
Abstract
Keywords
Introduction
Globally, paramedics are increasingly encountering patients with complex needs, reduced health literacy, mental illness concerns, communication barriers, complications of ageing, and who are negatively impacted by social determinants of health.1–5 Appropriate care planning for many of these presentations will often require consideration for pathways other than conveyance to a hospital Emergency Department (ED). Subsequently, traditional paramedic processes of patient consultation, that focus on a rapid clinical assessment, therapeutic intervention, and transport to definitive care,6,7 may no longer be fit-for-purpose for many patients. This is particularly true for paramedic-led care of patients presenting with complex, undifferentiated, non-acute and chronic conditions who may also require intermittent, and longitudinal care.8,9
In response, paramedicine continues to evolve and diversify by developing innovative paramedic roles and models of care. Often occurring within international ambulance health service models of care, extended practice roles have emerged to address a range of healthcare needs across the acuity of care spectrum, including in specialised areas such as critical, non-acute and primary care.8,10–13 Paramedics are also increasingly being employed outside of jurisdictional ambulance service settings, working within multidisciplinary team-based community clinics, urgent care centres, and primary healthcare.10,11,14
There is global heterogeneity in how these models of care and extended paramedic roles operate, resulting in diversity in the terminology used to describe them.8,11 However, these models share a common objective of meeting the needs of underserved and structurally marginalised populations and addressing unmet health service needs. Increasingly within the literature such models are being grouped under the consensus-defined umbrella term of Community Paramedicine (CP). 8 Where this article references these extended roles with increased skills and capabilities beyond traditional general paramedic roles the term CP will be also adopted.
Evidence indicates that paramedics transitioning into these CP roles may require additional support in the form of education and structured tools to provide effective, high-quality, and safe integrated healthcare.15–17 This includes advanced assessment and critical-reasoning skills that support decision-making beyond the standard capabilities of general paramedics.8–10,16–18 Published literature does provide some guidance for paramedics that includes utilising standardised clinical examination and procedural skills similar to those used in primary care.19–23 Also, in some countries such as Australia, entry-to-practice education does require curriculum and paramedic competencies to align with assessments that consider a patient's biopsychosocial and cultural needs.24,25
However, what has not been well described in the literature is an evidence-informed structured process that consolidates theoretical knowledge and advanced assessment skills to guide paramedics in performing a structured holistic consultation with patients who present with complex non-acute needs. 26
Purpose
This commentary expands on previous literature to emphasise the need to develop a standardised, structured consultation framework that supports paramedics transitioning from general paramedic roles into extended practice CP roles to conduct a comprehensive assessment with patients who present with complex non-acute needs.9,10,16–18 A framework that is evidence-informed, person-centred, and explores the patient's holistic biopsychosocial circumstances.27–29 Such a framework may also be applied more broadly to guide a holistic approach for all levels of paramedics when attending to patients with complex non-acute needs.
