
Abstract
Background
Mindfulness-based stress reduction (MBSR) has been shown to be beneficial for adults with inflammatory bowel disease (IBD), but little is known about its use in pediatric IBD.
Objective
This pilot study aimed to assess the feasibility and acceptability of an MBSR program delivered by live-video during the COVID-19 pandemic for youth with IBD.
Methods
Four cohorts of an 8-session MBSR program were conducted via a HIPAA-compliant, video-conferencing platform from winter 2021 to spring 2022. Mixed-methods data were collected through semi-structured focus groups, study-specific surveys, attendance data, and self-reported health-related quality of life (HRQOL) measures.
Results
Forty-six participants enrolled across 4 cohorts. Participants were 64% female, Mage=14.1 years, 36% non-Latinx White; most had Crohn’s disease (81%). Participants attended an average of 7.6 of 8 classes, with 69% attending all 8 classes. Majority of participants (77%) were satisfied or very satisfied with the program. Three themes emerged from the focus groups (n=27): (1) IBD-specific benefits: reduced stress (which some identified as an IBD trigger) and connecting with IBD peers; (2) mental health benefits; and (3) virtual MBSR was feasible and well-liked, but challenges were present. Pre- vs post-program data (n = 30) showed statistically significant improvements in HRQOL (P = 0.04), HRQOL social functioning (P = 0.03), and perceived stress (P < 0.01).
Conclusion
This pilot study of live-video MBSR for youth with IBD shows feasibility and acceptability, high rates of attendance and satisfaction, and potential benefits in quality of life and stress. MBSR is a potential adjunctive therapy in pediatric IBD.
Keywords
Introduction
Inflammatory Bowel Disease (IBD) is a chronic inflammatory gastrointestinal condition often diagnosed in the pediatric population that involves life-long care and treatment. When compared with healthy peers, youth with IBD are at increased risk of developing behavioral and emotional dysfunction as well as impaired self-esteem. 1 Children with IBD are at increased risk for psychosocial co-morbidities such as depression and anxiety, worsened quality of life, and less effective coping skills when compared to healthy population controls.2,3 These factors can greatly affect IBD patients’ health-related quality of life (HRQOL). Furthermore, IBD flares have been associated with various psychological triggers, including stress, negative affect, and major life events4-6 while low stress levels and engaging in active coping strategies have shown fewer relapses of disease. 7 Psychological stress also drives intestinal inflammation. 8 Therefore, targeting the stress response could be a potential avenue for adjunctive therapy in children with IBD.
While a variety of brain-gut therapies exist to modulate stress, Mindfulness-based stress reduction (MBSR) is one such intervention that has been effective at targeting the stress response. 9 MBSR, developed by Jon Kabat-Zinn at University of Massachusetts Medical Center in the 1970s, consists of an 8-week group program facilitated by a trained instructor to enhance participants’ innate capacity for non-judgmental, present-focused awareness. 10 MBSR directly focuses on 2 primary mechanisms to decrease stress: attention monitoring (focusing awareness on current thoughts, sensations, emotions) and acceptance (response without judgement or avoidance).11,12 MBSR and mindfulness interventions have been shown to be a beneficial therapy in adults with anxiety, depression, and IBD as well as in other pediatric chronic diseases.13-17 Benefits of the program may be due, in part, to findings that MBSR has an effect on decreasing the stress response physiologically as well as psychologically, including lowering cortisol, blood pression, pro-inflammatory cytokines and improving autonomic nervous system balance, and helping decrease inflammation.18-20
Ahola Kohut et al published the first mindfulness-based intervention trial in adolescents with IBD investigating the feasibility and acceptability of an 8-week mindfulness-based intervention program, consisting of two-hour,
Methods
Study Design
We designed a single-center, mixed-methods, non-randomized prospective pre/post pilot feasibility and acceptability trial at a large referral quaternary care pediatric IBD center. Our study was approved by the Children’s Hospital of Philadelphia’s Institutional Review Board.
Participants were approached via various recruitment methods including: clinics, IBD patient education days, the hospital’s research recruitment website, and email to the IBD patient listserv. Those between the ages of 12-19 years with a confirmed diagnosis of IBD (Crohn’s disease/ulcerative colitis/IBD-U) who had been seen for care of IBD in the last 6 months were eligible to participate. Participants also needed to have the ability to attend the live-video sessions and complete baseline and follow-up surveys with adequate equipment (computer, internet, audio/video capability) as well as English language proficiency (reading and speaking). In addition, participants were encouraged to be comfortable being on-camera for the duration of the classes.
