
Abstract
Background
The well-being of healthcare teams is an important consideration when seeking to improve patient experience and quality of care. Prior studies have found that changes to working conditions are most effective in improving clinician well-being. Integrative Group Medical Visits (IGMVs) modify working conditions in ways that have potential to improve clinician experience.
Objective
The objective of this study was to understand healthcare teams’ experiences with IGMVs.
Methods
In this qualitative study, interviews were conducted via Zoom and telephone with 21 clinicians, administrators, and staff from safety-net healthcare settings throughout the United States (U.S.) who have implemented IGMVs for patients with chronic pain. Interviews included questions about clinician experience, well-being, and satisfaction with the IGMV model. Interviews were recorded, transcribed, and coded using thematic content analysis by a team of trained qualitative researchers.
Results
The authors identified five themes describing how IGMV positively affected clinician well-being: organizational supports, human-centered engagement, collaboration with an interprofessional team, provision of guideline-concordant care, and enhanced meaning and purpose for the clinicians.
Conclusion
The current study was the first to use interviews from healthcare teams who have implemented IGMV to assess their experience. The themes identified warrant further investigation into IGMVs as a strategy to promote clinician well-being and mitigate aspects of burnout.
Introduction
Poor clinician well-being broadly impacts healthcare and has increased dramatically since the start of the COVID-19 pandemic. In 2020, 38% of physicians in the United States (U.S.) had at least one manifestation of burnout, which increased to 63% in 2021. 1 Burnout is characterized by emotional exhaustion, depersonalization, and decreased sense of personal accomplishment. 2 Root causes range from increasing productivity demands, shorter visits with patients, challenges in providing care to sicker and more complex patients, micromanagement of practice by insurance and administration, financial constraints, and long work hours. 2 Higher rates of burnout are associated with increased staff absenteeism, more medical errors, and diminished patient safety. 3 The Institute of Healthcare Improvement has prioritized supporting clinician well-being as one of its five key healthcare improvement goals, referred to as The Quintuple Aim. 4 Despite recent efforts, clinician burnout remains a significant challenge in healthcare. While burnout can be found in all positions and levels of healthcare, primary care clinicians are at particularly high risk. Studies have shown up to 70% of primary care physicians suffer from burnout, rates that are second only to residents. 5
In 2021, approximately 20.9% of U.S. adults experienced chronic pain. 6 To manage subacute and chronic pain, the CDC recommends prioritizing noninvasive nonpharmacologic approaches including exercise therapy, manual therapy, mind-body practices, massage, and cognitive behavioral therapy as first-line treatments. 7 Additionally, the Department of Health and Human Services’ National Pain Strategy has recommended a biopsychosocial approach which should be evidence-based, integrated, and interdisciplinary treatment. 8 Primary care clinicians have reported that limited time during visits and insufficient resources can make treating this complex patient population more difficult. 9 Thus, primary care clinicians treating patients with chronic pain may struggle to provide the recommended guideline-concordant care due to organizational constraints, which could negatively impact their well-being as clinicians.
Burnout is most effectively addressed with organizational-level approaches, specifically changes in working conditions. 10 The group medical visit model (GMV) alters the environment at the organizational level and is a change in healthcare service delivery. Clinicians involved in GMVs experience increased workplace satisfaction due to a shift in roles, allowing increased trust between clinicians and patients, improved patient self-management, and better understanding of patient backgrounds. 11 GMVs were defined in a recent systematic review as multiple patients receiving care concurrently in the same room or telehealth session, a licensed clinician billing and documenting the visit, and patient interaction occurring. 12 According to a systematic and scoping review of 55 studies on GMVs, session durations were on average 90 minutes and frequency of the sessions varied depending on the medical condition, from 1 to 10 sessions. 13 Group visits were facilitated by one to two health professionals, had common defining themes such as a shared medical condition, didactic components like medical topics and lifestyle modifications, and most included experiential learning or activities. 13 Of the 55 studies, 13 included mind-body or integrative medicine components. 13
Integrative Medical Group Visits (IMGVs) for chronic pain were originally developed in 2012 at Boston Medical Center and are a combination of established GMV models, principles of mindfulness-based stress reduction, and evidence-based integrative strategies for managing chronic pain. 14 They are led by a primary care clinician and a co-facilitator and are reimbursable by insurance. 15 Co-facilitators of the group can have various professional roles, examples include a nurse practitioner, acupuncturist, mental health provider, yoga teacher, or group program coordinator. 16 In a single-blind randomized controlled trial, there was a significant reduction in pain medication use, an increase in mental quality of life attributable to the intervention, and a reduction in emergency room visits in the group participating in IMGV compared to the group that had a single primary care visit. 14 A study conducted in 2017 found that at least 11 states were conducting IGMVs. 16 A more recent survey of integrative medicine in community health centers found that 43.7% of respondents from 32 states and territories were offering GMVs, though the proportion of those providing “integrative” services is unclear. 17
Previous pilot studies have investigated IGMVs for chronic pain and found it to be feasible and effective. 15 The present study examines how the IGMV model influences healthcare teams’ experiences. The purpose of this study was to understand the perspectives of clinicians when planning, implementing, and maintaining IGMV in safety-net healthcare settings.
