
Abstract
Paramedic work is associated with high staff turn-over, insufficient sleep and adverse health outcomes. Our understanding of the relationship between paramedic work and the health behaviours that may precede adverse health outcomes is limited, as few longitudinal studies have examined health behaviours in workers before they commence on the road work. Such research is needed to inform evidence-based recommendations specifically for new paramedics. The current observational cohort study examined self-reported sleep, dietary intake and physical activity in 21 intern paramedics: 15 female and 6 male (median age: 23.0 years [interquartile range (IQR): 4.0]) from an Australian ambulance service. A subset of participants (n = 16) provided fasting blood samples for cardiometabolic markers (cholesterol, triglycerides and fasting glucose). Data were collected quarterly (pre-shift work, 3 months, 6 months, 9 months and 12 months post commencement). Linear mixed models showed that the first 12 months of shift work were associated with poorer sleep quality (p = .036), consumption of fewer kilojoules (p = .026), reduced saturated fat consumption (p = .005) and lower sodium (p = .043) and sugar (p = .038) intake. There were significant increases in leisure time physical activity (p = .008). This study shows negative changes in sleep quality and improvements in diet and leisure time physical activity during the first 12 months of paramedic work. Individual differences observed in this study, and ongoing suboptimal dietary intake, highlight a need for larger studies with more participants and a focus on personalised strategies for new recruit paramedics.
Introduction
Paramedics provide urgent out of hospital healthcare across the 24 h day. These essential healthcare workers are exposed to occupation hazards including excessive physical and psychological demands, workplace violence and shift work.1–3 Paramedics globally show a high prevalence of mental health conditions 4 and workplace injury. 5 How and when health behaviours and health status change following the transition to paramedic work is not currently well understood. 6 Therefore, a better understanding of the transition to professional paramedic practice, and any impacts on health behaviours and health status, is needed.
One important risk factor that contributes to health outcomes in healthcare workers is shift work. Working at times incongruent with the body's circadian rhythms is associated with an increased risk of metabolic disorders, cardiovascular disease, mental health conditions and some cancers.7–9 The transition to shift work is a particularly challenging period, with numerous studies showing negative impacts on sleep and mental health, but not necessarily overall perceived health. 10 Paramedics may also be at risk for transition shock. Transition shock describes the ‘shock’ that one may encounter when their expectations of healthcare employment are at odds with their experience upon commencing in a new role. Transition shock may include feelings of anxiety, instability and insufficiency, 11 which may have detrimental effects on mental health and health behaviours.
A modest number of longitudinal studies suggest an association between shift work and suboptimal health behaviours. 12 However, the majority of existing field studies of shift workers are cross-sectional, or lack a pre-shift work reference, which is required to assess health behaviour changes in response to shift work. Without some measurements prior to commencing shift work, our understanding of how shift work impacts health behaviours is largely unclear. 6 Existing longitudinal studies without pre-shift work data points may be impacted by the healthy worker effect, which theorises that those who are healthier are more likely to remain employed. 13 Consequently, these studies may be underestimating the magnitude of the impact shift work has on health behaviours.
New graduate paramedics in Australia who want to work for public ambulance services are employed for their first year as ‘intern paramedics’. The intern year is designed to allow new graduate paramedics to be supervised and supported as they gain experience on the job. These intern paramedics undergo pre-employment orientations (i.e., training before working shift work). This pre-employment training presents an ideal opportunity to work with new paramedics prior to their commencement of shift work in order to better understand the impacts of commencing paramedic work. Thus, working with paramedic intern cohorts provides the opportunity to identify the type and timing of strategies most needed for new paramedics. The present study therefore aimed to investigate health behaviour changes during the first 12 months of shift work and whether these changes differ by sex or age with intern paramedics.
Methods
Study design
The present study was an exploratory observational cohort study, as such the manuscript is reported in line with Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Cohort study guidelines 14 and a completed checklist can be found in the Supplementary material. The full protocol for this study has been published previously. 1
A longitudinal repeated measures design as chosen to allow for the assessment of changes in health indicators and behaviours follows commencement of paramedic shift work. Thus, participants were asked to complete quarterly assessments at five time points (1 = pre-shift work baseline; 2 = 3 months post-baseline; 3 = 6 months post-baseline; 4 = 9 months post-baseline; and 5 = 12 months post-baseline). All measurements described below were completed at each time point except for sex and date of birth. Additional measures were also completed as outlined in published protocol, 1 only those relevant to current analysis are described below.
Participants
As this was an exploratory study, no formal sample size was calculated. We intended to recruit 40 intern paramedics.
1
All commencing intern paramedics at one Australian ambulance service over the period November 2020 to February 2022 were invited to participate. At this service, intern paramedics undergo initial training on a standard day schedule which involves inducting into routine operational requirements including safety, communications, manual tasks and emergency vehicle driving. Intern paramedics were eligible to participate in the present study if they met the following criteria:
Were a new recruit to the intern paramedic program, Had completed tertiary paramedic training within the previous 2 years, Had not had paid employment with another ambulance agency for a total of 12 months or more, and Were willing and able to complete data collection every 3 months.
All participants provided information consent to participant. The project received approval from South Australian Health Research Ethics Committee (#19/SAH/34) and CQUniversity Human Research Ethics Committee (000002226).
Measurements
Demographics
Demographic details included biological sex (‘What sex were you assigned at birth?’), date of birth and additional measures from the Standard Shiftwork Index, 15 including relationship status, living arrangements, shift working arrangements (i.e., overtime, rosters and shift length), shift work experience and years of prior employment. Following baseline (daytime training), all participants commenced work on a fast forward rotating shift system (two-day shifts, two-night shifts and four days off).
Blood samples
Participants could provide a fasting blood sample at each time point but were not required to provide these samples to participate in the study. Participants were asked to provide this sample in the morning following an overnight fast. The measures of interest were fasting glucose (millimoles per litre (mmol/L)), total cholesterol (mmol/L), low-density lipoprotein (mmol/L), high-density lipoprotein (mmol/L) and triglycerides (mmol/L).
Sleep
Sleep was assessed using the Pittsburgh Sleep Quality Index (PSQI). 16 The PSQI has demonstrated acceptable re-retest reliability and scale validity 16 and has been shown to be valid in samples of shift workers. 17 Additionally, the cut off of >5 yields a sensitivity of 89.6% in detecting poor sleep. 16 Average sleep duration was calculated from PSQI Question four ‘During the past month, how many hours of actual sleep did you get at night?’. Sleep component and global scores were calculated in line with the original scoring recommendations to provide an overall PSQI score for each timepoint, indicative of overall sleep quality. Cronbach's alpha is used as a measure of internal consistency of a scale, 18 with a commonly accepted cut off of >0.70 as acceptable internal consistency and values closer to 1.0 indicating higher level of internal consistency. 19 Cronbach's alpha for PSQI in the current sample ranged between 0.70 and 0.77 between timepoints (see Supplementary material).
