
Abstract
Introduction:
Temperature is a key factor influencing the occurrence of out-of-hospital cardiac arrest, yet there is no equivalent study in Hong Kong. This study reports results involving a large-scale territory-wide investigation on the impacts of ambient temperature and age–gender differences on out-of-hospital cardiac arrest outcome in Hong Kong.
Methods:
This study included 25,467 out-of-hospital cardiac arrest cases treated by the Hong Kong Fire Services Department between December 2011 and November 2016 inclusive. Simple correlation and regression analyses were used to examine the relationships between out-of-hospital cardiac arrest cases and temperature, age and gender. Calendar charts were used to visualise temporal patterns of pre-hospital emergency medical services related to out-of-hospital cardiac arrest cases.
Results:
A strong negative curvilinear relationship was found between out-of-hospital cardiac arrest and daily temperature (r2 > 0.9) with prominent effects on elderly people aged ≥85 years. For each unit decrease in mean temperature in °C, there was a maximum of 5.6% increase in out-of-hospital cardiac arrest cases among all age groups and 7.3% increase in the ≥85 years elderly age group. Men were slightly more at risk of out-of-hospital cardiac arrest compared with women. The demand for out-of-hospital cardiac arrest–related emergency medical services was highest between 06:00 and 11:00 in the wintertime.
Conclusion:
This study provides the first local evidence linking weather and demographic effects with out-of-hospital cardiac arrest in Hong Kong. It offers empirical evidence to policymakers in support of strengthening existing emergency medical services to deal with the expected increase in out-of-hospital cardiac arrest in the wintertime and in regions with a large number of elderly population.
Introduction
Out-of-hospital cardiac arrest (OHCA) is a critical and life-threatening condition. It has received increasing global attention because of low survival rates for OHCA patients.1,2 Hong Kong reported a high incidence rate of OHCA with 71.6 cases per 10,000 people in 2015, which was higher than 57 cases per 10,000 people in the United States3,4 and 44.4 cases per 10,000 people in South Korea. 5 The high case fatality rate of OHCA is found to associate with both patient and environmental factors. OHCA cases seemingly occur more frequently on days with extreme low and high temperatures.6–11 Moreover, studies have consistently showed that incidence/survival of OHCA is influenced by responsiveness of emergency medical services (EMS) as well as patient characteristics (such as gender, age, habits and medical history). Specifically, OHCA affects more male,12,13 elderly, 12 overweight, 13 and people with cardiovascular and respiratory diseases. 14 Seasonal patterns of cardiovascular mortality is also evident in United States,15,16 Britain, 17 Australia, 18 Germany 19 and Japan. 20
There have been no representative large-scale studies on OHCA in Hong Kong. The increasing number of OHCA cases expects to be a major public health concern for Hong Kong particularly in the presence of ageing population and increasing frequency of extreme weather events. A better understanding of weather-related and demographic effects on OHCA is helpful for relevant authority to better prepare for the expected increase in the demand for EMS. This study examines the relationships between OHCA cases and three aspects: (1) weather – ambient air temperatures, (2) demography – age and gender and (3) ambulance demand – temporal patterns. Findings of this study will have direct implications for public health policy and strategic planning of EMS provision.
Methods
The study data included 25,467 cardiac arrest cases (excluding incomplete and duplicate records) treated by EMS provided by the Hong Kong Fire Services Department (HKFSD) between December 2011 and November 2016 inclusive. Each OHCA record was anonymised and contained personal data (age, gender, medical condition etc.) and relevant items from the incident report (date, time, location, treatment rendered, outcome etc.). Ambient temperature data (including daily maximum, minimum and mean temperatures) for the same period were downloaded from the website of Hong Kong Observatory (HKO).
The relationships between OHCA cases and weather or demographic variables were examined by means of simple correlation and regression analyses. Temporal patterns of EMS were analysed using calendar charts or calendar heat maps 21 that use colour gradients to show hourly variations in the demand of EMS by days and months of the year.
Results
OHCA and air temperatures
Table 1 shows the percentage change in cardiac arrest cases for each unit drop of mean temperature in °C. The table entries register OHCA cases for ‘all age groups’ and the ‘≥85 years age group’. The number of OHCA cases tended to increase with decreasing mean temperatures. The maximum rate of change was 5.7% for all age groups and 7.3% for the 85 years and above age group. The elderly age group not only showed higher risks of OHCA in response to cold temperatures but also reacted much earlier at mean temperatures of 17°C and below compared with 14°C for all age groups.
Percentage change in cardiac arrest cases by temperature differences (values highlighted in bold represents the maximum rates of change in cardiac arrest cases and corresponding mean temperatures in ‘all age groups’ and ‘age group ≥85 years’).
