
Abstract
Community paramedicine is a globally evolving model of care where paramedics provide community-based, preventative and primary healthcare services. With increased global interest and adaptation of the community paramedicine model, there is a lack of a clear definition of the role of a community paramedic. This study sought to come to an international consensus on the definition of a community paramedic. A four-phase Delphi methodology was utilised to achieve a global consensus on the definition of a community paramedic. A systematic approach to expert identification was performed and reported in line with the Conducting and REporting of DElphi Studies standard. A total of 94 community paramedicine experts were identified and 76 experts consented to involvement in this Delphi. Response rate ranged from 81.6% (Phase 1) to 63.1% (Phase 2). Participants expressed the importance of community paramedic definition having components attributed to primary health care, health promotion, chronic disease management and advanced clinical assessment. Participants expressed that these are essential components of the community paramedic skill set, which distinguishes the role from other frontline paramedics. A final consensus with 91% agreement on the definition of a community paramedic was achieved. The four-phase Delphi achieved consensus on the definition of a community paramedic as follows: A community paramedic provides person-centred care in a diverse range of settings that address the needs of the community. Their practice may include the provision of primary health care, health promotion, disease management, clinical assessment and needs-based interventions. They should be integrated with interdisciplinary healthcare teams which aim to improve patient outcomes through education, advocacy and health system navigation. The adoption of the global consensus on the definition of a community paramedic will enhance efforts to promote the value of this specialist role, enabling a better understanding of how a community paramedic contributes to the wider healthcare system.
Introduction
Over the past two decades, innovative strategies such as the development of the extended care paramedics, 1 paramedic practitioners 2 and community paramedic roles, 3 have been pioneered by paramedic service providers internationally. These roles, collectively known as community paramedicine, aim to reduce the burden on overwhelmed health services, supplement primary health workforce shortages, and to improve the patient experience.4–6 As a globally evolving model of care,7,8 community paramedicine programs provide a bridge between primary healthcare and emergency healthcare, predominantly in rural, remote and other under-resourced communities. 9
Previous research undertaken in Australasia, North America and Europe, has evaluated outcomes, participant perspectives and benefits of community paramedic program implementation.5,10,11 While these studies have generally defined community paramedicine as a ‘non-traditional’ service delivery model, few have clearly defined or questioned the role description of a community paramedic. The International Roundtable of Community Paramedicine (IRCP) developed a broad definition of a community paramedic over a decade ago, which suggests that they practice within an ‘expanded scope’. While this might include the application of specialised skills, guidelines and protocols beyond base-level paramedic education and training, alternately the community paramedic might engage in an ‘expanded role’ working in non-traditional roles using existing skills. 12 This current definition, does not clearly identify the skill set, attributes, knowledge or unique descriptors that community paramedics from other expanded practice roles may have.
This lack of clarity affords services employing community paramedicine models of care the opportunity to use a variety of nomenclature to describe community paramedic roles. This variability in nomenclature may lead to a lack of consistency in approach and confusion to both internal and external stakeholders as to the role of a community paramedic. 13 Previous research has highlighted that there can be confusion about what community paramedics do in their role and this lack of consistent terminology only further contributes to this. 14
Literature outside of paramedicine has shown the value of providing evidence-based definitions of practice that differ from traditional models. Defining the specialist palliative care role has helped to differentiate between what care should be provided by specialist palliative care services versus non-specialists. 15 This streamlines services, clarifies when specialist involvement is required and defines what care non-specialists should provide in palliative medicine. 15 Similarly, the role of the pharmacists in disaster response has also been defined and this was found to help professionalise the role in disaster response signposting the importance and capacity pharmacists can bring in a non-traditional role. 16
Likewise, the development of a clear and consistent global definition of a community paramedic is important. It will enhance efforts to promote the value of this role, enabling a better understanding of how a community paramedic can contribute to a patient's healthcare journey. Consistency in definition will provide organisations the opportunity to move to a standardised position on the essential qualification, education, regulation and skill set requirements for the role. The aim of this study is to determine the global consensus definition of a community paramedic.
Methods
Theoretical foundation
This study used a Delphi methodology to come to a consensus on the definition of a community paramedic. While the Delphi methodology can be described as a method of inquiry 17 all research is embedded in a theoretical foundation or research paradigm. This study was embedded in the ontological underpinnings of interpretivism and informed by the paradigm of realism. Realism is underpinned by the belief that there is a single real world and truth, but our interpretation of it will differ due to an individual's context. 18 Where the paradigm of realism departs from the ontological underpinnings of traditional interpretivism approaches is that realism includes the belief that overtime through enquiry researchers can look to understand the single real world through the experiential accumulation of knowledge. Realism is expressed in the Delphi methodology throughout this study as many differing opinions and perspectives are brought together to uncover an agreed or central truth through the experiential accumulation of perspectives and knowledge. 18
Delphi methodology overview
A Delphi methodology, informed by the process described by Delbecq et al. 19 and Okoli and Pawlowski, 20 was utilised to achieve a global consensus on the definition of a community paramedic. 16 This involved a systematic approach to the identification of key global stakeholders, who would be recruited for this study, based on their expertise and knowledge of community paramedicine. Participants were invited to participate in a four-phase online Delphi questionnaire, via a Qualtrics survey. The methods and results are reported using the standard for Conducting and REporting of DElphi Studies (CREDES). 21
Identification of experts
An important aspect of the Delphi approach is the selection of experts. Following the guidelines provided by Delbecq et al. 19 the research team identified relevant experts and invited them to participate in the Delphi. In order to seek input from experts across all community paramedicine domains, the research team sought out representatives from four key stakeholder groups: (1) Management; (2) Clinical; (3) Governance; and (4) Academia. Having an equal representation of participants from each stakeholder group, provided a diversity of perspectives and experience in community paramedicine, to inform on the global community paramedic definition. A Knowledge Resource Nomination Worksheet (KRNW) was utilised to support the identification of key experts, as described by Okoli and Pawlowski. 20
The research team first identified the most prominent countries and jurisdictions who had implemented a community paramedic program or similar. This was established through a review of peer-reviewed and grey literature, to confirm the existence of these programs. Through the grey and peer-reviewed literature the research team first populated experts' names and contacts.