Additionally, the authors present an illustrative person-centred, holistic clinical consultation framework (the framework) for paramedics and CPs to follow during non-acute presentations. This framework is provided as both an example to aid understanding of the concept proposed, and as a foundation for further development (Figures 1 and 2). We purport that such a framework will guide and empower paramedics in gathering comprehensive information that supports critical reasoning and clinical decision-making to determine patient-centred care planning and complex case management needs. Additionally, we posit that this framework will bolster the confidence of paramedics working within multidisciplinary teams and improve expertise in navigating community-based health and social services. Furthermore, we assert that this framework will improve paramedic-led engagement, education and understanding of how the biopsychosocial factors of individuals can interplay and influence health and wellbeing. Positioning paramedics to respond to the holistic and health literacy needs of patients is likely to improve longitudinal care outcomes, promote community-based wellness and resilience, and reduce hospital dependency.27,30,31
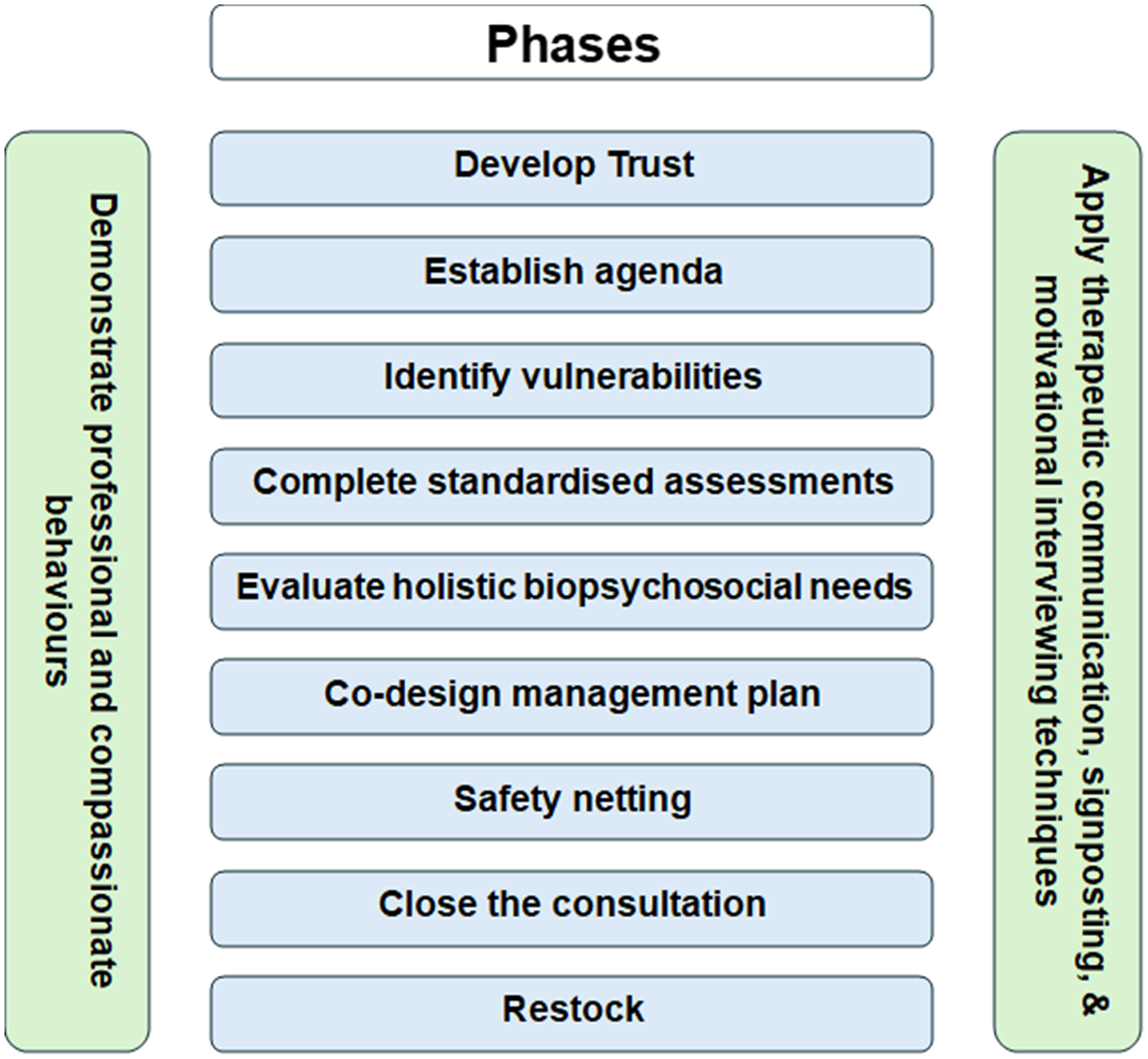
The person-centred holistic consultation framework for paramedics attending non-acute presentations: phases.