Participants were excluded if they had severely active IBD based on Physician’s Global Assessment (PGA) or requiring hospitalization or surgery to treat IBD, needing biologic induction, using prednisone dose > 20 mg daily, or taking antibiotics 3 months prior to the start of intervention. Those with a diagnosis of serious mental illness, pervasive developmental disorder, or intellectual disorder as determined by medical chart review or patient/caregiver report, had initiated or changed dosages of psychotropic medications in the last 3 months, or were part of another clinical trial involving an intervention were excluded. Those who were already regularly (weekly or more) practicing specific mind-body techniques (yoga, breath work or pranayama, biofeedback, hypnosis, guided imagery, meditation) were also excluded.
Written informed consent was obtained from participants (if aged >18 years old) and/or parents/guardians (for participants <18 years old) for those who met eligibility criteria and enrolled in the study. Assent was obtained from those participants less than 18 years old.
Procedures
Four cohorts of classes were conducted between Spring 2021 and Spring 2022. Participants were asked to contact the study team if any medication were changed, and chart reviews were also performed at the end of the 8-week sessions to assess for clinical status change during the study period that would exclude them from analysis. In addition, they were asked on their post-intervention MBSR questionnaire of any changes to their medication regimen. We tracked participant enrollment, session attendance, and program evaluation. We examined both quantitative and qualitative measures. Data on psychosocial functioning, IBD disease activity, and HRQOL was collected at baseline (T0), post-intervention (T8 weeks), and 3 months post-intervention (T20 weeks) using REDCap. Additionally, a focus group was conducted at the end of each cohort, for a total of 4 focus groups, to qualitatively assess feasibility, acceptability, and perceived benefits and challenges.
Intervention
The live-video MBSR program was taught by an expert instructor with experience with youth with chronic disease and conducted via an IRB-approved, HIPAA-compliant web conferencing platform, BlueJeans. Prior to the first class, participants were mailed the adapted MBSR class handbook, used in previous research.15,18 For each cohort, 8 classes were conducted once weekly on the same day and time every week, and the participants received email reminders prior to each class to encourage and increase attendance. Participants were guided through the sessions by the instructor, with modifications made as appropriate at the discretion of the instructor to enhance learning and participation. Each session was structured similarly: introductions, beginning mindfulness exercises, reflection on the content previously covered, didactic/experiential introduction to the week’s content, small group discussion, experiential mindfulness technique, and small/large group reflection followed by outlining the home exercises for the following week. Each class in the 8 week session had different areas of focus on various MBSR concepts and practices, e.g., mindful body awareness (gentle yoga, body scan), mindful attention (sitting meditation), walking meditation, present focus (using breath as an anchor).
Outcome Measures
Primary Outcomes: Feasibility and Acceptability
Feasibility was measured by recruitment, withdrawal rate, and class attendance, which was tracked via an enrollment log. Acceptability measures included participation and completion in group sessions and satisfaction with the intervention, measured via focus group analysis and a study-specific questionnaire. Focus group data also assessed perceived challenges and benefits of the intervention.
Secondary Outcomes
Quality of life was assessed via Impact-III and the Pediatric Quality of Live Inventory (PedsQL). Impact-III is a validated, disease-specific pediatric questionnaire that measures HRQOL in pediatric IBD patients age 9-17 years.22,23 PedsQL is a validated pediatric questionnaire that measures general HRQOL in children ages 8-17 years.24,25 The total score and emotional and social functioning scales were utilized given their relevance to the focus of the MBSR group intervention.
Stress was measured using the Perceived Stress Scale (PSS) and the PROMIS Pediatric Short Form Psychological Stress Experiences (8a). The PSS is a validated and widely used 10-item questionnaire that assesses the perception of stress in one’s life. 26 The PROMIS Psychological Stress Experiences form is a validated 8-item questionnaire that assesses children’s and adolescents’ thoughts or feelings within the context of their environment and/or internal challenges.