The representation of experts from all four key stakeholder groups was recruited as follows:
Management – The convenor of the international round table of community paramedics
22
was consulted for contacts of management and governance officials. Clinical – Was sought from the Management/Governance group via a snowballing recruitment technique, to include community paramedicine, clinical leaders and clinicians. Governance – Officials involved in the governance of community paramedicine initiatives, were recruited through web searches and via snowballing techniques, recommended by experts in other groups. Academia – Were recruited via review of published literature of relevance.
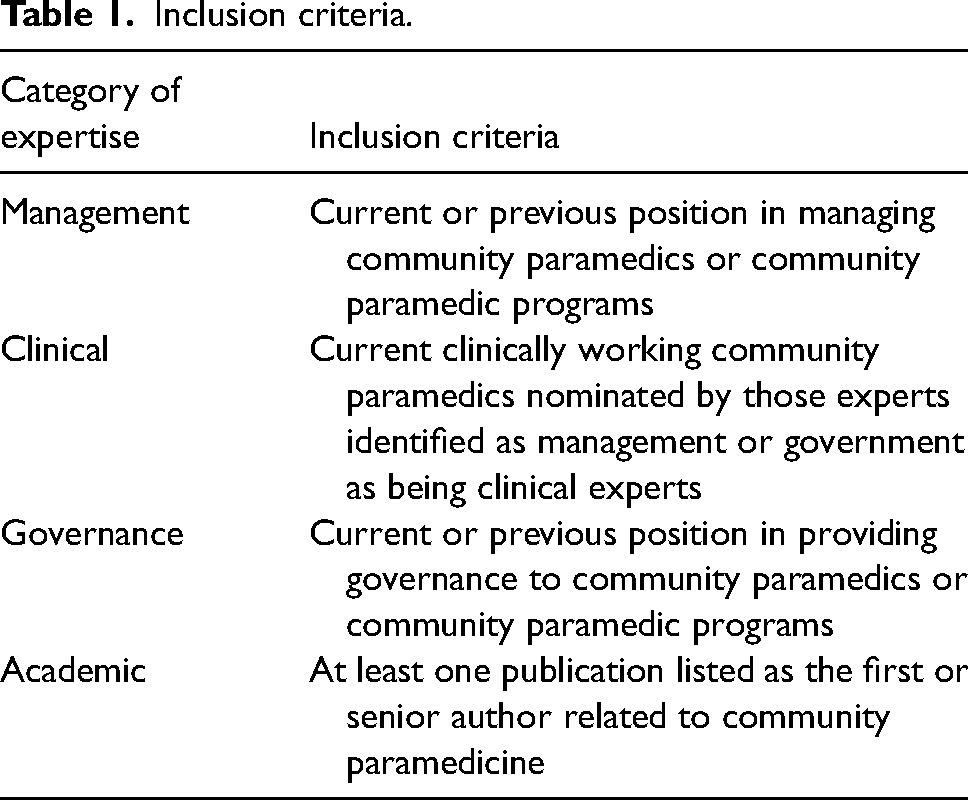
To be classified as an expert in each of the categories the inclusion criterion was applied (Table 1). Where experts could have been included across multiple categories the experts’ preferred criterion was applied.
Inclusion criteria.
After the initial population of names occurred in the KRNW, participants were invited to consent to be involved in the Delphi study via an electronic survey link. Participants were also encouraged to invite any other experts from their network to participate in the study, with the first round of contact aimed at increasing the size of the KRNW.
Delphi questionnaire
The Delphi questionnaire was conducted online via the use of Qualtrics software. The four-phase Delphi process is described in Figure 1.
