
Abstract

Keywords
Surgeon burnout is not a new topic, yet it remains a concerning one. Some reports note that its prevalence is neither slowing down nor stalling [23], while others suggest a plateau or slight decrease [17]. Regardless, burnout among surgeons affects not only individual physicians but also their patients and their loved ones [3]. Emotional exhaustion and depersonalization are hallmarks of burnout identified by the Maslach Burnout Inventory (MBI), a well-respected and used assessment [10]. Burnout can also be defined as a deficit in physical, emotional, and spiritual energy. Five potential contributors to physician burnout include conditioning related to training (eg, workaholism and perfectionism), stresses inherent to practicing medicine, specific job assignments (especially true for surgeons [10,11]), life outside of work, and leadership skills of the immediate supervisor [11]. Burnout in surgeons involves startlingly high rates of depression, anxiety, and suicidal ideation, creating stress on individuals, organizations, and healthcare systems [7,23,31].
In a recent report by Lu and colleagues in this journal, orthopedic surgery resident and faculty burnout at a single orthopedics institution were analyzed [36]. Using samples from both 2019 (n = 148; 79% response rate) and 2023 (n = 76; 40% response rate), they found that about one-third of faculty and residents experienced burnout in 2019; in 2023, the rate for residents remained stable but almost doubled for attendings. Six themes were evaluated: workload, control, reward, community, fairness, and values. Excessive workload was the top burnout contributor across all career stages, followed by lack of job control for residents and fairness for attending. Lu et al reported that the 2019 survey results catalyzed interventions aimed at reducing burnout: (1) to reduce workload there was a consolidation of annual training modules; (2) to achieve greater recognition there was increased research funding based on time spent teaching trainees; and (3) to build community a physician lounge and online access to fitness classes were created. These interventions were determined not to be successful in reducing burnout rates at the 2023 survey time.
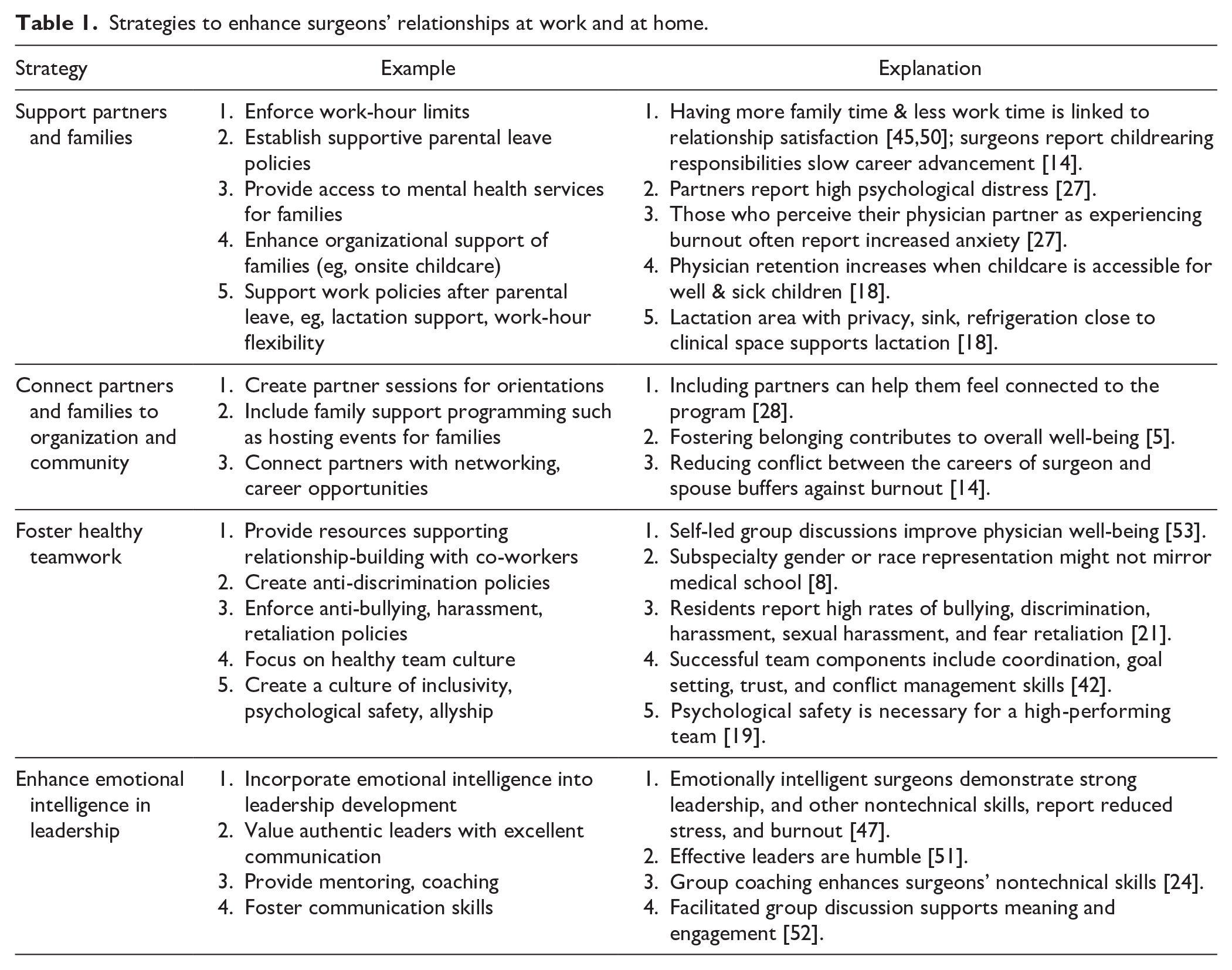
We believe one factor in physician well-being has not received enough attention: relationships (Fig. 1). A recent systematic review demonstrates high levels of anxiety and depression among surgeons [15]. A study using the Impact of Work on Personal Relationships (IWPR), a predictor of anxiety, depression, sleep-related issues, and unsolicited patient complaints, found almost 50% of surgeons identified as having moderate to severe IWPR [49]. Surgeons who have a social community at work and receive support from colleagues experience greater engagement and meaning in their work long after the interactions occur [52]. We propose that surgeons’ relationships at home and at work may be critical factors in their mental health, that relationship support is a missing piece of many organizations’ well-being support services, and that interventions focused on enhancing relationships should be used with other solutions, not as standalone strategies (Table 1). Our team of authors includes an orthopedic surgeon, a research psychologist specializing in social stress and belonging whose partner is a surgical resident, a medical social worker with expertise in systems theory emphasizing understanding individuals in the context of their relationships and environments who is the daughter of a surgeon, and a physician-scientist faculty development dean with expertise in workforce issues including physician retention.