Methods
Study Design
Researchers recruited clinicians, administrators, and staff from safety-net healthcare settings across the United States with experience implementing IGMVs for patients with chronic pain to participate in semi-structured interviews via Zoom teleconferencing. The overall aim of the parent study was to identify implementation determinants (ie, barriers and facilitators) for IGMVs in safety-net settings. As part of the study, the researchers asked participants about their perceptions of the impact of delivering IGMVs on clinician’s experiences of their work. It became apparent that clinician experience is an important consideration during the implementation of IGMV, so the current analysis thoroughly explores themes specifically related to clinician experience. The interview guide for the parent study was developed based upon the domains of the Consolidated Framework for Implementation Research, 24 a widely used implementation framework, to assess barriers and facilitators to implementation of IGMV.
Sample
To be included, IGMVs were billed and documented by a licensed clinician, multiple patients received care in the same room or telehealth meeting, patients interacted with one another, and integrative healthcare in the form of mind-body practice occurred. 18
Recruitment
The team used purposive and snowball sampling to recruit a sample representing geographically diverse areas of the United States. 19 Researchers recruited participants through notifications sent through e-newsletters from multiple integrative health professional organizations.
Data Collection
An experienced qualitative researcher (IR) conducted all interviews using a semi-structured interview guide developed in consultation with experienced qualitative researchers with expertise in IGMVs and implementation science (PG, JL). The study was approved by the University of North Carolina-Chapel Hill Institutional Review Board (21-3380) and considered exempt. Before beginning each interview, participants gave verbal consent to participate in the research study. Questions related to clinician experience were intended to assess if delivering IGMVs were feasible and acceptable to clinicians. Questions included “I’d like to hear more about your experiences with providers who participate in IGMV”, “What do you hear from providers about participating in this program?”, “What do they get out of the program?”, “What about for you, how is the load that you have, and how does doing this work affect you?”, “How was that experience for you of facilitating the groups and running the groups that you had designed?”
Interviews were audio-recorded via HIPAA-enabled Zoom 20 and recordings were transcribed using an encrypted transcription service, DataGain. 21 A team of research assistants verified transcripts by listening to each audio recording and confirming that the written transcript reflected what was said verbally. The team then uploaded verified transcripts into ATLAS. ti 23.3.4.28863 for Windows 22 for analysis.
Data Analysis
For the parent study, two team members independently coded transcripts using directed content analysis, 23 guided by the Consolidated Framework for Implementation Research, 24 to categorize barriers and facilitators to implementation of IGMV. Because the current analysis was not focusing on barriers and facilitators to IGMV in general, it was considered a secondary analysis with the focus being clinician experiences with IGMV. 25 The primary researcher (IR), who interviewed the participants for the parent study, was involved throughout this secondary qualitative analysis to ensure the contexts of the interviews were captured. 26 No additional interviews were conducted on the topic of clinician experience, only interviews from the original dataset were used. 26 The team did a second round of coding on a subset of the original dataset on text initially coded as “Implementation Process: Reflecting and Evaluating: Clinician Experience”. A trained researcher (MJ) then used an inductive thematic content analysis approach to identify themes within the specific topic of clinician experience. 29 MJ collaborated closely with the principal investigator (IR) throughout the secondary analysis to identify themes through iterative grouping of codes and discussion.
Results
Participant Characteristics.