Dietary intake
Dietary intake was assessed with the Automated Self-Administered 24-hour Dietary Assessment Tool (ASA24) food diary, 20 completed via phone interview with a trained researcher. The ASA24 is based on the United States Department for Agriculture's Automated Multiple-Pass Method which has been shown be valid and reliable20,21 and has been used in other studies of shift workers. 22 Where a participant reported a food that was not included in the existing ASA24 database, the researcher made note of the food and manually added the nutritional values during data extraction. The dietary variables chosen for the current analyses were kilojoules, caffeine, sodium, saturated fat and sugar and were chosen due to known associations with chronic disease risk. 23 For ease of data collection, food recalls were conducted at a time chosen by participants and thus could be provided across any point of the shift cycle or days off. Cronbach's alpha for ASA24 in the current sample ranged between 0.68 and 0.75 between timepoints (see Supplementary material).
Physical activity
Physical activity was assessed with the International Physical Activity Questionnaire – Long Form (IPAQ). 24 The IPAQ has been validated against accelerometer data and is also considered comparable to telephone administered physical activity report. 24 The IPAQ has previously been used in other studies of shift workers. 25 Data are quantified as metabolic equivalent of tasks (METs), with one MET approximately equivalent to 3.5 ml of oxygen per kg body weight per minute when sitting quietly. 26 In line with IPAQ guidelines, 24 walking was calculated to be 3.3 METs, moderate physical activity to be 4 METs and vigorous physical activity 8 METs. Total minutes per week were calculated, truncated if necessary (i.e., values over 4 hours per activity per day were truncated at 240 minutes) and multiplied by the relevant MET category, as in published guidelines. 24 Cronbach's alpha for IPAQ (without sedentary items as in previous studies 27 ) in the current sample ranged between 0.72 and 0.81 between timepoints (see Supplementary material).
Bias
To limit potential attrition bias, all participants were sent multiple reminders via REDCap and text messages to enhance response rates. To limit potential selection bias, all commencing intern paramedics at one Australian ambulance service during the recruitment period were invited to participate, if they were eligible. Additionally, analysis of those who completed the study vs those who did not was conducted to test for any confounding bias due to attrition.
Data analysis
Data were analysed utilising R 3.6.2 and R studio.28,29 Participants were categorised according to their participation in the study as (a) completed: with engagement from baseline through to the 12-month assessment, and (b) lost to follow-up: completed the consent form and subsequently formally withdrew or were non-responsive. Differences in baseline characteristics (i.e., demographics and behavioural measures) between completed and lost to follow-up participants were calculated with the Kruskal-Wallis test, or t-test using ‘psych’ package 30 depending on distribution of data. Distributions of data were assessed visually using histograms and via Shapiro-Wilks test.
To consider relationships between health behaviours, correlations between all health behaviours at each time point and across time points were examined. Due to the non-normal distributions of many variables, the Spearman rank correlation coefficient was used and correlations are presented as rho (ρ). Linear mixed models were chosen for examination of behavioural change over time due to superiority over traditional analysis of variance when analysing samples of multilevel data and for repeated measures designs and consideration of individual variations. 31 Additionally, linear mixed models can accommodate missing data when participants were missing data at one or more timepoints. Utilising the ‘lme4’ and ‘lmertest’,32,33 longitudinal changes in health behaviours were assessed via separately constructed models: specifically, with the behavioural health outcome (e.g., sleep duration) as dependent variable and fixed effects of time, sex (male, female) and age. A random intercept of participant ID was included and an interaction term between time and sex was also included. Models were based on an unstructured covariance structure due to the potential for correlation between random effects. The two-tailed significance level was set at α = .05 and was assessed using analysis of variance with Satterthwaite's method. Behavioural outcomes were compared to existing guidelines from Australia wherever possible, but sought from other jurisdictions where Australian guidelines did not provide specific recommendations (Supplementary material).
Results
Participants
A total of 53 intern paramedics provided initial informed consent. Of these, 46 participants engaged in at least one aspect of baseline assessment (i.e., provided some data), and 30 provided a full baseline assessment (i.e., completed online survey and phone interview). Of the 30 who provided a full baseline assessment, 21 participants provided data (at least three data points) across the first year of employment encompassing five data collection points (70% of those who completed baseline; attrition rate 30%). A comparison of baseline characteristics of those who completed the study (n = 21) and those who were lost to follow-up (n = 25) is presented in Table 1. Table 2 provides an overview of aggregated data for participant health behaviours at each time point, and frequency of meeting recommended behavioural guidelines is provided in the Supplementary material. Reasons for withdrawal or missed data point cited included ‘leaving job’, ‘too busy’ or ‘data collection to intense’.
Comparison of baseline characteristics of intern paramedics who completed and those lost to follow-up.
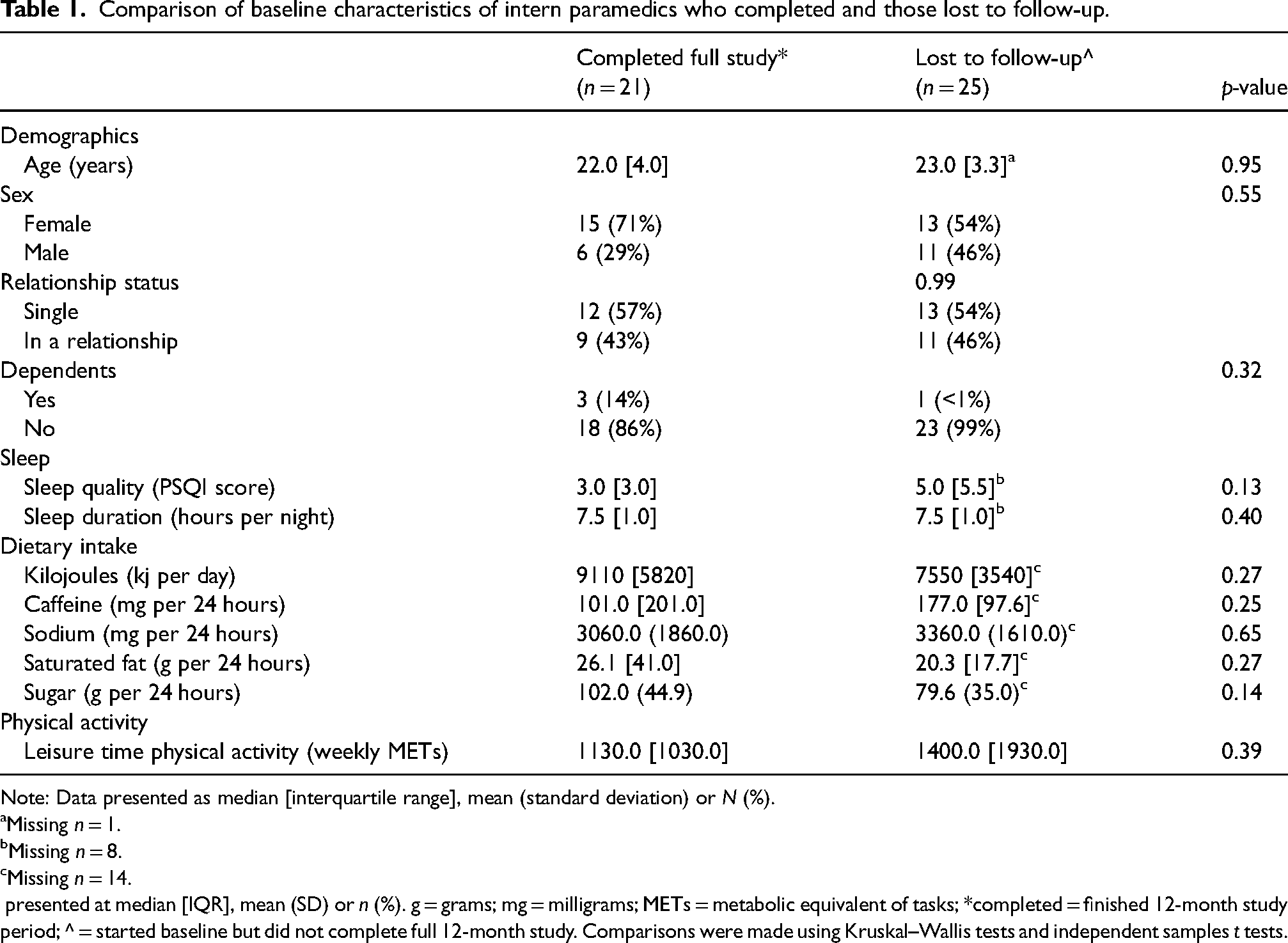
Note: Data presented as median [interquartile range], mean (standard deviation) or N (%).