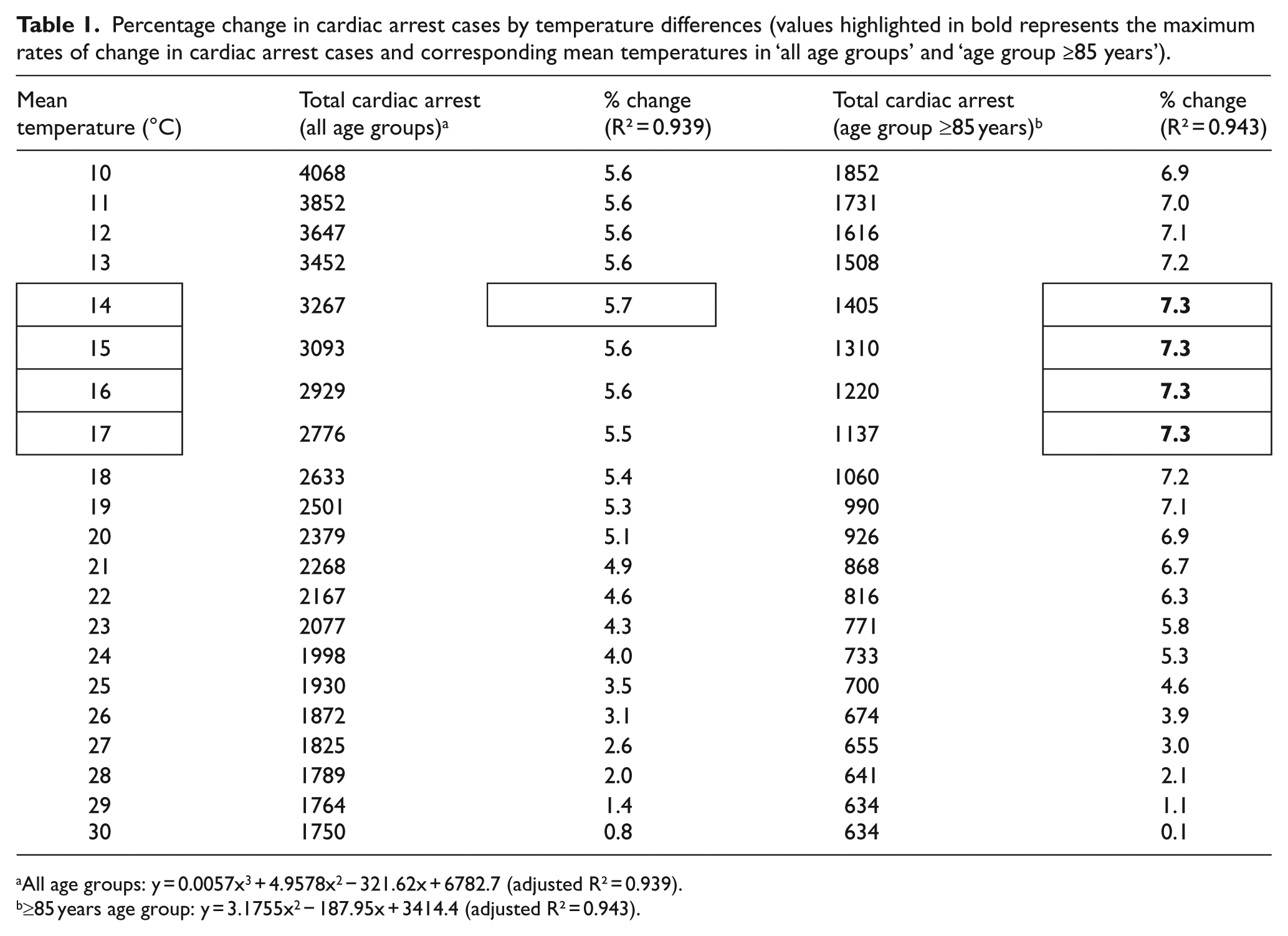
All age groups: y = 0.0057x3 + 4.9578x2 − 321.62x + 6782.7 (adjusted R² = 0.939).
≥85 years age group: y = 3.1755x2 − 187.95x + 3414.4 (adjusted R² = 0.943).
A strong negative curvilinear relationship was found between daily temperatures (including maximum, minimum and mean temperatures) and OHCA cases (r2 > 0.9; Figure 1). The plot shows that cardiac arrest cases increased exponentially with decreasing temperatures. More prominent effect was evident on daily minimum temperatures (r2 = 0.9507) as they dropped below 14°C. Although diurnal temperature difference is not uncommon in Hong Kong, the temperature difference gets comparatively larger in cooler season, especially from December to January. It is also noteworthy that cardiac arrest cases decreased with increasing daily maximum temperatures but then rebounded from 33°C onwards. The rebound implied that extreme hot temperatures could also be a risk factor for cardiac arrest. However, the overall trend for Hong Kong showed that extreme cold weather in the winter resulted in more cardiac arrest cases than hotter temperatures in the summer.