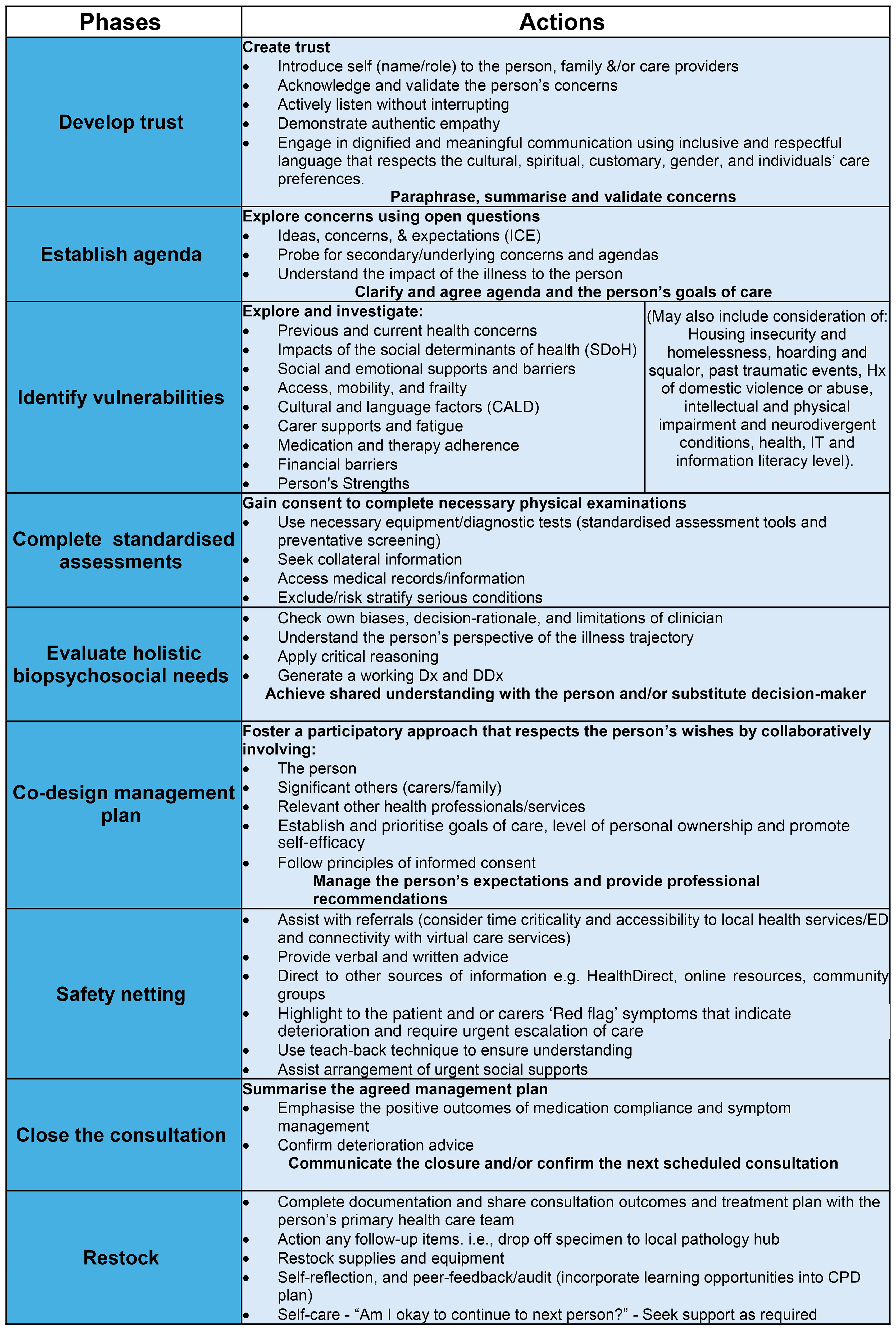
The person-centred holistic consultation framework for paramedics attending non-acute presentations: actions.