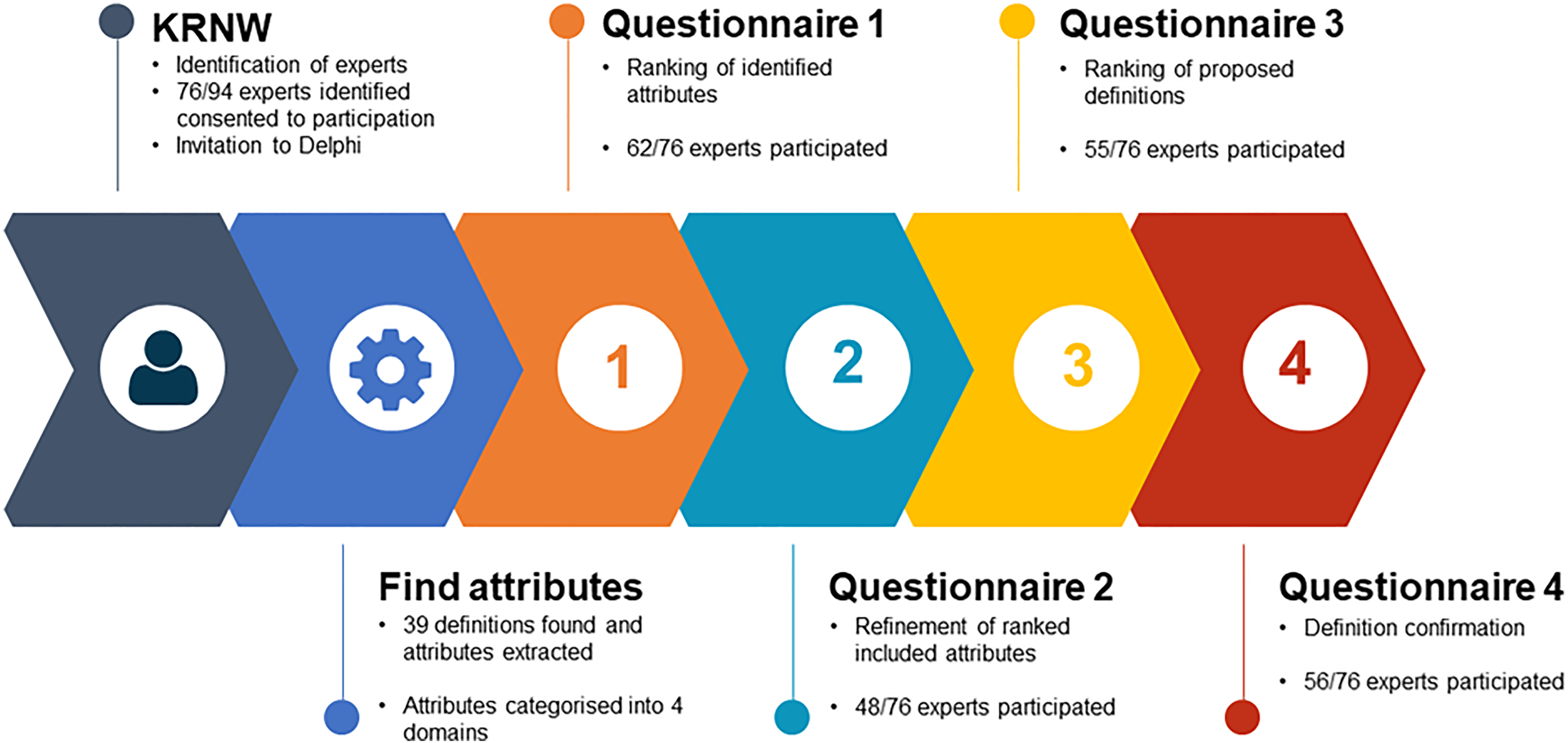
Overview of Delphi process.
Phase 1– ranking of attributes related to community paramedic
The first step towards reaching a global consensus on the definition of a community paramedic involved critiquing peer-reviewed literature to identify the key attributes of a community paramedic documented from previous definitions. Thirty-five (35) studies were identified which provided a definition of a community paramedic as well as six (6) association websites, see Appendix A. The key attributes were extracted from these definitions and placed into four categories after an inductive content analysis of the existing definitions. The categories created were (a) the role of a community paramedic; (b) the scope of practice; (c) integration within the wider healthcare system and (d) place of practice. Experts were asked at this phase to rank on a Likert scale of 0 to 5, 0 being not important at all to 5 being very important, the importance of that attribute being included in the definition of a community paramedic. The attributes with 80% of rankings scoring 4 (important) or 5 (very important) were then included for ranking in Phase 2. Specific definitions and attributes can be found in Appendixes A and B.
Phase 2 – the refinement of included attributes
From the list of attributes included in Phase 1, experts were asked to identify attributes that they believed should be included in the definition of a community paramedic (minimum of 5 and maximum of 7). Participants were also asked to identify attributes that they believed should be excluded from the definition of a community paramedic (minimum of 0 and maximum of 5). This process of attribute selection has previously been used in the formulation of the definition of Paramedicine by Williams et al. 23
Phase 3 – ranking of proposed definitions
After analysing the results from Phase 2, the research team formulated possible definitions of a community paramedic. The definitions were formulated by the research team via an iterative process informed by the highest ranked attributes results as well as the content analysis of the free text responses and the from Phases 1 and 2. From these results, the research team created three possible definitions that they felt satisfied the participants responses from Phases 1 and 2. Experts were then asked to choose a preferred and non-preferred option from the three community paramedic definitions put forward.
Phase 4 – definition confirmation
In Phase 4, a final and singular definition was presented to the experts. The definition was developed from the results of Phase 3. Experts were asked to confirm or reject the proposed definition of a community paramedic. Participants were provided free text responses at each stage of the Delphi process to comment on attributes and the proposed definitions.