aMissing n = 1.
bMissing n = 8.
cMissing n = 14.
presented at median [IQR], mean (SD) or n (%). g = grams; mg = milligrams; METs = metabolic equivalent of tasks; *completed = finished 12-month study period; ^ = started baseline but did not complete full 12-month study. Comparisons were made using Kruskal–Wallis tests and independent samples t tests.
Behavioral outcomes and fasting blood biomarkers (subsample) for intern paramedics separated by time point and by sex.
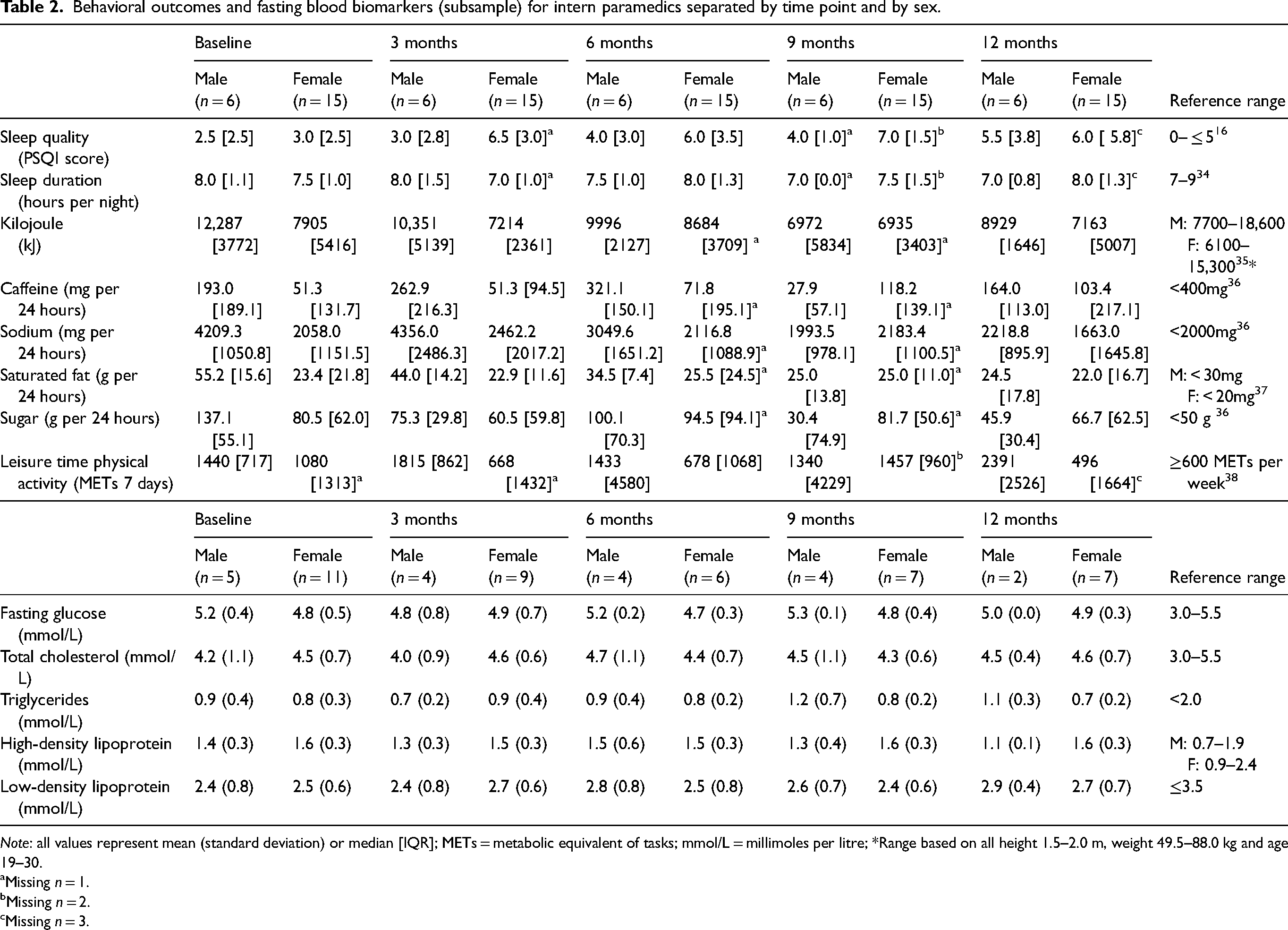
Note: all values represent mean (standard deviation) or median [IQR]; METs = metabolic equivalent of tasks; mmol/L = millimoles per litre; *Range based on all height 1.5–2.0 m, weight 49.5–88.0 kg and age 19–30.
aMissing n = 1.
bMissing n = 2.
Missing n = 3.
Blood samples
A total of 16 participants in the present sample provided blood at baseline, and between 9 and 13 provided a fasting sample at subsequent time points.
Associations between health behaviours
Relationships between different health behaviours both concurrently, and between timepoints, are shown in the Supplementary material.