Relevance
Contemporary ‘ambulance health service’ 32 paramedic assessments are often guided by principles of emergency system biomedical models; focused on a systematic rapid primary and secondary survey to identify time-critical concerns, and transportation to definitive care.6,7,33 An essential skill expected of paramedics is to provide resuscitative interventions for patients suffering time-critical medical emergencies. However, such incidents may account for as little as 6% of ambulance attendances. 34 There is also an increasing proportion of patients who present to ambulance services with complex biopsychosocial vulnerabilities and needs yet may not require conveyance to an ED for resolution of those needs.1,34,35 Paramedics commonly interact with patients who are structurally marginalised, elderly, or suffering from a multitude of life-impacting conditions such as dementia, anxiety, depression, social isolation, and exacerbations of complex chronic medical issues.3,36,37 These patients often present with non-acute conditions/complaints, do not require immediate advanced clinical interventions, and may be suitable for community-based healthcare services or virtual support, rather than care at a hospital ED.27,38–41
This has created a theory-practice gap and the need for a paramedic-specific framework to guide patient assessment during healthcare of patients with non-acute presentations to support clinical quality assurance and patient safety.27,42–44 Many traditional assessment frameworks, that focus on treating the patient's most urgent clinical needs in hierarchical order, have not been fully developed to explore culminating factors and social determinants of health that could be impacting on the patient's overall health and wellbeing.6,45 Traditional assessment approaches do not commonly consider enablers or barriers associated with primary health and social service accessibility, or question the supports in place for longitudinal or short-term care. Nor do they encourage a deeper understanding of the patient's caregiver and family network to explore the correlation of carer fatigue with increased emergency and health service dependency. In addition, non-acute presentations are viewed by some paramedics as not core paramedic or ambulance health service business. Negative aspects of paramedic culture and perceived role perception associated with lower-acuity incidents further pose a risk of poor decision-making and worse health outcomes for complex patients.46,47
We suggest that the rigidity of the dominant ‘ambulance health’ clinical consultation and assessment models should be complemented by an alternative holistic biopsychosocial assessment approach for non-acute presentations.
Previous research has highlighted the complexity of paramedic decision-making for patients who may not require emergency care.45,48,49 Intellectual skills, communication, clinical decision-making, professionalism, team-based approach to practice, safety and accountability have been identified as key education competencies crucial to contemporary paramedics moving into roles within an increasing scope of practice such as CP. 50 To be clinically effective and provide safe, high-quality healthcare, better suited to non-emergency presentations, paramedics transitioning to extended practice CP roles will often require additional supports and education on how to develop a new process of holistically assessing a non-acute patient.16,47,51–53 The development of an evidence-informed systematic consultation framework is therefore essential to equip CPs with the necessary structure to undertake a comprehensive clinical assessment which incorporates the physical, psychological, social, cultural, and spiritual needs of the patient.28,29,31,54,55 This will enable improved partnerships with patients and primary care providers, empowering paramedics to make well-informed healthcare decisions for people with non-acute presentations.32,56
Paramedics are regulated healthcare professionals in most Anglosphere countries, expected to follow principles of patient-centred care, and uphold professional capabilities to communicate clearly, sensitively, and effectively with the patient, family, caregivers, and other relevant parties in a culturally safe manner.24,32,57 The development of a supportive holistic framework will enhance communication, inclusivity and care planning with people who are structurally marginalised, and those with poor health literacy, who experience higher dependency on the ambulance and primary care services due to complex psychosocial needs and comorbidities.51,58 This includes a high proportion of patients requesting paramedic-led care because of long-term mental illness, alcohol and drug dependency, complex chronic illness, and adverse outcomes associated with ageing, disability, culture, and socioeconomic disadvantage.1,3,58–60
Effective communication, empathy and active listening can have a significant impact on a patient's health trajectory and engagement with health services.49,61 Furthermore, thorough history-taking and fact-checking during patient consultation are associated with diagnostic accuracy, patient satisfaction, adherence to therapy, enhanced patient outcomes, and reduced complaints.56,62–64
However, the disparity between the contemporary biomedical-natured approach of paramedic information gathering and the actual holistic biopsychosocial needs of the majority of patients seen by paramedics, remains inconsistent and unchallenged.13,65,66
The clinical nature of presentations frequently seen by extended practice paramedics aligns closely with presentations managed in primary care, by general practitioners (GPs), community nurses, practice nurses, and nurse practitioners. 2 With this in mind, we suggest that it is worth considering existing frameworks that align closely with models used by primary care health professionals.19,56,67 Some CP education programs do refer learners to well-established models of primary care patient consultation and principles of advanced history taking.19,68 These include the Calgary-Cambridge, Pendleton, and Neighbour's models.69,70 While potentially useful, these models are yet to have their applicability validated for paramedic practice in responsive ambulance health services or urgent and primary care settings. 67
We, therefore, recommend that a paramedic-specific, person-centred holistic consultation framework is developed to support the education and practice of paramedics transitioning into extended practice CP roles.
