
Abstract
Background
Triphala, a classical polyherbal formulation in Ayurvedic medicine, has traditionally been used for its diverse therapeutic properties, particularly its antioxidant, anti-inflammatory, and immunomodulatory effects.
Objective
This study aimed to evaluate changes in oxidative stress, antioxidant activity, and systemic inflammation following Triphala supplementation in individuals with post-COVID-19 condition.
Methods
Seventy-four participants (aged 18-53 years) with a history of COVID-19 were enrolled in a preliminary randomized, double-blind, placebo-controlled trial. Participants were randomly assigned to receive either placebo (n = 37) or Triphala (1000 mg/day; n = 37) capsules, taken 5 days per week for 8 weeks. Biomarkers assessed included malondialdehyde (MDA), protein carbonyl, superoxide dismutase (SOD), interferon-gamma (IFN-γ), and tumor necrosis factor-alpha (TNF-α), measured before and after supplementation.
Results
In the Triphala group, MDA (P = 0.026), protein carbonyl (P = 0.017), IFN-γ (P = 0.038), and TNF-α (P < 0.001) levels significantly decreased, while SOD activity increased (P = 0.008). In the placebo group, only SOD activity showed a significant increase (P < 0.001). However, no statistically significant differences were observed between the two groups in any of the primary outcomes.
Conclusion
Triphala supplementation may help reduce oxidative stress and systemic inflammation in individuals with post-COVID-19 condition. Future studies with higher doses or longer treatment durations are recommended to confirm and extend these findings.
Introduction
The COVID-19 pandemic has significantly impacted global health. Typically, COVID-19 presents as a mild upper respiratory illness caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). In severe cases, the virus can extend beyond the respiratory system and affect other organ systems. 1 Antiviral innate immunity includes both cellular and humoral components such as interferons and chemokines. A breakdown of this system impairs the body’s ability to control viral replication. 2
A growing body of evidence shows that individuals with COVID-19 may experience persistent symptoms following acute infection, including fatigue, dyspnea, and cognitive dysfunction—a condition commonly referred to as post-COVID-19 condition. This complication has the potential to become a significant global health issue, 3 as oxidative stress plays a critical role not only in the pathophysiology of COVID-19 but also, presumably, in post-COVID-19 condition. Moreover, inflammation and oxidative stress mutually exacerbate one another, leading to systemic hyperinflammation and coagulopathy in affected individuals. 4
Supported by the World Health Organization, traditional medicine has played a meaningful role in health remedies for people with COVID-19. Triphala (from Sanskrit: tri = three, phala = fruits), consisting of Emblica officinalis (E. officinalis), Terminalia chebula (T. chebula), and Terminalia bellerica (T. bellerica), is a polyherbal formulation used in Ayurvedic medicine to promote longevity and rejuvenation across all age groups. 5 Due to its rich content of polyphenols, flavonoids, and vitamin C, Triphala has been recognized for its effectiveness in disease prevention and health promotion. 6 For instance, a recent systematic review suggests that Triphala may improve lipid profiles, blood glucose levels, body weight, body mass index, and waist circumference under specific conditions. 7 Furthermore, studies have confirmed Triphala’s free radical scavenging capabilities, along with its antioxidant, anti-inflammatory, and immunomodulatory properties. 5
In addition to the use of modern medicine, seeking comprehensive knowledge regarding the therapeutic use of traditional medicine for the treatment of people with COVID-19 could open a window into Triphala’s clinical benefits and applications. Furthermore, positive findings on the topic could lead to significant means of attenuating the post-COVID-19 condition burden, thus reducing other burdens on personal and overall health. Accordingly, we sought to determine changes in oxidative stress and inflammatory biomarkers in individuals with post-COVID-19 infection following Triphala supplementation. Our hypothesis was that Triphala supplementation would improve oxidative stress and inflammation in those with post-COVID-19 condition.
Materials and Methods
Participants
This study was a preliminary randomized controlled trial conducted in 78 men and women with post-COVID-19 condition in Chonburi Province, Thailand. The sample size was calculated using a standard formula for comparing the mean values of two groups. Based on a study by Panahi et al., 8 participants who were supplemented with 1 g/day of curcuminoids for 8 weeks had reduced levels of malondialdehyde (MDA) to 15.62 ± 2.59 μmol/L, compared to 20.16 ± 3.11 μmol/L in the placebo group. With an α error of 0.05 and a β error of 0.20, the estimated sample size was 35 per group. After accounting for a 10% dropout rate, the final sample size was set at a minimum of 38 participants per group. This calculation was justified by the shared phytochemical properties of curcuminoids and Triphala, both of which contain polyphenols and antioxidants known to scavenge free radicals and reduce lipid peroxidation. Accordingly, Triphala was expected to exert a comparable biological effect on MDA levels, supporting the use of the curcuminoid study effect size for power analysis.
