
Abstract
Background:
Nearly half of subjects after COVID-19 still experience symptoms after 12 weeks, as described in the Post-Covid Syndrome (PCS). Other than the physical alterations perceived, mental health disorders have been frequently reported. Mindfulness-Based Interventions (MBIs) showed beneficial effects on psychological well-being in patients with respiratory dysfunctions, but they have been rarely tested in severe COVID-19 survivors.
Objective:
In a quasi-experimental study, test the clinical and psychological effects of a 12-week Tele–MBI in previously hospitalized COVID-19 patients and analyze the feasibility of the intervention.
Methods:
Subjects earlier hospitalized due to COVID-19 were enrolled 12 weeks after the infection onset, they were assigned to the intervention group (TG) or to the control one (n-TG). Subjects enrolled in the TG attended a 12-week home-based T-MBI and patients of both groups received multimodal rehabilitation interventions according to their own therapeutic needs. Mental health (anxiety, depression, post-traumatic stress disorder (PTSD) symptoms, sleep quality, self-efficacy, and resilience) and quality of life were detected before and after treatment. The feasibility of the T-MBI applied was also investigated.
Results:
A total of 88 subjects were included (44 in the TG and 44 in the n-TG; 63.6% males, mean age 64.4 ± 10.6). Most characteristics were similar between groups at the baseline; TG patients showed greater improvements in different psychological metrics (anxiety, depression, PTSD, resilience, and self-efficacy) compared to n-TG while no differences were found for perceived quality of life. T-MBI was well-accepted by patients.
Conclusion:
Tele-Mindfulness program seems effective in reducing anxiety, depression, and post-traumatic stress disorder symptoms and increasing resilience and self-efficacy in subjects who required hospitalization due to COVID-19.
Introduction
Since the pandemic outbreak in March 2020, more than 26 million subjects in Italy have been infected by SARS-CoV-2, 1 which has been considered the first Western country to be critically affected by COVID-19. 2 Other than severe clinical conditions that can arise in the acute phase,3,4 recent evidence proved that nearly 1 in 2 people still experience symptoms after 12 weeks from the infection onset, the so-called Post Covid Syndrome (PCS). 5
Various adverse persistent effects have been frequently reported concerning the physical domain, such as fatigue, dyspnea, and pain. 6 Other than the sustained physical alterations perceived, psychological disorders have been described by subjects with PCS: anxiety, depression, and Post-Traumatic Stress Disorder (PTSD) symptoms have been frequently noticed so far,5,7,8 similar to what was observed in patients recovered from other Coronavirus diseases. 9 The psychopathological origin of PCS seems multidimensional and related to infective factors and is partially caused also by psychological stressors. Biologically, anxiety and depression could be elicited by a non-resolution of physical symptoms (fatigue, pain, and dyspnea) and their consequences on activities of daily life. 10 Moreover, infective effects on immune response and neuroanatomical structure may contribute to justifying the presence of neuropsychiatric alterations.11,12 In addition, the pandemic socioeconomic impact further worsens mental health in COVID-19 survivors (ie, future uncertainty, traumatic memories, social isolation, and stigma). 8
Across psychological approaches potentially useful for alleviating anxiety and depressive symptoms related to COVID-19, Mindfulness-Based Interventions (MBIs) have been tested.13,14,15 Mindfulness consists of meditation practice with “paying attention, on purpose, moment-to-moment, in a way that is nonjudgmental and nonreactive.” 16
MBIs have shown positive effects on depression, anxiety, stress, and prosocial behavior, providing promising results also on chronic pain. 17 Concerning the effectiveness of MBIs in adults with respiratory dysfunctions, positive psychological consequences have been described in asthma and chronic obstructive pulmonary disease patients,18,19, even if the high heterogeneity reported in terms of treatment applications makes it difficult to have clear indications about the suggested intervention modalities. 20
Particularly, MBIs showed benefits on mental health due to COVID-19 pandemic for anxiety, depression, and stress perception but its effectiveness has been investigated mostly in the general population and rarely in COVID-19 subjects.13,14,15 Specifically, in COVID-19 patients a few applications have been analyzed. Wei in 2020 21 and Shayghan in 2021 22 conducted 2 Randomized-Controlled Trials (RCTs) which revealed an improvement in mental health in hospitalized patients after a 2-week tele-Mindfulness intervention. Indeed, Mindfulness Meditation seems effective in managing post-viral fatigue (such as PCS, Myalgic Encephalitis, and Chronic Fatigue Syndrome), 23 a key factor in COVID-19 recovery due to its relation to late-onset pain, and psychological well-being. 24 However, MBIs have been poorly investigated in severe COVID-19 survivors, and information on their effect in this cohort is still inconclusive.