Surgeons’ relationships at work affect relationships at home and vice versa. Both work and home relationships affect surgeons’ well-being, just as surgeons’ emotional and physical states affect relationships at home and work.
Strategies to enhance surgeons’ relationships at work and at home.
Enhancing Relationships at Work
Most research describing surgeon burnout focuses on surgeons’ experiences at work. In a recent survey of gastrointestinal surgeons (n = 604), 77% reported that while they would become a doctor again, less than 50% would either choose surgery or recommend that subspecialty to loved ones [31]. More than two-thirds of participants felt they did not have enough time for their personal lives. Surveyed surgeons noted they were “at the end of their rope” (81%), emotionally drained (74%), and “used up daily” (65%) [31]. These results mirrored Bremner et al’s [6] findings that 50% of surveyed cardiothoracic surgeons (n = 871) “dread coming to work,” 44% said they rarely have sufficient time to spend with family, and 52% reported their level of burnout affected the care they gave patients. Regarding the latter, a recent systematic review confirmed higher physician burnout is related to poorer patient safety [52]. Women surgeons are almost 3 times as likely to feel burnout as men are, even after controlling for race, age, and number of hours worked [32]. Burnout is a concern for not only physician well-being but also patient safety.
A potentially successful target is social interaction at work. A qualitative study by McNeill et al [39] of surgeons (n = 28) found that improving workplace social dynamics could aid in addressing burnout if hospital leaders also worked to improve surgeons’ access to resources for patient care. Participants cited workplace policies, especially on gender equity, as a major concern related to burnout. Interventions affecting social interaction engage the essential human need for belonging [2]. Belonging is the perception of being valued, appreciated, and aligned with the goals or values of a group or institution; it is the inverse of loneliness, the perception of deficits in the quality or quantity of social relationships [43]. Salles et al completed a multicenter study of surgical residents and found that feelings of social belonging had a high positive correlation with their mental and physical health and a strong negative correlation with their risk of attrition [43]. Meaningful relationships in one’s community, in this case professional community, are associated with better health, motivation to learn, and job performance [2]. West et al [52] conducted a randomized trial that showed biweekly facilitated group discussion on shared experiences, mindfulness, reflection, and learning increased physician engagement and decreased feelings of burnout, even a year later. These outcomes were replicated when physicians met every couple of weeks at a local restaurant, sharing a meal and spending the first 20 minutes of the meeting in a self-guided discussion related to values and meaning-making [53].
