficacy noted in these findings is also acknowledged within existing formal theories and models of health behaviours, particularly Social Cognitive Theory.74,75 Such formal theories are intended to be generalisable and predictive. A benefit of this substantive theory over formal theory is how specific it is to the context of this phenomenon, and how it captures the entirety of how experience is constructed. Future research considering integration of this theory with extant knowledge may be useful for its evolution.
Implications for paramedic practice and design of health system response
Theories of patient experience and models of health behaviour are useful to support professional domains.29,76 This research contributes knowledge that may assist to define scope, philosophy, role perception, and professional identity by explaining, and supporting understanding of, the needs of patients that paramedicine serves.75,76 As such, the findings should inform paramedic education, clinical practice, and quality indicators relating to non-conveyance.
The findings contribute new knowledge about how patients construct and interpret behaviours and skills of paramedics. 5 By highlighting how patients interpret these behaviours this research is useful to inform evidenced-based paramedic education, and practice, that recognises the importance of delivering compassionate care concurrently with clinical competency. The constructs identified may be useful to aid curriculum design at pre-registration level, and inform professional development interventions for those currently practicing as paramedics. Simulation is recognised as an effective teaching modality for paramedics; these constructs of patient experience, and the participants’ circumstances, may be useful in the design, and measurement of educational simulations focused on non-conveyance events.
These findings align with wider literature that suggests a shift away from research assessing appropriateness of patients accessing healthcare via emergency services, to investigate how best to provide them navigational support when they seek unscheduled healthcare.77–80 Participants described dynamic, complex circumstances, and individual vulnerabilities that led to them accessing healthcare via an emergency ambulance service. Other research has also recognised drivers of action to seek emergency care include perceived urgency, uncertainty, need for reassurance, timely access, and barriers to access primary healthcare.20,77,78,80–83
The participants valued paramedic-led healthcare in the community, and/or being assisted with navigation to access healthcare that suited their individual needs. Negative experiences occurred when patients felt their concerns were not validated, they were not taken seriously, or the reassurance offered was not sincere. This highlights the need of paramedics to consider individual patient's vulnerabilities that lead to them requesting emergency services. Understanding, and acknowledging a patient's vulnerabilities supports validation, trust and confidence in the paramedic; it further identifies the holistic needs of that patient to guide appropriate care planning.
The research supports ongoing consideration of paramedics to integrate into wider health systems outside of their traditionally understood roles. Paramedics were highly respected by participants as valued healthcare professionals; they supported patients by restoring confidence to self-manage their concerns, and/or provided definitive care in the community when they did not require ED attendance.
Non-conveyed cases represent a significant volume of ambulance service workload which, paradoxically, paramedics may not be well prepared to manage due to reasons of professional identity, role perception, organisational culture and training.84–86 Some Australian ambulance services have developed response models to meet increasing demand and changing community needs. This may involve specialist paramedics, more commonly being referred to under an umbrella term of ‘community paramedic’.7,87–93 Shannon et al. identified a lack of quality literature to guide formation of such programs; suggesting a need for evidence, that includes qualitative research, to develop education, scope and outcome measures into the impacts of such initiatives. 93 This research provides a conceptual framework of how patients make-sense of requiring and receiving unscheduled healthcare from paramedics in the community; it may be useful to inform curriculum design, clinical guidelines, and construction of outcome measures for such initiatives.
Patient-reported indicators of healthcare
This explanation of patient experience supports the growing body of literature that recommends validated tools that monitor patient experience should be included in performance and quality indicators of both ambulance service delivery, and paramedic care.35,37,38,70,94 Organisational audit or governance measures into non-conveyance cases could use this framework as a tool to assess whether a patient-centric approach has been followed during care.
Understanding why patients re-present to hospital or primary care should also be included for research that uses re-presentation rates as a metric when investigating patient-safety of non-conveyance. 1 In this research some patients reported presenting to ED by private means or attending their GP within hours to days of paramedic care that was part of an agreed plan between the paramedic and patient.
Limitations
At the time the research was being conducted, the setting of the research was being impacted by the COVID-19 pandemic. The findings of this research identified external factors including the pandemic environment as impacting on participants’ sense of vulnerability, increased difficulty accessing healthcare, and fear of exposure to infection in hospital. However, it is unknown to what extent this affected the overall concepts uncovered. Other research has suggested that this environment had a significant effect on requests for ambulance services, decisions about conveyance, and deaths from out of hospital cardiac arrests.95,96
The perceived roles of interviewer and participant may generate barriers to full disclosure of information, increase self-reporting bias and create perception of a power differential.46,47 Attempts to mitigate this included establishment of rapport at the beginning of interviews to encourage a sense of reciprocity.47,97
Conclusion
This research provides rich insight into the poorly understood perspective of patients’ experiences of non-conveyance. Patients’ experiences of non-conveyance encompass more than just the involvement of paramedic-led healthcare. Experience incorporates prior beliefs, past experiences, perception of self, and external factors when they are forced to realise their circumstantial vulnerabilities. It continues through interpretation of social interactions during paramedic-led healthcare to include a period of coping, self-managing in the community once paramedic care has ceased.
The conceptualisation of self-efficacy was identified as central to understanding how patients processed their journey through this phenomenon. Restoration of self-efficacy and the conveyance decision balanced on patients’ interpretation of their interactions with paramedics. Patients’ experience reinforced trust in paramedics when they perceive they have received both clinically professional, and compassionate care that acknowledges their unique vulnerabilities. When this coincides with conditions that do not require urgent attendance at ED, patients report restored confidence to self-manage in the community.
Future research could support validation and evolution of this theory; in particular, the impacts of applying this knowledge towards patient-centred care, paramedic education and practice, and design of quality indicators surrounding non-conveyance situations.
Footnotes
Acknowledgements
This research would not have been possible without the support of the participants who volunteered their time, sharing their vulnerabilities and experiences. Thanks also to NSW Ambulance for their support with recruitment, in particular Alyce Worboys. To maintain separation of confidential data, Alyce performed the substantial recruitment process of screening potential participants and mailing invitation letters.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
Financial support was kindly provided by the Australasian College of Paramedicine (ACP), the peak body representing and supporting paramedics across Australia and New Zealand. Funding from the Australian Government Research Training Program Scholarship also supported this research.