MBIs represent a viable way to treat patients, especially in pandemic situations thanks to the possibility of delivering interventions remotely, or for pursuing therapies in case of isolation caused by clinical conditions or socio-environmental limits. Thus, online MBIs are a cost-effective means for maximizing subjects’ treatments. In fact, internet-delivered MBIs can effectively reduce waiting lists and are less costly both for patients and clinicians, 25 and are promising for the continuum of care in mental health therapies.
For these reasons, this quasi-experimental study is aimed to test the clinical and psychological effects of a 12-week Tele-MBI (T-MBI) in previously hospitalized COVID-19 patients, analyzing the feasibility of the intervention applied.
Methods
This quasi-experimental study was conducted at the Ferrara University Hospital between June 2020 and December 2021; it has been approved by the local Ethical Committee (code EM66-2022_539/2020/Oss/AOUFe_EM1) and previously registered on ClinicalTrials (NCT04615390).
Subjects’ enrollment
We enrolled COVID-19 survivors after their discharge from the hospital units. We considered eligible patients responding to the following criteria at the time of enrollment: (1) age over 18 years; (2) diagnosis of COVID-19 (WHO criteria 26 ) that required an hospitalization; (3) neuromotor and/or pulmonary rehabilitation treatment during the hospital acute stay; (4) cognitive ability to provide informed consent to study inclusion; (5) absence of severe cardiopulmonary, hepatic, or renal conditions that can prevent them from participating in the study; and (6) no pregnancy.
After 12 weeks from the infection onset, thus following the hospital discharge, all subjects who responded to the previously described demographic and clinical characteristics have been reached out by the clinical research team and enrollment in the present study has been proposed. Patients were asked to participate in a 12-week asynchronous T-MBI program, as a part of a multidimensional integrated rehabilitation intervention. Patients who refused or did not have the chance to accept the intervention (ie, unfamiliarity with technology, absence of internet connection, lack of interest in the intervention or of a caregiver who could support the program execution) were considered as a control group (n-TG), after matching them for sex and age (accepting a range of ±5 years) to the subjects enrolled in the experimental one (TG).
Indeed, due to the pandemic situation caused by COVID-19 in our healthcare system structuring and conducting a Randomized Controlled Trial (RCT) was not possible, neither ethically appropriate.
T-MBI intervention
The T-MBI program consisted of an asynchronous set of meditation voice messages created and sent by a licensed and trained psychologist via WhatsApp for 12 weeks. The first day of meditation was guided by the psychologist for nearly 30 minutes, while in the following days, subjects were free to follow the T-MBI audio received (5-25 minutes); supervision was provided by the same psychologist through phone calls and text messages once a week or in a face-to-face modality when needed.