Sleep and physical activity
Poorer sleep quality (i.e., higher PSQI score) at T1 was associated with less physical activity at T2 (ρ = −.47), and poorer sleep quality at T2 was associated with significantly lower physical activity at T3 (ρ = −.53). Poorer sleep quality was also concurrently associated with lower levels of physical activity at T3 (ρ = .59). Conversely, longer sleep duration at T2 was associated with higher levels of physical activity at T3 (ρ = .59).
Diet and physical activity
Higher kilojoule intake at T1 was significantly associated with higher levels of physical activity at T2 (ρ = .62). Similarly, higher kilojoule intake at T2 was associated with significantly higher levels of physical activity at T3 (ρ = .76). Higher kilojoule intake at T2 was also concurrently associated with higher level of physical activity (ρ = .73). Higher levels of sodium intake at T1 were associated with more physical activity at T2 (ρ = .47); this was also true for sodium intake at T2 and physical activity at T3 (ρ = .56). Higher saturated fat intake at T1 was associated with more physical activity at T2 (ρ = .66); this was also true for saturated fat intake at T2 and physical activity at T3 (ρ = .57). Saturated fat intake was also associated with more physical activity at T2 (r = .59). Higher sugar intake at T2 was associated with higher levels of physical activity at T3 (ρ = .53).
Diet and sleep
Higher overall kilojoule intake at T4 was associated with shorter sleep duration at T5 (ρ = −.50). Higher levels of sodium intake at T4 were associated with shorter sleep duration at T4 (ρ = −.53) and at T5 (ρ = −.48). Additionally, higher saturated fat intake at T4 was associated with shorter sleep duration at T4 (ρ = −.52).
Sleep quality and duration
Individual variability both in sleep quality and sleep duration at baseline, and in response to commencing paramedic work, was considerable (see Figure 1A). There was a significant main effect of time (p = .036) and sex (p = .022) on subjective sleep quality (Table 3), reflecting an overall increase in poor sleep quality score (higher PSQI score, Table 2) during the first 12 months of paramedic work. This increase was greater, reflecting poorer sleep, among females. There were no significant main effects of time (p = .19) or age (p = .07) on self-reported sleep duration during the first 12 months of paramedic work (Table 2 and Figure 1B). There was, however, a significant interaction between sex and time (p = .010), indicating that female participants were more likely to report an increase in sleep duration over the intern year (Table 2).
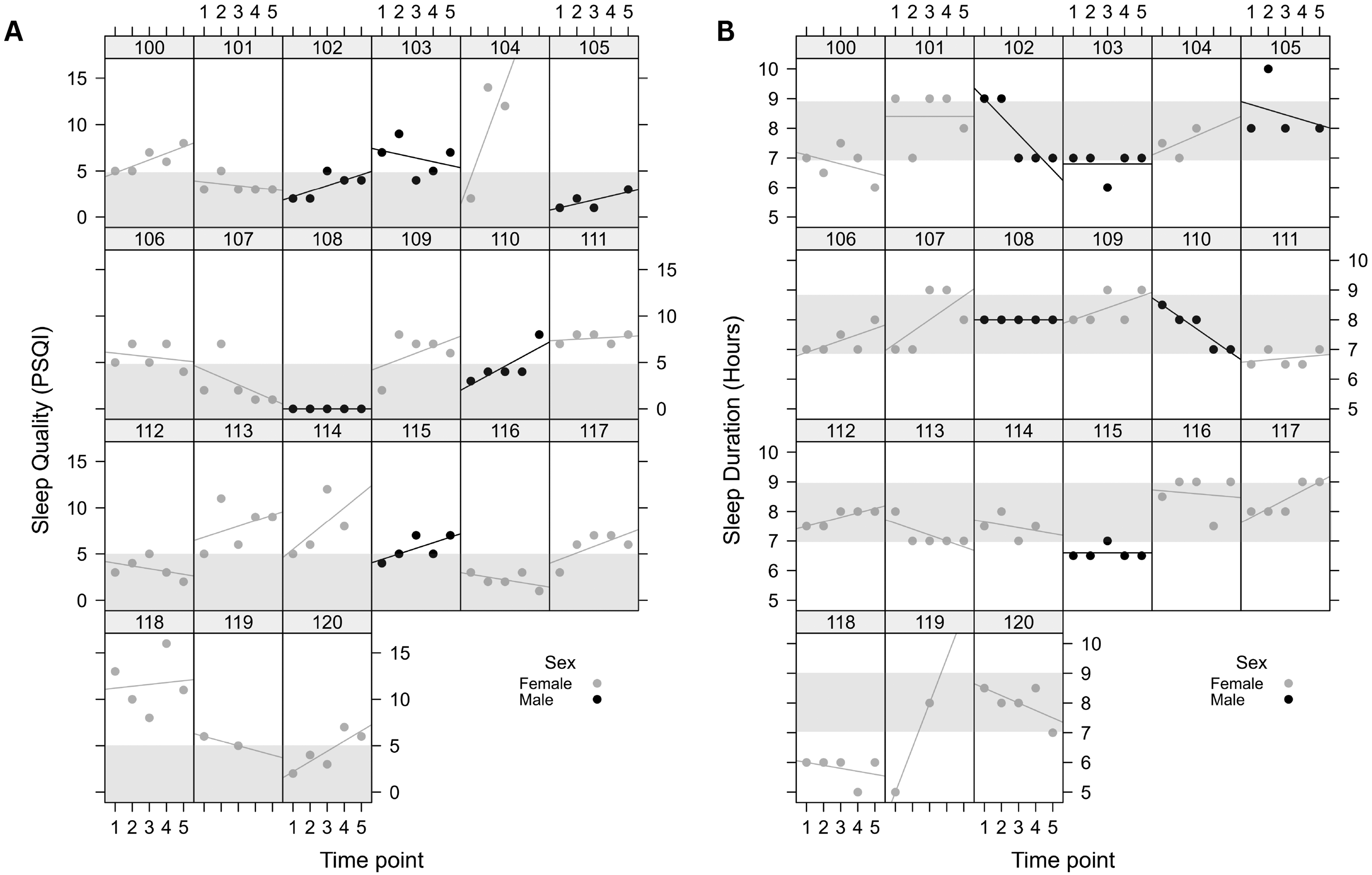
(A): Dot plot depicting sleep quality (PSQI) throughout the 12-month study period. Each box represents an individual participant, dots represent individual data point, X-axis represents five time points (T1, pre-shift work; T2, 3 months; T3, 6 months; T4, 9 months; and T5, 12 months) and Y-axis is the PSQI score. Shaded box denotes the optimal sleep quality recommended by PSQI. (B): Dot plot depicting sleep duration (hours) throughout the 12-month study period. Each box represents an individual participant, dots represent individual data point, X-axis represents five time points (T1, pre-shift work; T2, 3 months; T3, 6 months; T4, 9 months; and T5, 12 months) and Y-axis represents sleep duration. Shaded box denotes the optimal sleep duration for young-middle age adult.