Analysis
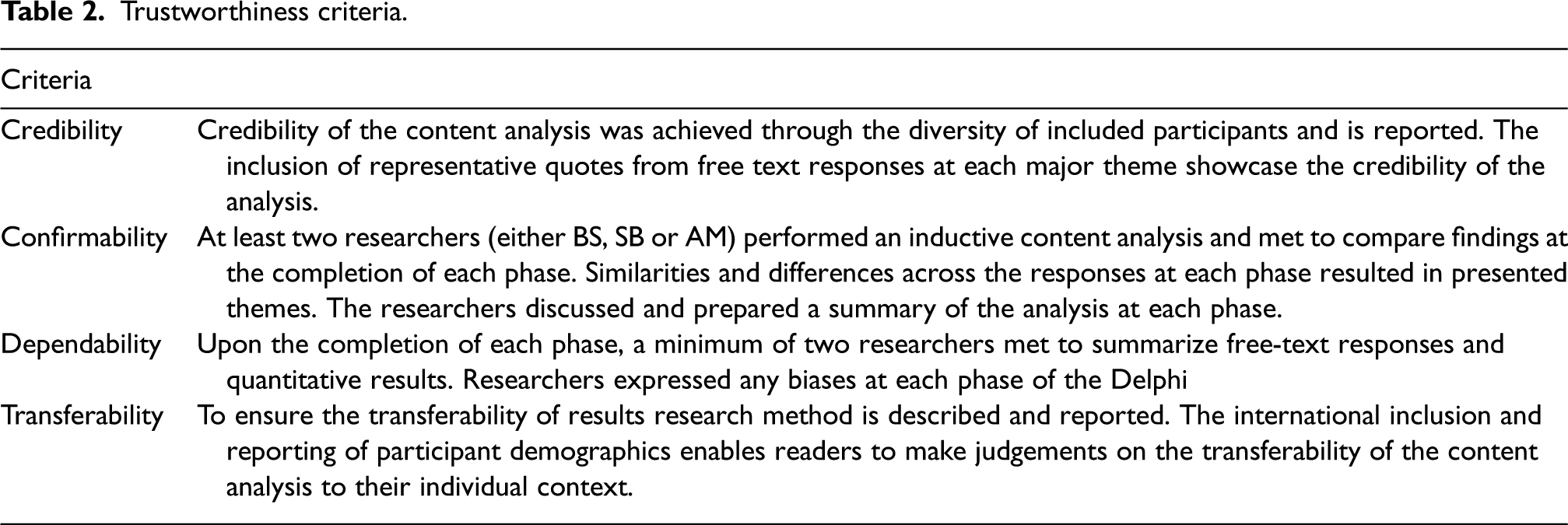
The data was exported from Qualtrics to Microsoft Excel for analysis. Descriptive statistics were used for summary statistics. Free-text responses were analysed by the research team via a descriptive inductive content analysis approach at each phase 24 and recorded in NVivo V.12 software. 25 Author (BS) read through each response thoroughly, coding responses as they related to the phase the responses corresponded to. Each participant response was analysed for meaning units (phrases or sentences expressing an idea). Meaning units were subsequently organised into codes, categories and themes. 24 This content analysis was used to identify frequently recurring items from the participants and where appropriate was used to inform each subsequent phase or presented as results. Trustworthiness in the content analysis approach across credibility, confirmability, dependability and transferability as outlined by Graneheim and Lundman 24 is outlined in Table 2.
Trustworthiness criteria.
Convergence of opinion
A minimum of four phases was designed to reach a consensus on the definition of a community paramedic and the final definition consensus a priori was set at 80%. While there is no consensus on the convergence of opinion, commonly 70% is used, however, the research team followed that as outlined by Stewart et al.
26
and aimed to achieve 80% consensus on the final definition provided in Phase 4. Once an agreement of at least 80% was reached, the research team was satisfied that the final phase of the Delphi was complete. If the agreement was found to be < 80%, the questionnaire would be recirculated showing the participant’s answer and the mean score of other participants for each question along with qualitative answers and they would then be invited to review their responses. To have closure on the final definition in Phase 4 in a timely manner and reduce the burden on participants, the research team planned to use two stop points as outlined in Okoli and Pawlowski
20
:
Consensus reached 80% indicating convergence of opinion. Iteration of each phase was stopped if the mean rankings for two successive iterations were not significantly different. This difference was to be measured using the McNemar’s test (pre–post-test).
20
Ethics
This study was provided ethical approval through Monash University, Human Research Ethics Committee, Project ID: 31384.
Results
Included experts
A total of 94 community paramedicine experts were identified and 76 experts consented to involvement in this Delphi. International experts included were drawn from Australia, Canada, Finland, Ireland, New Zealand, the United Kingdom and the United States of America. Raw numbers can be seen in Figure 2.