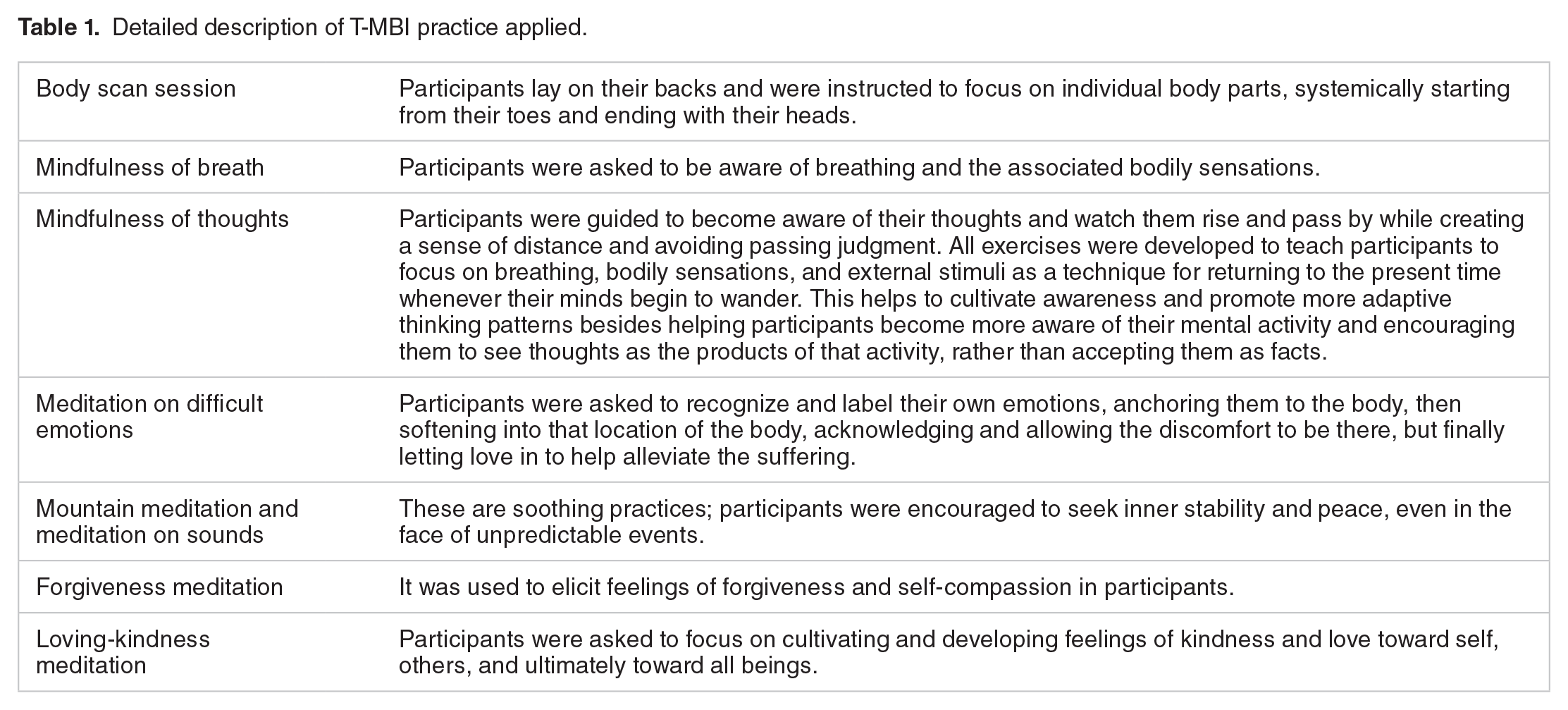
The T-MBI was based on recognized mindfulness practice programs, such as mindfulness-based cognitive therapy (MBCT) and mindfulness-based stress reduction (MBSR). 27 Throughout the entire T-MBI intervention patients were asked to take a “non-judgmental attitude, observing and accepting one’s own experiences and action in the present moment.” 28 The goal was promoting awareness and acceptance, focusing on own’s breath being careful on mind’s wanderings. Further details on the T-MBI applied are available in Table 1.
Detailed description of T-MBI practice applied.
Rehabilitation interventions
Subjects of both groups during the 12 weeks of observation undertook rehabilitation therapies according to the clinical needs pointed out by the physician during the hospital stay and lasted even after discharge. The wide range of clinical treatments included physiotherapy exercises, cardiopulmonary rehabilitation programs, and home physical activity advice.
Outcomes
At the subjects’ enrollment, thus after 12 weeks from infection onset, a series of demographic (age, gender, marital, and working status) and clinical information (length of stay, intensive care unit access, symptoms onset timing, disease severity according to WHO criteria, 26 functional status through 6 Minute Walk Test, and 5 Times Sit to Stand Test) were collected by the clinical research team.
Besides, a set of clinical tools aimed to analyze the main psychological areas were administered at subjects’ inclusion (T0) and after 12 weeks (T1) (that means after nearly 26 weeks from the beginning of infection), thus, right after the end of the T-MBI program for the patients involved in the TG.
- We focused on anxiety and depression as primary outcomes, assessed through the Italian version of the Beck Anxiety Index (BAI) 29 and of the Patient Health Questionnaire-9 (PHQ-9), 30 respectively. Both for BAI and PHQ-9, increased scores are related to worse symptom severity.
- To deeply investigate the mental health status of COVID-19 survivors involved, we also assessed post-traumatic subjective distress (PTSD) due to intrusive thoughts (IES-Intrusiveness), avoidance behaviors (IES-Avoidance), and hyperarousal symptoms (IES-Hyperarousal) through the Impact of Event Scale – Revised, 31 using a cut-off of 33 points to identify a possible PTSD case, 32 where higher values are related to more severe symptomatology. Moreover, self-efficacy was quantified through the General Self-Efficacy Scale (GSE) 33 and resilience via the Connor and Davidson Resilience Scale (CD-RISC), 34 in which higher scores indicate greater self-efficacy and increased resilience. The Pittsburgh Sleep Quality Index (PSQI) was administered to analyze sleep quality and related sleep efficiency 35 ; higher values correspond to compromised sleep quality.