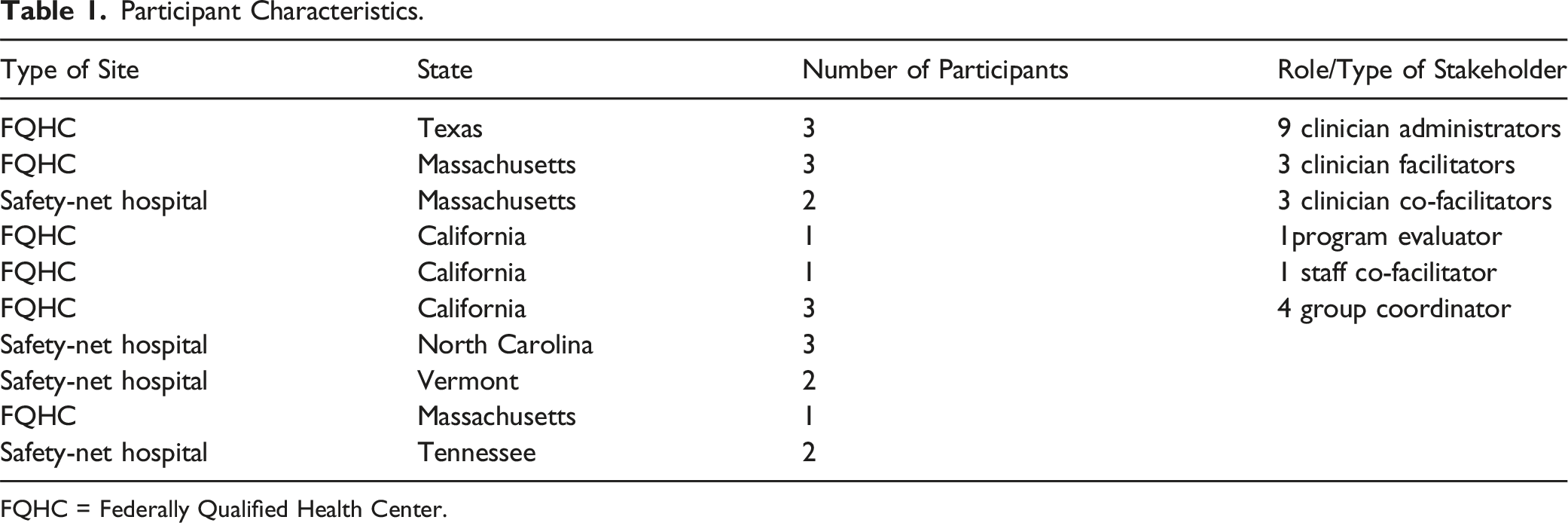
FQHC = Federally Qualified Health Center.
Thematic analysis of the transcripts relating to clinician experience resulted in five main themes related to the impact of IGMV on well-being, which will be described in more detail below. The identified themes are: (1) importance of organizational support, (2) human-centered engagement, (3) working with an interprofessional team, (4) providing guideline-concordant chronic pain care, (5) enhanced meaning & purpose for the clinicians.
Importance of Organizational Support
Interviews with staff and clinicians involved in IGMVs noted the importance of a supportive environment during the development and implementation of the group model. Participants emphasized the need for support from administration and upper management, provision of adequate training, and fair employment of integrative practitioners.
Administrative Support
Developing an original IGMV curriculum and recruiting patients to participate are tasks that clinicians find time consuming and challenging to take on. One participant noted that the initial phases of group development were demanding and that their organization ultimately found ways to reduce the burden. The organization hired a full-time group visit coordinator to help with implementation and site-specific group visit coordinators to support ongoing patient recruitment and retention. “Starting a group for a clinician, it used to be a daunting task. We took a lot of that work off of them, so it's something that's enjoyable again...not having to worry about recruitment and onboarding, and finding the patients and making sure the templates are correct in all of those small technical details, it's a lot more enjoyable for them to do the work.” -Group coordinator, 112
Starting a group was challenging and its maintenance required coordination and administrative support. “At the beginning, the prep work is the bulk and nobody's thinking about anything else, but after that launch it's not done, it doesn't go away. So, all of that work is still there and [we] just still have to maintain it.” -Group coordinator, 112
The groups required reminder phone calls, scheduling, and planning, which burdened the clinicians if they had to manage them. “I would call all the patients in between the weeks. So, between the sessions. So, Wednesday was a session, I would call them Friday, Saturday, Sunday, remind them, then call them before the session started. So I think I would spend like an hour or an hour and a half between the sessions to do this job…” -Intern, 125
One organization started with adequate administrative staff, but due to staffing changes during the COVID-19 pandemic, clinicians had to perform the coordination and administrative tasks instead. “The clinicians and the facilitators who were involved...had a ton of support. Like they weren't necessarily the ones who had to get food, get snacks, check people in, make reminder phone calls... all of those components were handled by staff during pandemic...[but] with folks getting deployed then they never came back, and then all of that work of the coordination was put on the facilitators. So much harder. Yeah, it's too much. I mean, reminder phone calls alone.” -Evaluator, 109
As the clinician above stated, expecting clinicians to facilitate the groups, document them in the medical records, and perform administrative tasks was “too much.”