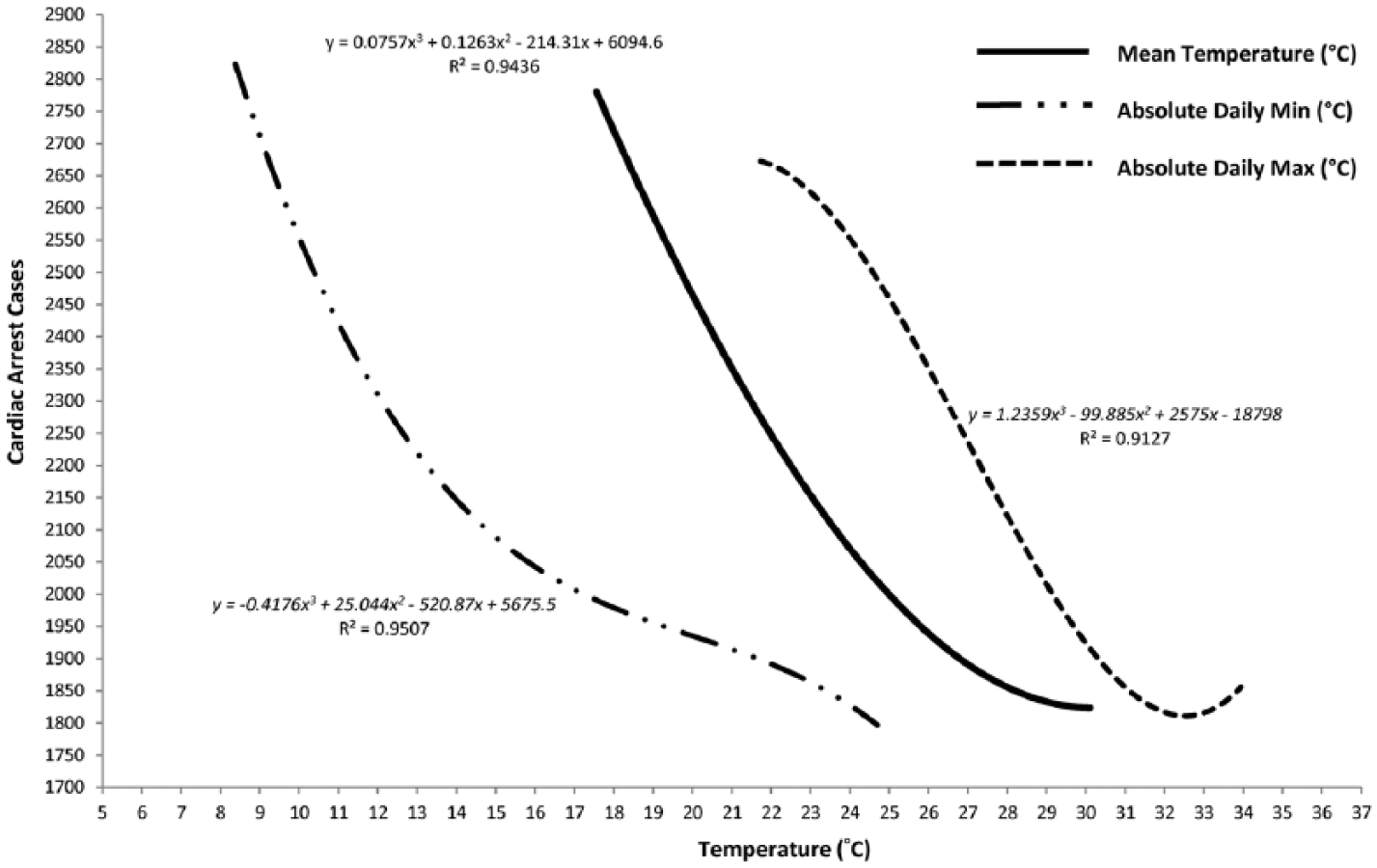
Relationships between daily temperatures (minimum, mean and maximum) and OHCA cases. Strong negative curvilinear relationships were evident between daily temperatures and OHCA.
Apart from the mean temperature, this study also found a strong positive curvilinear relationship between diurnal temperature variation (the difference between daily maximum and minimum temperatures) and cumulative OHCA cases (r2 > 0.97; Figure 2). The increase in cumulative cardiac arrest cases started to level off after a 6°C difference in diurnal temperature variation.