- As global measures of perceived quality of life, the Short Form-12 was collected and explored into the Physical (PCS-12) and Mental domain (MCS-12), 36 increased scores indicate better health conditions.
- Predisposition to MBIs was investigated through the application of the Mindfulness Attention Awareness Scale (MAAS) 37 ; higher values reflect greater mindfulness state aptitude.
For subjects involved in the TG, at the end of the T-MBI performed, feasibility and satisfaction related to the meditation program attended were investigated.
- Feasibility was highlighted by analyzing the rates of patients’ engagement in the T-MBI program measured by the percentage of sessions lost, withdrawals, and dropouts.
- Satisfaction was quantified through an ad-hoc questionnaire in which participants were asked to choose scores from 1 to 5 (Likert Scale) according to the rate of acceptability, utility, and satisfaction perceived.
Statistical analysis
Descriptive analyses were run using the Statistical Package for Social Sciences (SPSS) version 22. Further investigations were carried out in R using specific packages. All continuous variables were expressed as the mean ± standard deviation. Analysis of variance, Student’s t test, and chi-square test were used to highlight differences in the variables of interest (PHQ-9, BAI, IES-total score and its subscores, PSQI, Sleep Efficiency, CD-RISC, GSE, PCS-12, and MCS-12) between groups. All tests were 2-tailed, with alpha set at P < .05. Pearson’s correlation was used to assess the variables’ association. We adopted restricted maximum likelihood estimation (REML), a linear mixed-effects model, to analyze changes over time in the variable of interest; for this purpose, the “nlme” R package was used. 38 As a rough indicator of the model fit, the conditional (pseudo) R 2 was used. This measure describes the proportion of variance explained by both fixed (time and group membership) and random effects (participants) and was calculated according to Nakagawa 39 and Schielzeth 40 and further integration according to Johnson. 41 In fact, the group × time analysis allows to highlight the effects of time and intervention on the post-treatment results observed, considering both recovery time and intervention applied on psychological measures achieved at T1. As a measure of effect size, partial eta square (η 2 p) was obtained. The analyses were carried out with the “MuMIn” and with the “sjstats” packages running in R. Finally, given the presence of multiple analyses and to prevent Type I errors in null hypothesis, we used the Bejamini Hockberg False Discovery Rate (FDR) correction. 42
Results
The sample was composed of 88 subjects (44 in the TG and 44 in the n-TG), primarily male (63.6%), married (84.1%), retired (52.3%), holding a high school degree (53.4%). The mean age was 64.4 years and most of them (77.3%) had a critical form of COVID-19 according to WHO criteria (Table 2).
Demographic and clinical characteristics of the sample.

Abbreviations: 6MWT, 6 Minute Walk Test; 5TSTS, 5 Times Sit to Stand Test; ICU, Intensive Care Unit; LOS, length of stay; MAAS, Mindfulness Attention Awareness Scale; n-TG, non-Tele-Mindfulness Group; TG, Tele-Mindfulness Group.
, statistically significant.
Baseline description
The 2 groups were similar in terms of demographic characteristics, clinical severity, and Mindfulness inclination (MAAS score) (Table 2). All the subjects enrolled were infected during the first pandemic year, thus, before the immunization availability. No significant between groups differences were found for Intensive Care Unit stay, even if TG subjects experienced, on average, shorter lengths of stay. From a functional point of view, TG patients showed greater endurance levels (6MWT data), but comparable muscle strength (5TSTS) (Table 2). Concerning the psychological status of the subjects involved, no between groups differences were found for all the clinical measures detected (P > .05).
Generally, females showed greater anxiety (BAI) and PTSD (IES scores) symptoms, lower resilience levels (CD-RISC), and poorer sleep efficiency (Table 3).
Differences in the variables of interest at baseline according to sex.
