
Abstract
Objectives
Non-pharmacologic approaches are now considered best practice for the treatment of chronic pain. The purpose of this pilot study was to evaluate patient responses to a newly integrated clinic service called Mindful Awareness in Body-oriented Therapy (MABT) at a chronic pain clinic. MABT is designed to develop interoceptive sensibility for improved well-being and emotion regulation.
Methods
A one-group repeated measures design was used to examine MABT referral and delivery follow-through feasibility and change on health outcomes among chronic pain patients. Upon referral, participants were scheduled for the MABT program involving eight individual sessions with one of the clinic massage therapists trained in MABT. Measures were administered at baseline, post-intervention (3 months) and at 6 month follow-up). Outcome measures assessed physical and mental health distress, interoceptive awareness, and emotional well-being. Analyses included descriptive statistics and repeated measures ANOVA.
Results
Seventy patients were referred and 41 received at least one MABT session. Thirty patients (73%) completed the MABT intervention. Statistically and/or clinically significant improvements were identified for most subscales of the PROMIS-29 (the primary outcome), including Physical Function, Fatigue, Anxiety, Sleep Disturbance, Social Roles, and Pain Interference. Improvements in interoceptive sensibility and emotion regulation difficulties also demonstrated statistically significant and large effects.
Discussion
This pilot study demonstrates the feasibility of MABT referral and delivery follow-through when delivered in a real-life context. Significant improvements with large effects on outcomes in response to the MABT intervention program offers a promising non-pharmacological approach for chronic pain patients.
Introduction
In the last two decades, there has been a profound shift in approaches to treating pain, moving from a focus on nociception toward a biopsychosocial model that acknowledges pain as interconnected in biological, psychological, and social/cultural contexts. 1 In parallel, results from cross-sectional and longitudinal brain imaging studies suggest the chronification of pain is correlated with a shift away from acute pain circuits to the engagement of emotion circuits.2-4 Thus, enhancing self-regulation of arising sensory and affective experiences is now considered a candidate mechanism in promoting long-lasting reductions in pain and corresponding comorbidities.5,6 Non-pharmacologic approaches are now considered best practice for the treatment of chronic pain.7,8 However, complementary and integrative health (CIH) mind-body approaches that employ evidenced-based non-pharmacological interventions that conceptualize and treat chronic pain through a biopsychosocial framework and target self-regulation of arising sensory and affective experiences are currently underutilized.
One pathway to explore for the treatment of chronic pain involves developing interoception. Interoceptive awareness, defined as the process by which an individual attends to, appraises, and responds to bodily sensation, 9 is considered an iterative process requiring the interplay between subjective perception of and attention to internal bodily sensations, and the cognitive-affective appraisal of these bodily sensations thought to underlie self-regulation.10,11 Interoception is increasingly recognized as an important component of chronic pain conditions. 12 Two systematic reviews have investigated interoception in adults with chronic pain.13,14 Locatelli et al concluded that within chronic pain conditions, lower interoceptive awareness was associated with increased pain severity and frequency. Further, lower interoceptive awareness has been shown to predict increased symptoms related to central sensitization15,16 and to be associated with reduced descending pain inhibition processes. 17 Thus, interoception dysfunction (ie, a lack of sensory processing) is an important, yet understudied, transdiagnostic mechanism that may underly the development and maintanence of chronic pain.
Interoceptive awareness is typically introduced in mindfulness training by developing present moment attention to internal body sensations, for example attention to the sensations of breathing and related processes that can be linked to awareness and self-regulation. Two systematic reviews of non-pharmacologic approaches for chronic pain among mindfulness-based approaches, primarily mindfulness-based stress reduction (MBSR) or acceptance and commitment therapy (ACT) demonstrate moderate improvements in pain interference, fatigue and anxiety and small improvements in pain intensity, depression and physical disability.18-21 A study of mindfulness-based cognitive therapy for pain showed similar outcomes. 22 These mindfulness-based approaches were typically delivered as group-based programs. With exception of de Jong’s study, interoception was not measured.