Data capturing disease activity were collected using the sCDAI and PUCAI, both of which are validated disease activity indices used for pediatric Crohn’s disease and ulcerative colitis, respectively.27,28
Statistical Analysis
Demographics, feasibility data, and self-report of intervention acceptability were assessed via descriptive statistics. To assess changes in secondary outcomes at pre-, post-, and 3-month post-MBSR intervention, repeated measures analyses of variance (ANOVAs) with planned contrasts were conducted, with time entered as a within-subjects variable and group entered as a between-subjects variable. Pre-MBSR intervention values were used as the comparison group in planned contrast analyses. Statistical significance was determined by a 2-sided significance level of P < 0.05. Participants who met exclusion criteria were omitted from secondary analyses to reduce the likelihood of misinterpretation of results, although their focus group data were retained for acceptability and feasibility analyses. Focus group audio-recordings were transcribed verbatim using a professional transcribing service. The transcripts were de-identified and independently reviewed by 2 of the investigators (SV and LA) using the constant comparative approach associated with grounded theory. Each investigator developed codes which were then organized into categories and then into themes; member-checking and debriefing with the other investigators was done to verify our themes.
Results
Demographics
Demographics (N = 36 Participants)

aParticipants were allowed to provide multiple responses.
PUCAI: Pediatric Ulcerative Colitis Activity Index.
sCDAI: Short Crohn’s Disease Activity Index.
Baseline Characteristics of Each Cohort

CD: Crohn’s disease.
PedsQL: Pediatric Quality of Life Inventory.
PSS: Perceived Stress Scale.
PROMIS-Stress: PROMIS Pediatric Short Form Psychological Stress Experience (8a).
Primary Outcomes
Feasibility