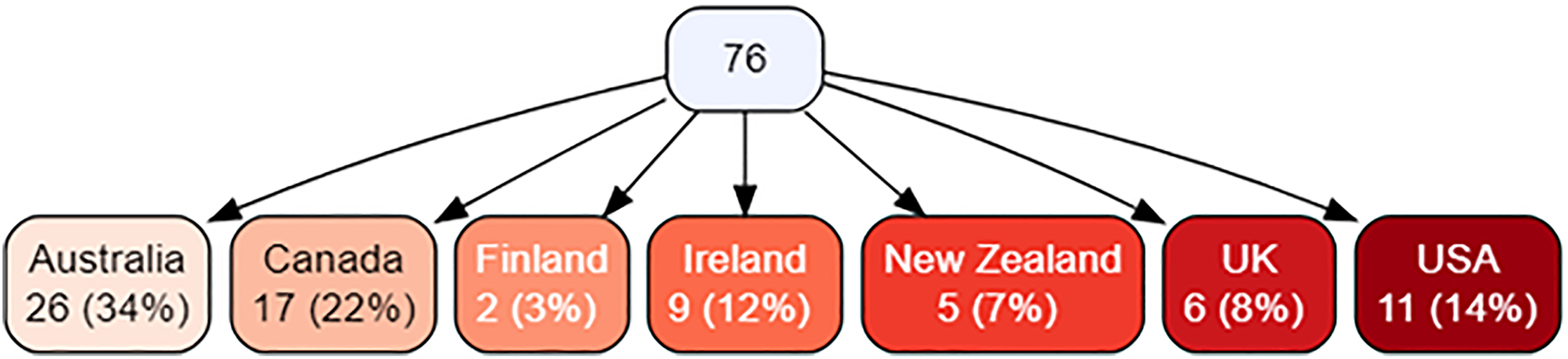
Jurisdictions of included experts.
The category of expertise of the 76 included experts had equal representation across all the included areas sought as shown in Figure 3.
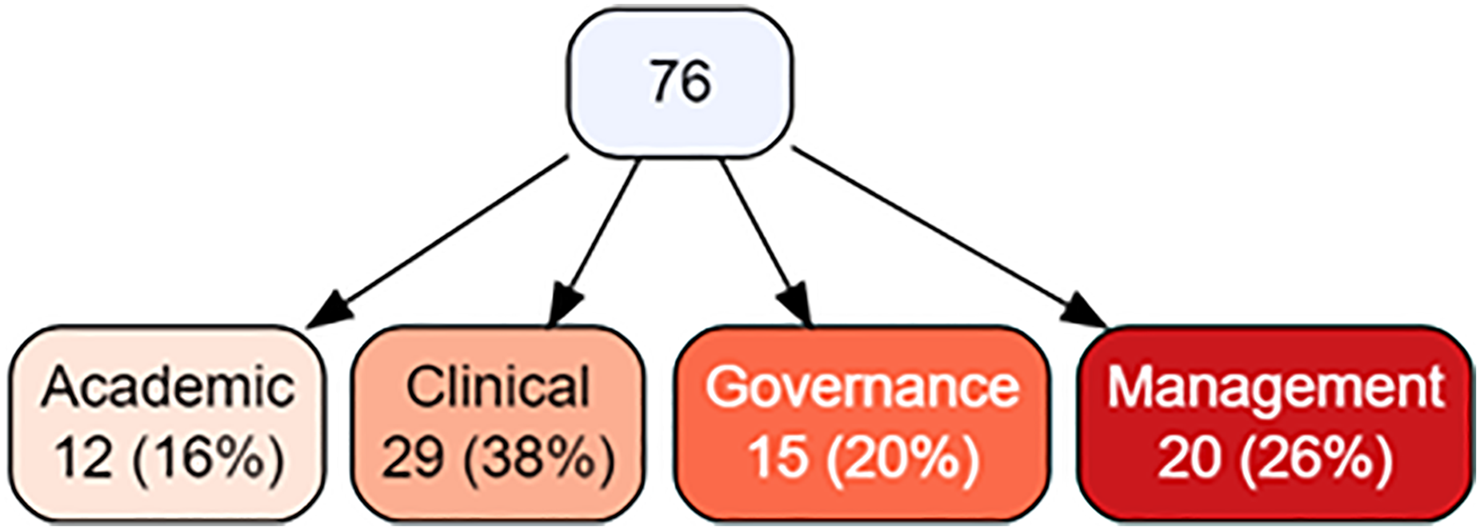
Category of expertise.
Phase 1
The questionnaire for Phase 1 was sent to 76 participants with a response rate of 81.6% (62/76). The 44 attributes extracted from currently existing definitions were ranked on a 5-point Likert scale, see Appendix C for results categorised by domains. There were 22 attributes, which included at least one attribute from each domain, which were scored by at least 80% of participants with a rank of 4 (important) or 5 (very important) and were included in Phase 2.
Content analysis of free text responses – Phase 1
Content analysis of the free text responses in Phase 1 highlighted three important themes; flexibility, interprofessional practice and education requirements. Participants expressed that attributes to be included needed to showcase the flexibility of the role, should highlight the role of interprofessional practice and that there is ambiguity in including prescriptive education requirements in a definition.
Flexibility
Flexibility as an attribute was commented on frequently, with participants stating that community paramedics and the models of delivery they worked in required flexibility and that this should be reflected in the definition. It should not be seen as a one size fits all approach, however. More like a range of possible alternatives that are selected based on any particular community need.
Interprofessional practice
Interprofessional practice and integration within the wider healthcare system was noted to be important attributes especially and that integration with the wider healthcare system was essential. However, participants felt that the place of practice did not need to be overly prescriptive due to the differing models found internationally and the variability in the focus each community paramedicine model may have. It shouldn't be limited to the patients home, it can be where ever the patient might be? We run an indigenous focused program which most participants/patients aren't in their usual homes. It could be on the street, in an ancillary support agency building, government agency building, etc.
Education requirements
Analysis of responses found that the education and experience requirements for the community paramedic role were a point of contention. These differences were evidenced by terminology such as certification, credentialing and competencies, generally associated with industry standards, and terms such as accreditation, registration and scope of practice, more often associated with professional standards. Most participants agreed that a consensus was needed for the community paramedic role to be standardised, however, others indicated that industry certification was sufficient or that external professional accreditation standards were an important criterion. Competency statements are more important as they will allow clinical experience to be recognised, rather than requiring further study.
