
Abstract
Background
In 2017, the American College of Physicians (ACP) designated Mindfulness-Based Stress Reduction (MBSR), an eight-week group program, as first-line non-pharmacological treatment for chronic low back pain. However, interprofessional collaboration between mindfulness instructors and Primary Care Providers (PCP) remains largely unknown.
Objective
We developed a survey to assess communication between mindfulness instructors and PCPs, identify predictors of referral to MBSR, and determine areas where interventions could increase patient access to MBSR.
Methods
The 25-question survey was sent via email to PCPs at the Division of General Internal Medicine, University of Pittsburgh, PA, the Piedmont Health Services Family Medicine Section, Chapel Hill, NC, the Boston Medical Center General Internal Medicine and Family Medicine Sections, Boston, MA, and the UMass Memorial Medical Center Family Medicine Section, Worcester, MA. We used descriptive statistics and logistic regression to analyze the data.
Results
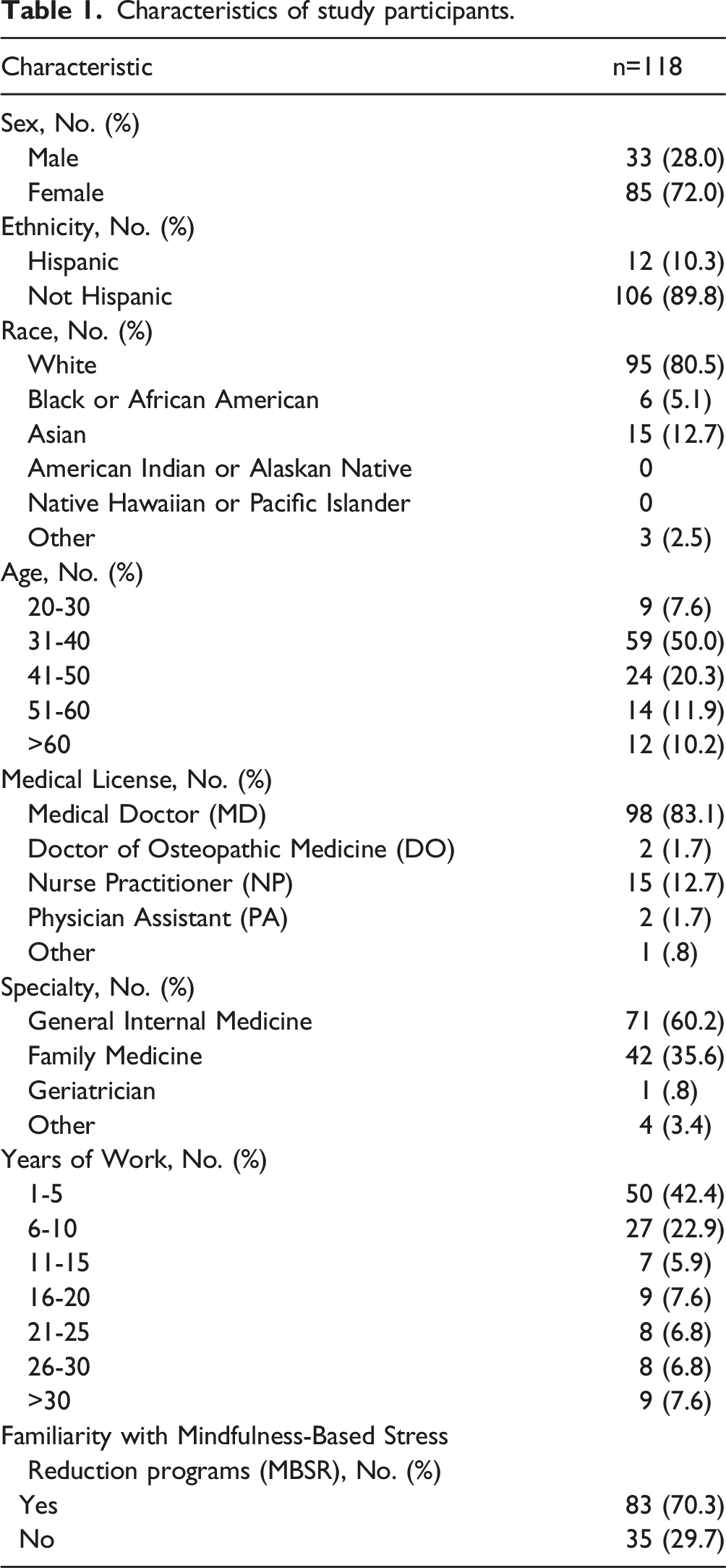
Among 118 eligible respondents, 85 (72.0%) were female PCPs, mean age was approximately 41.5±10.1, and the majority (65.2%) had been in medical practice ≤10 years. Of these PCPs, 83 (70.1%) reported familiarity with MBSR (95% CI: 62.1, 78.5), and 49 (59.0%) of them referred patients at least yearly. Of those who referred, 8 (16.3%) reported collaboration with mindfulness instructors. PCPs who were quite a bit or very much familiar with MBSR had 5.10 (1.10, 22.50) times the odds (P=.03), and those who were 50 years or younger had 3.30 times the odds (P=.04) of referring patients to MBSR. Frequency of PCPs’ personal practice of mindfulness was not significantly associated with referrals (P=.30).
Conclusion
This is the first study to assess interprofessional collaboration between mindfulness instructors and PCPs. Suggestions for a potential integrative health care model are included; further studies on methods to augment communication and education are warranted to improve the referral process and ultimately increase accessibility and utilization of mindfulness-based programs.
Introduction
The rise of mindfulness-based interventions (MBIs) within the integrated health care delivery system has made understanding collaboration between Primary Care Providers (PCP) and allied health professionals increasingly important for delivering the best care to patients with chronic diseases. Interprofessional collaboration has proven to provide many benefits in the health care setting, including improved education of different disciplines within the care team, greater teamwork, and better patient care with respect to shared decision-making in holistic care planning.1-4 Interprofessional care has also led to decreased healthcare utilization for medically complex, low income patients in the form of reduced emergency room visits and hospital admissions. 5 The literature, however, has not addressed interprofessional interactions between mindfulness instructors and PCPs nor referrals to mindfulness-based programs for patients with chronic conditions, such as low back pain.