Recruitment and Retention: 46 participants were enrolled between Spring 2021 and Spring 2022. Ten participants withdrew from the study, with the most common reason related to scheduling conflicts. Two participants withdrew due to difficulties maintaining interest and/or concentration with the virtual format of the intervention. The final sample consisted of 36 participants (Spring 2021: n=13; Summer 2021: n=10; Fall 2021: n=6; Winter 2022: n=7).
Attendance: Participants attended 7.58 classes out of 8 classes on average. Of the 36 total participants, 25 (69.4%) attended all 8 MBSR sessions. Eight participants (22.2%) missed 1 session only. The remaining 3 (8.3%) participants attended 5 or 6 sessions. Participants were present for the entire two-hour duration of each session for 86.8% of all attended sessions.
Technological difficulties: The majority (77.8%) of participants did not experience any audio or video difficulties during the course of the MBSR intervention. For those experiencing technological challenges, 16.7% did not utilize video features as intended (either due to technological challenges or choosing to leave camera off) for at least 1 session; 8.3% encountered difficulty with audio features for at least 1 session.
Acceptability
Focus Group Themes for MBSR Intervention (N = 27)
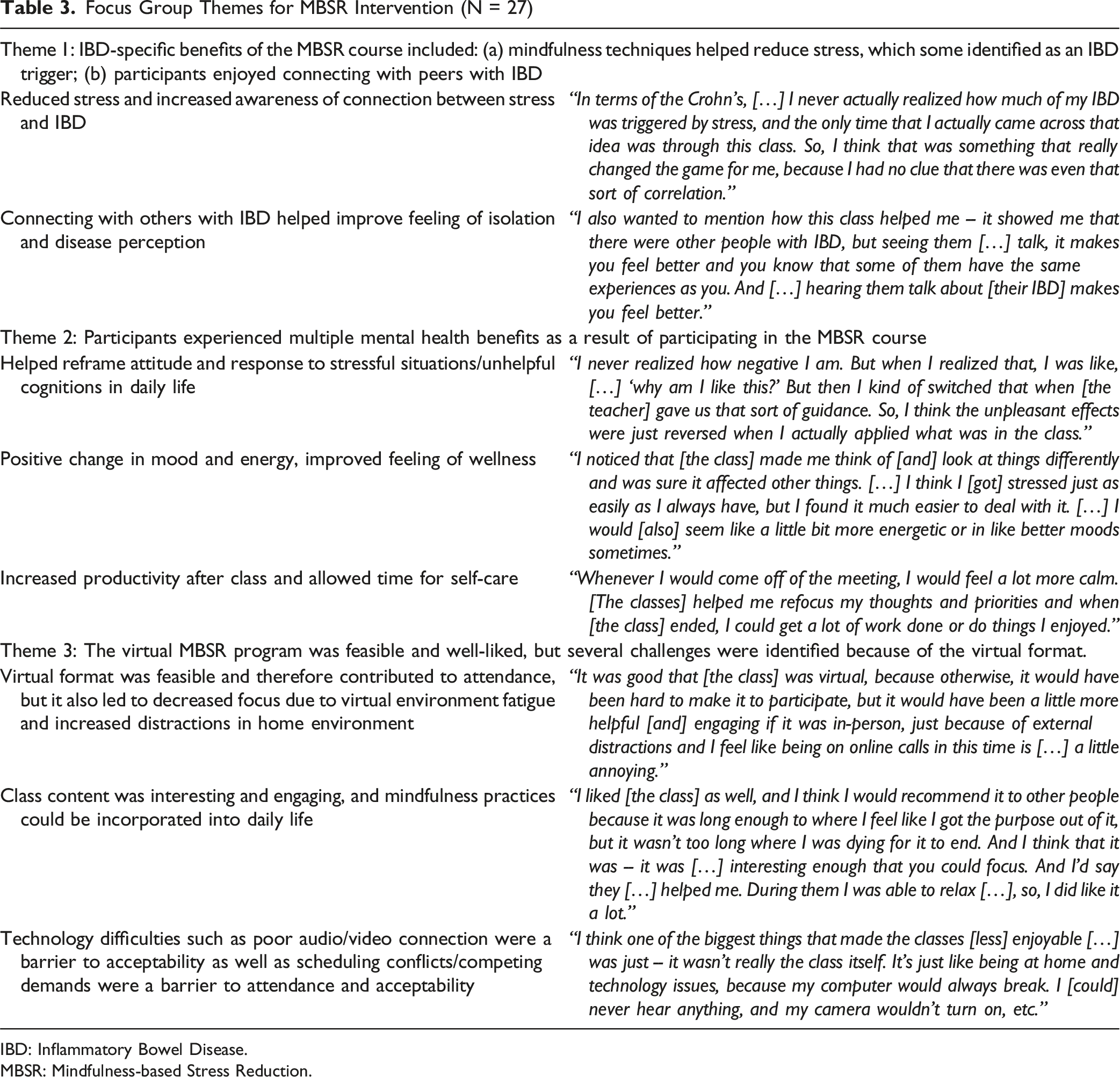
IBD: Inflammatory Bowel Disease.
MBSR: Mindfulness-based Stress Reduction.
Focus Group Participant Identified Solutions to Improving Feasibility/Acceptability

Self-report: In line with focus group data, 77.1% of participants reported they were satisfied or very satisfied with the MBSR intervention; only 2 (5.7%) participants expressed dissatisfaction. Similarly, 68.6% of participants reported they would be likely or very likely to recommend the MBSR program to others, with an additional 28.7% reported a neutral opinion; only one participant reported being unlikely to recommend the intervention.
Secondary Outcomes
Secondary Outcome Repeated Measures ANOVAs With Planned Contrasts (Baseline as the Comparison Group)
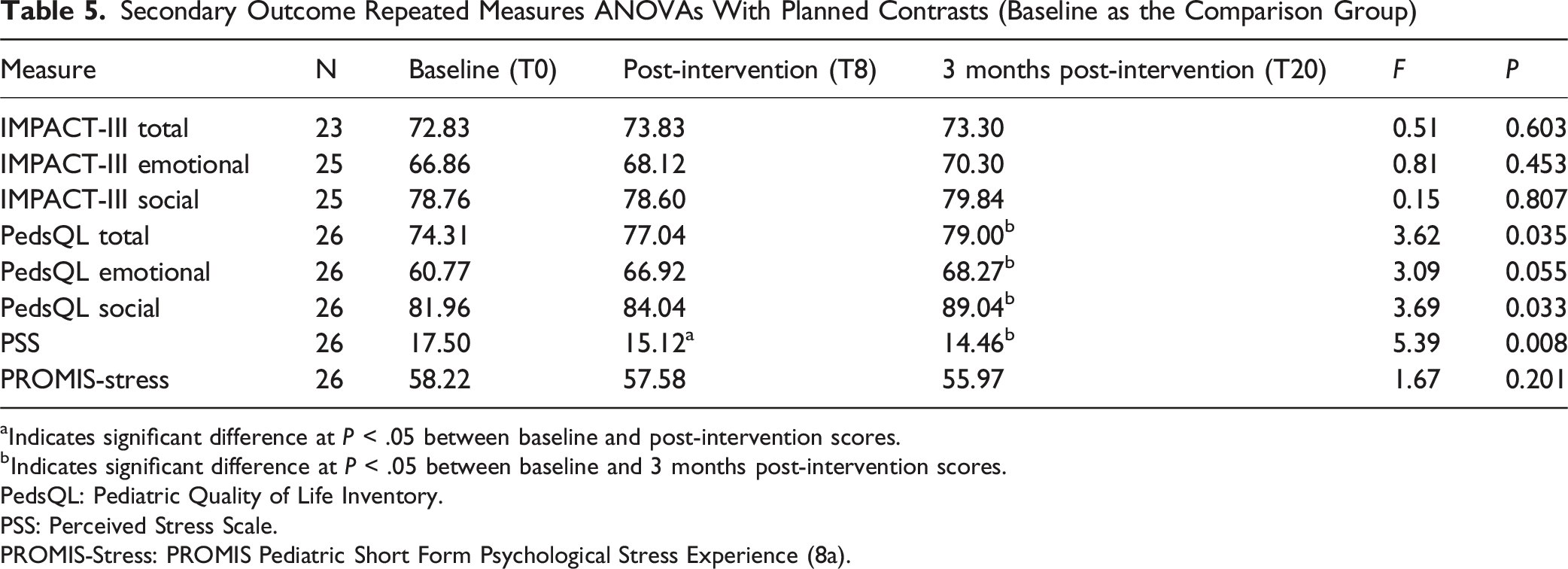
aIndicates significant difference at P < .05 between baseline and post-intervention scores.