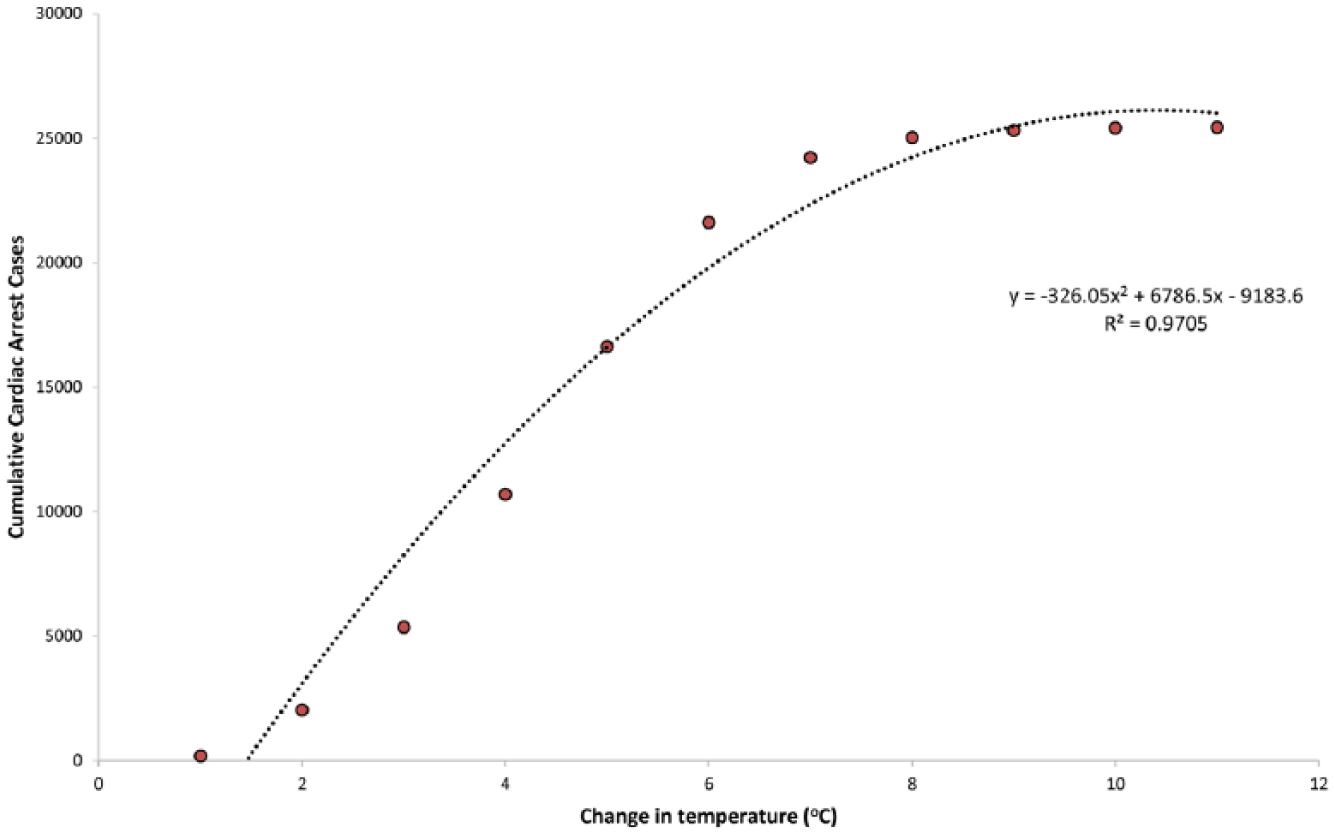
Relationships between diurnal temperature variations (°C) and cumulative OHCA cases. Strong positive curvilinear relationships were evident between diurnal temperature variations and cumulative OHCA cases.
OHCA and age or gender groups
Table 2 shows the breakdown of monthly OHCA cases by different age groups. The table shows that elderly people (aged ≥65 years) accounting for nearly 78% of total cases in the past 5 years were among the largest group contributing to OHCA cases in Hong Kong. The occurrence of OHCA among younger age groups was relatively lower. For instance, OHCA cases for the 30–64 years age group were only a third of cases for the 65 years and above elderly group. OHCA displayed an initial upward trend by age followed by a sharp increase in incidence after the age of 74 years.
Monthly cardiac arrest cases by different age groups (December 2011–November 2016).
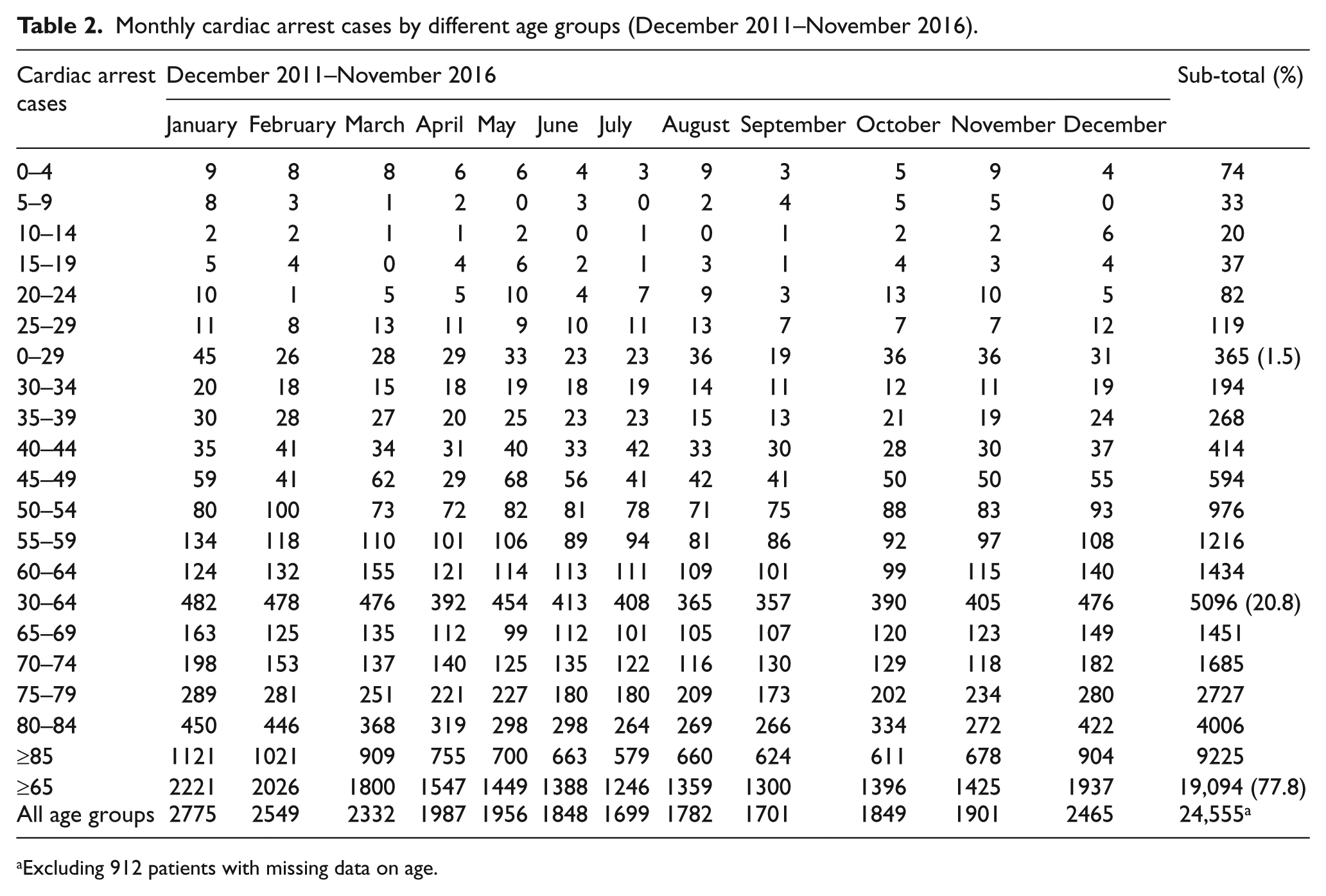