Although not explicitly defined, some respondents also suggested that experience was an important factor and should be recognised as part of a legitimate pathway into a community paramedic role. There was a mix of opinions over the level of qualification a community paramedic requires, however, the most common opinion supported a master’s degree as the most appropriate educational requirement for a paramedic to work in this role. Yes of course they need to know more, I feel a Masters degree in paramedic practitioner or community paramedicine is appropriate as it will take us through low and high acuity care and give us more credit with other health care professions. Certificates and diplomas are a thing of the past.
Some responses explicitly linked external, as opposed to industry, accreditation standards as an aspect of professional recognition for the community paramedic role as a specialised position. Many participants commented that education and competency would likely differ depending on inherent entry-level requirements and that prescriptive attributes associated with educational requirements should not be included in a community paramedic definition. [Education requirements] is an important part of the role but does not seem essential for the definition.
Based on analysis of attribute rankings and free text responses no further attributes were included beyond those already presented to participants in Phase 1.
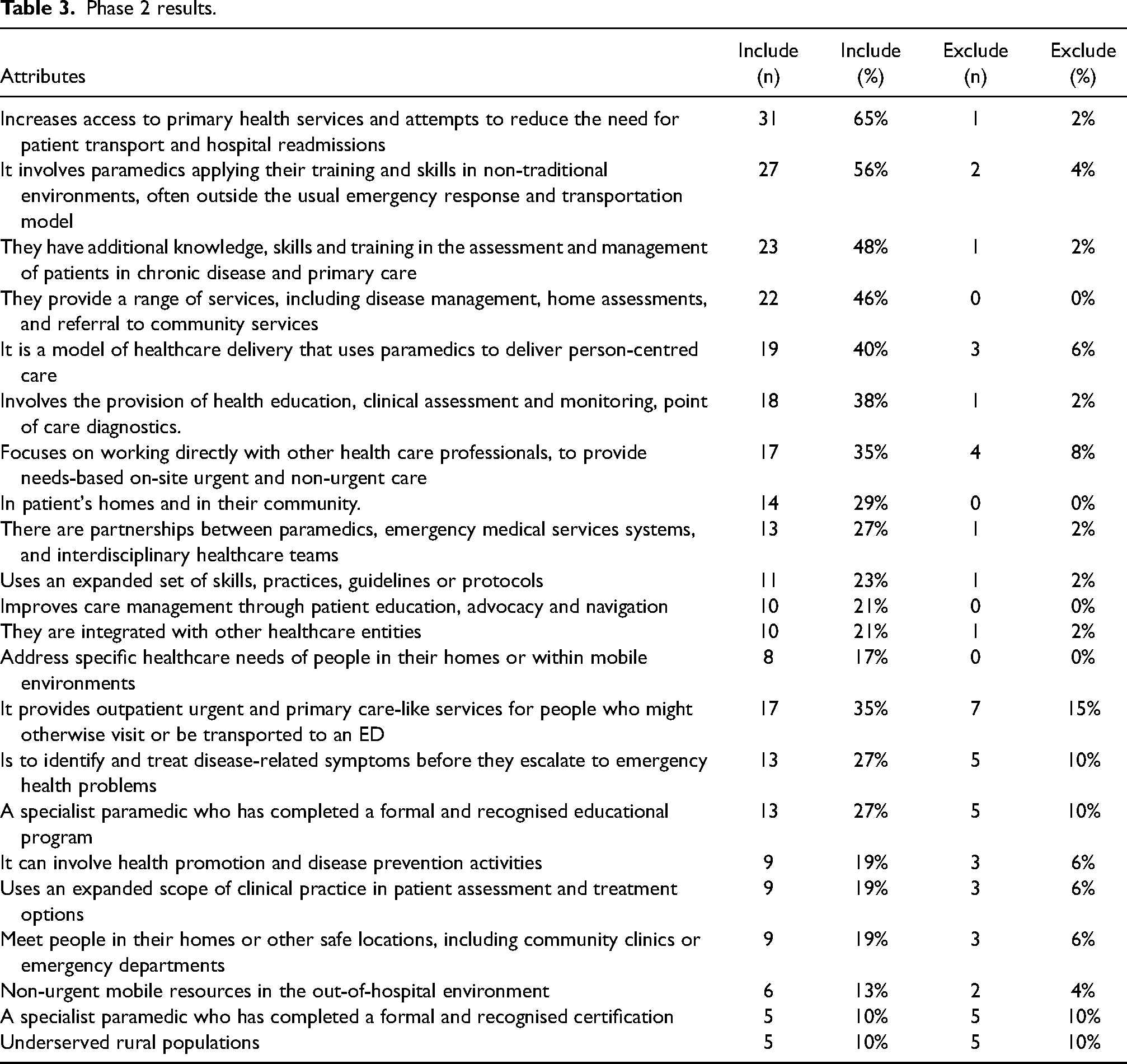
Phase 2
Phase 2 received 48 responses (response rate 63.1%). Only two out of the 22 attributes identified in the first phase were identified by more than half of the participants as ‘should be included’ in the definition (Table 3).
Phase 2 results.