bIndicates significant difference at P < .05 between baseline and 3 months post-intervention scores.
PedsQL: Pediatric Quality of Life Inventory.
PSS: Perceived Stress Scale.
PROMIS-Stress: PROMIS Pediatric Short Form Psychological Stress Experience (8a).
Discussion
Virtual adaptation of MBSR is a feasible and acceptable intervention in youth with IBD. Our study had a high retention rate of 78% (36 participants remained in the study out of the 46 enrolled) and nearly 70% attended all 8 classes with 90% attending 7 of the 8 classes, indicating high interest and engagement in the intervention. The main barrier to attendance was scheduling conflicts, suggesting that external factors to the intervention prevented participation. Our qualitative data further supports this; focus group results showed that the virtual nature of the intervention increased the likelihood of participation in patients who would otherwise not have considered enrolling in such an intervention. Therefore, our study suggests that virtual MBSR intervention may be more feasible than in-person formats, potentially removing a barrier that leads to decreased engagement and retention rates in similar MBSR interventions. 21
Two of the sessions were conducted during Spring-Summer 2021 (closer to the COVID-19 pandemic while most children were in virtual school), it is important to note that the last 2 sessions were conducted in Fall-Winter 2021-2022 when most participants returned to in-person school/activities. This argues that the results are still relevant post-pandemic as at least half the sessions were conducted in a post-pandemic environment. However, as the COVID-19 pandemic improved, we saw a decrease in enrollment of participants, likely due to a rise in in-person activities conflicting with ability to attend classes. Weekend classes could be considered as a way to combat this, though timing of such group interventions might pose an enrollment challenge given the wide variability in adolescent schedules. Furthermore, there has been a notable increase in both mental health disorders and the incidence of IBD post-COVID-19-pandemic.29-32 Increase in these disorders argues the need for further adjunctive therapies such as MBSR to be incorporated into traditional treatment paradigms to help patients, making our results applicable despite the intervention being conducted partly during the pandemic.
Participants reported positive experiences with the course content and were engaged in the sessions as evidenced by their commitment to stay for the duration of the two-hour courses. Our qualitative data suggest the participants experienced several noted benefits, including reducing stress, which can be a trigger of IBD-related symptoms for some. Recognizing that their emotional status and mood could affect their GI symptoms is an important connection to make for many patients with chronic GI illnesses such as IBD and can lead to empowerment over their body and their ability to manage their condition. Overall, a majority of the participants would recommend MBSR to other youth with IBD, indicating that they saw value and benefit from participating in the intervention.
Despite interesting and enjoyable intervention content and noted benefits (e.g., stress reduction, community formation with others with IBD), some participants acknowledged that the nature of the virtual format led to decreased engagement. Class length was cited as a barrier to engagement; future interventions could modify class content to be shorter, especially in the virtual environment, to help increase satisfaction and engagement. It is important to note that this intervention occurred at varying time points of the COVID-19 pandemic when virtual environment fatigue was at a high, potentially leading to decreased participant engagement.
Secondary outcomes were notable for improved PSS scores at both follow up time points (post-intervention and 3-month follow-up), suggesting that the virtual MBSR intervention had an acute and longer-term effect on stress. Given that stress has been implicated in disease exacerbation of IBD, 33 the MBSR intervention may offer benefits for physical health. The focus group data highlighted that participants noted a connection between stress levels and their GI symptoms and that the intervention provided adolescents with tools to help mitigate stress and respond to situations differently. This dovetails with the objective difference observed in the PSS scores pre-and-post intervention, further cementing the value to be potentially gained from this intervention.