Although social interactions occur across a spectrum, it may be useful to categorize them as possessing “light” and “dark” aspects (Fig. 2) [51]. On the light or aspirational side, healthy teams [19], along with authentic and emotionally intelligent leaders [40] relate to decreases in surgeon burnout [1]. Light-side interactions involve strengths-based learning interventions, typically identifying a shortcoming and engaging professional development strategies to ameliorate the concern [29]. The dark side of social interaction includes harassment, microaggressions, discrimination, and abuse, all contributors to surgeon burnout [4]. Dark-side interactions involve deficit-based learning interventions; they focus on what learners lack and then engage in punitive consequences in order to shape behavior [29]. Deficit-based learning leads to a lower perception of competence, effort, and intrinsic motivation than strengths-based learning. Both can affect behavior change when used appropriately [29].
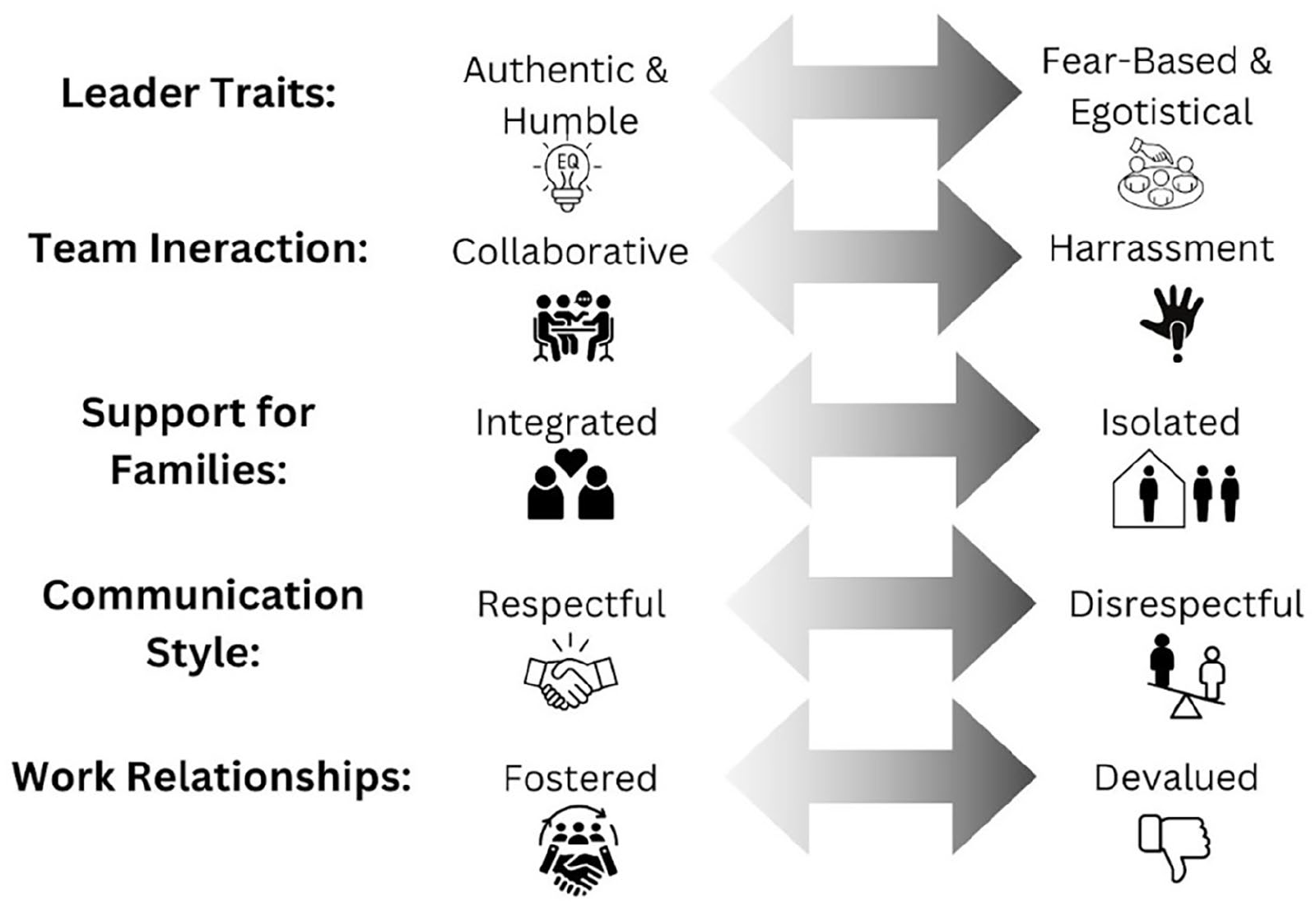
Emotional intelligence and relationship variables have been conceptualized as a “dark vs light” continuum [51]. These are not binary variables but rather conceived as a spectrum.