Upper Leadership Support
Participants reiterated that having the support of upper management to approve appropriate staffing to assist with administrative tasks was essential. Additionally, having the support of leadership could make the development, implementation, and maintenance of groups easier overall. “Leadership buy-in is super important. I think thinking through the arguments… in terms of how integrative group medical visits [have] the potential to address so many different needs and highlighting what those needs… depending on the audience, [and] just really garnering that support as early on as possible and having that just be part of the climate.” -Evaluator, 109
The above clinician reflected that being able to communicate how IGMV can address patient needs can help bolster the support of upper management. Having the support of leadership not only allowed for adequate staffing for administrative tasks but also helped garner support for fair reimbursement of integrative practitioners. Though employment of integrative practitioners is not an essential component of a successful IGMV program, it is important that all facilitators and clinicians are fairly compensated. “That's another phenomenon is that I think we're looking at how we employ the integrative therapists. I think we're at a place where we want them employed. Because otherwise it can set up a we-they dynamic.... [the integrative therapists] may not have a great opinion of the medical center, and that shows up in different ways, not ways that are really fractious but ways that are important.... how do you bring in people who have been doing work that's low cost and effective into a system that really doesn't value that.” -Clinician, 124
This clinician noted the importance of all team members feeling valued and fairly compensated for their contributions to the group, which can be challenging in a system that has previously only valued traditional healthcare.
Adequate Training
Lastly, participants felt that hiring clinicians who were interested in facilitating groups, as well as adequate training to learn about group facilitation was important for the sustainability of group visits. “It’s a concerted effort now. We've got a couple newer hires of nurse practitioners...and... a new director who's a physician. And the goal is to get all of them doing some type of group visit. We're training one of our newer nurse practitioners; she’s doing the mindful self-compassion training.... the other one has done is sort of an integrative nutrition and Health Coaching....and then our physician is also a Yoga Therapist, so he'll probably do some sort of movement-based group visit.” -Clinician, 121
Training staff in integrative medicine practices and providing ongoing training was an important component of staff experience. “So, that's why we... want people to have their own personal experience and then go through the training...and then start to teach and lead groups and with mentorship, and then once people have led two groups...we encourage them to do these additional workshops on specific topics where people often get caught up” -Clinician, 122
This clinician above suggested that leading groups was an ongoing learning process, and the provision of educational resources, mentorship, and training opportunities were important for continued confidence building and success.
The interviews with staff, administrators, and clinicians suggest that organizational supports around the integrative group medical visit, including staffing, upper management support, and training opportunities, can greatly affect the clinician’s experience. Clinicians identified that these organizational level supports must be in place to allow for the energy and time required to facilitate a group. Participants discussed how having adequate administrative staffing to assist with recruitment, reminder phone calls, and orientation was essential for successful implementation and sustainment of their IGMV programs. The support of upper management during adoption and maintenance of the program resulted in less burden on clinicians and helped programs be more successful. Lastly, clinicians greatly benefitted from the opportunity to participate in continuing education, so they felt prepared to facilitate the group and teach mindfulness and mind-body practices.