Our data also showed statistically significant improvement in overall quality of life from pre-intervention to 3-month post intervention as evidenced by the PedsQL measure. Further sub-analysis revealed significant improvement in the emotional and social functioning in the PedsQL questionnaire. While this may support that the MBSR intervention improves overall HRQOL, it is also possible that participants’ experienced improvements due to other factors (e.g., easing of pandemic restrictions, returning to more active lifestyles), although we did not see time X cohort interactions.
While MBSR is one of many brain-gut behavior therapies (BGBT) available, it is important to acknowledge there are other therapies such as CBT or hypnotherapy. 9 However, the advantages of our intervention over other forms of BGBT are several: the group format, virtual nature, and generalizability of the benefits to other aspects of life. For example, one of the major themes was the perceived camaraderie achieved through interacting with others with IBD that some other BGBT may not offer. However, it is important to screen patients prior to participating in virtual interventions for any serious/severe psychiatric co-morbidity or severe IBD to avoid harm. Therefore, characteristics of each patient should be considered when recommending various BGBT but for those who may benefit from group interactions in a virtual environment, interventions such as our live-video MBSR might be a feasible and acceptable option.
Limitations and Future Directions
While the results of this study indicate MBSR could be a potentially advantageous adjunctive therapy for children with IBD, there are limitations to the findings. First, the aim of this study was to assess feasibility and acceptability of a virtual adaptation of an already well-studied intervention. Therefore, the study was not powered adequately to detect statistically significant changes in the secondary outcomes. Despite this, we observed improvements in psychosocial functioning in line with other studies assessing this intervention suggesting that these findings are relevant. Additionally, the uncertainty of the COVID-19 pandemic should also be considered as a limitation in regard to the generalizability of our findings as 2 of the cohorts happened earlier in the course of the pandemic when virtual platform use was high while the latter 2 cohorts had much higher return to in-person activities/school.
The cohort was also overall ethnically/racially homogenous and the lack of Black, Latinx, and/or multiracial adolescents is another important limitation to consider. Equitable access to virtual interventions may also have limited interest/enrollment in the intervention and future iterations should consider offering support for reliable internet access/private space to attend sessions. Our study did not have an active control group and only included those with low baseline disease activity level. Future studies should consider an active control group or a waitlist control group and include participants with varying disease activity to assess if the changes were due to MBSR intervention, low disease activity, or relatively low starting baseline stress levels/symptoms. Future directions could include stool collection to examine the impact of the intervention on the gut microbiome and metabolome, as previous research has found higher perceived stress associated with significant differences in the gut microbiota and metabolome when compared to lower perceived stress. 34
In summary, our study showed that a virtual based MBSR program was highly acceptable and feasible in youth with IBD. Given the risk of mental health co-morbidities and the role of stress in IBD, providers should consider offering a holistic approach to treating IBD that includes stress management techniques. Stress reduction through MBSR could serve as a potentially helpful adjunctive therapy for youth with IBD and high psychological stress levels.
Footnotes
Ethical Considerations
We received approval from the Children’s Hospital of Philadelphia’s Institutional Review Board (IRB) for this study.
Consent to Participate
Written informed consent was obtained from participants (if aged >18 years old) and/or parents/guardians (for participants <18 years old) for those who met eligibility criteria and enrolled in the study. Assent was obtained from those participants less than 18 years old.
Author Contributions
Srisindu Vellanki, MD (SV). SV helped conceptualize and design the study. SV also conducted the focus groups and analyzed the focus group data. SV co-wrote the manuscript with Christina Holbein, helped edit, and finalize the manuscript. Christina Holbein, PhD (CH) helped conceptualize and design the study, analyzed the quantitative outcomes, co-wrote the manuscript, and helped edit, and finalize the manuscript. Adoma Boateng, BA (AB) contributed to conducting the study procedures. Naomi Pressman, MS RD (NP) contributed to conducting the study procedures. Jacqueline Kirsch, BS (JK) contributed to conducting the study procedures. Erica Sibinga, MD MHS (ES) helped conceptualize and design the study as well as helped edit and finalize the manuscript. Maria Mascarenhas, MBBS (MM) helped conceptualize and design the study as well as helped edit and finalize the manuscript. Lindsey Albenberg, DO (LA) helped conceptualize and design the study, analyzed the focus group data, as well as helped edit and finalize the manuscript. All authors approved the manuscript content and accepted for publication.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by the Children’s Hospital of Philadelphia, Division of Gastroenterology, Hepatology and Nutrition.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.