Linear mixed models showing health behaviours by time, sex and age.
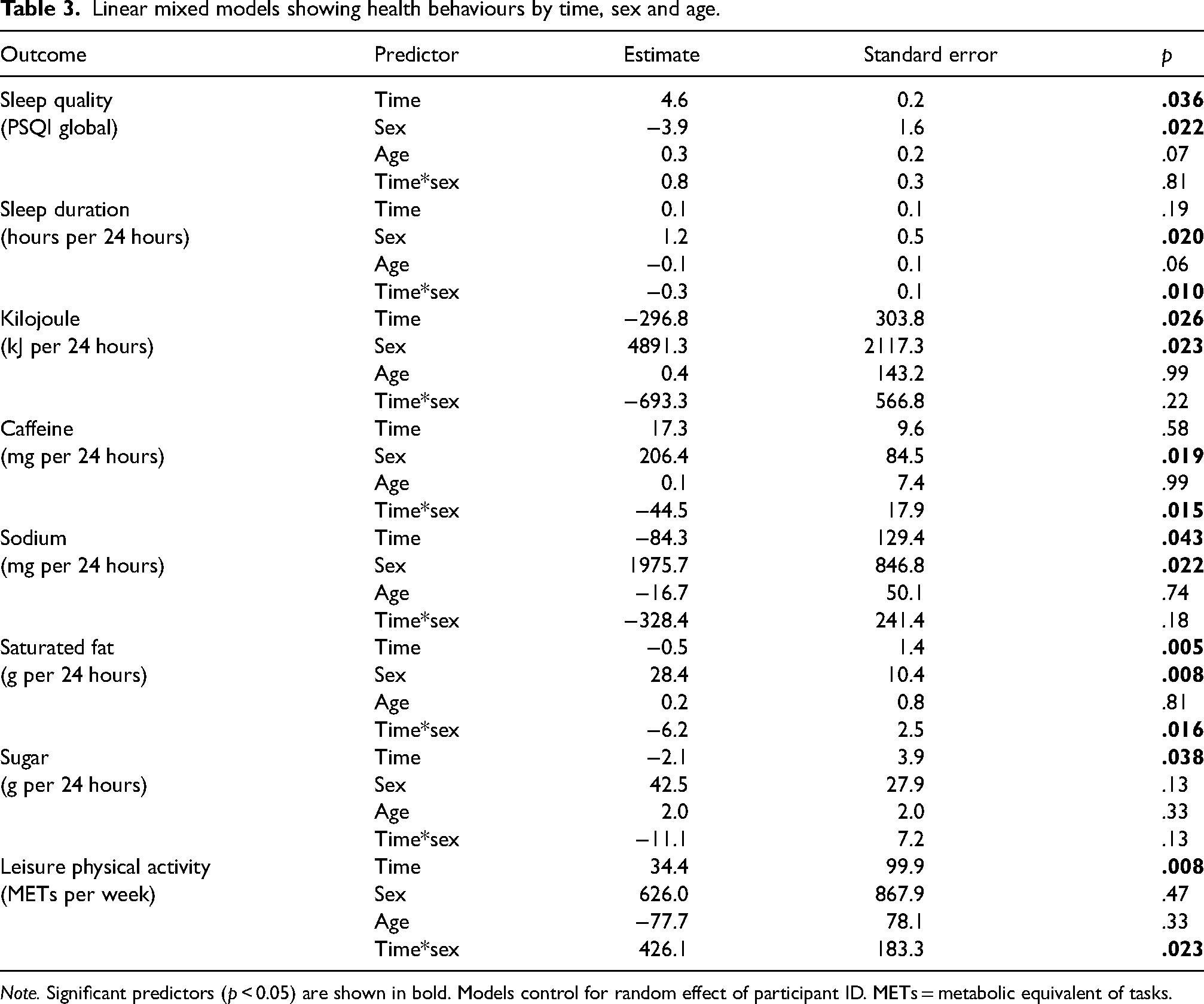
Note. Significant predictors (p < 0.05) are shown in bold. Models control for random effect of participant ID. METs = metabolic equivalent of tasks.
Dietary intake
As shown in Figure 2A, the first 12 months of paramedic work were associated with a significant decrease in kilojoule intake (p = .026), which was more pronounced in females (p = .023), but did not differ by age (p = .99) in intern paramedics (Tables 2 and 3). There was no significant main effect of time (p = .58) or age (p = .99) on caffeine intake during the first 12 months of paramedic work (Table 2 and Figure 2B). There was a significant interaction between time and sex for caffeine intake (p = .015), reflecting an increase in caffeine intake in females and a decrease of caffeine intake in males over time.
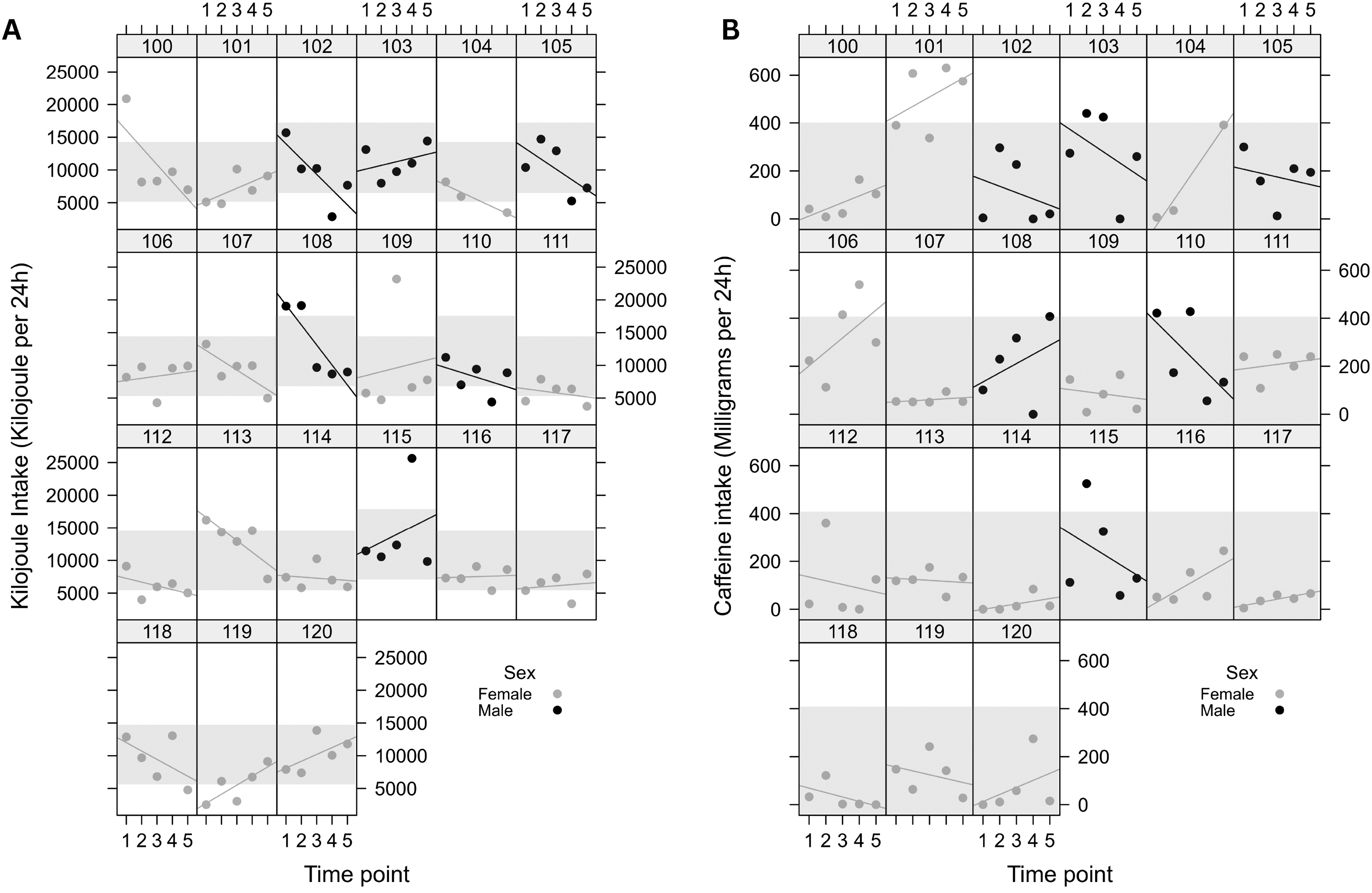
(A): Dot plot depicting the 24-hour kilojoule intake throughout the 12-month study period. Each box represents an individual participant, dots represent individual data point, X-axis represents five time points (T1, pre-shift work; T2, 3 months; T3, 6 months; T4, 9 months; and T5, 12 months) and Y-axis represents the 24-hour kilojoule intake. Shaded box representations the optimal kilojoule intake based on Australian guidelines. (B): Dot plot depicting the 24-hour caffeine intake throughout the 12-month study period. Each box represents an individual participant, dots represent individual data point, X-axis represents five time points and Y-axis represents the 24-hour caffeine intake. Shaded box represents the recommended caffeine intake.
