
Abstract
Objective
This study aims to investigate the experiences of individuals involved in implementing and delivering community paramedicine programmes across several different regions internationally, in order to identify key themes that can inform ongoing development and introduction of community paramedicine programmes.
Methods
In this study, participants were enlisted through convenience sampling and a snowballing method. They responded to a custom survey emphasising open-ended responses. We employed a qualitative reflexive thematic analysis, utilising an inductive coding technique at the semantic/explicit level. This approach allowed us to discern themes from the participants’ accounts of the programme's implementation and delivery, along with their perceptions of its strengths and challenges.
Results
Data was collected from 29 participants engaged in the development or delivery of community paramedicine programmes spanning seven countries. Five themes were created: (1) community drives the need, which emphasises the importance of community engagement and flexible response to health needs; (2) working with others, which underscores the necessity of collaboration with stakeholders for integration and relationship maintenance; (3) promotion and communication, focusing on clarifying roles and countering misconceptions; (4) recruitment and support of community paramedics, highlighting the significance of experienced paramedic recruitment and providing support for staff retention; and (5) research and evaluation, stressing the importance of data sharing for patient care and programme evaluation. These themes demonstrate the significance of community-centred approaches, interprofessional practice, and programme evaluation in community paramedicine.
Conclusion
This study highlights the significance of community-centred approaches, interprofessional practice, and programme evaluation in community paramedicine. These findings can inform policymakers and practitioners in the development and implementation of community paramedicine programmes, ultimately improving the health and well-being of communities across different regions internationally.
Introduction
Community paramedicine is a novel model of care in which paramedics provide person-centred primary health care, health promotion, disease management, clinical assessment, and needs-based interventions to serve a broader set of healthcare needs. 1 Within the United Kingdom, paramedics were provided with extended skills to treat more patients in the community from 2002. 2 This has since led to the expansion of the paramedic role outside of emergency ambulance services, with paramedics now also working more broadly as part of multidisciplinary care teams and within primary care clinics. 3 Over the same time, similar community paramedicine models of care initiatives were established in Canada, 4 Australia, 5 and the United States of America. 6 Now, community paramedicine programmes are widely implemented across different healthcare systems in Australia, New Zealand, Canada, Finland, the UK, and the USA. 7
The adoption of the community paramedicine care model is primarily spurred by shifts in paramedic service workloads, which echo the rise in ageing demographics and decreasing availability of alternative health services. 7 Owing to escalating pressures, such as aging populations, the rise of chronic diseases, health inequities, and resource limitations, healthcare systems worldwide are experiencing a shift towards a more fragmented approach to care. This fragmentation often manifests as a lack of coordination and integration in a patient's healthcare journey, resulting in potential gaps in care, missed opportunities for early intervention, and suboptimal health outcomes. 8 Community paramedicine developments have provided an opportunity for paramedics to be more widely employed across the health system in ‘non-traditional’ roles such as community paramedic programme roles. Community paramedicine programmes are models of care which may use paramedics to provide various approaches, including community assessment and referral, paramedic-led clinics for health promotion and preventative care, home visit programmes for high-risk individuals, and remote patient monitoring for chronic conditions. 9 Other models of care include integration within existing primary care centres working alongside general practice specialists, specialist response in collaboration with ambulance services, hospital discharge and transitional care support, mental health and addiction support, palliative care provision, and public health activities such as mass testing, vaccination clinics, and logistical support for public health partners.7,10 These diverse strategies aim to improve healthcare access, quality, and outcomes for various populations while addressing both medical and social needs. These programmes may offer a range of benefits for both patients and healthcare services as they improve access to healthcare for under-served communities, enhance patient outcomes through more frequent and longer patient visits, and increase patient satisfaction through the option of receiving care in the comfort of their own homes.11,12 From the perspective of healthcare services, community paramedicine programmes have been shown to be economically advantageous, 13 reduce acute healthcare utilisation and decrease the need for hospital admissions, 14 emergency department visits, ambulance service requests, and transport. 15
While the benefits of community paramedicine models of care are evident, their implementation is not without significant hurdles. One major factor is funding; securing sufficient permanent funding is essential for the success of any new programme, and this is especially true for community paramedicine programmes, which have often been established with seed funding or other funding that is not permanent in nature. 16 In addition to funding, community paramedicine programmes may be subject to different regulatory frameworks than traditional paramedic services. 17 Community paramedics typically require extra training that goes beyond the standard requirements for traditional paramedic roles. However, the extent of this additional training can vary, as it largely depends on the specific requirements of each programme.1,17 Finally, successful interprofessional collaboration with other healthcare providers, such as primary care physicians, nursing, and allied health staff is also essential for the successful integration of community paramedicine programmes into the wider healthcare system.1,7
Despite the numerous insights gained from previous research, there is no comprehensive guidance document or ‘road-map’ that addresses all the key strengths and challenges faced by healthcare services when implementing community paramedicine programmes. With the establishment of community paramedicine in Ireland in recent years 18 the Pre-Hospital Emergency Care Council sought to explore the experiences of other countries in establishing and delivering community paramedicine programmes. This was the principal driver of this research study. However, the necessity for this study extends beyond merely providing a ‘how-to’ guide for any agent aspiring to implement community paramedicine programmes. It aims to delve deeper into the complex interplay of various factors such as cultural, professional, organisational, and systemic that either facilitate or hinder the successful implementation of community paramedicine programmes. In this context, this research study is designed to understand the lived experiences of representatives from community paramedicine programmes from different countries and healthcare systems, thereby allowing a detailed exploration of the real-world advantages and challenges of implementing and delivering such programmes.
Methods
Qualitative approach
A reflexive thematic analysis approach, developed by Braun and Clarke 19 was chosen as the framework for our study because of its adaptability and theoretical flexibility. This method is a qualitative approach that aims to identify patterns and understand different participants’ experiences, perceptions, and understanding of a phenomenon. This approach was suitable for our research design due to the authors’ relativist/contextualist position. The ‘relativist/contextualist position’ is the belief that understanding of any concept or event is shaped by individual perspectives and specific circumstances, emphasizing that truth can vary based on these different contexts and viewpoints. An inductive approach to data analysis was used and through detailed accounts from participants of their experiences of community paramedicine programmes, we sought to identify experiences, strengths, and challenges faced by community paramedicine programmes across several different regions internationally.
Researcher characteristics and reflexivity
As a paramedic and university course coordinator, the lead researcher's experiences in both clinical practice and academia have informed their understanding of the challenges and opportunities faced by community paramedicine programmes. The researcher's background as a practitioner provided them with firsthand knowledge of the complexities involved in delivering healthcare in diverse settings, which has shaped their perspectives on community paramedicine as a novel model of care. The wider research team is composed of paramedics, a general practitioner, and university course coordinators who collectively possess a wealth of knowledge and experience in clinical practice, community paramedicine programme development, education, and research. The team's experiences have informed their understanding of the challenges and opportunities faced by community paramedicine programmes and have shaped their perspectives on this novel model of care. Throughout the research process, the team maintained an open and reflexive stance to competing ideas from other researchers and participants. We were mindful of potential biases that may have arisen from our experiences and preconceptions. We acknowledged the importance of reflexivity in research, seeking to deepen our understanding of the research context and enhance the trustworthiness and credibility of our findings. The team's diverse backgrounds, expertise in community paramedicine, and perspectives were instrumental in ensuring a comprehensive and nuanced analysis of the data. Both prior to data collection and again during data analysis, we drew on our collective experiences in clinical practice, education, and research, in order to collect and identify key insights and opportunities to enhance community paramedicine programmes. Our unique perspectives and reflexivity helped to broaden the scope of the research and ensure that the findings were relevant and applicable to a range of stakeholders.