The inclusion criteria were: (a) having post-COVID-19 symptoms for at least four weeks, including fatigue, headache, cognitive difficulty, hair loss, or dyspnea (symptoms worsened by exertion or concentration); (b) aged 18-59 years; and (c) having a normal body mass index (BMI 18.5-24.9 kg/m2). Exclusion criteria included: (a) regular physical activity (>150 minutes per week or >2 sessions per week); (b) regular consumption of dietary supplements (e.g., vitamins, antioxidants, herbs); (c) regular smoking or alcohol consumption (≥1 time per week); (d) food allergies, particularly to E. officinalis, T. chebula, or T. bellerica; (e) having any chronic or systemic illnesses, including hypertension, diabetes, cardiovascular, respiratory, endocrine, neuromuscular, musculoskeletal, liver, renal, immune, infectious diseases, or cancer; (f) participants presenting with signs of acute infection (e.g., fever, hyperpnea, dyspnea, palpitations) were also excluded.
To ensure a degree of homogeneity in symptom severity at baseline, all participants were assessed using a standardized symptom checklist for post-COVID-19 condition prior to randomization. Symptom severity for fatigue, dyspnea, cognitive dysfunction, and other commonly reported symptoms was rated on a 5-point Likert-type scale (0 = Not at all, 1 = A little bit, 2 = Somewhat, 3 = Quite a bit, 4 = Very much). Lower scores indicated milder or less frequent symptoms, whereas higher scores reflected greater severity. Participants with extreme symptom severity (e.g., requiring medical support or hospitalization) were excluded.
Withdrawal criteria were: (a) development of adverse symptoms related to the supplement (e.g., regular nausea, vomiting, dizziness, or syncope); (b) failure to consume at least 80% of the prescribed supplement; or (c) voluntary withdrawal or requirement to terminate participation for any reason.
Participant Screening
Screening included the use of a COVID-19 checklist (covering infection frequency and recovery time) and health questionnaires capturing general information, medical history, exercise habits, supplement use, and mental health. Baseline physical and physiological data were collected, including height, body mass, BMI, blood pressure, pulse rate, and temperature. To assess potential allergic reactions, all participants consumed one 500 mg capsule of Triphala at screening.
Ethics Statement
All participants provided written informed consent after receiving detailed explanations—both verbal and written—of the study objectives, procedures, risks, and benefits. The study protocol was reviewed and approved by the Human Ethics Committee of Burapha University (IRB1-050/2566) and registered on ClinicalTrials.gov (NCT06208761).
Experimental Protocol
After screening, 78 participants were randomly assigned to either the placebo group (n = 38) or the Triphala group (n = 40) using simple random allocation via IBM SPSS Statistics. Allocation concealment was implemented through central randomization, with a researcher (P.P.) generating the sequence and assigning participants.
The Triphala group received 1000 mg/day of Triphala capsules (500 mg before breakfast and 500 mg before dinner), while the placebo group received the same dosage of maltodextrin. Both were administered five days per week for eight weeks (Supplemental File). Blinding was maintained: participants, interventionists (S.I.), data collectors (N.P., S.B.), outcome assessors (Y.T.) and data analysts (O.B.) were all blinded to group allocation.
Participants recorded supplement intake and any adverse symptoms daily. They were instructed to maintain their normal lifestyle, including physical activity and diet. Weekly follow-ups were conducted via phone or the Line application to ensure compliance. Adherence was monitored using the pill count method and categorized as high (≥80%) or low (<80%).
Pre- and post-intervention assessments of oxidative stress biomarkers (MDA, protein carbonyls, and superoxide dismutase [SOD] activity) and inflammatory markers (interferon-gamma [IFN-γ], tumor necrosis factor-alpha [TNF-α]) were conducted under similar environmental and physiological conditions.
Supplements
Triphala capsules were supplied by Charoensuk Pharma Supply Co., Ltd. (Nakhon Pathom, Thailand), a GMP-certified herbal product company. Mature fruits of E. officinalis, T. chebula, and T. bellerica were washed, sliced, and dried at 45°C-50°C for 48 hours, with humidity controlled at <10%. The dried fruits were ground, sieved (no. 80-100), and filled into size 0 capsules (500 mg per capsule) using an automatic capsule filler. Capsules were stored in opaque Ziplock bags at room temperature. The foundational ratio between E. officinalis, T. chebula, and T. bellerica used in this study was 3:1:2, according to the Thai Herbal Medicine Properties Handbook.
Placebo capsules (500 mg maltodextrin) were prepared by Phanat Nikhom Hospital, Chonburi, Thailand, using the same preparation protocol as Triphala. Quality control included humidity (<10%), capsule weight deviation (<10%), and production under SOP-PHANAT guidelines at 22°C-28°C and <60% humidity.