Low back pain remains the leading cause of disability globally as well as the leading cause of disability in the United States.6,7 The United States spent $134.5 billion on health care for low back and neck pain between 1996-2016, yet the functional status of those suffering from lower back pain has declined despite numerous treatments and medical resources.8,9 Thus, accessible treatments with demonstrated effectiveness such as MBSR, an MBI for persons with chronic low back pain, offer evidence-based solutions to solve this healthcare gap. MBSR is a standardized eight-week program aimed to increase awareness, understanding, and acceptance of present experiences. This MBI has been growing in popularity and has become more available in the United States given its effectiveness in reducing anxiety, stress, depression, and pain.10-12 In its most recent guidelines, the American College of Physicians (ACP, 2017) recommended the use of MBSR as a first-line non-pharmacological treatment for chronic low back pain.13,14
MBIs are being more commonly incorporated into integrative medicine models given their proven effectiveness in treating various diseases. For instance, due to the increased data demonstrating the effectiveness of complementary practices to help treat chronic illness, and increased conventional practitioners practicing complementary health approaches, the integrative medicine model emerged to combine conventional and complementary methods to deliver holistic, patient-centered care.15-18 Integrative models have already shown benefits of mindfulness-based therapies utilized by their patients. For example, a prospective cohort study of Kaiser Permanente Colorado patients with chronic pain, chronic illness, or a stress-related problem and without uncontrolled psychiatric illnesses found that an eight-week MBSR program led to significant improvements in self-reported pain, psychological symptoms, and reduced health services utilization. 19
Findings from randomized control studies further support the incorporation of MBIs into integrative medicine frameworks. In one study for patients in a safety-net health system, those in an integrated, referral-based mindfulness program with a DSM-V diagnosis and without severe mental illness were significantly more effective in health behavior action plan initiation for their chronic diseases. 20 More recently, another randomized controlled study demonstrated that patients in the University of Utah primary care clinics with a physician-confirmed chronic pain diagnosis and were prescribed daily opioid use for 3 months or more but scored high for opioid misuse had significant improvements in chronic pain symptoms, opioid misuse, dosing, craving, and emotional distress when they were part of an 8-week mindfulness program. 21 Despite these positive findings from integrated mindfulness programs, Fuchs et al. 22 underscored how out of 130 eligible patients per month, only 6.5 patients attended the mindfulness-based group because they were not referred by their behavioral health counselor or PCP. While integrating MBIs in the primary care setting has shown initial results of efficacy for patients dealing with chronic diseases, obstacles to referral and participation exist and need to be described so that vulnerable patient populations have access to effective mindfulness therapies. Our study aims to elucidate patterns of collaboration between mindfulness instructors and PCPs as well as determine predictors of PCP referral to MBSR programs.