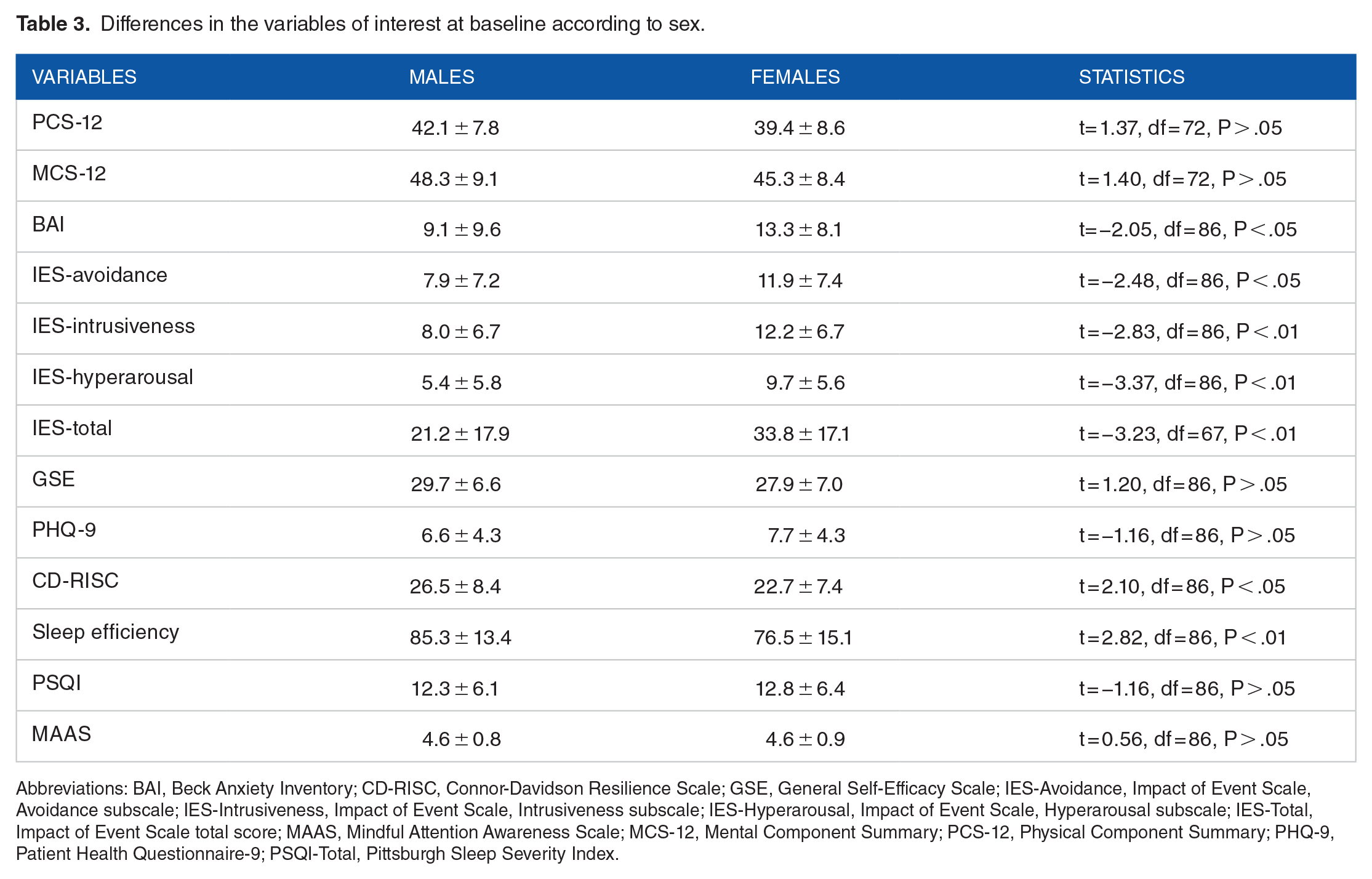
Abbreviations: BAI, Beck Anxiety Inventory; CD-RISC, Connor-Davidson Resilience Scale; GSE, General Self-Efficacy Scale; IES-Avoidance, Impact of Event Scale, Avoidance subscale; IES-Intrusiveness, Impact of Event Scale, Intrusiveness subscale; IES-Hyperarousal, Impact of Event Scale, Hyperarousal subscale; IES-Total, Impact of Event Scale total score; MAAS, Mindful Attention Awareness Scale; MCS-12, Mental Component Summary; PCS-12, Physical Component Summary; PHQ-9, Patient Health Questionnaire-9; PSQI-Total, Pittsburgh Sleep Severity Index.
Intervention results
Results related to the variables scores analyzed between TG and n-TG are shown in Table 4 and the conditional growth model is reported in Table 5. n-TG patients at T1 were more likely to be anxious and depressed, showing higher symptoms of hyper-arousal, and feeling less self-effective.
Within group differences in the variables detected before (T0) and after (T1) T-MBI.