Analysis of Triphala Powder Constituents
Triphala powder composition was analyzed by gas chromatography–mass spectrometry (GC-MS) using an Agilent 7890A GC system and Agilent 7000B MS (Agilent Technologies, USA), equipped with an HP-5 capillary column (30 m × 0.32 mm, 0.25 μm). 100 mg of Triphala powder was dissolved in 1 mL ethanol, and 2 μL of the sample was injected using a 5:1 split ratio at 250°C. Helium was used as the carrier gas at 1.0 mL/min. Oven temperature was ramped from 40°C (5 min hold) to 200°C (25 min hold), then to 280°C (61 min hold). MS analysis used electron ionization (230°C, 70 eV), scanning from 50-650 m/z. Data were processed using GC-QQQ software and the NIST MS Search 2.0 library.
Analysis of Oxidative Stress and Antioxidant Biomarkers
Approximately 2 mL of venous blood was collected into EDTA tubes. MDA concentration in plasma was assessed as a thiobarbituric acid reactive substance (TBARS) following the method of Kukongviriyapan et al., 9 with minor modifications. Briefly, 150 μL of plasma was mixed with trichloroacetic acid (10%), EDTA (5 mM), sodium dodecyl sulfate (8%), and butylated hydroxytoluene (0.5 μg/mL), followed by TBA (0.6%) and boiling for 30 minutes. After centrifugation (3500 rpm, 4°C, 5 min) (Eppendorf Centrifuge 5810R, Hamburg, Germany), the supernatant was measured at 532 nm (Eppendorf UV/Vis Basic BioSpectrometer, Germany). A standard curve was generated using 1,1,3,3-tetraethoxypropane (0.1-10 μmol/L).
Protein carbonyls were quantified using the Bradford dye-binding method, 10 with incubation of samples with and without dinitrophenylhydrazine in 3.6 M HCl for 1 hour in the dark. Proteins were then precipitated and redissolved in 6 M guanidine. Carbonyl content was quantified from the absorbance at 360 nm following subtraction of HCl-treated blanks by the use of a molar absorption coefficient of 22,000/M/cm.
SOD activity in serum was measured using the SOD Assay Kit - WST (Dojindo Laboratories, Japan). Each well received 200 μL of WST working solution and 20 μL of enzyme solution. Plates were incubated at 37°C for 20 min and read at 450 nm using a microplate reader (SpectraMax® ABS, Molecular Device, CA, USA). SOD activity (inhibition rate %) was calculated using the following equation: SOD activity (inhibition rate %) = [(Ablank 1 - Ablank 3) - (Asample - Ablank 2)]/(Ablank 1 - Ablank 3) x 100.
Analysis of Inflammatory Biomarkers
Approximately 4 mL of venous blood was collected in the morning after an 8-hour overnight fast using standard venepuncture technique. Samples were stored in clot-activator tubes and allowed to coagulate before serum separation. Serum concentrations of IFN-γ and TNF-α were measured using OptEIA™ ELISA kits (BD Biosciences Pharmingen, San Diego, CA, USA), according to the manufacturer’s instructions. Briefly, 100 μL of diluted capture antibody was added to each well of a microplate and incubated overnight at 4°C. The wells were then aspirated and washed three times, followed by the addition of 200 μL of assay diluent to block nonspecific binding. After a 1-hour incubation at room temperature, the wells were washed again (3 times). Next, 100 μL of either standard or serum sample was added to each well and incubated for 2 hours at room temperature. The wells were then washed five times, and 100 μL of working detection solution (Detection Antibody + Streptavidin-HRP) was added. After a further 1-hour incubation at room temperature, the wells were washed seven times, with each wash including a 30-second to 1-minute soak. Following this, 100 μL of substrate solution was added to each well and incubated for 30 minutes at room temperature in the dark. The reaction was stopped by adding 50 μL of stop solution. Absorbance was measured at 450 nm with wavelength correction at 570 nm using a microplate reader (SpectraMax® ABS, Molecular Devices, CA, USA).
Analysis of Renal and Liver Function
Renal and liver functions were assessed to evaluate the potential adverse effects of 8-week Triphala supplementation. Serum concentrations of creatinine and alanine aminotransferase (ALT) were measured using the VITROS CREA and VITROS ALTV slide methods, respectively, following standard clinical laboratory protocols (RIA Laboratory Co., Ltd., Chonburi, Thailand).
Assessment of Clinical Symptoms
Key clinical symptoms commonly associated with post-COVID-19 condition—including fatigue, respiratory symptoms (e.g., breathlessness, cough), cognitive impairment (e.g., memory difficulties, lack of concentration), and headache—were assessed using self-report questionnaires. Symptom severity was assessed using a 5-point Likert-type scale (0 = Not at all, 1 = A little bit, 2 = Somewhat, 3 = Quite a bit, 4 = Very much), with lower scores indicating milder or less frequent symptoms and thus reflecting better clinical status.