Excluding 912 patients with missing data on age.
The study also analysed the effects of temperature on cardiac arrest by age groups. Figure 3 shows the relationships between mean daily temperature and OHCA stratified by different age groups. Figure 3(a) reveals that the ≥65 years elderly age group compared with their younger counterparts was highly susceptible to OHCA with decreasing temperatures. The almost horizontal trend lines near the bottom of Figure 3(a) indicate that there were hardly linear relationships between temperature and cardiac arrest for the two younger age groups. Figure 3(b) shows a further breakdown of the ≥65 years elderly group into five age groups (65–69, 70–74, 75–79, 80–84 and ≥85 years) to examine effects of daily mean temperature on OHCA. The results clearly suggest the detrimental effects of cold temperatures on OHCA for people aged 85 years and above.
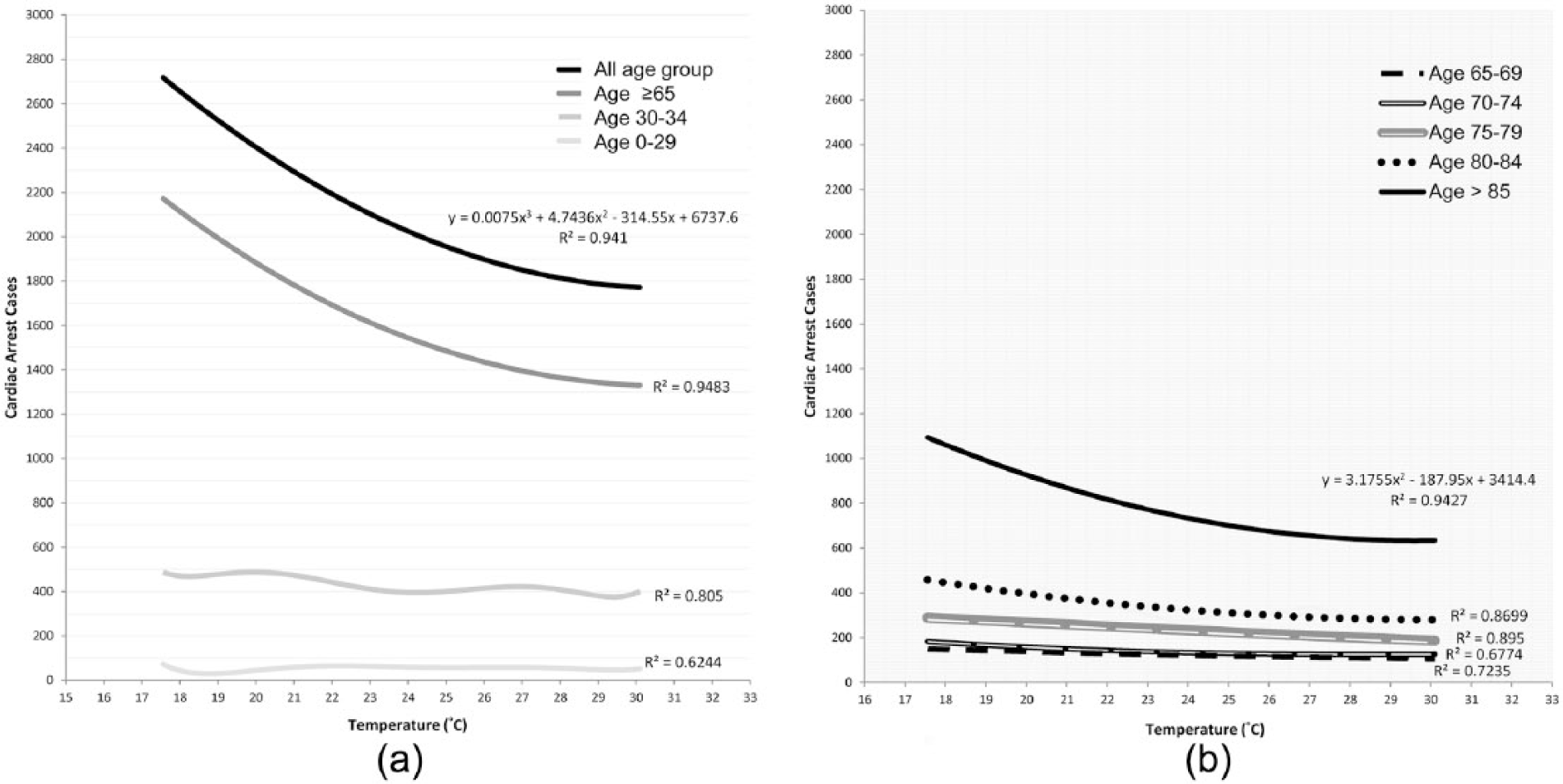