Methods
Study Design
In this cross-sectional study, we developed a 25-question survey that addressed the Interprofessional Education Collaborative’s Core Competencies of Values/Ethics, Roles/Responsibilities, Interprofessional Communication, and Teamwork between mindfulness instructors and PCPs. 23 The first competency, Values/Ethics, aims for mutual respect and values to be shared among different professions. The second, Roles/Responsibilities, requires a baseline knowledge of roles between providers so that the health care needs of the patient can be appropriately assessed and addressed. The third competency, Interprofessional Communication, identifies the importance of communication with patients, families, communities, and professionals from different fields while the fourth, Teamwork, recognizes the effectiveness of team dynamics in delivering patient-centered care. There were 7 questions for Values/Ethics (e.g., “How willing are you to learn about Mindfulness-Based Stress Reduction Programs to help your patients with chronic low back pain?”), 3 questions for Roles/Responsibilities (e.g., “How aware are you of the interventions used by the Mindfulness instructors in their sessions?”), 7 questions for Interprofessional Communication (e.g., “How would you rate your communication with the Mindfulness instructors?”), and 3 questions for Teamwork (e.g., “How much would you want to work in an interprofessional care setting with Mindfulness instructors?”). Values/Ethics were assessed for all study participants while the latter 3 domains, Roles/Responsibilities, Interprofessional Communications, and Teamwork, were only assessed for those who collaborated with MBSR instructors. Questions were adapted and modified from Ward et al. 24 where attitudes of Australian medical oncologists toward collaboration with palliative care services were evaluated. We did not entirely utilize existing surveys as we were particularly interested in barriers to collaboration and wanted to ascertain attitudes based on the Interprofessional Education Collaborative’s Core Competencies. The 5-point Likert Scale was used to rank the answers. Anchors are included in Appendix A. Adaptive questioning was used to direct those who indicated that they were not familiar with MBSR, never recommended MBSR to their patients with chronic low back pain, or never collaborated with mindfulness instructors to the end of the survey.
Demographic data including sex, race, ethnicity, age, medical licensure, years of practice, and specialty along with four open-ended questions regarding participants’ beliefs on the effectiveness of MBSR for patients with chronic low back pain were also included (Appendix A). By asking how PCPs developed their knowledge of MBSR (e.g., “How did you develop your knowledge of Mindfulness-Based Stress Reduction?”), whether there was apprehension or barriers to referrals (e.g., “Do you believe providers are apprehensive about referring their patients to Mindfulness-Based Stress Reduction for pain management? If so, why?”), and positive/negative experiences working with mindfulness instructors, the open-ended questions were used to determine areas of intervention for improving PCP knowledge and referrals to MBSR. 25 This survey research study was approved by the Boston Medical Center and Boston University Medical Campus Institutional Review Board.