Statistical Analyses
All data were expressed as mean ± standard deviation (SD). Normality and homogeneity of variance were tested using the Shapiro–Wilk test and Levene’s test, respectively. Differences within groups (pre- vs post-supplementation) and between groups (Triphala vs placebo) were analyzed using two-way repeated measures analysis of variance (ANOVA), followed by Bonferroni post hoc tests for multiple comparisons. Where appropriate, paired t-tests were used to confirm within-group changes. Effect sizes were calculated using Cohen’s d. For all relevant outcomes, the following were reported: mean change, percent change, effect size, 95% confidence intervals (CIs), and P-values. Statistical analyses were performed using IBM SPSS Statistics (IBM Corp., Armonk, NY, USA), with the threshold for statistical significance set at P < .05.
Results
Physical and Clinical Characteristics
Participants were recruited between 9 May 2023 and 15 August 2023, with follow-up conducted from 16 July 2023 to 22 October 2023. The final participant visit occurred on 22 October 2023. A total of 78 participants were screened and enrolled. After randomization, 38 were allocated to the placebo group and 40 to the Triphala group. One participant from the placebo group (2.63%) and three from the Triphala group (7.50%) withdrew due to non-compliance with the 8-week supplementation protocol. Ultimately, 37 participants in each group completed the study (97.37% for placebo, 92.50% for Triphala) (Figure 1). CONSORT Flow Diagram for the Randomized Controlled Trial
Physical and Clinical Characteristics in Participants Before and After the Placebo and Triphala Interventions

Data are mean ± standard deviation. CI, confidence interval. *Significantly different from before intervention (P < .05).
Clinical parameters showed comparable infection frequency (1.21 ± 0.42 vs 1.32 ± 0.64 times; P = .399) and recovery time from the latest infection (8.52 ± 5.80 vs 8.91 ± 6.79 months; P = .789) between placebo and Triphala groups, respectively (Table 1).
Triphala Powder Constituents
GC-MS identified 40 compounds in Triphala powder (Figure 2, Table 2). Benzenetriol (RT 17.73 min) was the most abundant, accounting for 48.82% of the total peak area. Other major compounds included n-hexadecanoic acid (9.44%), oleic acid (8.33%), linoleic acid (6.52%), β-monoolein (4.82%), β-sitosterol (3.71%), 5-hydroxymethylfurfural (2.21%), and catechol (2.06%). Analysis of a Sample of Triphala Powder Using GC-MS Triphala Chemical Constituents Analyzed by Using GC-MS

Oxidative Stress and Antioxidant Status