Research paradigm
In conducting this research, the lead researcher adopted a critical realist approach 20 as well as a complexity theory lens 21 to guide the analysis of qualitative data. Complexity theory recognises that healthcare systems are complex, adaptive systems characterised by interrelated and interdependent components, non-linear relationships, and emergent behaviours. 19 In the context of this research, complexity theory helps to understand, predict, and manage the dynamic interactions between various elements, such as patients, healthcare providers, organisations, and policies. By applying complexity theory to healthcare, researchers and practitioners aim to develop more effective strategies for patient care, resource allocation, and healthcare system design and the impact community paramedicine programmes have on these healthcare components. This theoretical approach acknowledges that simple, linear solutions may not always be sufficient to address the multifaceted challenges in healthcare and that embracing the inherent complexity can lead to more resilient and adaptive solutions. 22 This epistemological stance was coupled with a critical realist approach. The ‘critical realist approach’ is a philosophical perspective that is underpinned by the belief that while there is a reality that exists independently of our perceptions, our understanding of that reality is shaped by our social, cultural, and personal lenses. This approach allowed the researchers to acknowledge the existence of multiple layers of reality while recognising the intricate interplay between individual, social, and systemic factors that influence the implementation and delivery of community paramedicine programmes.
Study participants and setting
Participants who were designated as representatives for their individual community paramedicine programme were eligible to be included in the study. It is important to note that community paramedicine programmes and models of care vary across the world and these differing models are described in the introduction. As such the participants setting varied as we collected international experiences that encompassed a broad range of community paramedicine programmes.
Recruitment process
Community paramedicine programmes across seven countries known by the research group to have implemented community paramedicine programmes in health service delivery were targeted for recruitment. The countries were Australia, Canada, Finland, Ireland, New Zealand, the UK, and the USA. We sought to elicit responses from a diverse range of programmes across multiple countries while acknowledging that it would not be possible within the scope of this study to identify or describe every implementation of community paramedicine that exists. Thus, this approach was predominantly stakeholder-led, which enabled the identification of target programmes across the countries that have well-established community paramedicine programmes. To achieve recruitment first, we established a team with experience in community paramedicine with lived experience across five countries: Australia (BS, BW, KB, POM), Canada (AB, CL, JH, ML, MN), Ireland (AB, RC, TB), the UK (GE), and the USA (GW, POM). We contacted colleagues with expertise in community paramedicine in these jurisdictions, as well as Finland and New Zealand. This approach harnessed the expertise and network of the team to identify potential study participants.
Participant selection
Convenience sampling, supplemented with a snowballing technique, was used to recruit participants. The study team identified potential participants for the study by first collating a list of community paramedicine programmes through their prior knowledge and research. Within each programme, the team identified potential participants based on their roles and responsibilities within the programme. In instances where the correct person to engage with was unclear, the team sought assistance from key personnel in the respective services to identify the most appropriate contact person. Once identified, the team contacted potential participants via email and invited them to participate in the study. Potential participants were recruited until enough data were collected to enable the research team to ‘answer the question’ in a way considered to be a diverse representation of the experience of community paramedicine programmes across the globe. At the end of recruitment, there were 34 potential community paramedicine programme representatives invited and 29 responded meeting the eligibility criteria and provided consent to participate. Participants were given numbered identifiers and any specific identifying information from quotes used in the results was redacted.
Data collection
We used Qualtrics software to conduct an online survey to gather the experiences of community paramedicine programme representatives. The survey was custom-designed to align with our research questions. To create the survey items, we first thoroughly reviewed existing literature on community paramedicine programmes. 7 This was done to understand the key areas of interest in the field. Additionally, we consulted with experts on our research team to make sure the questions were relevant and would cover the research aim to gather a diverse range of experiences, exploring both the benefits and challenges of implementing and delivering community paramedicine programmes. The final survey consisted of a mix of question types. We had 14 primary questions, all of which were solely, or had the option of, open-ended responses designed to allow respondents the freedom to express their experiences and insights in their own words. Questions that used a structured format, such as multiple-choice format, also were designed to have the option for open-ended responses to allow for straightforward numerical analysis and comparison of responses (see Appendix 1).
Before administering the survey, we conducted a pilot test within the research team to assess the content and clarity of the survey questions. While this pilot provided valuable feedback for improving the survey, we acknowledge it as a limitation of our study. The pilot test was done within the research team, which may not fully represent the diverse perspectives of our target respondents, possibly affecting the validity of our survey. Following the pilot, the survey was disseminated and data collection occurred from November 2021 to February 2022. We sent a reminder three weeks after the initial invite to potential participants to optimise participation.
Analysis
Data analytic strategies
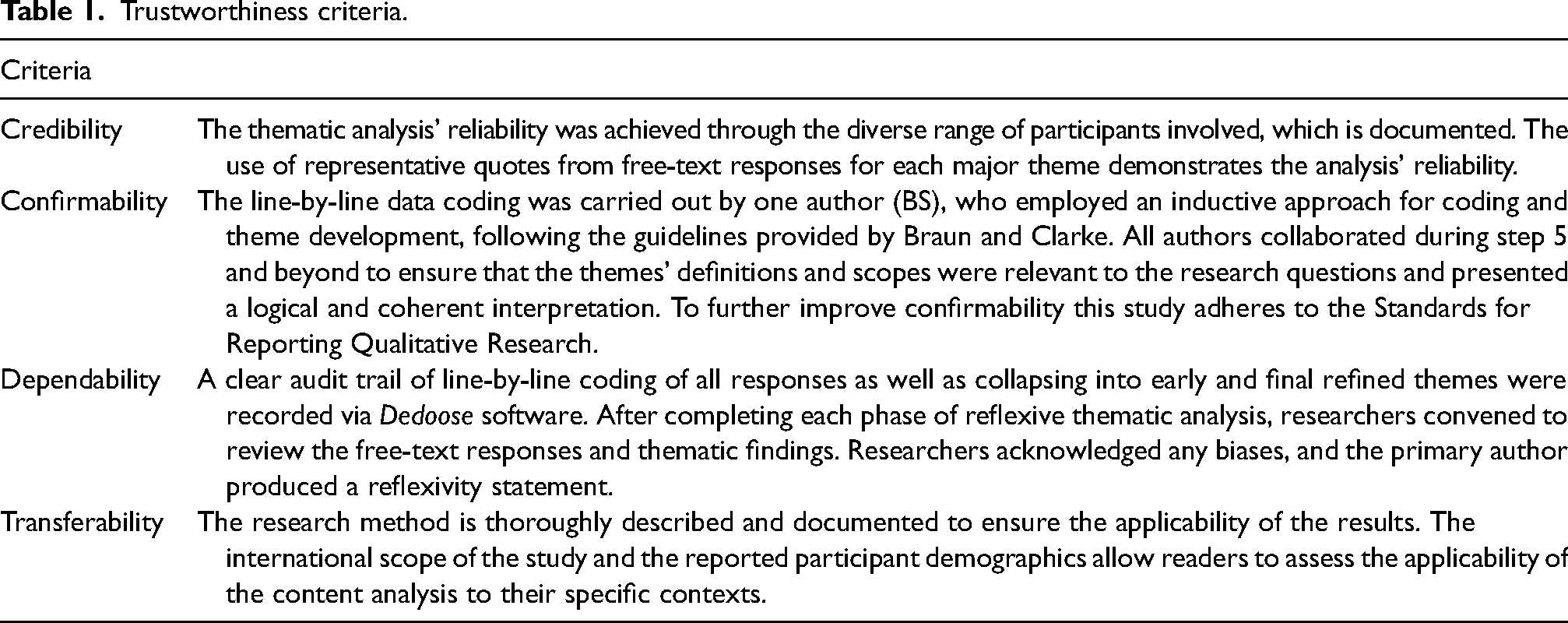
Braun and Clarke's approach to thematic analysis was used as a framework within our reflexive thematic analysis methodology. 19 One author (BS) undertook the initial data analysis which were recorded using Dedoose software. 23 Data analysis used an inductive approach to coding and theme development and due to the specific nature of the research question, we identified themes at the semantic/explicit level. 24 All authors met during step 5 and beyond to ensure the definition and scope of the themes answered the research questions and were plausible and coherent. Trustworthiness in this approach encompassing credibility, confirmability, dependability, and transferability as detailed by Graneheim and Lundman 25 is presented in Table 1. This article adheres to the Standards for Reporting Qualitative Research (SRQR). 26
Trustworthiness criteria.