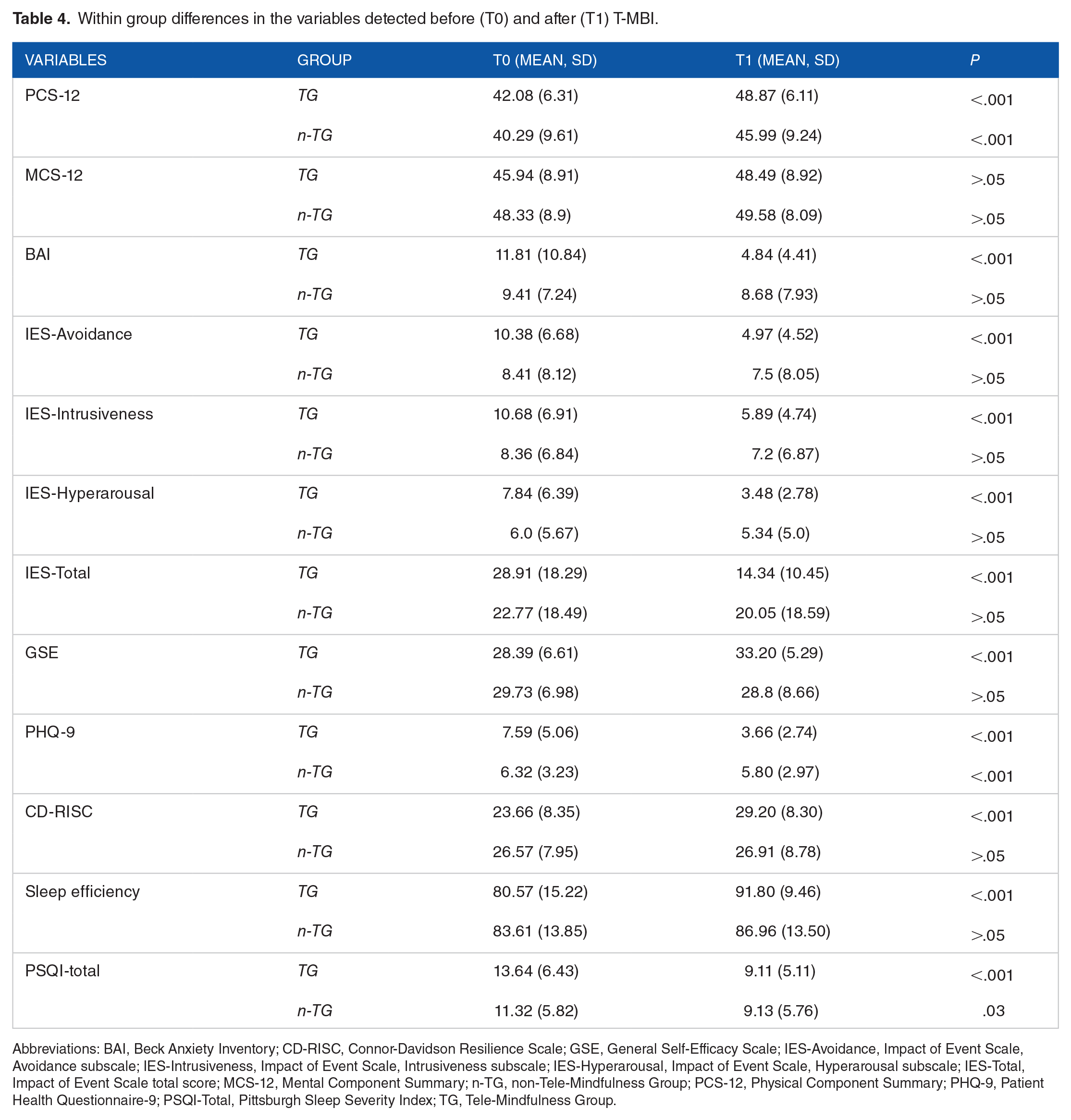
Abbreviations: BAI, Beck Anxiety Inventory; CD-RISC, Connor-Davidson Resilience Scale; GSE, General Self-Efficacy Scale; IES-Avoidance, Impact of Event Scale, Avoidance subscale; IES-Intrusiveness, Impact of Event Scale, Intrusiveness subscale; IES-Hyperarousal, Impact of Event Scale, Hyperarousal subscale; IES-Total, Impact of Event Scale total score; MCS-12, Mental Component Summary; n-TG, non-Tele-Mindfulness Group; PCS-12, Physical Component Summary; PHQ-9, Patient Health Questionnaire-9; PSQI-Total, Pittsburgh Sleep Severity Index; TG, Tele-Mindfulness Group.