In the Triphala group, plasma MDA concentrations significantly decreased (1.50 ± 0.82 vs 1.08 ± 0.64 μmol/L; P = .026), as did protein carbonyl concentrations (0.05 ± 0.04 vs 0.03 ± 0.03 nmol/mg protein; P = .017) after 8 weeks. No significant changes were observed in the placebo group. Between-group comparisons showed no statistically significant differences in post-intervention MDA (Cohen’s d = 0.018, 95% CI: −0.61 to 0.18, P = .289) or protein carbonyl concentrations (Cohen’s d = 0.028, 95% CI: −0.01 to 0.03, P = .184) (Figure 3). While the mean change in MDA was not different between groups, the mean change in protein carbonyl was significantly greater in the Triphala group (0.00 vs −0.02 nmol/mg protein; P = .048). Malondialdehyde (MDA) (A) and Protein Carbonyl (B) Concentrations in Participants before and after the Placebo and Triphala Interventions. Data are Mean ± Standard Deviation; n = 37 Each. *Significantly Different From before Intervention (P < .05)
SOD activity significantly increased in both groups: from 51.48 ± 10.23% to 58.39 ± 14.37% in the Triphala group (P = .008), and from 48.36 ± 9.75% to 53.87 ± 10.88% in the placebo group (P < .001). Between-group differences were not significant (Cohen’s d = 0.007, 95% CI: −6.45 to 3.27, P = .516) (Figure 4), and neither mean nor percentage changes in SOD activity differed significantly between groups. Superoxide Dismutase (SOD) Activity in Participants before and after the Placebo and Triphala Interventions. Data are Mean ± Standard Deviation; n = 37 Each. *Significantly Different From before Intervention (P < .05)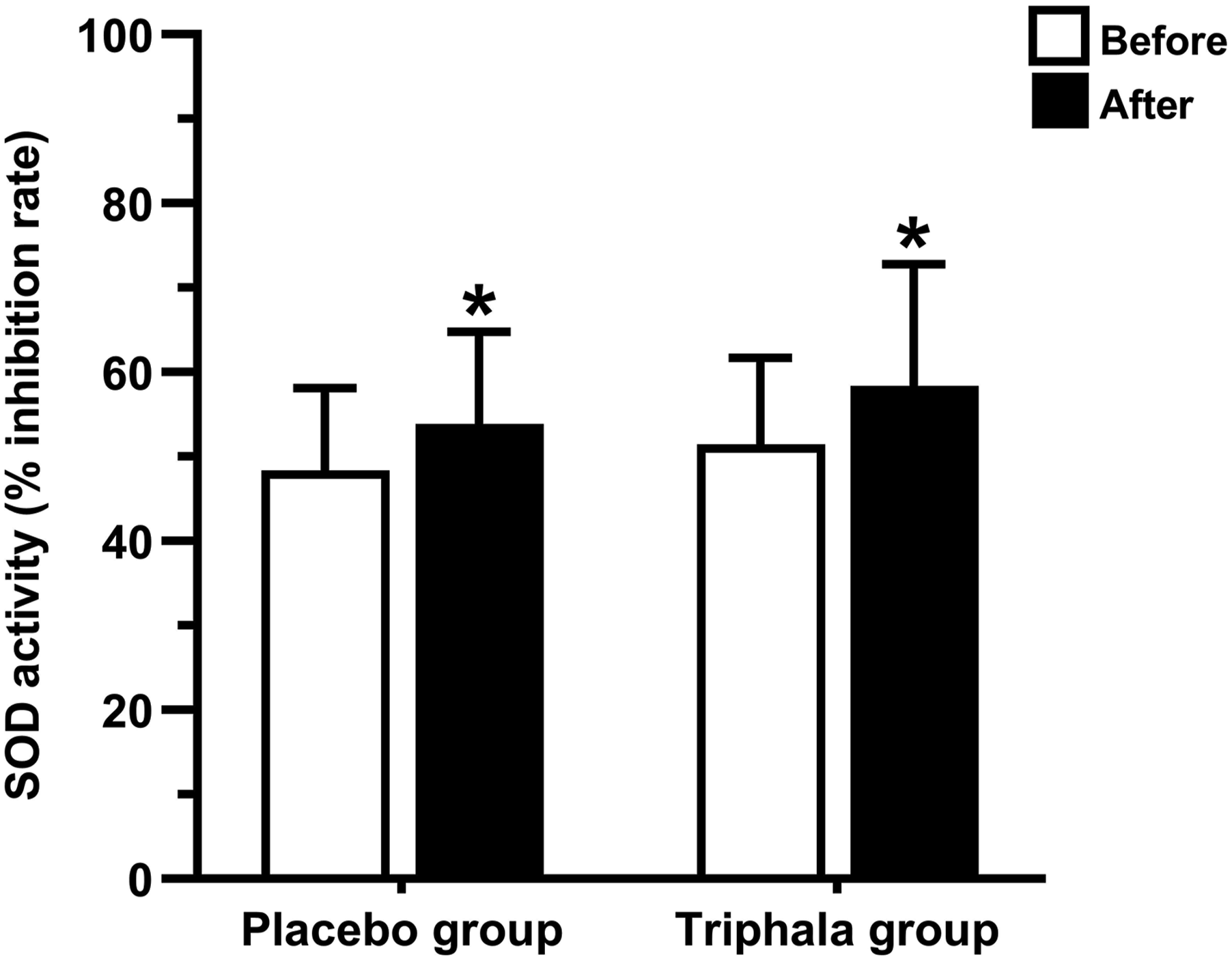
Inflammation
Serum IFN-γ and TNF-α levels significantly decreased in the Triphala group after supplementation (IFN-γ: 6.34 ± 4.37 vs 4.95 ± 3.16 pg/mL, P = .038; TNF-α: 1.54 ± 0.77 vs 1.08 ± 0.67 pg/mL, P < .001). No significant changes were observed in the placebo group. Between-group comparisons revealed no significant differences in IFN-γ (Cohen’s d = 0.029, 95% CI: −0.59 to 2.93, P = .187) or TNF-α (Cohen’s d = 0.250, 95% CI: −0.17 to 0.64, P = .051) concentrations (Figure 5). However, the mean change in TNF-α concentration was significantly greater in the Triphala group (−0.05 vs −0.46 pg/mL; P = .001). Interferon-Gamma (IFN-γ) (A) and Tumor Necrosis Factor-Alpha (TNF-α) (B) Concentrations in Participants before and after the Placebo and Triphala Interventions. Data are Mean ± Standard Deviation; n = 37 Each. *Significantly Different From before Intervention (P < .05)
Clinical Symptoms
Clinical Symptoms Scales in Participants Before and After the Placebo and Triphala Interventions

Data are mean ± standard deviation. *Significantly different from before intervention (P < 0.05). #Significantly different from placebo intervention (P < 0.05).
Renal and Liver Function
Renal and Liver Function in Participants Before and After the Placebo and Triphala Interventions

Data are mean ± standard deviation. ALT, alanine aminotransferase.