Data Collection
The survey was created in REDCap, a secure online survey application, and responses were recorded anonymously. The survey’s REDCap link was originally sent out via email to Administrative Assistants at three health care system sites where MBSR programs were available. These sites included the Division of General Internal Medicine, University of Pittsburgh, PA, the Piedmont Health Services Family Medicine Section, Chapel Hill, NC, and the Boston Medical Center General Internal Medicine Section, Boston, MA. Additionally, the UMass Memorial Medical Center Family Medicine Section, Worcester, MA and Boston Medical Center Family Medicine Section, Boston, MA were later added as recruitment sites in order to reach the goal number of respondents, i.e., 100.
Inclusion/Exclusion Criteria
Participants had to read the Exempt Information and consent to take the survey. PCPs needed to meet the following inclusion criteria: 1) Belong to one of the following institutions: UPMC General Internal Medicine Division, Piedmont Health Services Family Medicine Section, UMass Memorial Medical Center Family Medicine Section, or Boston Medical Center Family Medicine or General Internal Medicine Sections; 2) Be 18 years of age or older; 3) Be a licensed PCP; and 4) Be English-language speaking. Participants who filled out a completed survey were then invited to voluntarily provide their names and email addresses to be entered in a lottery to win a $500 gift card.
Statistical Analysis
Data was collected between March 12th and June 23rd, 2021. Only completed surveys agreeing to participate and meeting inclusion/exclusion criteria were analyzed. Data from non-responders were not collected given the nature of the survey as it was sent out broadly to all eligible PCPs and information could only be collected from responders. Descriptive statistics computed for demographic characteristics and participant responses to survey questions included number of responses per category as well as their percentages. Logistic regression modeling was used to estimate the odds ratios and their 95% confidence intervals of referring patients to MBSR programs. The analysis was restricted to those who were familiar with the MBSR program (n = 83). Unadjusted and full adjusted analyses were performed on the demographic characteristics found in Table 2, and variables whose unadjusted p-values were less than .25 were reported in Table 3. The variable of familiarity with the MBSR program was grouped into two groups (a little bit or somewhat, quite a bit or very much). Categories were collapsed for some variables due to limited sample sizes and the inability to include some Likert scale variables in a model without a reduction in the number of parameters to be estimated. All statistical analyses were performed using SAS version 9.4 at an α=.05 level of significance. Description of the open-ended questions was based on the recurring types of answers received, i.e., work, education, and personal experience for the question about developing knowledge of MBSR; and lack of knowledge, low patient acceptance, insurance coverage/referral difficulties, and availability/accessibility of MBSR programs for the question about apprehension in referring to MBSR.
Results
Study Participants
Characteristics of study participants.
Values/Ethics
A summary of study participant response breakdowns are included in Figure 1. Out of 118 PCPs that responded, 70.3% (n = 83) reported being familiar with MBSR programs with a 95% confidence interval (62.1 - 78.5). Of the 83 PCPs that were familiar with MBSR, 83.1% (n=69) were a little bit or somewhat familiar with MBSR (Table 2). For the 29.7% (n=35) who were not familiar with MBSR, 97.1% (n = 34) were at least a little bit willing to learn about MBSR to help their patients with chronic low back pain. Of the 83 participants, 66.3% (n=55) indicated that they themselves practiced mindfulness meditation at least yearly and 67.4% (n=56) of them reported that, to their knowledge, there were mindfulness programs available to their patients at their current institution (Table 2). In terms of recommending MBSR to their patients with chronic low back pain, 59.0% (n = 49) of the 83 participants familiar with MBSR reported that they did refer their patients to MBSR programs (Table 2). Of the 34 PCPs who did not recommend patients to MBSR, 94.1% (n=32) were at least a little bit interested in doing so. Only 16.3% (n = 8) of the PCPs who recommended MBSR collaborated with the mindfulness instructors about the care of their patients with chronic low back pain. The other 83.7% (n = 41) were at least a little bit willing to collaborate with mindfulness instructors. Breakdown of survey responses. Characteristics of study participants familiar with MBSR by their status of patient referral to MBSR programs.