Foundational framework
To provide clarity around the recommended concept, an evidence-informed example of the framework is provided (Figures 1 and 2). This framework provides a structured, systematic approach aimed at supporting paramedics to conduct a thorough holistic biopsychosocial consultation with a patient with non-acute concerns. It focuses heavily on principles of person-centred care while also considering the paramedic's own agenda, for example, self-care and continuing professional development.
Content validity
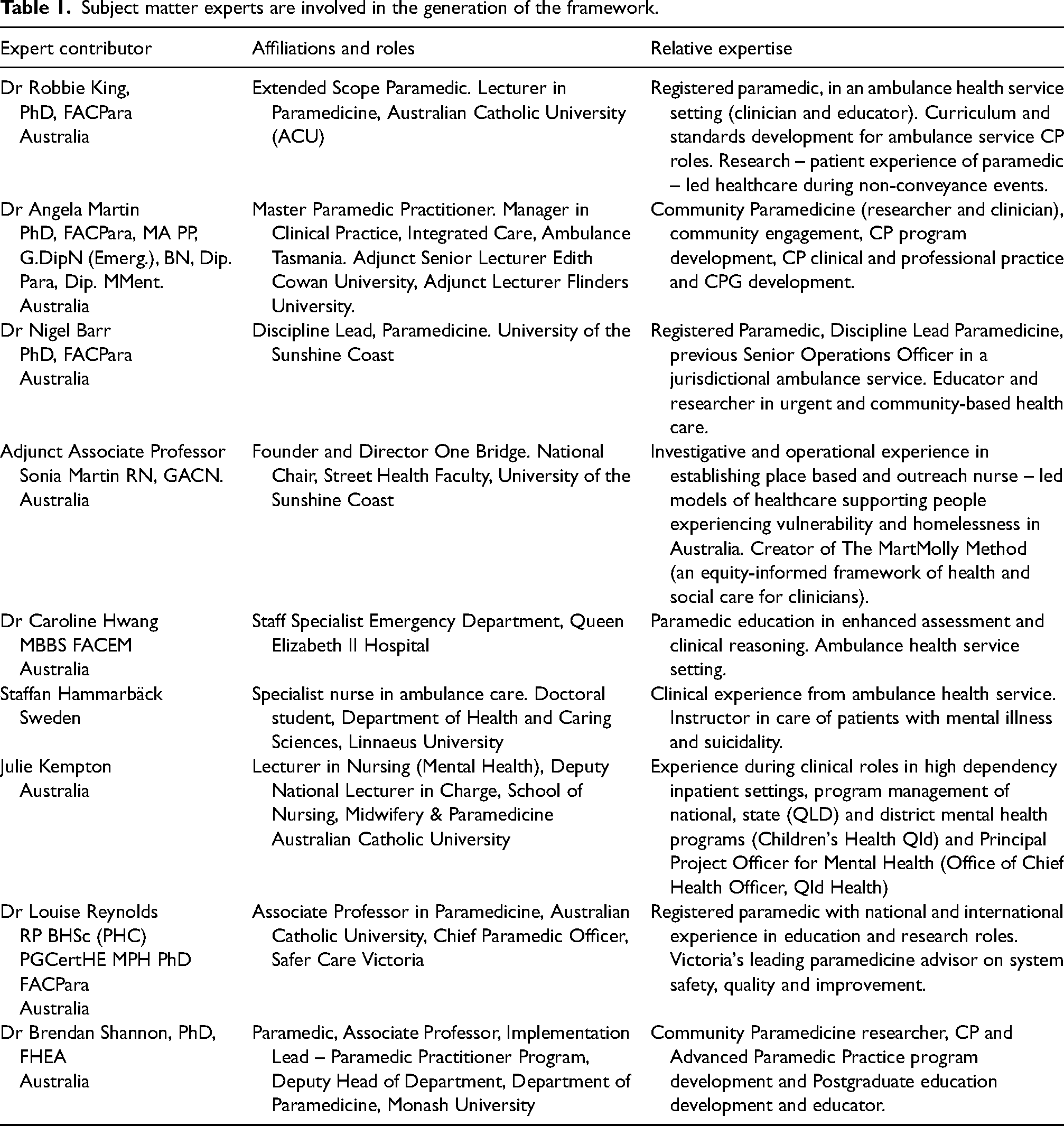
The proposed framework was generated through informal iterative discussions between multidisciplinary healthcare leaders, paramedics, academics, and subject matter experts of international community paramedicine and extended practice models (Table 1). In addition to expert opinion, the framework content was informed by several medical and primary-care consultation and interview models described in the literature, including the Calgary-Cambridge, Pendleton, and Neighbor's models.69–75 Paramedic and patient influences have been considered through the inclusion of person-centred care philosophy, 29 and evidence-informed paramedicine research into patient and paramedic experience that attributed to the chronological flow of the framework.27,76,77 Research into the development of community paramedicine has been incorporated into the design.10,78 The competency standards expected of Australian paramedics are also embedded within this framework, 24 along with the Australian Commission on Safety and Quality in Health Care standards and the National Safety Quality Health Service standards (NSQHS) for Australian ambulance health services.32,57 Although Australian-based, there is potential for international applicability with this framework due to the universal similarities of CP roles.
Subject matter experts are involved in the generation of the framework.