The purpose of this study was to examine an intervention called Mindfulness Awareness in Body oriented Therapy (MABT). MABT is an innovative mind-body approach designed to reduce symptomatic distress and improve self-regulation of arising sensory and affective experiences by targeting processes of interoception. 23 MABT is delivered individually (1:1) in a sequenced approach designed to coach clients in the development of interoceptive skills. MABT has been successfully delivered in diverse populations including individuals with substance use disorders, trauma history of childhood sexual abuse, and HIV. The feasibility, acceptability, and safety of MABT for the treatment of chronic pain was initially demonstrated through a pilot study with female veterans with co-occurring chronic pain and PTSD, 24 and has been shown to be similarly feasible, acceptable and safe to deliver in many larger randomized controlled trials, including a recently completed study (n = 303) of MABT for individuals in medication treatment for opioid use disorder (MOUD), 50% of whom had chronic pain. 25 In the study of MABT as an adjunct to MOUD vs MOUD, pre to post intervention findings demonstrated significant improvement in pain severity, pain activity interference, physical symptom frequency, symptoms of post-traumatic stress and interoceptive awareness. 25 A next step in MABT research is to evaluate the feasibility of implementing MABT as a clinical service for chronic pain within the context of real-life clinical care.
This pilot study was designed to evaluate the feasibility of delivering MABT to patients in treatment for chronic pain when offered as an integral service for clinic patients. Our first aim was to explore the feasibility of MABT implementation (ie, how many patients scheduled sessions after referral, how many patients completed the MABT program, and potential barriers for delivery). Our second aim was to examine MABT treatment response by assessing the change on health outcomes from baseline to 3- and 6-month follow-up on PROMIS-29 measures of distress (primary outcome), and secondary outcomes of interoceptive awareness, emotion regulation difficulties, resilience, and flourishing. We hypothesized that participants would show a significant reduction in physical and psychological symptoms of distress on PROMIS measures (primary hypothesis) and a significant increase in interoceptive awareness, resilience and flourishing from baseline to 6-month follow-up (secondary hypothesis).
Materials and Methods
Study Design
A hybrid-type 2 pilot implementation-effectiveness study design was employed at the Vanderbilt Osher Clinic for Integrative Medicine (OCIM). This pilot study collected preliminary data to support a future hybrid effectiveness-implementation study designed to examine outcomes of MABT in a chronic pain clinic. The findings related to implementation, or system level outcomes, show high levels of clinic staff/stakeholder acceptability, uptake and adoption of MABT. 26 The current manuscript reports on the patient outcomes, specifically patient response to a new intervention (ie, MABT) when delivered as an integral component of clinic services, examining referral and intervention delivery follow-through, and the change over time on health outcomes in response to MABT. MABT was delivered by massage therapist staff at OCIM who were trained in the MABT approach. The study was approved by Vanderbilt University’s IRB, and initial plan details were registered with ClinicalTrials.gov (NCT05289024). The power, based on prior MABT research,27,28 a one-group sample of n = 34 was determined to be adequate to show statistical significance on symptomatic distress when alpha = 0.05, a standardized effect size (d) = 0.5, and power (1-β) = 0.80.
Procedures
Setting
Vanderbilt OCIM is an integrative medicine clinic that employs non-pharmacological approaches, including mind-body methods, for the treatment of pain. The clinic provides 17,000 appointments a year to patients seeking treatment for chronic pain, of which approximately 1700 appointments are for massage therapy. 29 The majority of patients at Vanderbilt OCIM have private insurance. 29 However, insurance in the State of Tennessee does not cover massage therapy and therefore massage therapy appointments must be paid for out of pocket.
Upon initial visit, all patients were asked to complete a REDCap survey to gather health data, including standardized measures to assess stress, pain, and other indicators of well-being. Consent to use de-identified survey data for research is requested on this initial intake survey. Similar surveys are administered at regular intervals to all ongoing patients, and it is thus considered usual care to be surveyed on health outcomes at this clinic.
Nurse Practitioners see all patients at intake and collaboratively develop a treatment plan with the patient to address their health care needs. Serving a highly distressed population, the majority of patients seen at OCIM have co-occurring chronic pain and mental health conditions.
Recruitment
OCIM Nurse Practitioners, Physical therapists, Psychotherapists, or Massage Therapists referred patients experiencing chronic pain to MABT through an order in EPIC, the electronic medical records system. Only those who provided consent to use de-identified data for research at initial intake as a clinic patient could be referred to this project. With this exception, there were no inclusion or exclusion criteria for referral. This consent approach supported the goals of matching procedures of usual care, as this project was designed to examine service adoption and use within the context of usual care.
Referred patients were contacted by front desk staff to confirm interest in MABT, and to set up a series of eight sessions and related payment for the MABT program. Once scheduled, the patient was sent an email link with a REDCap survey to assess health outcomes used for this project.
Mindful Awareness in Body-Oriented Therapy (MABT) Intervention
Key MABT Components.