Roles/Responsibilities
All eight PCPs who collaborated with mindfulness instructors were at least a little bit aware of the interventions used by mindfulness instructors in their sessions. They also agreed or strongly agreed that MBSR should be considered as a treatment option for chronic low back pain. In terms of the power differential for patient care responsibility between mindfulness instructors and PCPs, 62.5% (n=5) stated that they were neutral and 12.5% (n=1) agreed that there was a power differential.
Interprofessional Communication
All eight PCPs who collaborated with mindfulness instructors did so at least yearly and reported that their collaboration increased the quality of their patients’ care at least a little bit. Of these eight PCPs, 12.5% (n=1) reported not being able to express their concerns about patient care to mindfulness instructors. The other 87.5% (n=7) felt at least a little bit able to do so. On the other hand, 87.5% (n=7) of the PCPs felt that the mindfulness instructors were somewhat able to express their concerns to them while only 12.5% (n=1) reported that mindfulness instructors were not at all able to express their concerns. Additionally, 62.5% (n=5) of the PCPs believed that greater communication with mindfulness instructors would be more effective in managing their patients' chronic low back pain while 12.5% (n=1) disagreed and 25.0% (n=2) were neutral.
Teamwork
All eight PCPs who collaborated with mindfulness instructors were somewhat interested in working in an interprofessional care setting with mindfulness instructors as well as somewhat interested in doing so in an online format such as Zoom, Google Hangout, Skype, etc. But in regards to referring their patients to online MBSR sessions, the eight PCPs were split, with 50.0% (n=4) being neutral or disagreeing that they would, while the other 50.0% (n=4) agreed or strongly agreed.
Predictors of Referral to MBSR
Predictors of patient referral to MBSR programs. Age younger than 50 years old and greater familiarity with MBSR were significantly associated with referrals to MBSR. Frequency of PCPs’ personal practice of mindfulness meditation was not significantly associated with referrals to MBSR.

*P-value < .05
Top Reasons for Developing Knowledge of MBSR from Open-Ended Questions
PCPs who were familiar with MBSR reported developing their knowledge of mindfulness through many different avenues. We grouped the total number of answers (n=65) to this free response question into three different categories: education (56.9%), work (26.1%), and personal experience (35.3%). Education included residency education (e.g., “It was part of my training in residency.”), medical school education (e.g., “From my medical school. I did work with a mentor who taught meditation.”), Grand Rounds presentations, and continuing medical education courses (e.g., “CME course through Harvard years ago.”). Work included their institutional programs (e.g., “This is incorporated through VA Pittsburgh as a part of the Whole Health approach to treatment of patients with chronic medical conditions and pain which had mindfulness integrated in their practices.”), research (e.g., “We have researchers in the division.”), and colleagues (e.g., “Discussion among other primary care clinicians.”). Personal experience included interest (e.g., “I am aware of this generally as I read about alternative and complementary therapies.”) and personal practice (e.g., “taught meditation by a meditation teacher, do yoga regularly.”).
Top Reasons for Provider Apprehension Towards MBSR
There were also a number of reasons as to why providers were apprehensive about referring patients to MBSR. We grouped the total number of answers (n=47) to this free response question into four different categories: lack of knowledge (27.6%), low patient acceptance (29.7%), insurance coverage/referral difficulties (23.4%), and availability/accessibility of MBSR programs (29.7%). Lack of knowledge included providers’ lack of insight about the evidence-based benefits of MBSR (e.g., “I think there is lack of knowledge about it and its efficacy and hesitancy about how to frame to patients.”). Low patient acceptance included providers’ beliefs that patients would not be willing to try MBSR (e.g., “Because of the fear of patients rejecting this idea outright, and then expressing that we as physicians must not be taking their pain seriously if our recommendation is mindfulness, not, say, medication or surgery. Basically fear of losing or breaking trust.”). Insurance coverage/referral difficulties included providers’ lack of knowledge about insurance coverage for MBSR programs and how referrals to these programs work (e.g., “there are no available programs covered by insurance.”). Availability/accessibility of MBSR programs included providers’ lack of knowledge about whether MBSR existed in other languages and how feasible it was for patients to enroll in such programs (e.g., “I am not sure if these services are available in languages other than English and if the cost would be prohibitive.”).