Relationships between daily mean temperature and OHCA cases stratified by age groups: (a) all age groups 0–29 years (n = 654), 30–64 years (n = 5096), ≥65 years (n = 19,094) and (b) finer breakdown of 65–69 years (n = 1685), 75–79 years (n = 2727), 80–84 years (n = 4006), ≥85 years (n = 9225).
Apart from age, gender is also an important and non-modifiable factor for OHCA. Figure 4 shows significant differences existed between men and women in OHCA (p < 0.05) where men (55.6%) were more likely than women (44.4%) to experience OHCA. The graphic plot also shows that monthly OHCA cases for men consistently outnumbered women by 8.6–16.3%. Precipitated by changing temperatures, OHCA cases for both genders had larger numbers in winter (December–February) as opposed to summer (June–August) months.
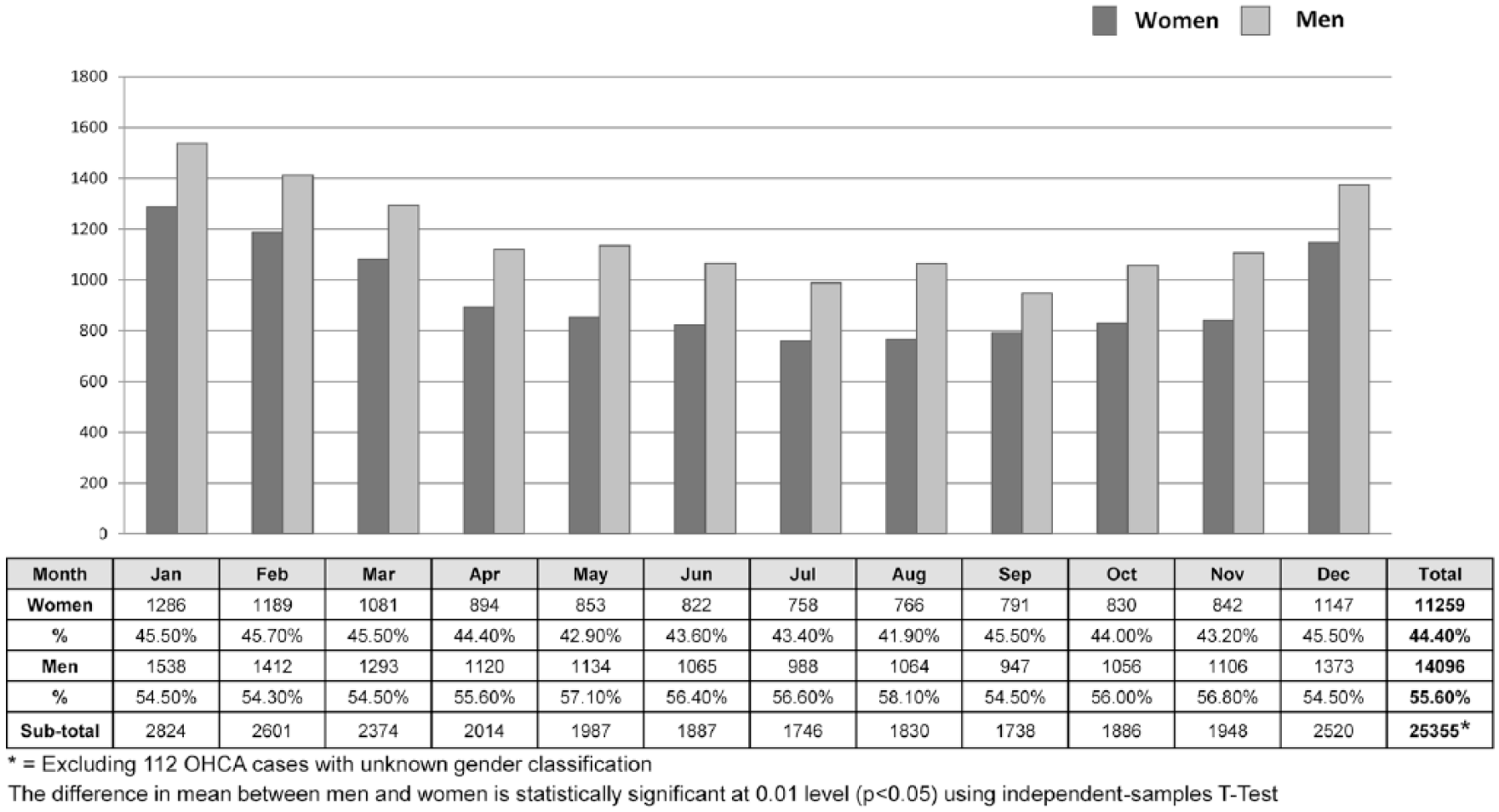
Monthly OHCA cases by gender groups (December 2011–November 2016).
Temporal patterns of OHCA