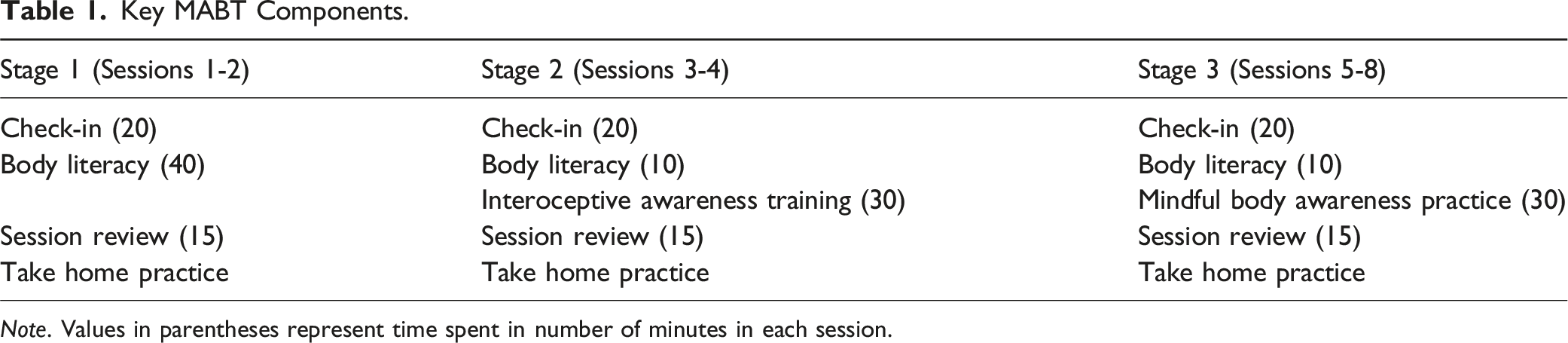
Note. Values in parentheses represent time spent in number of minutes in each session.
MABT, which integrates the use of touch-based coaching to teach interoceptive awareness, was delivered by two experienced massage therapists who were clinic employees trained to deliver the MABT protocol. To evaluate fidelity of the intervention, the massage therapists had a specific set of post-session notes to document delivery of key MABT components in the medical chart, and they met regularly for clinical supervision over the course of the project with the first author (C.J.P). To review these notes and to discuss delivery and any clinical concerns that may have been raised during sessions.
Data Collection & Measures
Descriptive sample characteristics (ie, age, sex, race), health diagnoses, referral diagnoses, and MABT session attendance records were collected from the clinic’s electronic medical record. Health outcomes were collected at three timepoints: baseline, and 3- and 6-month follow-up and were collected via online REDCap surveys that were administered by email link or at an in-clinic visit.
Primary Outcomes
The Patient Reported Outcomes Measurement Information System (PROMIS)-29 is a 29-item self-report measure to assess functioning and well-being in physical, mental and social domains of health. 31 PROMIS-29 v2.0 assesses pain intensity using a single 0-10 numeric rating item. The PROMIS-29 v2.0 also assesses seven health domains (ie, physical function, fatigue, pain interference, depressive symptoms, anxiety, ability to participate in social roles and activities, and sleep disturbance) using four items for each domain. 32 The scale is rated on a 5-point Likert-type scale (1 = Never to 5 = Always). A minimally important difference (MID) to identify meaningful change can be calculated and is defined as a T-score change of 3 points for PROMIS-29 subscales.33,34 The internal consistency in this sample was excellent for all domains: physical function (α = .87), anxiety (α = .81), depression (α = .93), fatigue (α = .94), sleep disturbance (α = .88), social role (α = .93), and pain interference (α = .95).
Secondary Outcomes
The Multidimensional Assessment of Interoceptive Awareness (MAIA-2) 35 is a 37-item instrument that assesses adaptive body awareness. The scale is rated on a 6-point Likert-type scale (0 = Never to 5 = Always). A higher score is thought to indicate more adaptive body awareness. The total scale reliability in this sample was α = .93. There are eight scale factors that make up the MAIA, organized into five domains: General Awareness of Body Sensations domain is measured via the Noticing scale, which refers to the awareness of comfortable, neutral, and uncomfortable body sensations: Emotional and Attentional Responses to Bodily Sensations domain is measured via the Not-Worrying and the Not-Distracting subscales. Not-Worrying scale assesses the tendency not to worry or experience emotional distress with sensations of pain or discomfort. Not-Distracting scale assesses the tendency to not ignore or distract oneself from uncomfortable body sensations such as pain; Attention Regulation domain is measured by the Attention Regulation scale, which captures the tendency to maintain and regulate attention to body sensations; Awareness of Mind-Body Integration domain is measured by the Emotional Awareness, Self-Regulation and Body Listening subscales. Self-Regulation refers to the ability to control psychological distress by consciously attending to body sensations. Emotional Awareness refers to consciousness of the interrelation of emotions and body sensations. Body Listening refers to active listening to the body for insight; Tendency to Trust Body Sensations domain is measured by the Body Trusting scale. All factors demonstrated acceptable to excellent reliability (Noticing, α = .85, Not-Worrying, α = .78; Not-Distracting, α = .90.; Attentional Regulation, α = .95.; Emotional Awareness, α = .89.; Self-Regulation, α = .86.; Body Listening, α = .88.; Body Trusting, α = .81).