Discussion
Our study sought to address a gap in the literature concerning patterns of collaboration between mindfulness instructors and PCPs and ascertain predictors of referral to MBSR for patients with chronic low back pain. We developed a survey with questions based on the Interprofessional Education Collaborative’s Core Competencies of Values/Ethics, Roles/Responsibilities, Interprofessional Communication, and Teamwork. We found that a majority of PCPs had a general idea about MBSR programs and were willing to refer their patients with chronic low back pain to the program. However, much fewer had actually referred patients as part of their practice in addition to collaborating with mindfulness instructors.
Interprofessional Collaboration Between Mindfulness Instructors and PCPs
Only 6.8% of the 118 respondents (n=8) reported some type of collaboration with mindfulness instructors. Since the few providers who communicated with mindfulness instructors found that it improved patient care, methods to augment communication should be considered. This could include use of a common electronic health record or integrating medical practitioners with mindfulness instructors in the healthcare setting or over online formats that would allow for more efficient and effective communication.26,27 From survey responses, PCPs were somewhat interested in working in an interprofessional care setting with mindfulness instructors and were also open to doing so via online platforms, probably due to ease of communication. With the onset of the COVID-19 Pandemic making online communication platforms more accessible, there has been an increased comfort level in using web-based video platforms for meetings. 28 We are currently testing this online platform in a pragmatic clinical trial of MBSR delivered via Telehealth. 29 Although Wahbeh et al. 30 reported that their participants actually preferred the internet format over individual or group formats for mindfulness meditation interventions, PCPs in our study were not unanimous concerning online referrals to MBSR. It may be beneficial for future studies, such as qualitative investigations, to assess the rationale behind PCPs’ preferences for in-person MBSR courses compared to online offerings.
Factors Impacting Referral to MBSR
We found that age less than 50 years old and more familiarity with MBSR were significantly associated with referrals to MBSR. It is possible that PCPs who were 50 years old or younger were more likely to be exposed to MBSR in their medical school education or through other forums of continuing medical education. Increased familiarity with MBSR could mean more PCPs were aware of the benefits of this program for alleviating chronic low back pain and were therefore more likely to refer their patients. These associations highlight the need to expose and educate clinicians about the evidence-based benefits of MBSR for chronic low back pain early in their careers.
Other factors impacting referrals that we acquired from open response questions include inadequate knowledge with respect to the efficacy of mindfulness-based programs, the referral process, and accessibility to programs. Providers believed that their patients would prefer medications, which are covered by insurance, and tend to work more quickly than an 8-week program. This belief held by patients that medications are more effective than non-pharmacological pain treatment modalities (NPM) has been described as a barrier to the usage of NPMs. 31 Many misconceptions currently exist around mindfulness-based interventions including the lack of knowledge pertaining to both efficacy as well as safety.32,33 However, there is extensive literature detailing the effectiveness of mindfulness meditation for the treatment of illnesses such as stress, depression, substance abuse, and chronic pain. 34 Studies are beginning to argue against the harmful adverse events experienced during mindfulness meditation sessions.35,36 Furthermore, the risks associated with mindfulness meditation are significantly lower compared to conventional therapies for chronic low back pain, such as addiction, overdose, and depression with long-term opioid use; gastrointestinal, cardiovascular, and renal risks with NSAIDs; and operative and postoperative complications with surgery.14,37,38 While PCPs who worked with mindfulness instructors did not report barriers to interprofessional collaboration between the two fields of healthcare, knowledge of what mindfulness instructors do in their MBSR sessions was a possible reason as to why providers were not able to educate their patients about the benefits of MBSR. Becker et al. 31 also described how the lack of awareness and knowledge from both providers and patients about what NPMs entailed led to another barrier of NPM utilization.