Exploring the lighter side of social interactions at work, we begin with a focus on healthy teams. Granek et al [25] interviewed surgeons from cardiothoracic, neurosurgery, and ophthalmology subspecialties and 9 countries, finding that healthy teams (a group of compassionate colleagues), straightforward communication, and collaboration as a departmental value were related to greater career satisfaction. They also found decreased career satisfaction was associated with leaders whose actions generate feelings of fear and scarcity, departments experienced as competitive, egotistical colleagues, and surgeons’ feelings of loneliness. The authors propose that effort to foster healthy teams in surgical departments could promote psychological safety and improve workplace culture. Prioritizing professional relationships in surgical departments and focusing on team interactions can also support a decrease in workplace bullying, discrimination, and harassment [8]. When mentorship, allyship, and other positive work relationships are expected rather than suggested, job satisfaction scores increase and feelings of burnout decrease [8]. Surgical residents who have a sense of camaraderie with one another also express higher rates of well-being than those who do not feel safe or supported in their learning environments [54]. Organizations can combat surgeons’ burnout by committing time, space, and resources to building connected teams [41] and prioritizing interpersonal connections [46].
Workplace interactions are also positively affected by leaders creating a culture that values emotional intelligence (EQ). This light-side social interaction shows up in surgeons who receive coaching on authenticity and emotional intelligence, both of which are associated with reductions in depression and burnout [40,48]. Waters et al [51] found surgeons are most likely to connect with leaders interested in introspection, and surgeons’ relationships with supervisors can play a defining role in how they feel at work. A systematic review found that leadership training tends to focus more on cognitive skills than on character and EQ development in leaders [48]. Surgeons with greater insight into themselves and others are less likely to feel burnout, more likely to experience job satisfaction, and more likely to have higher rates of overall well-being than surgeons without these skills [38]. Catalyzing strengths-based programming that focuses more on EQ than cognitive intelligence (IQ) may provide emotional support and resources to surgical departments [4]. Training for leaders on EQ can catalyze positive outcomes in the context of surgical teams and patients’ experiences [51].
Research shows harassment, bullying, microaggressions, and discrimination are correlated with surgeon burnout [9,21,37]. According to Golisch et al [23], “burnout is a culmination of small insults over many years.” Microaggressions (subtle conscious and unconscious insults that catalyze discriminatory and derogatory stereotypes) and mistreatment (any form of discrimination, harassment, or abuse) [8] within the workplace have been studied as factors in surgeon burnout [38], with greater effects for female rather than male surgeons [8,38]. Addressing discrimination and focusing on inclusive excellence is paramount [16]. Deficit-based strategies such as consequences [29] for discrimination and harassment may contribute to a reduction in surgeon burnout [8].
Several individual characteristics relate to surgeon well-being and decreased burnout. One survey of surgeons (n = 348) found that psychological flexibility and resilience were related to surgeons’ mental health [26]. Unlike many personality traits, flexibility and resilience can shift and grow, leading to long-term positive implications for surgeons’ emotional health as individuals and team members [26]. Similarly, mental toughness correlates with life satisfaction; surgeons with higher levels of mental toughness might experience less burnout [33]. Duckworth et al [12] demonstrated the construct of grit, first defined by Angela Duckworth as “sustained and focused application of talent over time,” as inversely correlated to emotional exhaustion and depersonalization in orthopedic surgeons [34]. They propose that focusing on supporting surgeons’ grit might relate to lower burnout scores; measuring grit periodically may serve as a risk assessment, with lower levels representing a higher risk of burnout.