The Difficulties in Emotion Regulation Scale- Short Form (DERS- SF) 36 is an 18-item measure that attempts to assess emotional regulation difficulties. There are six subscales: nonacceptance of emotional responses, difficulty engaging in goal-directed behavior, impulse control difficulties, lack of emotional awareness, limited access to emotion regulation strategies, and lack of emotional clarity. The scale is rated on a 5-point Likert-type scale (1 = Almost Never to 5 = Almost Always). Higher scores correspond to more difficulties in emotion regulation. The internal consistency in this sample was excellent (α = .89).
The Brief Resilience Scale 37 is a 6-item measure designed to assess the ability to bounce back or recover from stress. The scale is rated on a 5-point Likert-type scale (1 = Strongly Disagree to 5 = Strongly Agree). Higher scores indicate greater resilience. The BRS demonstrated good internal consistency in this sample (α = .89).
The Flourishing Scale 38 is an 8–item scale of the person’s self-perceived functioning in important areas such as relationships, self-esteem, purpose, meaning, and optimism. The scale is rated on a 7-point Likert-type scale (1 = Strongly Disagree to 7 = Strongly Agree). A high score represents a person with many perceived psychological resources and strengths. The Flourishing scale demonstrated good internal consistency in this sample (α = .85).
Data Analysis
Descriptive statistics of means (M) and standard deviations (SD) were calculated for all variables. Prior to data analyses, variables were examined to evaluate data compliance with parametric analysis assumptions. Mann-Whitney U tests identified significant baseline differences between completers (attending ≥ 6 MABT sessions) and non-completers (attending < 6 MABT sessions). Attendance to at least 6 of the MABT sessions was necessary for completer status, due to receipt of at least 75% of the intervention program and receiving instruction in all key elements of the MABT program (eg, Stages 1-3).
Participants were included in the analysis to examine change in health outcomes if they completed baseline and at least one of the two follow-up assessments (delivered at 3 and 6 months after baseline), reducing the sample size to 29. Four participants missed the 3-month assessment but completed the 6-month assessment, 9 participants completed their 3-month but missed the 6-month assessment, and 17 completed both 3-month and 6-month assessments. Multiple imputations were used to handle missingness. A repeated Measures ANOVA was conducted on each outcome. A protocol developed by Ginkel et al (2014) was used to pool the results from the imputed data sets. Post hoc analyses with Bonferroni adjustments were conducted if overall repeated measure ANOVA test statistic was significant. Bonferroni adjustments were also conducted on the overall repeated measures ANOVA P-value based on 12 comparisons. T-scores were calculated and reported for the PROMIS-29 subscales and were used to signify minimally important difference from baseline to post intervention, and baseline to 6-month follow-up.30,31,33,34 Partial eta squared (n 2 ) was calculated to assess effect size and characterize the magnitude of change for each variable across time. Pearson’s correlations were conducted to characterize overall relationships between variable change scores. All analyses were completed with SPSS v. 29 (Statistical Package for the Social Sciences, 2013).