Results of linear mixed-effects model.

Abbreviations: BAI, Beck Anxiety Inventory; CD-RISC, Connor-Davidson Resilience Scale; GSE, General Self-Efficacy Scale; IES-Avoidance, Impact of Event Scale, Avoidance subscale; IES-Intrusiveness, Impact of Event Scale, Intrusiveness subscale; IES-Hyperarousal, Impact of Event Scale, Hyperarousal subscale; IES-Total, Impact of Event Scale total score; MCS-12, Mental Component Summary; PCS-12, Physical Component Summary; PHQ-9, Patient Health Questionnaire-9; PSQI-Total, Pittsburgh Sleep Severity Index; *, statistically significant.
Results of linear mixed-effects model fit by restricted maximum-likelihood estimation (REML).
Except for PCS-12, MCS-12, and PSQI, all the variables showed significant interactions (Time × Group) in the expected direction (Table 5). We observed the hypothesized Time × Group effect for BAI and PHQ-9, with significant lower scores found in the TG compared to the n-TG one, with a higher effect size for PHQ-9 than BAI (η 2 p = .37 and .15, respectively); the conditional R 2 was 93.25 for the BAI and 95.97 for the PHQ-9.
These results indicate significantly lower levels of PTSD in terms of intrusive reminders, emotional and behavioral avoidance, and hyperarousal distress at T1 for the TG compared to the n-TG; effect sizes were almost comparable across all the subscales and generally small (η 2 p = .10 for IES-avoidance; η 2 p = .10 for IES-intrusiveness; η 2 p = .13 for IES-hyperarousal; η 2 p = .14 for IES-total), conditional R 2 ranged from 93.05 for IES-avoidance to 93.83 for IES-total.
Even for resilience (CD-RISC) and self-efficacy (GSE), TG subjects reached greater improvements compared to n-TG controls; effect sizes were moderate for both measures (η 2 p = .13 for CD-RISC and η 2 p = .14 for GSE), and the conditional R 2 was 93.88 for CD-RISC and 92.6 for GSE.
Lastly, sleep efficiency was significantly higher at T1 in the TG than in the n-TG (η 2 p = .10), with conditional R 2 = 93.59. No significant interaction effect was observed for PSQI, PCS-12, and MCS-12.
Feasibility and satisfaction
The overall adherence to the program was high; only 2 participants of the TG dropped out during the T-MBI program due to personal reasons (4.5%). Generally, patients reported high satisfaction rates about the experimental intervention tested (mean = 3.9/5 ± 0.7), and many felt to recommend T-MBI to others (mean = 4.3/5 ± 0.6). Patients reported that the most relevant perceived benefits from the T-MBI were managing emotions (mean = 3.1/5 ± 0.6), improving interpersonal relationships (mean = 3.1/5 ± 0.7), increasing energies (mean = 3/5 ± 0.8), and relieving stress (mean = 2.9/5 ± 0.7).
Discussion
This quasi-experimental study focused on the feasibility and clinical effectiveness of a home-based Tele-Mindfulness program on mental health in previously hospitalized COVID-19 subjects. The T-MBI applied revealed positive effects in reducing anxiety, depression, PTSD symptoms, and improving resilience and self-efficacy in a cohort of patients who had a severe form of COVID-19, that required hospitalization and rehabilitation interventions.