The conceptual framework proposes that paramedics progress through nine phases of consultation (Figure 1). The first phase relates to concepts associated with developing trust, opening the consultation with introductions, developing rapport and active listening to validate the patient's concerns.27,63,75 The second phase involves establishing an agenda and patient care goals. 79 The third phase delves into the patient's wider structural and circumstantial vulnerabilities and social determinants of health potentially impacting health and wellbeing. The fourth phase involves the paramedic undertaking a comprehensive clinical assessment and fact-finding through medical records and collateral documentation.1,11 The fifth phase encompasses evaluating and confirming the holistic and biopsychosocial needs of the patient.70,71,74 Phase six involves the participative co-design of a management plan with an emphasis on encouraging patient self-efficacy, balancing goals and managing expectations.32,63,74 The seventh phase relates to safety netting, ensuring mechanisms are in place to safeguard the patient, ensuring they can access more urgent care should their presentation deteriorate.69,80,81 The eighth phase involves summarising the plan and closing the consultation, while the ninth phase gives an opportunity for restocking, documentation, and self-reflection.69,74,82
To develop clinically effective relationships and promote patient self-efficacy, the paramedic must consistently demonstrate professional and compassionate behaviours and apply therapeutic communication (with signposting and motivational interviewing techniques) as required.24,27,83
Figure 2 proposes suggested actions necessary to complete each phase. We stress the significance of the paramedic's investment in the first phase. We argue that developing rapport with the patient and establishing trust embeds the foundations for achieving an effective and efficient consultation.27,84 This is supported by a meta-analysis by Howick et al., 63 that identified when clinicians take time to express empathy and induce positive expectations, improvements are seen in patients’ psychological and physical conditions and satisfaction with care. Mastering the art of listening, allowing the patient to speak without interruption, and be heard and valued, will further provide rich insights into the patient's agenda and goals of the consultation.