Results
Recruitment Feasibility
Of the 70 participants referred, 15 declined the MABT program (for an array of reasons including financial, unable to contact, and lack of interest (see Figure 1). Another 13 referred patients expressed initial interest but didn’t follow through and cancelled any scheduled session(s); reasons for lack of follow-through were similar reasons for declining, but many are unknown (see Figure 1) due to clinic cancelation process which was via automation and didn’t require a reason. Forty-one (∼59% of those referred to MABT) completed the baseline assessment and were enrolled in the study. Flow diagram.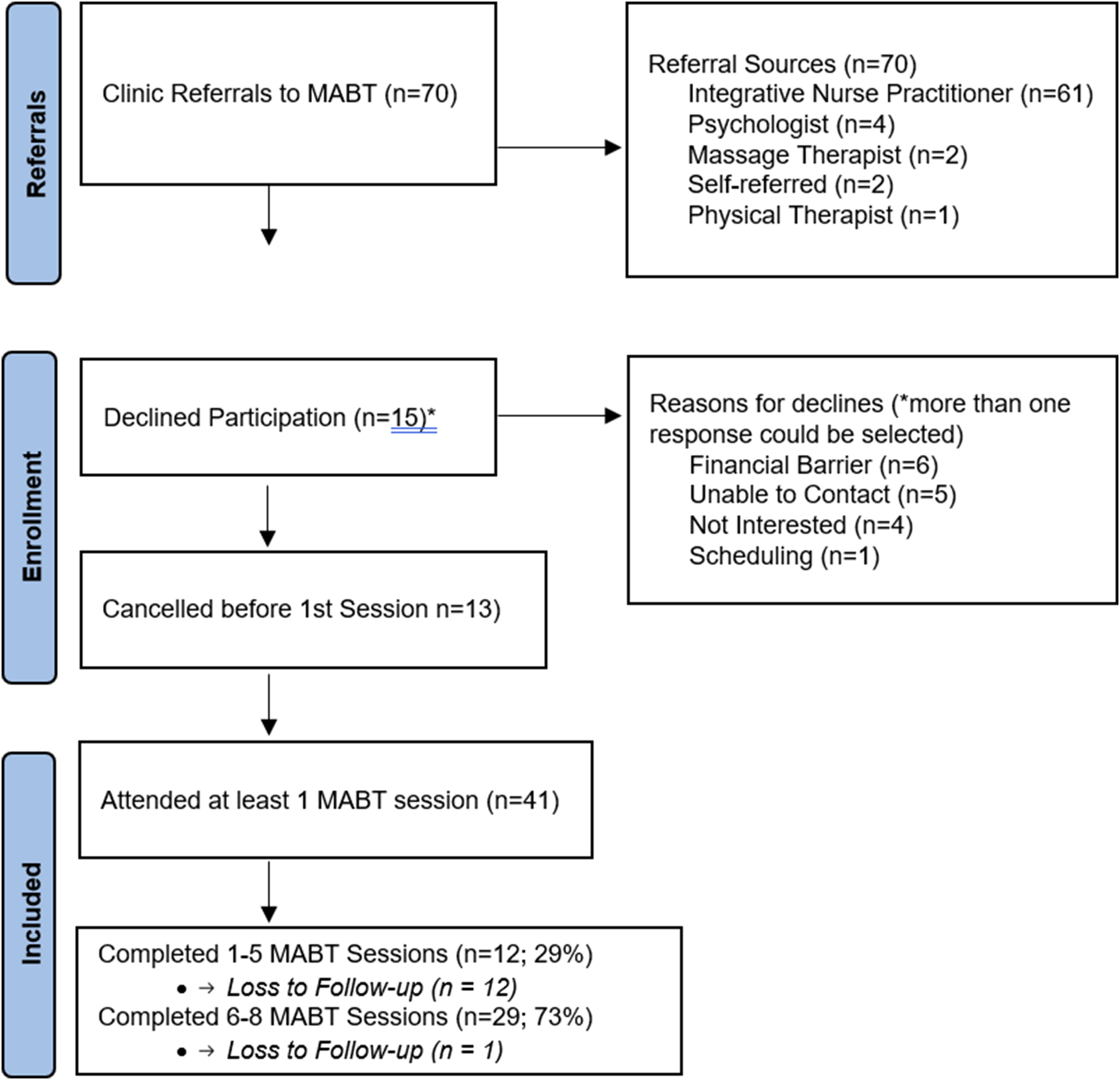
MABT Implementation Delivery Feasibility
All participants attended at least 1 MABT session. Of these, 11 (∼27%) did not complete the intervention but attended between 1-5 total sessions. Reasons for non-completion varied greatly and some are unknown, but were largely due to complicated health or personal circumstances such as co-occurring health issues, surgery and inability to continue in a timely fashion post-procedure, care for family members, financial barriers, etc. Of the 11 who did not finish the intervention, none completed either of the follow-up assessments (at 3 or 6 months).
Thirty participants (73%) completed the intervention program, and with one exception all completed at least one follow-up assessment (see Figure 1).
Sample Characteristics
Participant Characteristics (n = 41).