The first 12 months of paramedic work were associated with a significant decrease in saturated fat intake (p = .005) that did not differ by age (Table 3). There was a significant interaction between time and sex for saturated fat intake (p = .016) reflecting lower saturated fat intake over time in males (Figure 3A). As shown in Table 3, and visually in Figure 3B, significant main effects of time (p = .043) and sex (p = .022) but not age (p = .74) on sodium intake were found, reflecting a significant decrease in sodium intake during the first 12 months of paramedic work, which was more pronounced among male intern paramedics.
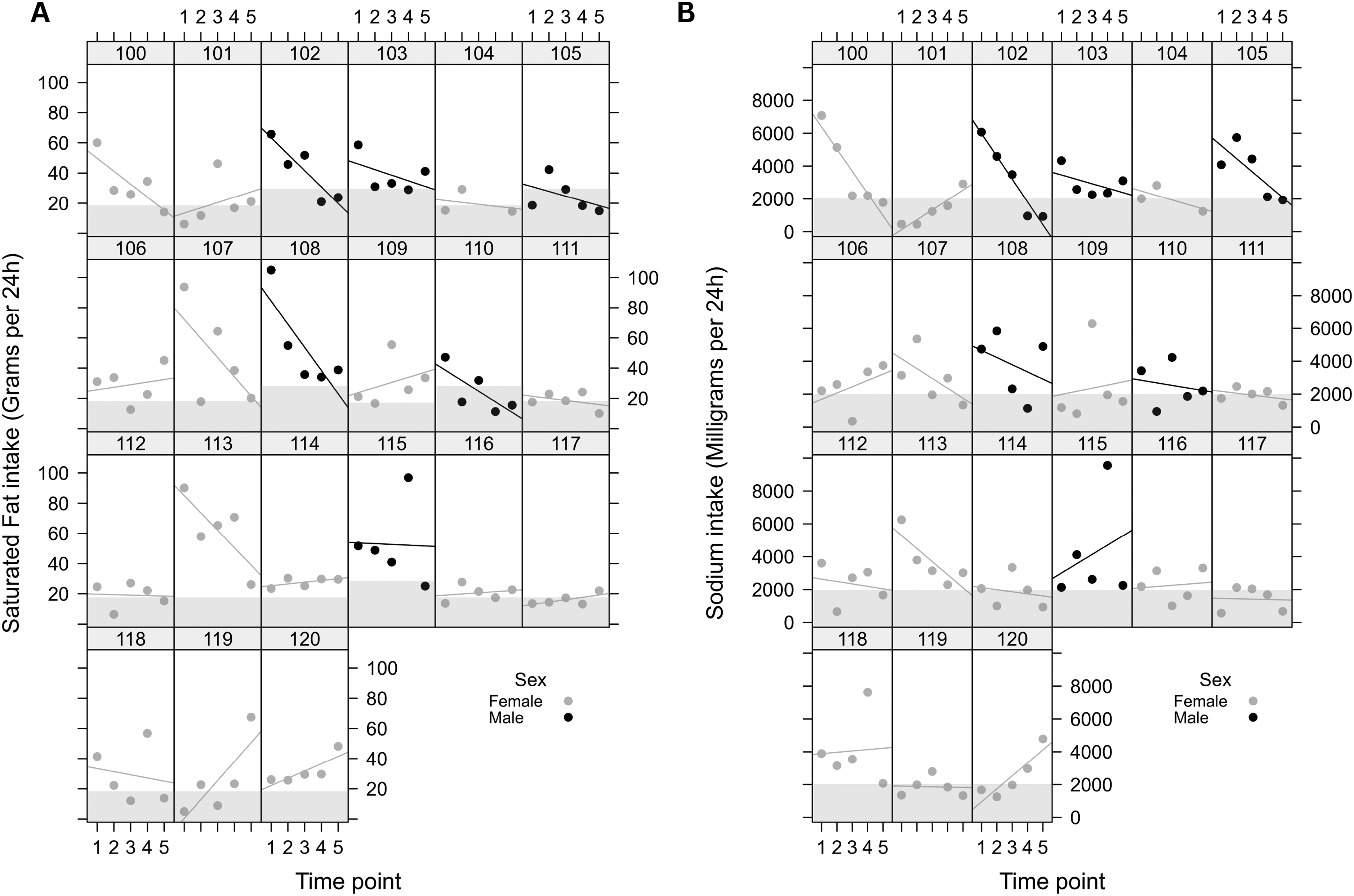
(A): Dot plot depicting the 24-hour saturated fat throughout the 12-month study period. Each box represents an individual participant, dots represent individual data point, x-axis represents five time points and y-axis represents the 24-hour saturated fat intake. Shaded box represents the recommend daily saturated fat intake. (B): Dot plot depicting the 24-hour sodium intake throughout the 12-month study period. Each box represents an individual participant, dots represent individual data point, X-axis represents five time points and Y-axis represents sodium intake. Shaded box represents the recommended daily caffeine intake.