Discussion
Regarding the significant and reciprocal roles of oxidative stress and inflammation in the pathophysiology of post-COVID-19 condition, 4 this study accordingly sought to investigate the anti-oxidative and anti-inflammatory effects of Triphala supplementation in participants with post-COVID-19 condition. In this study, oxidative stress and inflammatory cytokines closely associated with immune function such as IFN-γ and TNF-α were determined. We found that the concentrations of MDA, protein carbonyl, IFN-γ, and TNF-α were significantly reduced, and SOD activity was significantly increased following 8 weeks of Triphala supplementation.
In accordance with the Thai Herbal Medicine Properties Handbook, the foundational ratio between E. officinalis, T. chebula, and T. bellerica was set at 3:1:2. This formula is optimal in respiratory rehabilitation for resolving respiratory symptoms, which are the most common symptoms post COVID-19 infection. Among the three herbs in Triphala, E. officinalis is possibly the most important medicinal plant, as it plays a major role in reducing oxidative stress and systemic inflammation.
In this study, Triphala supplementation significantly reduced the concentrations of IFN-γ and TNF-α, and these results may be attributed to several mechanisms. Based on studies in arthritis-induced rats, Triphala extract exhibited anti-inflammatory effects, including decreased pro-inflammatory cytokine production. 11 Reports from in vitro and in vivo studies suggest that Triphala and its extracts reduce inflammation by lowering the expression of pro-inflammatory mediators through the inhibition of redox-sensitive IκB kinase activity, blocking NF-κB nuclear translocation, and reducing DNA binding to NF-κB. 12 Furthermore, Triphala has been shown to alter the immune system and act as an immunomodulatory agent. 13 In a phase I clinical study conducted in healthy volunteers, the consumption of dietary Triphala resulted in significant immunostimulatory effects on cytotoxic T cells (CD3− CD8+) and natural killer cells (CD16+ CD56+). 14
Furthermore, we found that Triphala supplementation significantly increased antioxidants, namely SOD activity, and decreased oxidative stress as a result of products, i.e., MDA and protein carbonyl concentrations. These results are similar to those in previous reports. For instance, in rats with stress-induced ulcers, Triphala supplementation increased antioxidants such as glutathione in intestinal brush border cells and decreased oxidant levels through myeloperoxidase and xanthine oxidase in the epithelium. 11 In addition, based on several studies conducted in animal models, Triphala treatment increased the expression of SOD-2, 15 restored the activities/levels of catalase (CAT), SOD, glutathione-S-transferase, glutathione peroxidase (GPx), and total reduced glutathione,16,17 and decreased MDA levels.17,18 Notably, numerous in vitro studies have shown that Triphala possesses high antioxidant potential, as it was found to quench free radicals and induce SOD and CAT antioxidant enzymes. 19
Based on GC-MS analysis, benzenetriol was found to be the most abundant compound in Triphala powder, with a peak area of 48.82%. 1,2,3-benzenetriol (pyrogallol), in particular, has been studied as an antimicrobial and antioxidant compound 20 and is classified as a polyphenolic compound. Polyphenols are highly relevant for their beneficial impact on health, as they protect against cardiovascular diseases, various types of cancer, and inflammation-related chronic degenerative diseases prevalent worldwide. 20
Considering each of the three herbs that form Triphala, E. officinalis, previously mentioned as possibly the most important medicinal plant, contains several active phytochemicals such as pyrogallol, tannins, gallic acid, vitamin C, emblicanin-A, emblicanin-B, pedunculagin, and punigluconin, which possess free radical scavenging, antioxidant, anti-inflammatory, and immunomodulatory activities. 21 Many studies have reported the beneficial effects of E. officinalis in both human and animal experiments. For instance, in two randomized, double-blind, controlled clinical studies, E. officinalis extract at 250 mg and 500 mg for 12 weeks significantly improved endothelial function and reduced biomarkers of oxidative stress (nitric oxide [NO˚], glutathione, and MDA), systemic inflammation (high-sensitivity C-reactive protein; hsCRP), and lipid profiles in patients with type 2 diabetes mellitus (with improved glycosylated hemoglobin) and metabolic syndrome.22,23 An investigation of the effects of E. officinalis on rat brains found that SOD, CAT, and GPx activity increased and lipid peroxidation decreased after 7 days of treatment. 24 The authors suggested that the antioxidant activity of E. officinalis may stem from tannins (or tannoids), which have vitamin C-like properties.