Change in Health Outcomes: Primary (PROMIS) Outcomes
Physical Function, Anxiety, Fatigue, Sleep Disturbance, Social Role, and Pain Interference demonstrated a minimally important change/difference (MID) from baseline to 3-month and these were maintained to 6-month follow-up. Depression and Pain Intensity did not meet the positive change criteria for a MID. Notable was the number of participants with large reductions in anxiety symptoms. At baseline, sixteen participants (55%) had anxiety T scores at least 1 SD above the norm; at 3-month follow-up 12 (75% of this subgroup) showed a T score reduction of .5-1.5 SD.
Mean Change in Outcomes (n = 29).

Note. Bold text indicates significant P-values after Bonferroni corrections. The F (df) and P-values are from the within subject main effect of time pooled from 10 imputations of the data (multiple imputation).
Abbreviations: PROMIS-Patient-Reported Outcomes Measurement Information System; MAIA- Multidimensional Assessment of Interoceptive Awareness; DERS-SF- Difficulties in Emotion Regulation Scale Short Form; BRS-Brief Resilience Scale; SD- Standard Deviation.
Partial ή2: Physical function = 0.194; Anxiety = 0.119; Depression = 0.046; Fatigue = 0.25; Sleep disturbance = 0.199; Social role = 0.293; Pain interference = 0.241; Pain intensity = 0.191; MAIA (Overall) = 0.441; DERS-SF (Total) = 0.307; BRS = 0.111; Flourish = 0.078.
Change on Secondary Health Outcomes
Repeated measures ANOVAs showed significant improvement and large effect sizes on MAIA Total, F (2, 44) = 22.6, P < 0.0001, ή 2 = 0.44 and DERS Total, F (2, 53) = 12.5, P < 0.0001, ή 2 = 0.31, see Table 3. Post Hoc analyses with Bonferroni adjustments showed that scores increased from baseline to post-intervention (3-month assessment) and from baseline to 6-month follow-up (see Table 3). There were improvements on the Brief Resilience Scale and Flourishing Scale but the changes were not significant although medium effect sizes were observed for both measures (ή 2 = 0.111 and .078 respectively), see Table 3.
Supplement Table 1 Illustrates Change Over Time on the Specific Scales of the MAIA-2 and Subscales of the DERS-SF. On the MAIA, With the Exception of the Not-Distracting Scale, all Scales Showed Significant Mean Improvement and Very Large Effects (Ranging From .26 −.41). On the DERS-SF, Significant Mean Improvement and Large Effects Were Observed on the Awareness, Goals, Acceptance and Impulse Subscales; the Clarity and Strategies Subscale Scores did Not Reach Significance and Lower Effect Sizes Were Observed (See Supplement Table 1).
Correlations Between Change in Outcomes
Baseline to 6-month change in pain interference was moderately and significantly correlated with change on the majority of other PROMIS variables, including physical functioning (r = −.62), anxiety (r = .49), depression (r = .55), fatigue (r = .46), sleep disturbance (r = .37), and highly and significantly correlated with social roles (r = −.80). Change in pain interference was also moderately and significantly correlated with change in interoceptive sensibility (MAIA total) (r = −.61), resilience (r = −.57), and flourishing (r = −.42). In addition, change in interoceptive sensibility was moderately and significantly correlated with change in physical function (r = .49), social roles (r = .57), pain (r = .48), resilience (r = .44), and emotion regulation difficulties (r = −.49) (see Supplement Table 2).
Discussion
This study demonstrated MABT recruitment and delivery feasibility within the context of a real-life clinic, with 50% of the patients scheduling MABT sessions after initial referral, and 73% of those that scheduled completing the intervention. The MABT completion rate was perceived by clinic staff to be high for this clinic population, particularly given that it was for a new and unfamiliar service. 26 The completion rate highlights the perceived value of the program among this chronic pain sample, particularly given the lack of insurance coverage for massage therapy in the region where this study took place, and the consequent requirement that patients pay out-of-pocket for MABT sessions. These findings may reflect a broader increase in patient value of CIH for pain management as reflected in a recent study showing higher CIH utilization for pain management among those with chronic pain in the United States. 39
Six of the eight PROMIS subscales met the threshold for minimally important difference (MID), demonstrating preliminary evidence of MABT’s positive effect on critical outcomes for well-being among those living with chronic pain.33,40,41 There was a significant mean effect across time with high effect sizes (ή 2 range from .19-.29) on the PROMIS subscales of physical function, fatigue, sleep disturbance, social role, pain interference and pain intensity. Notably, the PROMIS outcome improvements that showed significant immediate post-intervention change were maintained or demonstrated further positive change over the follow-up period (to 6 months), indicating a lasting effect. As the majority (n = 15) of these patients had been OCIM patients for some time (1-5 years), these positive and maintained improvements in health outcomes are particularly notable.