Human-Centered Engagement
The group medical visit model allows clinicians to spend more time with patients, and patients to share experiences and knowledge with each other. One clinician reported gaining energy from seeing patients support each other and saw patients benefit as well. “…it just gives me a lot of joy and fuel to see them helping each other. It’s really cool... it excites me [when patients are] active in their own health and then maybe potentially interested in more of an advocacy or research role too.” - Clinician, 120
Participants suggested this group structure allowed patients to find common ground and bond through shared experiences. Participants also explained that patients tended to reveal their strengths, personalities, and lived experiences, facilitating connections between staff and patients, as a co-facilitator of a group described below. “I think that's been really helpful to see clinicians connect to patients…and understand their personalities at such a deep level and I think…[clinicians] have really valued that…admiring how persistent a patient is or …how honest a patient is…valuing the stories...[and] experiences that the patient brings to the group.” -Co-facilitator, 127
Not only did clinicians value hearing patient experiences and getting to know their personalities, they also reported that the group visit model allowed for quality human-to-human interactions. “I think it’s extremely rewarding; I think you get to know your patients in a much deeper way. When they’re talking to each other, they just reveal so much more about themselves…what I love about it is you see their strengths, right? Like when you see one patient giving advice to another patient.” -Clinician, 110
One clinician reported that the group structure “just changes the equation, it’s a much more spacious and human-centered way to engage” -Clinician, 108. These deeper and more personal interactions seemed to create a healing and supportive environment for both patients and clinicians. One program director reported that IGMV reduced perceived “walls” between clinician and patients. “I think it’s a healing thing for people and it’s one of the most wonderful things about group visits… you’re breaking down a little bit of the wall between the clinician and…patient and we're all just people walking a common path together.” -Director/clinician, 122
The overall stronger rapport between both parties gave patients the opportunity to support their peers and seemed to increase engagement in their own health journey. Lastly, clinicians found that the integrative medicine portions of the group were mutually beneficial. “...when you’re leading a group, you're meditating at the end. So, you're going to leave with that relaxed wonderful feeling too as a clinician, it’s like the ricochet.”- Group coordinator, 106
Overall, clinicians and patients seemed to experience quality human interactions that facilitated moments of joy and relaxation, strengthened relationships, and felt supportive and healing.
Working with an Interdisciplinary Team
Several participants noted the presence of an interdisciplinary team approach. An interdisciplinary team is a process in which various types of staff members work together and share knowledge, expertise, and skills to contribute to patient care.
27
The makeup of the interdisciplinary teams varied among the clinics interviewed. Most clinics included a medical clinician (physician’s assistant or medical doctor), a co-facilitator, and administrative personnel. Some clinics also employed additional practitioners such as nutritionists, acupuncturists, and yoga teachers. Four clinicians from four different organizations mentioned the positive effects they experienced while working in an interdisciplinary team, including opportunities to brainstorm and collaborate, as mentioned by this group coordinator. “I just remember every single time IGMV was brought up and I interacted with a clinician or facilitator, it was always [about] how we can help the patients more. Like, ‘What can we do this week? How are the patients doing? What improvements are we seeing? How should we like make this more beneficial or make this better?’” -Group coordinator, 125
Similarly, another staff member expressed that having multiple clinicians while facilitating the group “was much more manageable. I wasn’t the only clinician and/or moderator, so there was somebody to always bounce off of” -Clinician, 105. Clinicians collaborated outside of the group visits and used each other to facilitate more interaction and discussion during the groups. Patients noticed this positive working relationship among clinicians, which set a good example for the group dynamics. “We work great together. We really enjoy working with each other. We built relationships with each other which then translates out when you're working with our patients as well.” -Clinician, 102
Lastly, clinicians reported feeling less emotional burden when they could share the experience with another clinician. The interdisciplinary interactions among clinicians brought levity and opportunities for creativity when discussing the care of a complex patient population. “[The] team piece is just huge. I can't even imagine being one or two people working with the challenges that folks who come in have had in terms of their suffering. So...I’m grateful for that all the time...That's the thing of how do you keep this group of people who are working with suffering every day sharp? How do you keep your primary therapeutic agents flourishing? I do think the buoyancy of that team is huge...we're all in this together working together, there is a lot of humor, that's not dark humor, during those case reviews [and] staff meetings it has a light feel to it. And I think people really are [interested in] what other people are doing...there's a lot of respect between the different disciplines. But I think the team approach is huge. I think we all have the feeling that when things are difficult, we have a group of minds thinking about something” -Clinician, 124
Notably, the clinical setting where this participant worked is unique because they facilitate IGMVs and hold interdisciplinary case reviews, which is not standard for primary care practices. Nonetheless, the interdisciplinary approach inherent to IGMVs enabled clinicians to collaborate and offer each other emotional support. Participants reported that clinicians involved in IGMVs for patients with chronic pain felt supported by one another and benefitted from the collaboration, emotional support, and energy that was associated with an interdisciplinary team.