Content analysis of free text responses – Phase 2
Limited free text responses were provided by participants during this phase. The only pertinent component of the analysis of the free text showed that the use of the term specialist could be problematic and should be avoided in the proposed definition: Community Paramedicine will need leaders (specialists and consultant paramedics) but the role should not be the role domain of ‘specialists’.
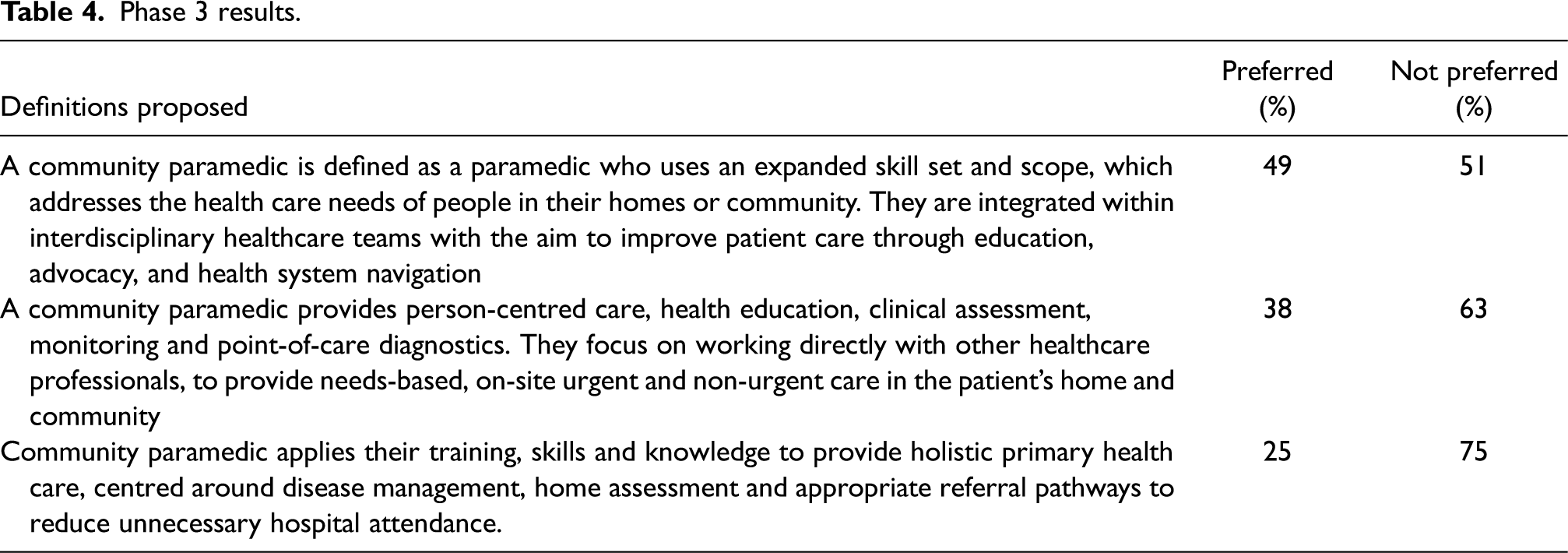
Phase 3
Phase 3 received 55 responses (response rate 72.4%) where participants chose a preferred and least preferred option from three created definitions (Table 4).
Phase 3 results.
Content analysis of free text responses – Phase 3
Free text responses in Phase 3 were used by the research team to better refine and provide a proposed final definition in combination with the quantitative results. Two themes were created based on the responses provided; avoid using specialist term and suggestion that no specifics on scope or skills be included in the definition. Participants noted that the use of the term specialist in a proposed definition was problematic and should be removed: I just don't like the ‘specialist paramedic’ element – as this is a formal level of practice within the UK. I don't like how ‘skillset’ is so prominent. Need to focus on patient care, not vocational notions such as skillset.
Phase 4
A total of 56 responses (response rate 73.7%) were received in Phase 4 (final questionnaire). The participants were presented with the proposed definition formulated by the research team based on the results from the previous three rounds. Participants were asked to accept, defer or reject the proposed definition and had the opportunity to provide qualitative feedback. Ninety-one percent (n = 51/56, 91.1%) reported that they believed it captured the definition of a community paramedic satisfactorily and accepted the proposed definition.
Content analysis of free text responses – Phase 4
Only 11/56 participants provided further free text responses in Phase 4. One theme was noted that aided in the refinement of the final definition, the importance of integration.
Participants noted that the final definition should be aspirational to say that community paramedics ‘should’ be integrated with interdisciplinary health care teams rather than they ‘can’ be as originally provided: Rather than ‘can be integrated’ I think it ‘should be integrated’. I can’t see how a community paramedic that lacks this integration can in fact function or provide a service. The essential nature of the care is its integration within the broader provision of community care – community paramedicine/paramedic cannot and does not live in isolation. A community paramedic provides person-centred care in a diverse range of settings that address the needs of the community. Their practice may include provision of primary health care, health promotion, disease management, clinical assessment and needs based interventions. They should be integrated with interdisciplinary health care teams which aim to improve patient outcomes through education, advocacy, and health system navigation.