In contrast, mean depression symptoms did not significantly change and showed a low effect, likely due to the overall lack of elevated depression symptoms in this sample. Anxiety symptoms, meanwhile, showed a medium effect size. Sixteen out of 29 study participants in this sample had elevated anxiety (above moderate cutoff) and the majority (75%) showed a reduction to below this cut-off, as reflected in the MID. As indicated in Table 2, among the baseline characteristics of study participants, anxiety symptoms showed the most notable difference between the intervention non-completers (who had higher mean anxiety) than the completers. Unfortunately, due to the unexpected lack of assessment response among the non-completers, we do not know how those with high anxiety who did not complete the intervention may have responded to the intervention.
Among the PROMIS measures, the intervention showed the largest effects in Pain Interference (ή 2 = .24), a key indicator of pain management that includes indicators of both affect and activity and Social Roles (ή 2 = .29), an indicator of involvement in and satisfaction with work, relationships and activities. As reflected in the high change correlation between these two scales, these are closely related constructs. Given the selection bias due to a lack of follow-up data primarily among those who didn’t complete the intervention in this small one-group pilot, interpretation of these findings is limited. That said, the observed improvements in pain management and well-being align with recent findings from an MABT study (n = 303) for people on medication for opioid use disorder, 57% (n = 172) of whom had chronic pain, 26 supporting the benefit of interoceptive training through MABT for chronic pain patients.
The baseline PROMIS-29 scores in this cohort were comparable to patients with chronic pain across pain and spine clinics in the United States, 42 with the exceptions of higher fatigue and anxiety among current study participants. The substantial reductions in anxiety symptoms among those with elevated anxiety, and the significantly correlated change between anxiety and pain interference (see Supplement Table 2), highlights the potential relationship between these health outcomes. Fewer participants showed elevated depression compared to anxiety in this sample, so it is unknown whether a similar pattern might be true with depression in a larger sample.
Among the secondary outcomes, the significant immediate and maintained positive change in interoceptive awareness, along with the large effect size, matches findings from prior MABT randomized controlled trials.26,28 A recent neuroimaging study shows that increases in MAIA in response to MABT were associated with increased sensory processing, 43 indicating brain plasticity and potential to develop and change interoceptive capacity in response to interoceptive training. Chronic pain is one of many conditions that is understood to involve interoceptive dysfunction.12,13 These promising findings and the significant change correlations between the MAIA and other study outcomes such as pain interference, physical function, and emotion regulation (see Supplement Table 2) suggest the importance of future study to examine improved interoceptive sensibility as an underlying mechanism for key health outcomes associated with chronic pain.
The reduction and maintained change in emotion regulation difficulties is also notable. Emotion regulation can be described as a person’s ability to modulate the emotional state and expression, and includes which emotions people experience, when and for what duration they have the emotions, as well as how emotions are experienced and expressed. 44 Many studies have found direct associations between emotional dysregulation and chronic pain, pain-related disability, and depressive symptoms. 45 Further, results from cross-sectional and longitudinal brain imaging studies suggest the chronification of pain is correlated with a shift away from acute pain circuits to the engagement of emotion circuits.2-4 Thus, enhancing self-regulation of affective experiences is now considered a candidate mechanism in promoting long-lasting reductions in pain and corresponding comorbidities. Our current findings are congruent with previous studies that suggest training in emotional regulation is associated with improved pain interference, reduced disability, and decreased anxiety among people with chronic pain.45,46
The maintained improvement on many of the health outcomes to the 6-month follow-up matches findings from prior MABT studies in which a maintained effect has been at least partially attributed to the continued practice of interoceptive skills learned in MABT.27,28,47 While take home practice data was not formally collected from patients in this study, the therapists documented use of take-home practice (which is an integral component of the intervention approach), in medical notes associated with each patient session. A review of the medical notes in the electronic medical records indicates consistent use of home self-practice by participants in this project, suggesting the potential positive role of MABT home practice underlying the maintained positive outcomes over time.