Figure 5 reveals discernible seasonal and temporal patterns of OHCA according to the EMS demands. The calendar chart (Figure 5(a)) shows a daily high incidence of OHCA at about 200–300 cases between 06:00 and 11:00. The high incidence period seemed consistent throughout the year with an exceptionally high incidence in January that peaked at 07:00 (Figure 5(b)). Figure 5(b) also shows that the incidence of OHCA was generally higher in cooler (November–March) than the other seasons. Conversely, a relatively low incidence of fewer than 100 cases was found between midnight and 03:00, especially from June to October. These daily and monthly profiles had been consistently demonstrated in the pre-hospital cardiac arrest demand over the 5 years of study period.
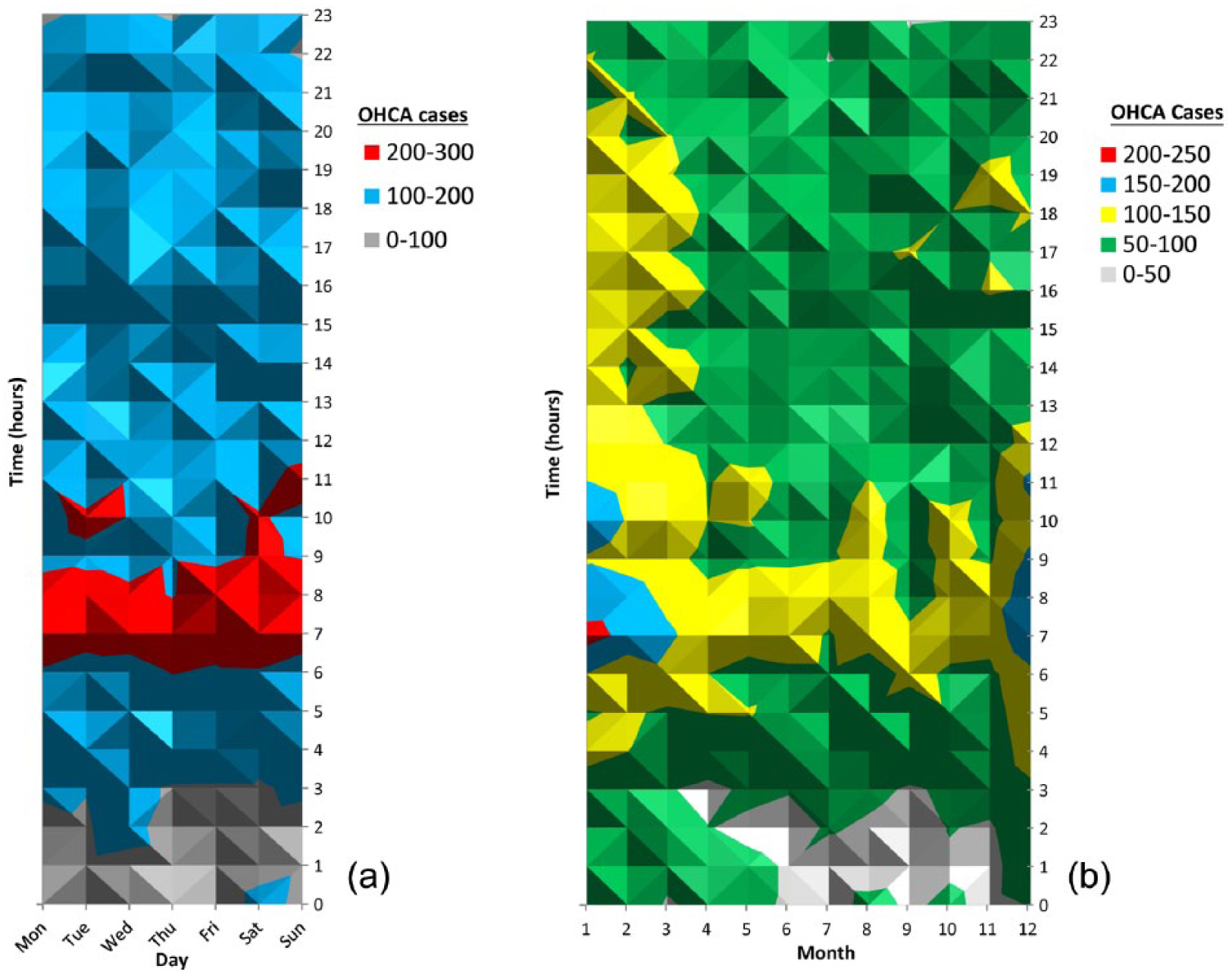
Temporal patterns of OHCA cases in Hong Kong (December 2011–November 2016): (a) total OHCA cases by day of week (December 2011–November 2016) and (b) total OHCA cases by month (December 2011–November 2016).