Secondly, T. bellerica is one of the oldest medicinal herbs in Ayurveda, containing diverse bioactive phytochemicals such as gallic acid (a typical derivative of pyrogallol), glucoside, tannins, corilagin, ellagic acid, ethyl gallate, galloyl glucose, chebulagic acid, and arjunolic acid. Its biological and pharmacological effects, including antioxidant, anti-inflammatory, and immunomodulatory activities, have been extensively documented. 25 An in vitro study demonstrated the potential effects of T. bellerica fruit and its bioactive compound ellagic acid in mitigating oxidative stress in liver tissue due to increased activities of SOD and CAT and reduction of hepatotoxicity produced by an anti-inflammatory drug. 26 Another study demonstrated that T. bellerica extract treatment inhibited free radical-induced low-density lipoprotein (LDL) oxidation and macrophage inflammatory response by decreasing mRNA expression of TNF-α, interleukin (IL)-1β, and lectin-like oxidized LDL receptor-1, which is related to atherosclerosis. 27 Furthermore, a separate study showed that T. bellerica extract and gallic acid protect against lipopolysaccharide-induced inflammation and oxidative stress by suppressing the MAPK/NF-κB pathway while activating the Akt/AMPK/Nrf2 pathway. 28
The third constituent of Triphala is T. chebula, renowned as the king of medicinal plants in Ayurveda due to its fruit, which contains a wide range of phytochemicals, including high levels of phenolic acids, flavonoids, tannins, and other bioactive compounds. The biological and pharmacological properties of T. chebula, particularly its antioxidant and anti-inflammatory activities, have been extensively described. 29 An in vitro study 30 reported that chebulagic acid isolated from T. chebula fruits demonstrated potent inhibition against cyclooxygenase (COX)-1, COX-2, and 5-lipoxygenase, key enzymes involved in inflammation and carcinogenesis. It also showed potent antioxidant properties with potential to prevent oxidative damage. A recent animal study revealed that supplementation with T. chebula extract increased levels of immunoglobulin M, IL-4, and IL-10 and decreased IL-6 in serum. It also increased CAT, SOD, GPx, and total antioxidant capacity activities while decreasing MDA concentration. 31 Human clinical studies in patients with metabolic syndrome 32 and type 2 diabetes mellitus 33 demonstrated that T. chebula fruit possesses antioxidant and anti-inflammatory activities. These studies observed significant improvements in MDA, NO˚, glutathione, and hsCRP levels after 12 weeks of treatment with 250 and 500 mg of T. chebula compared to baseline and placebo.
Regarding clinical symptoms, decreases in MDA, protein carbonyl, IFN-γ, and TNF-α concentrations, alongside an increase in SOD activity after 8 weeks of Triphala supplementation, may be partially linked to improvements in fatigue, headache, and respiratory symptoms. However, no notable changes were observed in cognitive symptoms. This discrepancy may reflect the multifactorial nature of post-COVID-19 cognitive impairment (brain fog), which is influenced not only by inflammation and oxidative stress but also by neurovascular alterations, persistent viral particles, microglial activation, and neurotransmitter dysregulation. The antioxidant and anti-inflammatory properties of Triphala may be insufficient to address these complex neurological mechanisms, particularly within the relatively short 8-week timeframe. Cognitive improvements may require a longer intervention period, higher dosage, or more sensitive and objective assessments (e.g., neuropsychological testing, neuroimaging). Further analysis using the Pearson correlation coefficient supported a link between antioxidant status and clinical outcomes, showing that SOD activity was negatively correlated with fatigue scores in the Triphala group (r = −0.482, P = .011). Interestingly, fatigue and headache scores also improved in the placebo group, potentially related to increased SOD activity, although no significant correlations were found. Given the small sample size, these results should be interpreted as preliminary and require confirmation in larger clinical trials. Supporting this interpretation, a proof-of-concept mechanistic study 34 reported that long-COVID, post-viral chronic fatigue, and affective symptoms were associated with oxidative damage, diminished antioxidant defenses (notably GPx and zinc), and heightened inflammation, including increased myeloperoxidase, NO˚, and lipid peroxidation–related aldehyde formation.
In terms of intervention compliance (adherence), the information in this study was collected via participant self-report using the pill count method. Among the 37 participants in each group, 30 (81.08%) in the placebo group and 32 (86.49%) in the Triphala group had high adherence to the intervention protocol (≥80%). No safety concerns were raised, and no adverse events were reported as related to either placebo or Triphala supplementation, including allergies, uncomfortable digestive-related symptoms (e.g., nausea, vomiting, bloating, constipation, diarrhea), dizziness, syncope, loss of appetite, or weight loss.