As shown in Table 3, and visually presented in Figure 4A, there was a significant main effect of time (p = .038) but not sex (p = .13) or age (p = .33) on sugar intake, reflecting a significant decrease in sugar intake across the 12 months of paramedic internship, irrespective of age or sex.
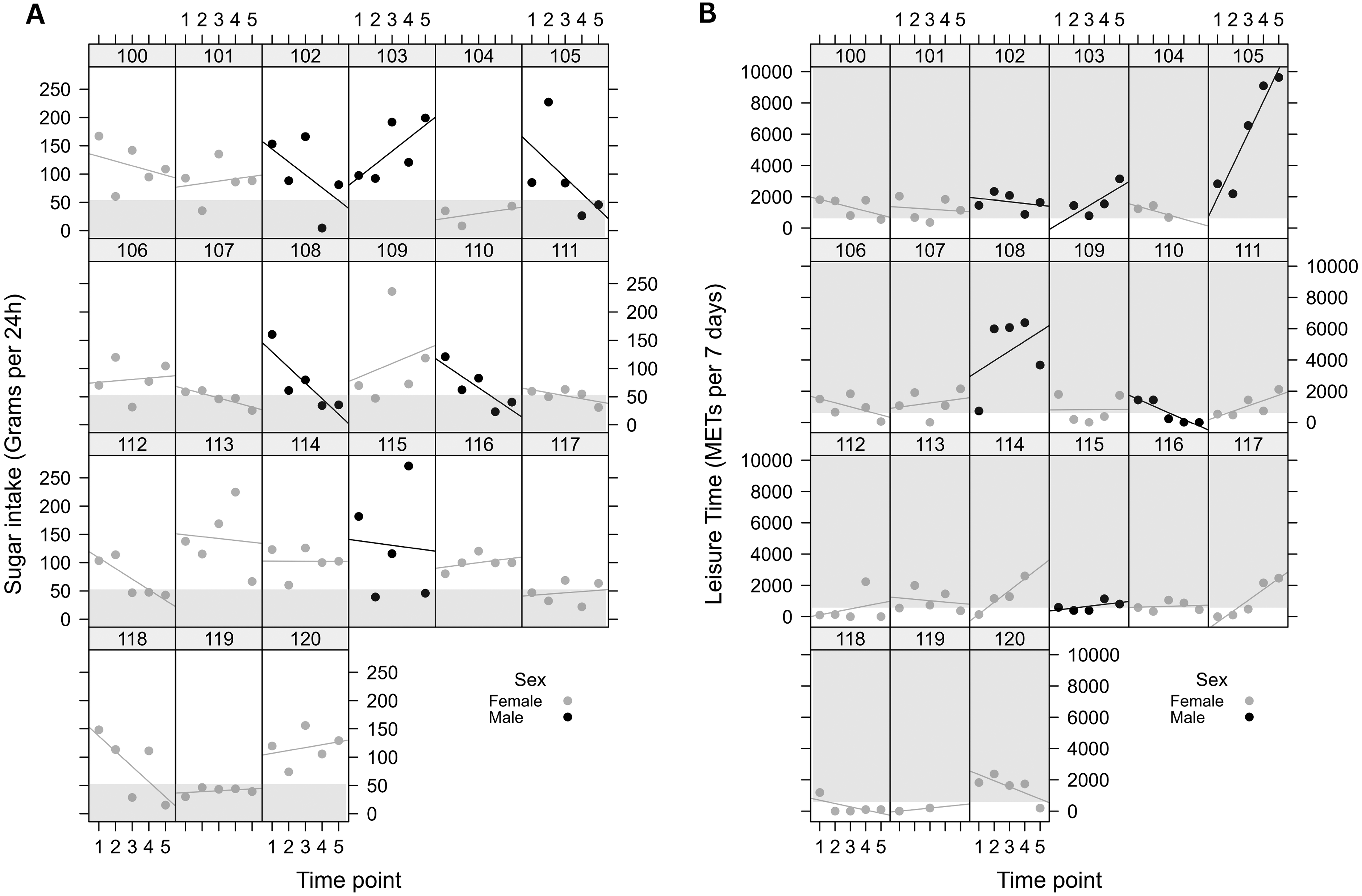
(A): Dot plot depicting the 24-hour sugar intake throughout the 12-month study period. Each box represents an individual participant, dots represent individual data point, X-axis represents five time points and Y-axis represents the 24-hour sugar intake. Shaded box represents the suggested daily sugar intake. (B): Dot plot depicting the seven-day leisure physical activity throughout the 12-month study period. Each box represents an individual participant, dots represent individual data point, X-axis represents five time points and Y-axis represents the seven-day leisure time METs. Shaded box denotes suggested the optimal leisure time physical activity.
Physical activity
There was a significant main effect for time (p = .008) but not for sex (p = .47) or age (p = .33) on leisure time physical activity during the 12 months of paramedic internship (Table 3). There was a significant interaction between sex and time, indicating that the increase in leisure time physical activity was more pronounced in male intern paramedics (Figure 4B).
Discussion
Our study showed that the first 12 months of intern paramedic employment was associated with decreased sleep quality and changes in both physical activity and dietary intake. Commencing paramedic internship was associated with pronounced between-person variations in health behaviours. These individual differences are critical for developing useful intervention strategies, as existing literature has historically focussed on aggregated group data, limiting our understanding of these nuanced between-person differences. 39 The between-person differences are informative for the development of support strategies and demonstrate the importance of considering interindividual responses to onset of shift work. Together, these findings highlight the need for considering personalised support strategies and interventions for new shift workers.
In our modest sample, female sex was associated with poorer sleep quality across the intern year, while male shift workers were more likely to decrease kilojoule and sodium intake and increase physical activity, consistent with the existing literature on shift workers. 40 The majority of the intern paramedics reported good sleep quality and sufficient sleep duration before commencing paramedic work. Intern paramedics reported a significant decline in sleep quality, but not sleep duration, during the first 12 months of paramedic work. Those with poorer sleep quality or shorter sleep duration at baseline reported more prominent negative impacts on sleep (i.e., inadequate sleep after shift work onset) compared to those with adequate sleep at baseline (i.e., these intern paramedics maintained similar sleep to baseline levels). Broadly, our self-report findings are in line with previous literature including actigraphic measures of sleep, where intern paramedics showed increased insomnia symptoms (self-report) but also an increase in total sleep duration (actigraphy) during the first 6 months of shift work. 41 Likewise, another study of intern paramedics showed that total sleep duration (actigraphy) did not change with shift work, but there was a significant increase in poorer sleep quality. 42 This developing body of literature suggests that paramedics may be able to obtain similar to baseline levels of sleep duration, but may feel their sleep is not as restorative or restful.