Discussion
This study is the first large-scale and representative account of OHCA and its demand for EMS in Hong Kong. It offers not only the much needed evidence about temperature and age–gender effects on OHCA occurrences but also temporal trends in cardiovascular demand in EMS. Similar to findings in the literature, this study confirms the negative effects of ambient temperatures on OHCA in Hong Kong. In particular, cold temperatures (see Table 1 and Figure 1) and large diurnal temperature variations (see Figure 2) are risk factors for cardiovascular incidents which exacerbate in older age groups (see Table 2 and Figure 2). This phenomenon can be attributed to the inability of older people to endure exposure to and sudden drops in cold temperatures, 22 while cold temperatures have been known to raise blood pressure in normotensive and hypertensive individuals.23–25 It is also possible that elderly people may have other chronic illnesses leading to OHCA although not substantiated in this study due to incomplete data on medical history. As the elderly population in Hong Kong expects to double from 15% in 2014 to 32% in 2041, 26 the HKFSD must cater for the expected increase in OHCA and its demand for EMS.
A recent study in Japan showed that the occurrence of OHCA is attributable not only to low temperatures but also to high temperatures. 27 The OHCA cases in Hong Kong also appeared to rise, albeit by only a small proportion, when the daily maximum temperatures reached 33°C and above (Figure 1). This observation suggests that cardiac arrest occurrences may be exacerbated by extreme high temperatures as much as low temperatures. As the number of very hot days (daily maximum temperature ≥33°C) in Hong Kong’s summer is likely to increase with climate change, 28 the number of OHCA cases expects to rise in the foreseeable future. This rising trend warrants attention and further exploration of the impacts of very hot weather on OHCA.
This study also finds that men were more likely than women to suffer OHCA, in which approximately three in five cases occurred in men (see Figure 4). The finding agrees with observations reported in the United States4,29,30 and consistent with results in past research.21,22 Accounting for temperature and age–gender effects on OHCA determined through this study, cardiovascular demand for EMS in the future would have been underestimated for elderly people especially in months of low temperature. Similar results have been established in a recent study on future emergency ambulance demand in Hong Kong. 31
The temporal breakdowns of OHCA-related demands for EMS (see Figure 5) reveal seasonal and daily variations that can help improve service preparedness and provision. For example, a surging demand for EMS involving cardiac arrests in the winter months and early morning hours suggests critical time/period for efficient allocation of ambulance resources, such as trained paramedics and advanced cardiovascular life support equipment. Optimal allocation of resources and effective preparedness strategies can improve survival from OHCA in which timeliness and quality of life-saving equipment and procedures can make a big difference.4,32 It is also important to take preventive measures during the winter months, such as opening more cold shelters and provision of warm clothing for vulnerable populations, including elderly and socially disadvantaged people, even when temperatures are moderately cold. Different people may have different adaptability and responses to changing temperature.
Future study shall focus on spatio-temporal analysis of OHCA to examine temporal patterns of service demands across the whole territory of Hong Kong. The spatio-temporal approach is necessary to identify hot spots or high-risk neighbourhoods for OHCA. 33 Integrating both spatial and temporal factors in the analysis of OHCA will provide more robust and reliable estimates for the strategic planning and delivery of future EMS.
Conclusion
This study initiated by the HKFSD represents an unprecedented local territory-wide study to investigate the impacts of ambient temperature and age–gender differences on the occurrence of cardiac arrests in pre-hospital settings of Hong Kong. The study helps inform management practices and suggest policy changes to improve EMS guided by research-based evidence. Identifying high-risk groups and temporal variation in service demand is a first step towards improving existing service provision.
Footnotes
Acknowledgements
The authors would like to thank the Hong Kong Fire Services Department and the Hong Kong Observatory for supplying necessary data to the study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.