Our findings support the beneficial efficacy of Triphala supplementation in attenuating oxidative stress, inflammation, and clinical symptoms. As this study was conducted in individuals with post-COVID-19 condition, the findings may offer an alternative approach for managing COVID-19 and mitigating its long-term consequences. Moreover, the supplementation regimen used in this study was determined as safe, as it did not induce renal or liver injury post-supplementation. After 8 weeks, participants in both placebo and Triphala groups had normal creatinine levels, unchanged from baseline (clinical range 0.67-1.17 mg/dL). All participants in the Triphala group had normal ALT concentrations; one participant’s ALT decreased to within the clinical range (<50 U/L) compared to an elevated baseline value. Conversely, two participants in the placebo group showed increased ALT levels relative to baseline. Given the short-term nature of the intervention, future studies with long-term Triphala protocols should evaluate toxicity further. Regarding toxicity, a recent rat study 35 reported no signs of acute toxicity (5000 mg/kg Triphala) or chronic toxicity (600, 1,200, and 2400 mg/kg/day for 270 days) based on hematology, biochemistry, and tissue histopathology. The authors concluded that long-term Triphala administration in rats is safe and well tolerated. Moreover, previous reviews 36 have demonstrated that Triphala and its phytochemical constituents exhibit protective effects against acute hepatic toxicity induced by high doses of drugs and chemicals, which may be attributed to the high levels of phenolic and polyphenolic compounds present in its constituent plants.
Study Limitations
To our knowledge, there are limited randomized and non-randomized controlled trials assessing the anti-oxidative and anti-inflammatory effects of dietary Triphala in humans. This study is the first human investigation to evaluate Triphala supplementation’s impact on oxidative stress and inflammation as primary endpoints, specifically in participants with post-COVID-19 condition. However, there are several limitations. First, well-established doses and treatment durations based on previous studies are insufficient. Therefore, we based the Triphala dose on the manufacturer’s recommendations, which primarily target gastrointestinal disorders. This may have partially contributed to the predominantly non-significant differences between the Triphala and placebo groups, although the Triphala group demonstrated greater improvements overall. Future trials using higher doses or longer supplementation periods are necessary to better determine Triphala’s efficacy and safety before broader clinical application. Second, immune cell functions—such as white blood cell count, response, differentiation, culture, and growth—were not directly measured. Thus, conclusions about immune modulation remain limited and warrant further investigation. Third, long-term clinical symptoms and hospital readmission data post-intervention were not collected. The absence of these data limits our ability to predict Triphala’s long-term clinical impact, highlighting the need for future studies to address these outcomes. Finally, while GC-MS analysis identified numerous bioactive compounds in Triphala powder, including benzenetriol (pyrogallol), n-hexadecanoic acid, oleic acid, and various polyphenols, the systemic bioavailability and pharmacokinetics of these compounds remain to be fully elucidated. Many polyphenolic compounds typically exhibit low oral bioavailability due to poor absorption, extensive metabolism by gut microbiota, and rapid conjugation in the liver. For example, compounds like gallic acid and ellagic acid undergo extensive biotransformation to metabolites such as urolithins, which may themselves possess biological activity. Despite potentially low plasma concentrations of the parent compounds, these metabolites can contribute significantly to systemic antioxidant and anti-inflammatory effects. Furthermore, the lipophilic constituents (e.g., oleic acid) may have better absorption and systemic distribution, potentially mediating some of the observed effects. The clinical implications of this complex pharmacokinetic profile suggest that the efficacy of Triphala supplementation depends not only on the presence of these active compounds but also on their metabolism, bioactivation, and tissue distribution, which may vary among individuals. Future studies incorporating pharmacokinetic profiling and metabolomics are warranted to better understand the relationship between compound exposure and clinical outcomes, optimize dosing regimens, and enhance therapeutic efficacy.
Conclusion
This preliminary study suggests that Triphala supplementation at a dose of 1000 mg per day, administered 5 days per week over 8 weeks, may help reduce oxidative stress and inflammation in individuals with post-COVID-19 condition. Improvements were also observed in clinical symptoms, including fatigue, headache, and respiratory complaints. These findings indicate that the benefits of Triphala may extend beyond its traditional gastrointestinal and rejuvenative uses to include potential applications in managing inflammation-related conditions.
However, as most primary outcomes did not show statistically significant differences between the Triphala and placebo groups. Thus, this limitation underscores the need for further research involving larger sample sizes, longer intervention periods, and mechanistic investigations to validate and expand upon these findings.
Supplemental Material
Supplemental Material - Ameliorative Effects of Triphala Supplementation on Oxidative Stress and Inflammation in Individuals with Post-COVID-19 Condition: A Preliminary Randomized Controlled Trial
Supplemental Material for Ameliorative Effects of Triphala Supplementation on Oxidative Stress and Inflammation in Individuals with Post-COVID-19 Condition: A Preliminary Randomized Controlled Trial by Suwipa Intakhiao, Nattaphol Prakobkaew, Surachat Buddhisa, Orachorn Boonla, Yothin Teethaisong, Sukrisd Koowattanatianchai, Piyapong Prasertsri in Global Advances in Integrative Medicine and Health
Footnotes
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was financially supported by the Faculty of Allied Health Sciences, Burapha University, Thailand under Grant AHS 08/2566.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.