In terms of accessibility, some PCPs stated that they forgo MBSR as a treatment option for their chronic low back pain patients because insurances to their knowledge do not cover such programs. Lack of referral knowledge could explain why 55 PCPs reported that there were mindfulness programs available to their patients with chronic low back pain at their current institution but more than half indicated that they never recommended them. In addition, PCPs who were aware of MBSR programs available were still not able to refer non-English speaking patients due to the lack of availability of such programs. This highlights the need for more culturally adapted MBSR programs. Considering Castellanos et al. 39 ’s systematic review and Roth & Stanley 40 ’s study, literature suggests that completion of culturally adapted MBSR programs leads to fewer chronic pain visits and greater improvement of mood and illnesses. Therefore, efforts to increase the availability of these programs in other languages are critical. Becker et al. 31 highlighted this finding as well, noting that high cost of treatment and lack of NPM availability were important access barriers.
Education and Support for PCPs Regarding Mindfulness-Based Care for Chronic Pain Patients
Besides increased knowledge of mindfulness programs for better overall patient care and more referrals, patients’ ratings of clinical encounters suggest that patient-centered care increased when their clinicians were more mindful, less stressed, and less burnt out.41-43 Methods of acquiring information about MBSR which could be readily integrated into the medical curriculum include Grand Rounds, medical school/residency lectures, and even participatory MBSR programs for providers, i.e., truncated options but teaches the concepts sufficiently. Multiple studies have already investigated avenues of developing physicians’ knowledge of mindfulness. Virtual curricula consisting of online videos, live instruction, and self-study modules were found to be effective in promoting well-being in physician assistants, interns, residents, and attendings at both community and academic health centers.44-48 Additionally, medical students have shown interest in learning and practicing mindfulness during clinical rotations. 49 Rac & Chakravarti 50 have proposed eight recommendations on how to integrate mindfulness practices for education and student benefit into the medical school curriculum. These include institutional support, building mindfulness into the curriculum, making sessions selective rather than mandatory, utilizing certified mindfulness facilitators, incorporating mandatory introductory workshops before beginning the mindfulness courses, maintaining a consistent schedule, using comfortable, accessible spaces, and crafting mindfulness sessions around evidence-based MBIs, such as MBSR.
A possible solution to the problems of referral, reimbursement, and health equity access is the integration of the group medical visit in primary care practices. Thompson-Lastad et al 51 found that safety-net institutions in 11 states which offered integrative group medical visits (IGMVs) to treat a range of chronic conditions improved access to non-pharmacologic approaches to chronic illness care and health promotion. IGMVs entail shared medical appointments of 5-20 patients in the same space where providers spend 1-3 hours combining biomedical care with complementary health approaches such as meditation, yoga, or acupuncture for visits including prenatal care, diabetes management, and chronic pain support. 52 Providers can bill patients’ insurance as a standard medical appointment but guidelines for billing insurance remain unclear.53,54 That being said, IGMVs for chronic pain have been associated with outcomes such as lower pain intensity, less opioid medication use, and reduced depressive symptoms.55,56
Clinical Applications
In the Canadian integrative healthcare clinics (IHC), Gaboury et al. 57 endorsed dual education and/or training as a possible input of teamwork that facilitated interprofessional collaboration by reducing barriers and conflicts and contributing to an increased awareness of other healthcare paradigms. Thus, an ideal integrative health care model would include integrative group medical visits with a robust compensatory billing system, interprofessional teamwork between conventional and complementary health practitioners with options for in-person collaboration or telehealth, and education of other health care disciplines to facilitate better partnerships. Using a model where PCPs understand the value of mindfulness therapies, can refer patients to programs without barriers to care, and can collaborate easily with allied professions will undoubtedly lead to better overall patient-centered care and outcomes.