Our study demonstrates that some health behaviours declined when commencing shift work, which was most apparent at the 6-month follow-up where we saw an increase in poor sleep quality, kilojoule, caffeine, sodium, saturated fat and sugar intake, as well as lower levels of physical activity. The suboptimal health behaviours observed at 6 months of paramedic work are suggestive of transition shock. 43 Transition shock, while largely being explored with mental health symptoms, has been described by new British paramedics 44 and is likely relevant to our current sample. Following the 6-month assessment, many paramedics showed improvements in dietary intake and an increase in physical activity. Graduate nurses have described using health behaviours (e.g., getting good sleep and drinking milk) to overcome transition shock. 45 One potential interpretation is that intern paramedics may have used modifications in their own health behaviours (i.e., the observed increase in physical activity) to cope with transition shock.
High levels of sugar, saturated fat and sodium intake in combination suggest a potential role for interventions related to dietary behaviour, although it is important to note that findings from such interventions are mixed in the current literature. Evaluations of interventions in other occupations such as manufacturing workers, pilots and firefighters have demonstrated efficacy. 46 However, the success of occupational interventions with dietary interventions in healthcare appears less effective. 47 Health behaviour promotion is complex and multifaceted, 48 and interventions for paramedics will need to consider specific occupational challenges such as unpredictable meal times and long periods away from kitchen facilities, insufficient rest breaks and opportunities to eat meals, as well as fatigue. 6 Furthermore, as shown in our findings, there is significant between-person variability in health behaviours in intern paramedics, and these between-person differences must be considered when developing interventions with this group of shift workers.
During the first 12 months of paramedic work, intern paramedics reported an overall increase in leisure time physical activity. However, despite an overall increase in physical activity and median physical activity for males and females being above minimum guidelines (>600 METs per week, Table 2), 38 40%, 35%, 43%, 16% and 45% of the intern paramedics in our sample did not meet the weekly leisure time physical activity guidelines at baseline, 3 months, 6 months, 9 months and 12 months, respectively (Supplementary material). These findings are consistent with the working aged general Australian population, where three out of four people do not meet weekly activity guidelines. 49 It is also important to note that at most time points, almost half of the sample did meet the activity guidelines. For those who did not meet the activity guidelines, it is possible that the low levels of physical activity are due to barriers to leisure time physical activity, rather than lack of motivation to exercise, as reported by experienced paramedics. 50
The findings from our exploratory study highlight a need for greater consideration of perceived sleep and objective measures of sleep duration at an individual level to better understand the impacts of shift work onset on sleep. Additionally, the self-report measures of health behaviours in the present sample highlight the need for tools and data collection approaches better suited to examining health behaviours of shift workers. For example, the current study utilised the ASA24 food diary system, a validated tool for dietary intake. 51 However, the dietary data reported in the current study are specific to a 24-hour period convenient for the intern to complete their interview, and thus differences in intake between shifts were not recorded. Future studies may consider collecting dietary data on each shift type and days off, recognising that this approach does add additional burden to participants. Additionally, novel, low burden ways to collect sleep, dietary intake and physical activity data in shift workers are needed. Given the significant between-person variability seen in the adaption to paramedic shift work, it is crucial that future work with paramedics takes account of the unique occupational challenges, and an individual's characteristics (e.g., sex, age and baseline health behaviours), when developing and providing support strategies. There is a clear need for support strategies in this workforce,6,52 and our findings, while from a modest sample, highlight a need for these strategies to consider the individual, rather than targeting group-based interventions.
Limitations
The findings from the current study must be considered in light of some limitations. Foremost, while the intended recruitment target was reached, the final sample size of completed participants is modest, limiting statistical power and generalisability. The attrition rate of 30% was consistent with other longitudinal shift work studies, which report attrition rates between 30% and 35%.53–55 It is possible that the low baseline completion and the high attrition rate in the current study were in part due to the impacts of COVID-19 on the new intern paramedics. The majority of intern paramedics recruited for this study were required to train and work at a time of high operational pressure during the pandemic, which added strain to an already demanding occupation.
The present study was conducted in a small sample from a single ambulance service in one state of Australia, as such similar results may not be observed in a like-sample in other ambulance services. Future studies should aim to investigate health behaviours in a larger sample and across multiple ambulance services, to better generalise findings.
Additionally, the current analysis is limited by largely self-report behavioural measures. Self-report measures may be susceptible to reporting bias, and thus, future studies should consider whether more objective behavioural measures can be utilised within this population.
A further limitation of the present study is the absence of objective body mass index (BMI) data over time. The study had intended to collect anthropometric data during a face-to-face baseline visit, which was not possible due to COVID-19 related project changes. Self-report BMI was collected, but was not available for all participants at all timepoints and consequently was not included in the present analysis. Further, we did not conduct assessments of cardiovascular fitness due to an already extensive protocol which included blood and stool samples.
Conclusion
In a modest sample of intern paramedics, the first 12 months of paramedic work were associated with substantial interindividual differences in health behaviours over time. Overall, a decline in sleep quality, with an increase in physical activity, was apparent in the cohort. Additionally, there were some potentially beneficial changes to diet, although the overall reduction in kilojoules over time suggests these findings must be interpreted with caution. There were substantial interindividual differences in response to onset of paramedic work, suggesting a need for individualised support strategies during commencement of paramedic work. Future intervention studies should move beyond group-based interventions to support positive health behaviours in paramedic populations in order to support health behaviours and improve health outcomes in the medium to long term.
Supplemental Material
sj-docx-1-pam-10.1177_27536386241288304 - Supplemental material for Sleep, dietary intake and physical activity changes with onset of shift work in intern paramedics
Supplemental material, sj-docx-1-pam-10.1177_27536386241288304 for Sleep, dietary intake and physical activity changes with onset of shift work in intern paramedics by Meagan E. Crowther, Sally A. Ferguson, Robert J. Adams and Amy C. Reynolds in Paramedicine
Footnotes
Acknowledgements
The authors wish to acknowledge members of the research team who contributed to development of research questions included in this study, including Mr Chris Howie (South Australian Ambulance Service), Professor Keith Townsend and Dr Rebecca Loudoun (Griffith University), Associate Professor Jessica Paterson (Flinders University) and Dr Kaja Kovac (Central Queensland University).
Authors’ statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper. All authors have met the requirements for authorship.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The current project was funded by grants awarded to Amy Reynolds from the Australasian Sleep Association and Central Queensland University. First Author, Meagan E Crowther, was supported by a Research Training Program Scholarship.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.