Enhancing Relationships at Home
Strong social bonds are a fundamental human need [5], contributing to resilience and perseverance in the face of adversity and burnout. The most important relationships in the lives of many surgeons are those outside of work, including a spouse or partner and children. Nearly 87% of physicians are or have been married, with a majority of unmarried physicians being in romantic relationships [13] and most surgeons (88%) having children [14]. While often powerful protectors of well-being, these relationships can also be a source of stress and strain for surgeons. A 2011 study of physicians in the United States and the Netherlands found that having a spouse at home is associated with lower stress and burnout, while work getting in the way of family time is related to greater physician stress and burnout [35]. Studies of otolaryngology chairs and obstetrics and gynecology chairs have found links between low spousal support (eg, not listening to work-related problems or understanding about extra work hours) and greater emotional exhaustion and depersonalization [20,30]. Dyrbye et al [14] surveyed 7134 surgeons and found that work-home conflicts, high hours worked per week, and resolving work-home conflicts in favor of work are major drivers of burnout. They found that women surgeons were particularly likely to experience work-home conflict, that 1 in 5 surgeons reported conflict between their career and their spouse’s career, and that 23% of surgeons reported childrearing responsibilities slowed their career advancement. According to a recent survey of physicians (n = 253), the top contributors to marital distress were job stress, work hours, children, and sex, while strong communication, finances, and children were linked to marital stability [13]. These findings highlight the need for supportive family dynamics to improve physicians’ well-being.
Spouses and children are also affected by physician burnout. A study of 203 physicians’ spouses found that nearly 70% report moderate to severe anxiety and depression and 60% report secondary trauma symptoms [27]. There was a link between spousal symptoms and their perception of burnout in the physician partner; individuals who reported higher burnout in their partner also reported more severe psychological symptoms in themselves. An investigation of the spouses of orthopedic residents and attending physicians found that many, reported psychological distress, with 18% of resident spouses and 10% of faculty spouses affected [44]. Spouses who worked outside the home (68%) reported higher marital satisfaction but also high levels of emotional exhaustion and depersonalization. Supporting the spouse of the surgeon in the spouse’s interests, career, and well-being appears to be an important factor in work satisfaction for the surgeon [44]. In a recent survey, a majority of the spouses of cardiothoracic surgeons reported their partner’s career had a moderate to severe impact on the family (63%), the surgeon’s schedule left little to no time for family (63%), and they rarely had time for intimacy (51%) [50]. Nearly 1 in 4 spouses reported that interactions at home with their surgeon spouse were rarely calm and good natured. Perhaps the experience of burnout and distress is bidirectional between spouses, suggesting that supporting their spouses may support surgeons themselves. A survey of partners of physicians (n = 56) conducted by the founder of The MedCommons, an organization aimed at supporting physicians’ partners and families, found the partners reported they were lonely and the organizations had not helped them connect with other partners of physicians (Fig. 3) (personal communication, Elizabeth Landry, November 18, 2024). These examples suggest the need for interventions that are inclusive of physicians and their families.
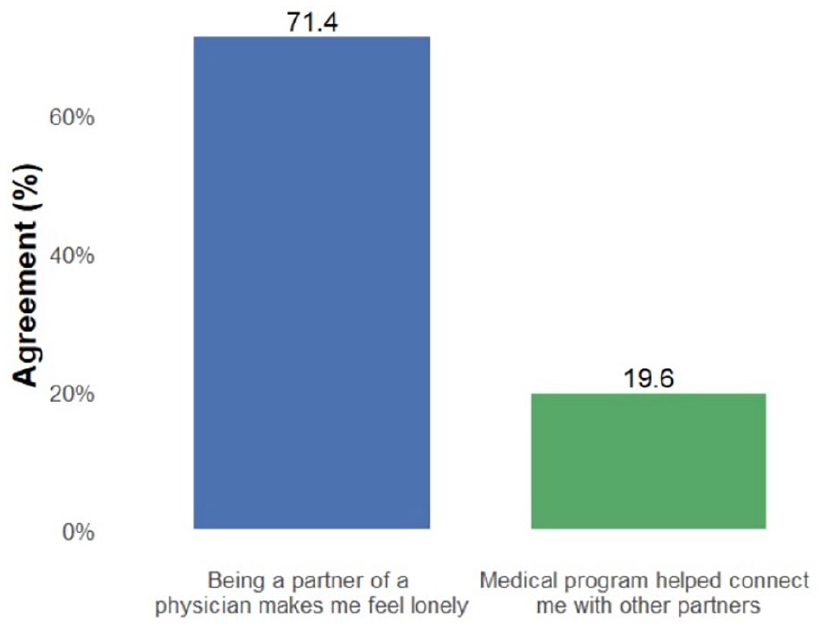
An online survey by MedCommons of the partners of physicians (n = 56) (personal communication, Elizabeth Landry, November 18, 2024).