Ethics
Ethical approval was granted by Monash University (MUHREC Project ID: 36383). All participants provided informed and signed consent.
Results
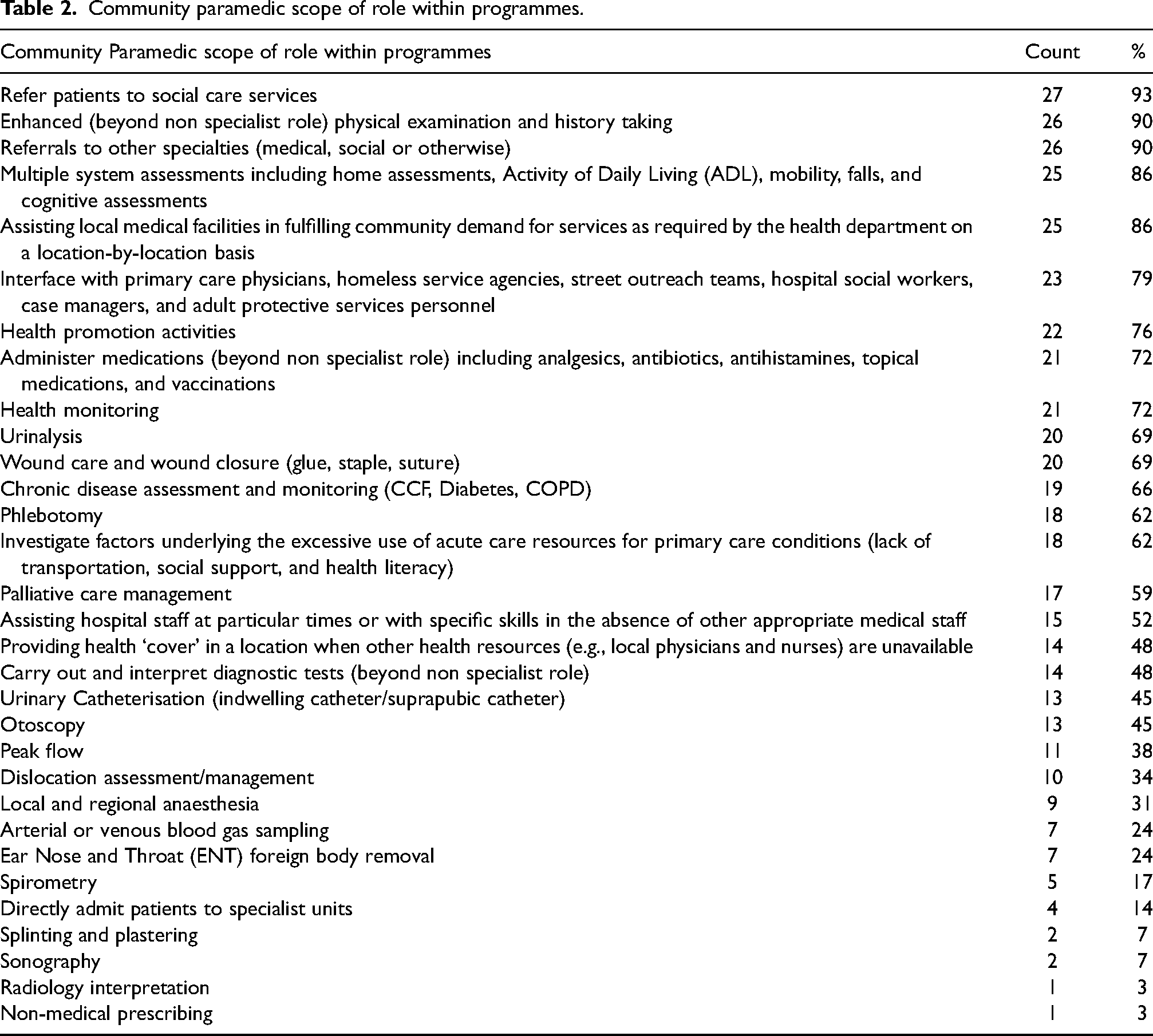
A total of 29 individual responses were received representing 7 countries. Participants and their respective programmes were from Australia (n = 6), Canada (n = 7), Finland (n = 2), Ireland (n = 1), New Zealand (n = 1), the UK (n = 4), and the USA (n = 8). The participants included represented programmes that utilise a diverse range of service delivery models. Fourteen (48%) of the programmes operate under a proactive model of service delivery, actively providing health monitoring and follow-up care to patients referred from sources outside of emergency call-taking systems, or primary paramedic crew requests. On the other hand, five (17%) of programmes adopt a reactive model, focusing on responding to immediate needs presented by emergency calls or requests from primary paramedic crews. Ten (34%) of the represented programmes use a mixed model of care, combining both proactive and reactive strategies. This mixed approach aims to balance the benefits of preventive, ongoing care with the necessity of being able to react quickly to emergencies and immediate needs. The counts of the specific scope of the role of the community paramedics in the included participants’ programmes are outlined in Table 2.
Community paramedic scope of role within programmes.