The positive changes seen in this study align with the findings from the implementation science portion of this project 26 in which we examined clinic stakeholder perspectives on the acceptability, adoption and uptake of MABT. A key finding related to adoption and uptake of MABT within the clinic was that MABT was perceived to address a gap in clinical services. Specifically, MABT was perceived to be uniquely appropriate for patients who were struggling with emotion regulation difficulties, particularly for those who would benefit from individual guidance and from a somatic approach to learn interoceptive skills to support increased emotional awareness and regulation, and it was suggested that a variety of clinicians be cross trained in MABT to increase potential for delivery and insurance coverage. Relatedly, MABT training is relatively brief and inexpensive compared to many advanced professional trainings, involving an intensive 1-week in-person course followed by subsequent practice and internship involving protocol delivery to two clients with weekly online supervision for certification. MABT can be delivered by therapists/practitioners who are licensed to touch (ie, massage therapists, physical therapists, occupational therapists, nurses) and by mental health therapists utilizing client self-touch. The current study results align with the staff perspective that chronic pain patients needed help with emotion regulation and aligns with literature suggesting that emotion regulation may be a key mechanism underlying positive change on pain related outcomes.5,6
There are multiple study limitations, primary among them is that this was a relatively small one-group study, with a homogenous sample (mostly white and female). As a one-group study, we were not able to compare MABT to usual care, thus limiting our ability to assess treatment effects. Also, only those who completed the intervention were motivated to complete any follow-up assessment, resulting in selection bias. This lack of completion of follow-up assessments by the intervention non-completers was unfortunate but not surprising due to the lack of incentives/payment for assessment, or knowledge among participants that their data would be retrospectively used to assess intervention feasibility. Because of this we were not able to compare health outcomes between those who had fewer vs more MABT sessions, limiting our ability to explore the impact of intervention dose or for whom the intervention may have been most beneficial.
Strengths of this study was the ability to evaluate MABT referral and delivery feasibility in the context of real-life clinic services, utilizing the same overall referral, scheduling, and health outcome assessment procedures as for all other services offered at the clinic; likewise, the intervention was delivered by massage therapists who were clinic employees. While we couldn’t compare the changes in health outcomes to a control group receiving usual care, most participants in this study were long-term patients at this clinic and their baseline outcomes indicated significant distress that changed in response to a relatively brief (8 week) intervention. Future research is needed to address these limitations through a larger randomized controlled trial with a more heterogeneous sample to test treatment effects and inform further efforts toward implementation.
In addition, only self-report measures were used in this pilot project, and it would be recommended to include physiological measures specific to pain processing which would be particularly helpful for examining underlying mechanisms that may be associated with improved interoceptive sensibility among those with chronic pain. For example, future studies may benefit from utilizing micro-longitudinal designs that employ ecological momentary assessment, to allow within-person variations in a range of symptoms to be examined, as well as adjustment for person-level variables. Studies using brain imaging (eg, fMRI or electrophysiology) may shed light on the neural underpinnings associated with interoception and pain.
In conclusion, these findings demonstrate MABT referral and delivery feasibility in the context of a pragmatic real-life clinic context and provide preliminary support for MABT as a potential non-pharmacological intervention for the treatment of chronic pain. Future larger studies of MABT are needed to test efficacy and to examine larger scale implementation as an integral component of clinic services.
Supplemental Material
Supplemental Material - Patient Outcomes Improve in a Pragmatic Implementation Pilot Study of Mindful Awareness in Body-Oriented Therapy (MABT) for Chronic Pain
Supplemental Material for Patient Outcomes Improve in a Pragmatic Implementation Pilot Study of Mindful Awareness in Body-Oriented Therapy (MABT) for Chronic Pain by Cynthia J. Price, Dana Dharmakaya Colgan, Erin Abu-Rish Blakeney, Jacquelyn S. Pennings, Claudia Davidson, Kathryn A. Hansen in Global Advances in Integrative Medicine and Health.
Footnotes
Acknowledgements
The authors would like to acknowledge Taylor Koval LMT and Brian Wingate LMT for their many contributions to this study. We also want to express our appreciation of the study participants, and the Osher Clinic staff at Vanderbilt University.
Authors’ Contributions
C.P., E.B. and K.H. conceptualized and designed the study. J.P. and C.D. managed the data analysis and assisted with data interpretation. C.P, D.C., K.H., and E.B. contributed to data interpretation and manuscript writing. All authors have approved the submitted version and are personally accountable for their individual contributions to this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is supported by Massage Therapy Foundation; University of Washington School of Nursing RIFP Intramural Grant Program (Troop Fund); Dr Abu-Rish Blakeney’s time during data analysis and manuscript writing was supported by an NIH Career Development Award; 1K23HL144910-01A1.
IRB Approval
ClinicalTrials.gov registration: NCT05289024
Ethical Statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.