One avenue to improving relationships may be to increase the quantity and quality of time spent together. The number of minutes spent awake together directly predicted marital satisfaction in physicians’ marriages [45]. Burnout and distress for families of cardiothoracic surgeons were lowest when physicians worked 60 hours per week, suggesting that work-hour limitations may be a protective factor [50]. Institutions can also support surgeons and their families through programs dedicated to family support. Recruitment and retention programs that are the most successful consider family needs, career opportunities for spouses, and community building for the physician and family [28]. For example, Hale et al [28] suggest strategies such as incorporating a spouse and significant other session into residency orientation or inviting spouses and partners to social events to foster a sense of belonging; it may also be critical to offer access to family counseling and mental health services. We believe that effective interventions incorporate the bidirectional relationship between stress at home and stress at work to promote surgeon well-being.
In conclusion, we suggest that social interactions and relationships at work and at home are crucial considerations in addressing surgeon burnout. Interventions that are strengths-based (eg, coaching, mentoring, and developing healthy teams) and deficit-based (eg, consequences for discrimination and policies to combat harassment) have been shown to impact behavior. Strengths-based interventions tend to lead to more positive feelings and outcomes for the participant. Similarly, improving personal relationships and minimizing work-home conflicts can alleviate the stressors that contribute to burnout. We hope that future research will shed light on these components of surgeon burnout. Physicians, their families, their patients, and healthcare organizations all stand to benefit.
Supplemental Material
sj-pages-4-hss-10.1177_15563316241313364 – Supplemental material for Surgeon Burnout and Relationships: A Missing Component in the Ongoing Conversation
Supplemental material, sj-pages-4-hss-10.1177_15563316241313364 for Surgeon Burnout and Relationships: A Missing Component in the Ongoing Conversation by Rebecca E. Glavin, Emily M. Silver, Steven L. Frick and Julie K. Silver in HSS Journal®
Supplemental Material
sj-pdf-1-hss-10.1177_15563316241313364 – Supplemental material for Surgeon Burnout and Relationships: A Missing Component in the Ongoing Conversation
Supplemental material, sj-pdf-1-hss-10.1177_15563316241313364 for Surgeon Burnout and Relationships: A Missing Component in the Ongoing Conversation by Rebecca E. Glavin, Emily M. Silver, Steven L. Frick and Julie K. Silver in HSS Journal®
Supplemental Material
sj-pdf-2-hss-10.1177_15563316241313364 – Supplemental material for Surgeon Burnout and Relationships: A Missing Component in the Ongoing Conversation
Supplemental material, sj-pdf-2-hss-10.1177_15563316241313364 for Surgeon Burnout and Relationships: A Missing Component in the Ongoing Conversation by Rebecca E. Glavin, Emily M. Silver, Steven L. Frick and Julie K. Silver in HSS Journal®
Supplemental Material
sj-pdf-3-hss-10.1177_15563316241313364 – Supplemental material for Surgeon Burnout and Relationships: A Missing Component in the Ongoing Conversation
Supplemental material, sj-pdf-3-hss-10.1177_15563316241313364 for Surgeon Burnout and Relationships: A Missing Component in the Ongoing Conversation by Rebecca E. Glavin, Emily M. Silver, Steven L. Frick and Julie K. Silver in HSS Journal®
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Human/Animal Rights
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration.
Informed Consent
Informed consent was not required for this commentary.
Required Author Forms
Disclosure forms provided by the authors are available with the online version of this article as supplemental material.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.