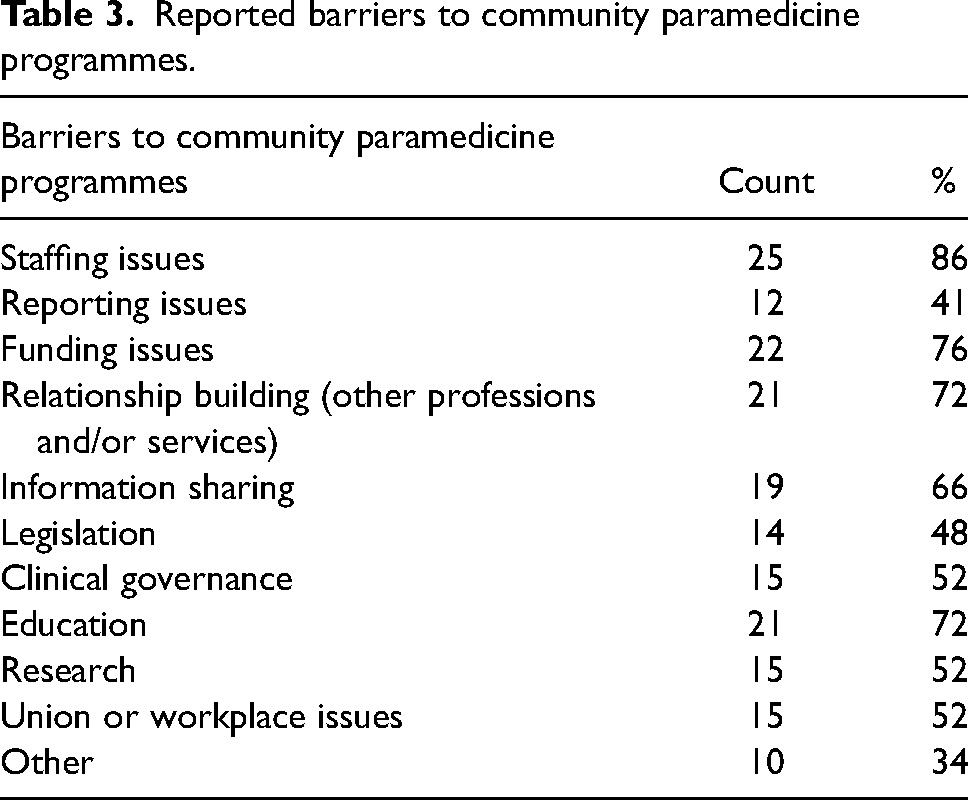
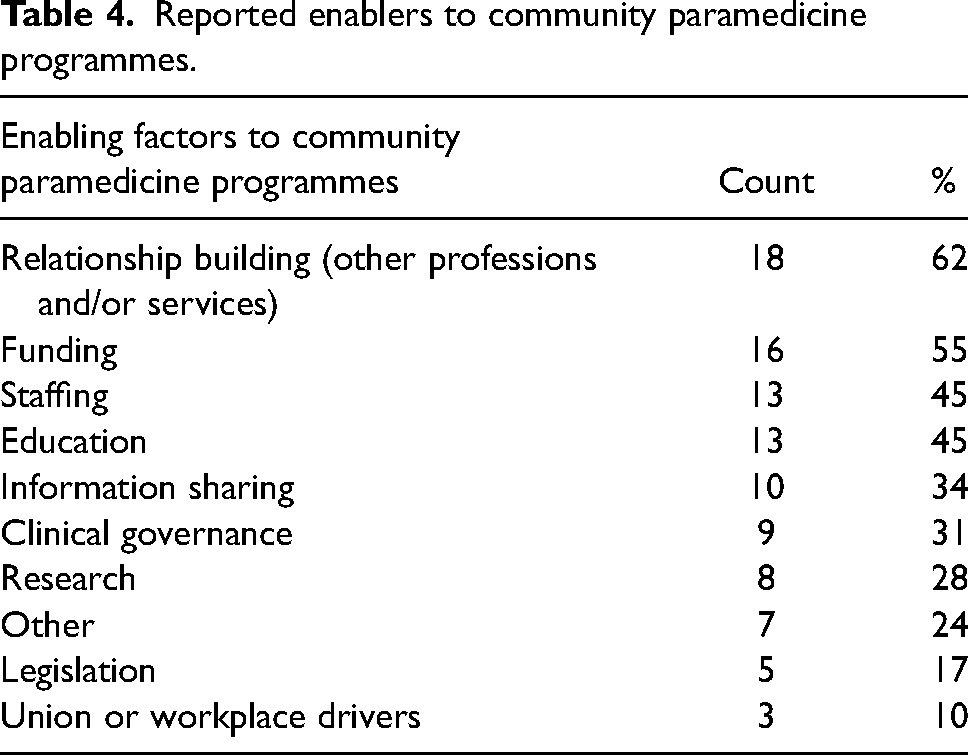
Tables 3 and 4 provide an overview of the response counts to the individual key enablers and barriers to community paramedicine programmes recorded by participants.
Reported barriers to community paramedicine programmes.
Reported enablers to community paramedicine programmes.
Overall, five themes with subsequent subthemes were produced from the data-rich open-ended survey responses which explored the participants’ experiences of the advantages and challenges of community paramedicine programmes. The five themes produced and presented below are: ‘community drives the need’, ‘working with others’, ‘promotion and communication’, ‘effective recruitment and support of community paramedics’, and ‘research and evaluation’. These themes encompass aspects such as community engagement, collaboration, role communication, paramedic recruitment and support, and data-driven evaluation, respectively. Figure 1 provides an overview of the five themes and their associated subthemes.
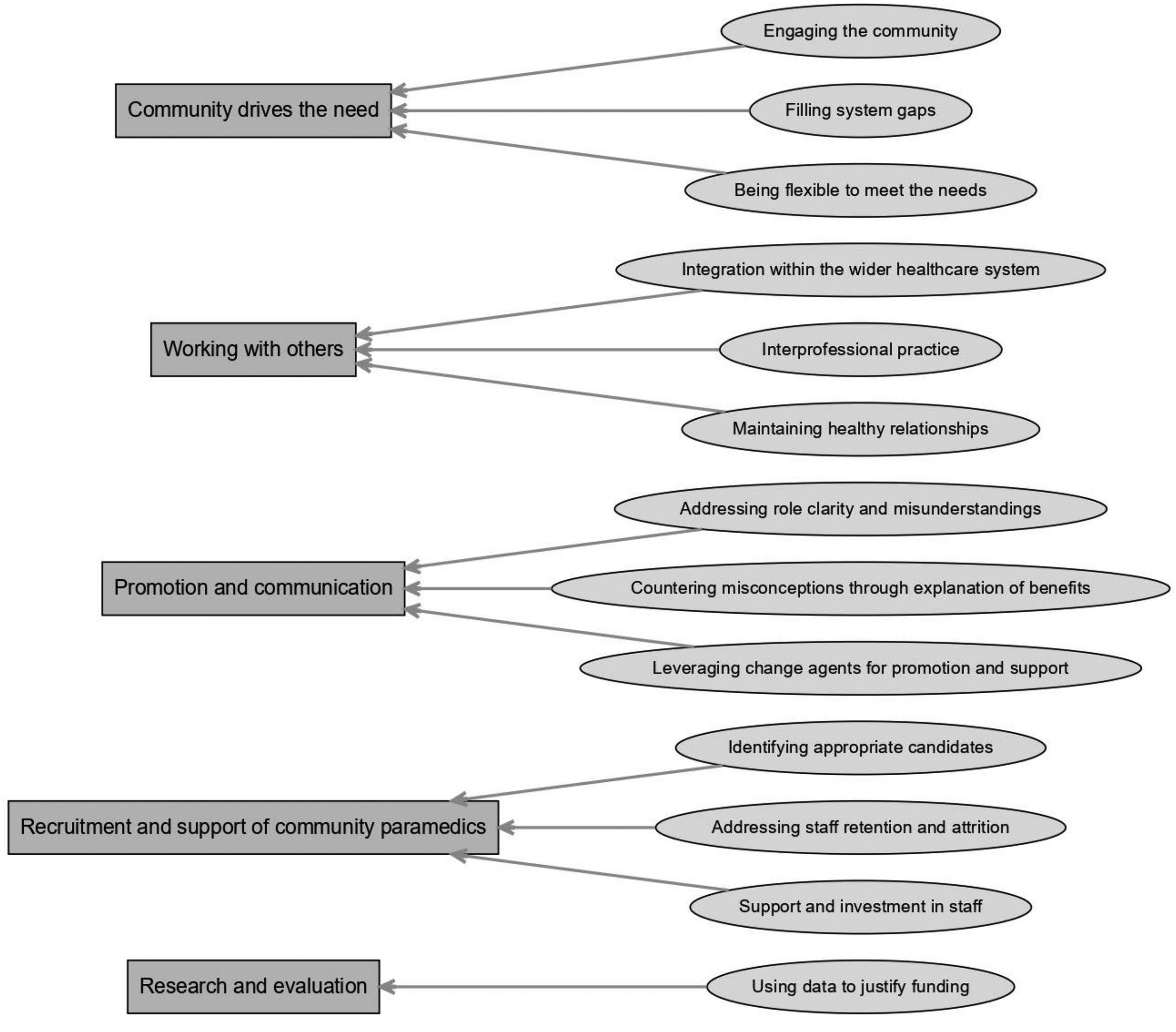
Themes and subthemes.