Discussion
This Delphi has provided an international consensus on the definition of a community paramedic. This is despite the significant variation in models of service delivery provided across international borders and the differences in underlying general paramedic qualifications and scope of practice. 2 These findings indicate that regardless of education and paramedic scope of practice, the skill set, knowledge and aims of community paramedic roles can be universally adaptable. The community paramedic definition covers a vast area of practice, and the length of the definition reflects this while still providing significant key differences between established and accepted paramedicine definitions. 23 This definition concedes that primary health care, health promotion, chronic disease management and advanced clinical assessment are core components of the community paramedic skill set, that distinguishes the role from other frontline paramedics.
Participants noted in Phase 1 the importance of autonomy of practice over direct medical direction by physicians as a key factor of relevance to the community paramedic role. It should be noted that this may not be reflective of common practice internationally and will depend on underlying education, clinical supervision, and governance structures inherent in the underlying paramedic practice level. 27 For example, autonomy in practice, including the ability to prescribe medication, is integrated within general practice in some areas in the United Kingdom. 28 However, the medical direction may be a requirement in some community paramedic programs where governance structures require it. 29 Despite this, the autonomy of practice is something that paramedics with appropriate training, qualifications and experience are capable of and is something to aspire to for those in areas where this is not yet possible. 30
Throughout the Delphi process content analysis of the free text, responses were valuable in exploring the nuance of the community paramedic role and requirements for the definition. In particular educational requirements for the community paramedic role were a point of contention. It was noted that entry-level paramedic education did not sufficiently address the knowledge needed to work in a community paramedic role and that experience was also required. The need for specialist community paramedic education beyond entry-level education is implied by the work of the US-based Paramedic Network, 31 which has developed a model curriculum and set up an accreditation system, while the International Board of Speciality Certification has also set up a system to certify individual community paramedic specialists. 32 Further work is required to ascertain the educational requirements for this role. Now at least with consistency in definition, regulatory organisations can move to standardise the education, qualifications, and skill set requirements for the role in their system.
The final phase of the Delphi study revealed that participants placed a strong emphasis on the importance of integrating community paramedics into interdisciplinary care teams. This approach to care delivery has been shown to be particularly effective for patients with complex needs, as it allows for a more comprehensive and collaborative approach to decision making and care.33,34
Limitations
While a robust process was conducted to perform this Delphi and was reported utilising an established guideline for reporting in the CREDES guideline there are still limitations. 21 Only 76 of 94 experts identified, consented to participation. Representation of all experts came from only western or European countries with a skew towards Australian-based experts, which may bias the definition to suit this region. There are established variations in models of service delivery and scope of practice amongst community paramedics across the globe so this definition may not be specific enough to suit all community paramedic roles. However, the final round of 91% consensus on the definition resulting from this Delphi does highlight that the definition does satisfy most experts’ opinions, despite these regional variations.
There was decay in participation rates throughout the four phases of the Delphi process, with 73.5% of the original participants included participating in the final phase. Despite this decay, previous research has shown that stability in consensus is generally achieved with Delphi participation numbers of at least 20 participants. 35 With 56 participants included in the final phase of this Delphi the concern with decay in participation is reduced.
Implications
The importance of this research and attaining a consensus definition of a community paramedic supports the standardisation of terminology and supports understanding and advancement of the international community paramedicine model of care. Previous research has highlighted that the non-traditional and unique aspects of the community paramedic role, are routinely misunderstood, not only by external stakeholders but by other Paramedics and direct managers.14,36 With a consistent definition, the role, scope, and purpose of a community paramedic, could be better understood by health industry leaders and program funders. This will support those developing and implementing community paramedic roles, and advocate the advantages, explaining how they differ from traditional Paramedic roles while standardising the professional view of community paramedic roles. Additionally, it should be noted that the definition of paramedicine 23 has some overlap with the community paramedic role and that many aspects of the traditional paramedic role may be covered in a definition of community paramedic. As the access to essential primary care continues to be a challenge across the globe, 37 jurisdictions may choose to incorporate the community paramedic role within existing traditional Paramedic roles in emergency response, however, the central focus of a community paramedic versus traditional paramedic role will require a core focus on improving patient outcomes through education, advocacy and health system navigation. A final implication that must be considered is that strict use of the definition may limit future flexibility and hinder advancements in the field. To avoid this, it will be important for clinicians, academics and policy makers to remain open to ongoing development and the potential need to redefine the community paramedic role in the future.
Conclusion
Through the utilisation of a four-phase Delphi process, with 91% consensus, an international consensus on the definition of a community paramedic has been developed. The adoption of the global consensus on the definition of a community paramedic will enhance efforts to promote the value of this specialist role, enabling a better understanding of how a community paramedic contributes to a patient's cycle of care and will assist in informing a standardised position on the qualifications, education, regulation, and skillset the role requires.
Footnotes
Author contributions
BS, SB, PO, NF, AM, MK, KS and ALM conceived the study. BS, SB, PO, NF, AM, MK, KS and AM equally designed the study and the questionnaires. BS and ALM undertook the data collection and data analysis. BS, SB, PO, NF, AM, MK, KS and ALM equally interpreted the data. BS drafted the manuscript and circulated it to authors for contribution. SB, PO, NF, AM, MK, KS and AM edited drafts and approved the current manuscript for publication. BS is the author responsible for the overall content as the guarantor.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Appendix A. Community paramedic definitions identified
Appendix B. Attributes
Utilising content analysis, common attribute themes were identified, and four domains were developed:
The focus and aim of community paramedicine. Scope of practice of community paramedics. The role of community paramedicine within the wider healthcare system. Place of practice.