Strengths and Limitations
Strengths of this study include a large sample of PCPs and multiple study sites from four United States cities with differing health care systems. Limitations involve responses from majority white-identifying physicians, MD providers, and female doctors. A web-based survey, rather than mailed, was chosen due to time and cost savings as well as the advent of the COVID-19 Pandemic. 58 However, this leads us to potentially forgo participants who would have preferred to fill out a paper survey instead. Another limitation is that we did not include a definition of mindfulness meditation in the survey as mindfulness meditation has many definitions in literature. 59 However, this question was within the context of MBSR, not other forms of MBIs, in order to set the frame of reference for the participants. We also did not specifically define what familiarity with MBSR programs meant (familiarity with evidence or outcome), and PCPs answered this question based on their own interpretations of MBSR. Unfortunately, a qualitative analysis of open-ended questions could not be conducted due to the paucity and brevity of responses by participants; only results for the first questions were included as associated responses were more substantial in content and length. Additionally, although unadjusted and full adjusted analyses were performed to focus on the covariates of age, more than half of the sample (70.3%) were between the ages of 31 and 50, and future studies should consider a broader age range.
Directions for Future Research
The generalizability of these findings to other health care settings (inpatient) and populations (rural) in the United States is unknown. Future surveys would need to assess institutions where MBSR is not offered as well as locations not geographically located in the eastern United States. We also directed this survey to primarily departments where PCPs operate, such as General Internal Medicine and Family Medicine. Future studies could also focus on including other sections that encompass PCPs, such as Pediatrics and Oncology. In addition, this survey could be adapted to evaluate mindfulness instructors’ attitudes towards PCPs. This information would yield a more complete insight into interprofessional relationships between PCPs and allied health professions. While we assessed frequency of meditation practiced by PCPs, we did not query actual time practiced as meditation can vary widely between practitioners of mindfulness. Since physicians have voiced difficulties in fitting a formal training program on mindfulness into their schedules, research to develop and assess other modes of mindfulness education are needed, i.e., workshops or grand rounds, psychoeducational handouts on mindfulness meditation and benefits for providers to read, and encouragement of providers to take part in MBIs offered in their medical setting. 60
Conclusion
We found that while most of the PCPs in our sample had a general understanding about MBSR programs, less than half recommended it to their patients, and only a few actually interacted with mindfulness instructors. PCPs also did not have to practice mindfulness themselves in order to refer patients to MBSR. Given that patient care improved with increased communication between mindfulness instructors and PCPs, methods such as integrative practices would allow for better communication. Moreover, since younger age and more familiarity with MBSR were significantly associated with referrals to MBSR, opportunities aimed at bolstering educational programs are essential in educating PCPs about the evidence-based efficacy of MBSR in treating chronic low back pain. This would ease their comfort in referring patients as well as their confidence in educating their patients about the non-pharmacological benefits in alleviating their pain symptoms.
Supplemental Material
Supplemental Material - Characterizing Interprofessional Collaboration and Referral to Mindfulness-Based Stress Reduction Programs
Supplemental Material for Characterizing Interprofessional Collaboration and Referral to Mindfulness-Based Stress Reduction Programs by Dhanesh D Binda, Janice M Weinberg, Tra Nguyen, and Natalia E Morone in Global Advances in Health and Medicine
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported within the National Institutes of Health (NIH) Health Care Systems Research Collaboratory by the NIH Common Fund through cooperative agreement U24AT009676 from the Office of Strategic Coordination within the Office of the NIH Director and by the NIH through the NIH HEAL Initiative under award number UH3AT010621 from the National Center for Complementary and Integrative Health (NCCIH). This work was also supported by the NIH through the NIH HEAL Initiative under award number U24AT010961. The content was solely the responsibility of the authors and does not necessarily represent the official views of the NIH or its HEAL Initiative. This work was also supported by K24AT011561 from NCCIH.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.