Theme 1: Community drives the need
This theme encompasses data that highlights the predisposing factors influencing the development of community paramedicine programmes. It included subthemes that showed the importance of engaging the community, filling system gaps, and being flexible to meet the needs of the community. The unifying theme was that the community drives the need for community paramedicine programmes.
ID 19 – Decide where the community is best served, design the programme geared towards that with plenty of room for flexibility and/or growth.
ID 2 – Most importantly it needs to be responsive to the local community needs.
A consistent observation revealed that the presence of underlying unmet community health and social needs served as a driving force behind the establishment and execution of many of these programmes. These health and social needs were often interlinked, and social needs included addressing homelessness and housing, loneliness, substance abuse, and elder abuse.
ID20 – Most of what exists now [in our programme] is well managed and coordinated on the back of a coronial inquest that was set up after 6 indigenous deaths of 33–43-year-olds between [redacted] and [redacted]. These were from the itinerant population, sleeping rough in and around the town.
ID 12 – Our service area has a large population of persons living at or below the poverty level, a large population of persons of Hispanic descent. Some of these individuals are here legally, while many are here illegally, often deterring them from accessing the traditional healthcare system. Our programme focuses on elderly populations, which are also a prevalent demographic in the area, but we also engage any person in the community who requires access to healthcare outside of traditional mechanisms.
Engaging the community
Community-driven needs played a critical role in the development and implementation of community paramedicine programmes. As addressed above, these programmes primarily focus on addressing the unmet health needs of vulnerable population groups. Direct engagement with the community in the early stages of programme development allowed for the identification of underlying issues and the adaptation of programmes to changing needs.
ID 6 – Liaise with stakeholders from the outset and understand thoroughly what they would need to see from the programme for them to regard this as something they wish to support.
ID 3 – make the steering group broad and multi-professional added with a patient member.
Filling system gaps
Community paramedicine programmes were often found to have emerged in response to healthcare system failures that reduced the accessibility of care for patients in the communities they served. Adjusting traditional paramedic services to offer more nuanced and appropriate alternatives was a key aspect of these programmes.
ID 5 – Patient need. A great majority of calls for service are for low acuity and complex calls. This has been driving the case for new models of paramedic care. The Community Paramedic programme is but one of a number of organizational approaches to better connect patients to more appropriate care.
ID 3 – Increased financial pressure led to looking at alternative models of care with economic benefit. The Community Paramedicine programme provided more nuanced care and was cheaper than an emergency dispatch.
Being flexible to meet the need
Programme flexibility was found to be crucial in addressing the unique health needs of communities. Service delivery models were designed in response to these needs, and the importance of remaining flexible and adaptable over time was emphasised. Continual assessment of community needs and adjustments to service delivery models and patient cohorts were found to be necessary for successful community paramedicine programmes.
ID 8 – Routinely (annually or 6 monthly) review your procedures and scope of practice to identify and adapt to changing community needs. Don’t be closed off, it is an ever-evolving role and processes.
ID 17 – Paramedics were able to assist with controlling outbreaks in the County by providing community swabbing and vaccination clinics in convenient, accessible locations. The Service worked collaboratively with our partners (Public Health, Family Health Teams, Community Services, hospitals, retirement homes, and Long-term Care facilities) to assess the needs of residents. Some residents who are vulnerable had challenges related to transportation, mobility, marginalization, and social isolation which created barriers to accessing the mass vaccination clinics.
Theme 2: Working with others
This theme highlights the importance of collaboration for the success of community paramedicine programmes. Effective cooperation with internal and external stakeholders, integration within the wider healthcare system, and interprofessional practice were found to contribute to the long-term viability of these programmes.
Integration within the wider healthcare system
Avoiding siloed operations and being integrated within the wider healthcare system was critical for community paramedicine programmes, as their purpose is to address gaps in healthcare delivery. Participants suggested situating these programmes externally to existing ambulance services to prevent being contained within service silos.
ID 22 – If at all possible, build a programme that is outside both EMS and the regional health service but is comprised of members of each. This will enable staff to own the programme and not be beholden to their respective silos.
Involving programme members from diverse areas was found to also help the creation of an integrated programme. Integrated programmes assisted with continuity of care and involved multiple care providers and referral pathways.
ID 11 – Building relationships with other services, alternatives to transport pathways to other services in primary and secondary care [are key].
ID16 – We also have data to support that the creation of Community Paramedicine programmes without buy-in and collaboration with primary care will not work, as we do not have a means to arrange the follow up care patients will require. Therefore, these partnerships are key in our provincial implementation plan.
Interprofessional practice
Participants expressed that interprofessional conflict can be a challenge that may arise, and as such working with community members and other healthcare professionals was deemed essential for successful community paramedicine programmes that bridge the gap between community, paramedic services, and hospital-based health services.
ID 5 – Our programmes have had a tremendous challenge integrating into the existing system of healthcare (toe's feeling stepped on), and a general lack of understanding about the role and value of a Community Paramedic.
ID 8 – Promotion of the programme to other external health professionals is important and the messaging of how I can support you to help with your workload – that it's a collaborative approach not about taking away patients. Get health professionals to do ride-alongs or placements so they can understand and see what Community Paramedics do. It makes the role seem less threatening to professional boundaries.
ID 18 – It can be viewed by other professionals as stepping on their turf and the communication of how we can help you do your role really helps.