Discussion
This article emphasises the need for a consultation framework for paramedics transitioning into innovative extended practice CP roles when attending to patients with complex non-acute needs. It further provides a foundational consultation approach that scaffolds education and practice for paramedics transitioning into CP roles to better explore a patient's holistic biopsychosocial needs. The authors also provide a methodological approach to develop this framework further; a participatory approach co-designed with consumers and insight from a multidisciplinary team who hold a broad range of expertise of the subject matter.
A person-centric aid to guide paramedic-patient communication and decision-making for patients presenting with non-acute needs is pivotal in supporting robust care planning and case management. This framework provides a structured process towards assessing and addressing the full spectrum of a patient's needs, including biological, psychological, cultural, and social factors. It bridges the gap between commonly applied traditional ‘ambulance health service’ emergency-focused approaches of assessment to guide paramedic-led care of people with complex and chronic non-urgent, non-acute presentations. By providing this structure, the framework may improve role clarity for paramedics transitioning into these positions and enhance understanding between allied health colleagues. A holistic comprehension of the patient will support paramedic-led decision-making and better inform the selection of standardised assessment and screening tools to improve continuity of care. 85 We also propose that by equipping CPs with a consultation framework more congruent with the nature of presentations they attend may result in improved job satisfaction and purpose, psychological safety, well-being, and enhance recruitment and retention to these roles.46,86
This framework could also be considered as an inclusion to complement foundational paramedic practice for ambulance health service paramedics who commonly attend complex non-acute patients. Such a framework may help paramedics in generalised roles manage diagnostic uncertainty, stratify risk, and ultimately support more comprehensive and holistic decision-making. This may enhance person-centred care, decisions regarding the necessity of ED conveyance, and the suitability for patient referral to alternative care pathways.
Experienced paramedics may already incorporate elements of the proposed framework in their practice. However, this approach may be unstructured, lack insights from external disciplines, and omit key components of advanced consultation models.
The shift towards paramedics providing scheduled, preventative, and primary healthcare has generated a mixed response within the profession, despite the evident need, capacity, and capability. 5 Traditional perceptions and emergency service culture may be inadvertently impacting the progression of these roles. Some view these unconventional roles and models of care as a digression from traditional ambulance service practice and responsibilities. 13 This is despite peak national paramedicine professional bodies, influential leaders, and researchers’ advocacy for legislative amendments and for paramedic inclusion, recognition and representation in health policy and health system reform.5,87 The authors posit that the advancement of extended practice paramedic roles represents an overdue evolution of paramedicine, particularly across Australasia. Innovative CP models proven internationally over the past two decades, have alleviated pressure on healthcare systems and significantly improved patient outcomes.18,22,44,88
It is essential that paramedicine research continues to embrace value-based care models to accommodate the increasing number of complex, chronic, diverse, and non-emergency care needs. 89 These patient groups include individuals facing socioeconomic challenges, gender disparity, 90 mental illness, 91 individuals in need of palliative care, and structurally marginalised populations whose access to healthcare is limited by logistical and financial barriers. 59 These marginalised populations also encompass people who have experienced trauma, including the enduring effects of intergenerational trauma and colonisation. Concurrently, the discipline should embrace and invest in the diversification of paramedicine education and practice codesigned with community members, and through interprofessional research, education, and practice.31,92,93 This approach may support the evolution of paramedicine and help define its boundaries to enhance outcomes for the communities the profession serves.