The burdensome effect of the COVID-19 pandemic caused critical consequences not only in the acute phase of the infection, both for patients and for healthcare systems, but also in the long-term sequelae, resulting in persistent symptoms, body impairments, and dysfunctions, comprehensively described in the Post Covid Syndrome (PCS). 43 Across the different domains that could be affected by PCS, mental health represents a primary therapeutic need, due to the relevant presence of anxiety, depression, and sleep disorders in these subjects. 8
The clinical effects of the T-MBI applied are consistent with the results previously described in the literature 21,22; online mindfulness interventions improved psychological distress inducing more functional coping strategies in COVID-19 patients. However, these applications were tested in hospitalized patients, when the influence of several other variables (such as the environmental setting, acute clinical conditions, and medications) could significantly impact the mental health changes observed. The long-term psychopathological status after COVID-19 represents a therapeutic challenge due to the overall complexity of the PCS; the absence of a full resolution of physical symptoms, the presence of traumatic memories, and still perceiving difficulties in activities of daily living execution could exacerbate psychological disorders. The core feature of mindfulness practice which is focusing on the present moment, with acceptance and refusing judgments and criticism, could alleviate patients regarding fear about their future, worries related to physical recovery, being aware of the sensations felt in that moment. Indeed, MBIs have been widely tested in the treatment of persistent conditions, such as chronic pain, 44 fibromyalgia, 45 and somatization disorder, 46 providing benefits in pain reduction, depressive symptoms, and quality of life. 47 Practicing mindfulness-based meditation seems to activate the posterior cingulate cortex and other brain areas involved in self-regulation, adaptive behavior, and interoception. 48
Despite positive changes in psychopathological dimensions, no between groups differences have been found in the overall perceived quality of life after the 12-week period, both in the physical and mental components. Certainly, quality of life is a deeply complex concept that is influenced by several factors other than multiple psychological features. The present study was performed during the first phase of the pandemic irruption, that is before the immunization availability, and the global social crisis strongly affected the common perceived well-being.
Surely, the present study has limits that need to be considered. First, the study design, thus the absence of a randomized controlled group, strongly influences the quality of the project and the conclusions achieved. However, the match performed for age and sex of the subjects enrolled in the same cohort should have partially reduced potential bias derived from different patients’ baseline characteristics. Indeed, the patients in the control group did not differ significantly from the experimental group in terms of baseline clinical and demographic variables, including mindfulness inclination and psychopathology, which was mild in both groups. Therefore, it is plausible that many patients declined the experimental intervention due to low motivation to engage in a 20-minute mindfulness practice, as they may not have perceived mild levels of anxiety or depression that would prompt them to seek additional treatment. Conversely, patients who were more physically impaired and with a history of longer hospital LOS more frequently refused TG; these baseline differences may have impacted the final psychological outcomes observed. However, the decision to not take part in the T-MBI proposed might be explained by the fact that they wanted to forget the hospitalization and not be in contact any more with healthcare providers. Additionally, given that the average age in both groups was over 60 years, some patients may have been less comfortable using technology for the intervention.
Moreover, the positive attitude in accepting the T-MBI proposed could have influenced the related results. Besides, the decision to take part in a telerehabilitation intervention is not only a matter of coping inclination, but it is also linked to barriers such as familiarity with technologies, and device availability. 49
Additionally, the pandemic situation did not allow for different preliminary project construction, thus, it seemed not ethically appropriate to intentionally discriminate against potentially beneficial interventions. Furthermore, all the subjects involved executed multiple rehabilitation treatments, with type and intensity dependent on their own specific clinical needs, other than T-MBI, and identifying the single role of the home-based mindfulness intervention in these results is not possible. Although MBIs are usually applied in association with other interventions, and the definition of concomitant therapies was the same for both groups. The multiple interactions with the health-care team of the TG compared to the n-TG may have contributed to T-MBI outcomes; however, all patients were attending rehabilitation interventions, thus, the increased number of contacts with the clinicians might have a partial role. For these reasons, the conclusions derived from this study, even if they require caution, provide relevant information in a pragmatic way.
Clinical Message
Lastly, the application of a remote home-based mindfulness-based intervention as part of a global, tailored, rehabilitation program seems feasible and effective in reducing anxiety, depression, post-traumatic stress disorder symptoms and increasing resilience and self-efficacy in previously hospitalized COVID-19 subjects.
Footnotes
Author Contributions
Conceptualization, S.S. and G.M.; Data curation, S.S., G.M., and L.Z.; formal analysis, G.M and L.Z.; investigation, G.F., N.S., A.B., N.L., F.M., and G.M.; methodology, S.S., A.B., N.L., F.M., and G.M.; project administration, S.S. and G.M; supervision, S.S.; validation, S.S., G.M., and L.Z.; visualization, S.S., G.M., and L.Z.; writing—original draft, G.M and L.Z.; writing—review and editing, S.S., G.F., G.M., L.Z., and L.G.. All authors have read and agreed to the published version of the manuscript.
Availability of Data and Materials
The data that support the findings of this study are available from the corresponding author, SS, upon reasonable request.
Declaration Of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: For this research, S.S. was partially funded by the University of Ferrara (FIRD 2022).
Consent for Publication
NA.
Code Availability
NA.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Committee of Area Vasta Emilia Centro, Regione Emilia Romagna (Italy) (EM66-2022_539/2020/Oss/AOUFe_EM1.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.