Maintaining healthy relationships
Maintaining healthy relationships underpinned collaborative approaches and interprofessional practice. These relationships were vital for providing integrated care, as community paramedicine programmes need to work alongside primary care experts to facilitate patient access across both services.
ID 19 – Primary care providers are a vital tool for the success for the patients. It provides better continuity of care for the patient overall.
ID 2 – Many happy moments are easily forgotten, and some stressful connections can easily destroy a lot.
ID 7 – Relationship building has required attention and engagement. Concerns from primary health care providers have needed additional attention.
Theme 3: Promotion and communication
This theme encompasses the data showing participants’ perspectives on the importance of articulating the role and benefits of community paramedicine programmes. Addressing role clarity, countering internal and external misconceptions through promoting a programme's objectives, advantages, and its complementary nature to existing healthcare roles was found to be critical for success.
ID 8 – Issues with overall paramedic workforce in understanding that not every patient needs to be transported and understanding, Community Paramedics can overcome this by leading the role and selling the idea by making the scope of practice freely available so that standard paramedics can know what Community Paramedics can do and offer to their patients helps to overcome this barrier.
Addressing role clarity and misunderstandings
A noteworthy subtheme indicated that community paramedicine models of care can be misinterpreted by both internal paramedic services and external stakeholders within the broader healthcare system. This confusion stemmed from the challenge these models pose to conventional understandings of paramedics’ roles within the healthcare system and their capacity to address the community needs.
ID 18 – Management needs to understand what value add the Community Paramedicine programme brings as it challenges key performance indicators. Ambulance services are about the race to the emergency. [With] management, and the higher up you go, the more this idea is enhanced and can limit management and governance systems getting on board with the idea.
Countering misconceptions through explanation of benefits
Participants noted their early identification of this barrier and discovered that elucidating the programme's contributions to the wider healthcare system, patient outcomes, and enhancement of existing services facilitated stakeholder buy-in and improved the acceptability and integration of community paramedicine models of care.
ID14 – Develop guidelines and communication of standard points so all teams are sharing a common message. Be clear of what the Community Paramedic can and cannot do to support care teams.
ID 18 – Showing value to other professions has been a real driver which pushed the establishment of the programme. Outreach promotion has helped to build relationships with other professions about what value add they can bring. Sell yourselves by promoting what value you can add and remember that you are part of a system not isolated on your own.
Leveraging change agents for promotion and support
Participants underscored the importance of engaging with key decision-makers, communicating the programme's benefits, and securing their support as crucial elements for long-term success. Employing social media and programme champions, particularly within paramedic services, proved to be an effective method for promoting the value of community paramedicine models of care.
ID14 – Start with early adopters, people interested in starting the programme that will become champions.
ID 13 – Word of mouth and twitter have been useful, especially since the pandemic prevented me from dropping in to services to introduce myself. General Practitioners are very supportive too, and integrated me into their team from our first meeting.
ID12 – Having excellent success building relationships from an interdisciplinary standpoint, as well as throughout the healthcare continuum. We run into some instances of Registered Nurses in particular telling us to ‘stick to driving the ambulance and leave the medicine to people who know what they are doing’, I attribute these to a lack of education about what our teams are capable of and failure to understand the training and education that our teams possess.
Theme 4: Effective recruitment and support for community paramedics
This theme emphasises the importance of recruiting and retaining suitable staff for community paramedicine programmes and providing them with the necessary support and resources to ensure successful service delivery.
Identifying appropriate candidates
Participants highlighted the need for experienced paramedics with specific personality traits and key attributes, such as patient advocacy, compassion, and leadership.
ID 8 – Need the right person for the job-recruitment need to identify the right personality and [they] must be passionate about patient advocacy.
Participants emphasised that staff members in these programmes must possess appropriate prior experience, as the role may not be suitable for inexperienced or entry-level paramedics. In doing so, they serve as positive role models for the programme, whether it is integrated within an existing paramedic service or situated within the broader healthcare system. Participants also discussed the need for specialised education for these paramedics. There was a general agreement that paramedics in these roles require additional training in areas not covered by standard entry-to-practice paramedic education programmes. It is important to note that this varied across countries, particularly between those adopting entry-to-practice degrees based on other health disciplines and those utilising a public safety model. Where post-graduate courses were not available, in-service education was utilised.
ID 29 – Ideally, the paramedics should be well experienced;5 years with post-graduate university qualifications in community paramedicine/extended care/paramedic practitioner. An in-service education programme should be focused on developing good physical examination and diagnostic skills as well as sound clinical decision making and reasoning abilities (this is something I teach and emphasize in our programme). Appropriate equipment e.g., Istat should be provided to allow for adequate assessment and safe decisions to be made at the point of care. Practice guidelines/protocols should be robust and allow for adjustment based on clinician judgement. They should also be evidenced-based and paramedic led with advice from medicine, but not dictated by medicine. Clinical governance should be provided by trained and experienced Community Paramedics.
Addressing staff retention and attrition
Retaining staff was found to be challenging due to workforce shortages, and there was the risk of skilled paramedics being recruited by other employers and increasing service demands.
ID14 – We have concerns based on available paramedics (shortage provincially), COVID staffing issues due to isolation/illness, and not everyone is suited to a Community Paramedic role but overall, most are receptive.
ID 9 – A concern is the length of time to train and attrition rate when leaving to work elsewhere in the NHS.
ID13 – We currently have no contracts for our roles (first cohort of staff), and no additional pay. During the project we had difficulties with local management however this is not an issue for me now. It was a factor in my decision not to stay in the project beyond my initial contract though.
ID19 – There is no ongoing education/professional development of the role, which is also a barrier for staff retainment.
Support and investment in staff
Recruiting the appropriate staff involved providing them with robust practice systems, flexible work environments, and clinical governance structures. Clinical supervision and 24/7 medical consultation for escalation when necessary were crucial support mechanisms for community paramedics, who often work in isolated contexts.
ID 3 – Local district level and bigger regions – Clinical supervision undertaken by local experienced equivalent. 24/7 consultations with emergency physicians as required.
ID 13 – [Community Paramedics] spend half day per fortnight in general practice working under supervision. General Practitioners also provide mentorship, allowing me to discuss recent patients I have attended.
ID 8 – Time in Community Paramedic role (single crew), time in communications and dispatch used to identify Community Paramedic cases and dispatching them, and then time on emergency crew (double crew). I feel mixed models are very important for staff.
Theme 5: Research and evaluation
This theme underscores participants’ experiences with data sharing, which was used for patient care updates, programme evaluation, and quality improvement. They also tackled the importance of addressing system-level challenges that come with data collection and dissemination. One significant subtheme that was created, which will be further discussed, is the use of data to justify funding. Participants expressed this as a crucial aspect in securing continuous programme funding. Participants emphasised the need for data collection from the planning phase to drive development and support other programmes in their growth. Formal research provided dependability and negotiation power with key stakeholders for continued funding.
ID17 – Data Collection is very important for many reasons including quality assurance and improvement purposes.
ID 14 – Lack of human resources to do research; we collect a lot of data but no means to move it forward.
ID 15 – Action research – always reflect on current practices and make needed adjustments along the way. Ask for help – research to find best practices.
ID 4 – Evaluation of the community paramedicine programme must be constant and the programme should be flexible when reformation needs appear.