We hope this article contributes to the ongoing discourse of existing commentaries while establishing a platform for further discussion and feedback from paramedic and multidisciplinary subject matter experts.13,78
Limitations
Although the framework has demonstrated content validity, it is provided as an example, intended to assist explanation of the concept of a novel paramedic-patient consultation framework. The framework's development has not yet incorporated patient or public engagement, undergone evaluation by a broader range of experts, or been validated in any setting. The clinicians involved in developing this framework work in diverse care models, though many are from ambulance health service backgrounds. This may have contributed to the focused actions suggested within the framework towards paramedics situated within these responsive settings. Effective application of such a consultation framework requires supplementary education and continued professional development. 62 Therefore, the authors express caution in the use of the framework in a clinical or educational setting until further refinement and validation.
Future research
To address these limitations, the authors and an expanded multidisciplinary research committee, aim to generate an evidenced-informed consultation framework that empowers and enables paramedics undertaking primary care activities either in a distinct role or as a component of their broader paramedic role, to adopt a systematic person-centred assessment approach for non-emergency presentations that (1) comprehensively determines a patient's holistic needs and health literacy level; (2) enhances clinical-decision making; (3) fosters shared-care practice and consultation with multidisciplinary health team members and primary care providers; and (4) empowers consumers through collaborative partnerships with them in care planning, goal setting and case management.
A paramedic-led patient consultation framework for non-acute presentations will be developed using a co-designed, multiple-method approach guided by an implementation science framework and realist philosophy. 94 A focused nominal group technique, guided by a review of the literature, will provide an opportunity for input from multidisciplinary experts.95,96 The resulting framework will then be further refined through expert consensus by applying an online modified Delphi study technique. 97 Implementation science approaches such as the Consolidated Framework for Implementation Research (CFIR), 98 will be used to guide and evaluate the process of translating the framework into practice.
Conclusion
Paramedics transitioning into extended practice CP roles, require a supportive structured framework to gain an appreciation of the holistic biopsychosocial complexities that impact on a person's health, lifestyle, and wellbeing, along with an approach that forms a foundation for reflective practice and quality assurance.
Paramedics are increasingly valued and respected for the capabilities and knowledge that they bring to integrated healthcare models. As the paramedic role diversifies, and clinical capabilities expand it is essential that professional capabilities are underpinned by evidence-informed practice that safeguards high-quality standards of care. Paramedics are well positioned to provide person-centred care for structurally marginalised people in the community who have unmet non-acute biomedical and psychosocial needs. However, this requires a philosophical shift from commonly applied traditional paramedic assessment processes towards an alternative contemporary person-focused consultation that values the holistic needs of people with complex non-acute needs.
This article proposes a novel holistic person-centred framework intended for use by paramedics, particularly those transitioning into extended practice CP roles, to guide a structured clinical consultation process with patients who present with complex, undifferentiated, and non-acute needs.
Footnotes
Author contributions
Robbie King (Conceptualization; Project administration; Writing - original draft; Writing - review & editing); Angela Martin (Writing - original draft; Writing - review & editing); Alan M. Batt (Writing - original draft; Writing - review & editing); Sonia Martin (Writing - original draft; Writing - review & editing); Nigel Barr (Writing - original draft; Writing - review & editing); Caroline Hwang (Writing - original draft; Writing - review & editing); Bill Lord (Writing - original draft; Writing - review & editing); Peter O'Meara (Writing - original draft; Writing - review & editing); Louise Reynolds (Writing - original draft; Writing - review & editing); Staffan Hammarbäck (Writing - original draft; Writing - review & editing); F Shaun Hosein (Writing - original draft; Writing - review & editing); Julie Kempton (Writing - original draft; Writing - review & editing); Brendan Shannon (Writing - original draft; Writing - review & editing).
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: A/Prof Alan M. Batt is a Deputy Editor for Paramedicine, but played no role in editorial decision making, which was conducted in adherence to the journal's blind review policy. All other authors declare no conflict of interest.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.