ID 9 – Navigation of data between services remains challenging, a ‘joined up’ longitudinal review of care is still not simple to report.
ID 20 – Poorly managed by our organisation from the start! Community Paramedics have developed their own data collecting application by working with the Department of Human Services. They have provided the expertise and hardware to enable a comprehensive point of care ‘client contact’ data collection means (via a cloud-based system and iPad) that has an online dashboard for real-time data observation.
Using data to justify funding
Overcoming data-sharing difficulties proved beneficial for programme evaluation and timely patient care. Data collection was vital for securing ongoing funding. Participants acknowledged that funding arrangements were often ad hoc and different from standard paramedic service funding allocations. They encouraged exploring non-traditional funding mechanisms and emphasised that using research and data to demonstrate programme impact was essential for communicating with current or potential funding bodies, despite challenges in data sharing.
ID 23 – data gathering and management is absolutely essential for not just justification of budget items but overall support both from the service and other community leaders, but even all the way to the state levels or even insurers.
ID 16 – Funding has been our biggest barrier to date. We have implemented all our programmes to date with 3rd party funding and finding sustainability through the government and the [health authorities] has been challenging. We have limited our expansion because we do not know if the work will be financially supported moving forward.
Discussion
The findings from this study provide valuable insights into the strengths and challenges of implementing community paramedicine programmes worldwide. Based on the themes identified, several key points of discussion emerge, providing a comprehensive understanding of the complexities involved in successfully integrating these programmes into existing healthcare systems.
The first theme identified the importance of community engagement and needs identification for community paramedicine programmes to be effective, as well as continual reassessments. This is in line with previous studies that emphasised the importance of accurately identifying community needs to create effective community paramedicine programmes. 27 However, there is ambiguity around the terminology, with some confusion between assessing the health and social care needs of a population versus understanding community resource capacity. From a community paramedicine perspective, it is critical to assess the health and social care needs of the population using a standardised approach. 27 This is important to ensure that community paramedicine programmes are designed to address individual care needs, such as high chronic disease burden compounded by social isolation and mental health concerns, while fostering inter-agency collaboration with other health or social care partners. 27 Community needs assessments are mentioned within the Canadian Standards Association framework for community paramedicine programmes 28 and instruments like the interRAI Community Paramedicine Contact Assessment 29 are emerging to assist programmes in identifying these needs. 30 While individual health services may internally recognise the importance of community needs assessments, a standardised and uniform approach could provide increased clarity regarding the most suitable methods and is an area of further research required.
Identifying and resolving interprofessional conflicts, which can lead to significant breakdowns in health service delivery, is crucial. 31 The success of community paramedicine programmes hinges on the creation and preservation of solid partnerships with various healthcare providers and organisations, promoting integration with the larger healthcare system. 32 Participants underscored the need to cultivate relationships with general practitioners, primary care clinics, and other allied health professionals so that community paramedicine programmes can enhance and complement, rather than conflict with existing services. Our findings corroborate earlier studies that highlight the significance of positive interprofessional relationships for the successful operation of community paramedicine programmes. 31 Challenges often arise within interprofessional practice in healthcare, even though it is a well-documented phenomenon. 33 While some cases of interprofessional practice have brought about substantial benefits to the coordination of patient care, 34 it can also obstruct team performance. 35 Interprofessional conflicts can arise from threats to professional identity, perceived disparities in treatment, values, and assimilation, or when team members experience insults, humiliation, and friction. 36 In community paramedicine programmes, avoiding potential interprofessional conflict arising from the duplication or perceived duplication of existing services is important. To ensure the success and smooth integration of these programmes into the broader healthcare system, proactively mitigating conflicts rather than merely addressing them as they occur can be important. To achieve this, it is recommended to involve care partners in the planning stages of programme development. 37 This collaborative approach will foster an environment of cooperation and mutual understanding. 38
Another vital aspect of effective community paramedicine programmes is the promotion and communication of the programme's objectives and benefits. Previous literature has shown that addressing misconceptions and clarifying the role of community paramedics is crucial for securing buy-in from stakeholders and facilitating integration within the healthcare system.1,39 Leveraging change agents, such as programme champions, and utilising social media platforms were found to help promote the value of community paramedicine models of care, dispel misconceptions, and build trust among other healthcare professionals 40 and the community. Prior studies in palliative care 41 and hospital-based readmission risk programmes42,43 have revealed that common misconceptions regarding the programmes’ roles can be hindered by persistent miscommunication. Overcoming these issues may be achieved through clear purpose statements and the use of change agents to dispel misconceptions. Programme developers and managers should be aware of this when integrating community paramedicine programmes, as it highlights the importance of effective communication and collaboration in ensuring a successful implementation.
The success of community paramedicine programmes may necessitate a distinct governance and clinical supervision structure compared to traditional paramedic services. Medical oversight in community paramedicine programmes varies, where some studies describe remote medical oversight or physician support15,44,45 but the exact roles undertaken by physicians are often unclear. 46 While some researchers argue that robust clinical supervision is required in jurisdictions with limited legislation supporting professional roles, 47 others emphasise that medical supervision should not hinder the development of community paramedics’ professional practice. 48 Governance structures that facilitate the integration and utilisation of community paramedics are essential. Existing protocols may not always be followed or may not cover all aspects of the community paramedicine role, such as social assessments. 14 Thus, as community paramedicine programmes continue to develop and expand, it becomes increasingly important to re-evaluate and adapt clinical supervision and governance structures to ensure the effective delivery of patient-centred care. This may involve refining medical oversight roles, strengthening standard operating procedures, and addressing potential gaps in legislation to support community paramedics in their potentially expanded scope of practice or the transition to true autonomous, yet team based, practice. 17
The study highlights research and evaluation of programmes as a critical theme, emphasising the importance of data collection and sharing for programme flexibility and adaptation and to ensure sustained funding. Participants faced challenges in data collection and sharing; however, overcoming these obstacles can significantly enhance programme outcomes and facilitate the development of best practices. Moreover, a recent systematic review suggested that electronic mobile recording devices could potentially standardise the collection of comprehensive, timely, and accurate health data for field-based research. 49 Similarly, gathering data and evaluating the improvement in quality-adjusted life years for programmes can demonstrate not only individual-level outcomes but also contribute to a robust economic evaluation. This approach provides the solid foundation needed for decision-makers to commit to continuous funding. 50 While traditional medical research primarily focuses on biopsychosocial outcomes, it is crucial for future healthcare studies of community paramedicine programmes to address aspects such as treatment costs and economic evaluations.
In our interpretation of participants’ responses, we heavily leaned on complexity theory and a critical realist approach, as referenced in the methods. Complexity theory has been recognised as a useful tool in health services research, particularly in areas like knowledge translation and interprofessional collaboration, due to its potential to capture and understand intricate dynamics within healthcare systems. 51 We employed this theory to unravel the challenges faced by community paramedicine programmes, viewing them not as isolated elements, but as components of a complex, interdependent healthcare delivery system. This approach extended our understanding of the impact of these programmes beyond individual patient outcomes, considering wider implications such as resource allocation and healthcare system design. Simultaneously, our critical realist stance, increasingly adopted in the study of health and social care systems, allowed us to delve into the multiple layers of reality that influence the implementation and delivery of community paramedicine programmes. 52 This stance guided our investigation of the interplay between individual, social, and systemic factors shaping the experiences and perceptions of those involved in community paramedicine.
This framework, serving as a lens through which we conducted our research, influenced our data collection, analysis, and discussion of findings. Moreover, these approaches hold promise for future research in community paramedicine. They provide a blueprint for systematically exploring the complex dynamics at play in the implementation of such programmes, thus enabling researchers to deepen their understanding of these initiatives and their implications for healthcare delivery.
Limitations
When interpreting the results, several limitations should be considered. First, participants self-identified as representatives of their community paramedicine programmes, which may not fully capture the range of experiences within these programmes, and their perspectives may not represent the entire team or organisation. Second, the study's geographical scope was limited to seven countries, possibly excluding programmes in other countries that may encounter different experiences and challenges. Nevertheless, to the research team's knowledge, this is the first true international synthesis of community paramedicine programme experiences, encompassing all countries that have published peer-reviewed evidence of existing programmes. The research team comprised a diverse group of international community paramedicine experts, which enhanced the understanding of existing community paramedicine programmes. An additional limitation is the use of survey data to collect experiences from the representatives. This method may not provide information as rich or detailed as face-to-face interviews or focus groups, and the survey questions might not address all relevant aspects of community paramedicine programme implementation and challenges. The development of our survey, while comprehensive and guided by literature and field expertise, may still contain potential biases. These biases might stem from the subjective selection of literature or unconscious predispositions of the expert consultants. This could have influenced the framing of questions, leading to unintended skewing of responses. The pilot testing of our survey was conducted within the research team. While this approach provided initial feedback on content and clarity, it also presents a limitation. The research team may not fully represent the diversity of perspectives in the larger pool of community paramedicine programme representatives. This limitation could impact the external validity of our survey, restricting the applicability of our findings to wider contexts. However, the surveys offered flexibility and open-ended questions, allowing participants to express themselves and reveal areas not already included in the survey design. Despite these limitations, the study offers valuable insights into the experiences, strengths, and challenges faced by community paramedicine programmes across several different regions internationally, which can inform the development and implementation of future programmes.
Conclusion
Community paramedicine programmes hold great potential for delivering benefits to patients, healthcare services, and the wider community. This study provides a unique, in-depth exploration of the practical realities of implementing and delivering community paramedicine programmes across diverse healthcare systems. While the potential benefits and success factors of these programmes have been reported in other studies, our research contributes to the existing body of knowledge by offering a consolidated, cross-cultural perspective based on the lived experiences of representatives involved in these programmes. According to study participants, the success of these programmes hinges on several factors, including addressing community and healthcare system needs, fostering robust interprofessional collaboration, promoting effective communication, recruiting and supporting skilled and dedicated community paramedics, and gathering and analysing data for quality improvement and funding purposes. By tackling challenges and capitalising on the strengths of existing community paramedicine programmes, healthcare systems can better serve underserved populations, optimise resource use, and enhance patient outcomes.
Supplemental Material
sj-docx-1-pam-10.1177_27536386231188595 - Supplemental material for The advantages and challenges experienced with the implementation and delivery of community paramedicine programmes: A qualitative reflexive thematic analysis
Supplemental material, sj-docx-1-pam-10.1177_27536386231188595 for The advantages and challenges experienced with the implementation and delivery of community paramedicine programmes: A qualitative reflexive thematic analysis by Brendan Shannon, Alan M. Batt, Georgette Eaton, Matthew Leyenaar, Peter O’Meara, Tomas Barry, Chelsea Lanos, Gary Wingrove, Brett Williams, Michael Nolan, Ray Carney, J.D Heffern and Kelly-Ann Bowles in Paramedicine
Footnotes
Declaration of conflicting interests
Alan Batt is a deputy editor and Kelly-Ann Bowles is an associate editor of the Paramedicine Journal.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was commissioned and funded by Prehospital Emergency Care Council of Ireland and was awarded following a competitive tendering process.
Data availability statement
De-identified participant data is available upon reasonable request from the corresponding author BS.
Supplemental material
Supplemental material for this article is available online.
Appendix 1 Survey questions asked of participants
Please select all that apply or provide further information in the other textbox.
□ Proactive (responding to patients referred to community paramedics from sources outside of emergency call-taking systems. This includes providing health monitoring and follow-up care after referral and enrolment into a community paramedicine programme). Please also outline where referrals from the programme primarily come from □ Reactive (responding to patients who seek care only if they use an emergency call-taking and dispatch system or only if a primary paramedic crew on scene request community paramedic attendance) □ Other
□ Enhanced (beyond non-specialist role) physical examination and history-taking □ Phlebotomy □ Arterial or venous blood gas sampling Urinalysis □ Peak flow □ Spirometry □ Wound care and wound closure (glue, staple, suture) □ Local and regional anaesthesia □ Urinary Catheterisation (indwelling catheter/suprapubic catheter) □ Splinting and plastering □ Dislocation assessment/management □ Multiple system assessments including home assessments, Activity of Daily Living (ADL), mobility, falls, and cognitive assessments. □ Administer medications (beyond non-specialist role) including analgesics, antibiotics, antihistamines, topical medications, and vaccinations. □ Assisting local medical facilities in fulfilling community demand for services as required by the health department on a location-by-location basis. □ Assisting hospital staff at particular times or with specific skills in the absence of other appropriate medical staff □ Providing health ‘cover’ in a location when other health resources (e.g., local physicians and nurses) are unavailable. □ Chronic disease assessment and monitoring (CCF, Diabetes, COPD) □ Health promotion activities Health monitoring □ Referrals to other specialties (medical, social or otherwise) □ Carry out and interpret diagnostic tests (beyond non-specialist role) □ Refer patients to social care services. □ Directly admit patients to specialist units □ Investigate factors underlying the excessive use of acute care resources for primary care conditions (lack of transportation, social support, and health literacy) □ Interface with primary care physicians, homeless service agencies, street outreach teams, hospital social workers, case managers, and adult protective services personnel □ Palliative care management Radiology interpretation □ Sonography □ Otoscopy □ Ear Nose and Throat (ENT) foreign body removal □ Other (please detail)
Please note this response should outline the minimum education and experience required to be selected into a community paramedic role as well as the educational requirements to practice in a community paramedic role. If relevant, please provide the nature of the postgraduate education programmes required.
If possible, how is this different from the existing governance structure if the role operates within an ambulance service?
*Rotational means do your community paramedics routinely rotate in and out of the community paramedic programme role, e.g., rotate through time in a community paramedic role, then time in a traditional emergency response role, then perhaps time in dispatch or communications in a consistent rotational manner)
Please select all relevant options below and elaborate on the points with adequate detail:
□ Staffing issues □ Reporting issues □ Funding issues □ Relationship building (other professions and/or services) □ Information sharing □ Legislation □ Clinical governance □ Education □ Research □ Union or workplace issues □ Other
Please select all relevant options below and elaborate on the points with adequate detail.
□ Staffing issues □ Reporting issues □ Funding issues □ Relationship building (other professions and/or services) □ Information sharing □ Legislation □ Clinical governance □ Education □ Research □ Union or workplace issues □ Other
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.