Providing Guideline-Concordant Chronic Pain Care
Several clinicians also stated that the groups offer an excellent and essential option for referral for patients with chronic pain. Because the groups last much longer than a typical one-on-one visit, clinicians felt that they are able to deliver care that is recommended for people with chronic pain, which they considered equal to or better than one-on-one visits. “the group kind of takes that element of urgency away from those things because you're providing...quality care versus, I need to hit all these measures in 20 minutes. I need to cover all of this in 20 minutes.” -Group coordinator, 112
The additional time required by the group format gave patients more time to receive education on healthy food options, pain management strategies, stress management strategies, sleep hygiene, and other important lifestyle adjustments. Patients also had more time to ask questions, which improved self-efficacy in their health management and strengthened their relationships with peers and clinicians. “It was really humbling. When you see a person who’s done a couple of groups...[and] a year-and-a half later, [they stated] ‘I was talking to my psychiatrist and I'm off of five medications.’ You see somebody who has on their own [stopped], asked their clinician to wean them off their opioids and return to work. You see story after story... it’s that empowered hope. It’s a self-efficacious hope. It’s a sense of yes, there’s tremendous struggle and I am totally awesome... I’m resourceful and capable and I've got this tool”. -Clinician, 108
The clinician above reported that over time, IGMV participation helped a patient develop increased autonomy over their own health and gain newfound hope for their future quality of life. One participant mentioned that often in the FQHC setting, clinicians felt they lacked sufficient resources for patients with chronic pain. Clinicians valued having a group they felt confident would benefit the patient’s health. “Primary care clinicians are burnt out on pain specifically. They don’t have all the tools that they want. The resources that they can connect their patients with are incredibly limited, particularly within FQHCs. And so, the fact that there’s a program like this where they’re like, okay, I can just refer a patient, and then they'll take care of them...it’s been well received...we’re talking to leadership about how this can help to address clinician burnout, we’re talking to them about how exciting it is to be offering these types of programs from an equity perspective.” -Evaluator, 109
Clinicians found the extended time spent with peers, group facilitators, and a clinician in the integrative group medical visit setting effective. Clinicians appreciated having a group as a referral option for patients, knowing that guideline-concordant chronic pain care would likely be provided.
Enhances Meaning and Purpose for Clinicians
Overall, clinicians felt more meaning and purpose facilitating the groups compared to the one-on-one visits. Eight different clinicians and staff reported that interactions between patients and clinicians during IGMV were fulfilling. “And I think that that has been one of the most satisfying parts for me…being in group is always great, because people share and you see how they get better, but I think that life cycle of somebody’s process from being in a state where they don’t feel like anything can help their pain to the point where they are resistant to group, they don’t want to try… now they’re the ones that are coming back in every group, every cohort. That I think for me… that brings me joy, because I get to see that process and see how beneficial groups have been.” – Group coordinator, 103
Clinicians noted that seeing their patients improve enhanced their wellbeing and brought joy back into their role as a medical clinician. Additionally, the dynamics between the patients during IGMV provided a refreshing perspective and energy to the clinicians’ day. “…that’s what’s keeping me going, that's what I’m looking forward to on that Wednesday night is that I get to be in this group… and these patients…have this atmosphere around them and this energy with them, and it kind of just revitalizes and refreshes the perspective of health care for the clinician…” -Group coordinator, 112
Clinicians benefited not only from the energy created by most groups but also found purpose and inspiration in the groups, ultimately reducing feelings of burnout. “I do think running the groups gives me meaning [and] purpose. It’s empowering for me to empower the patients. I think about this as their group and I’m just facilitating their group, and I do think it helps reduce my burnout. I think I'm happier running the group.” -Clinician, 104
The inherent interactions in a group that recognized a common humanity created a positive experience for everyone involved. Clinicians reported that improved rapport and understanding of their patients motivated, energized, and reduced their symptoms of burnout. Relationships between themes identified in qualitative interviews, healthcare team well-being, and burnout.
Discussion
Burnout can be caused by many factors including clerical burdens, increasing productivity demands, shorter visit times with patients, caseloads with sicker and more complex patients, lack of input or control with respect to workplace issues, loss of control and autonomy, loss of meaning at work, and long work hours.2,28 Organizational changes that are suggested to address burnout are reflective of the drivers of burnout and include increasing organizational and administrative support, protecting clinician time with patients, promoting clinician connectedness and teamwork, improving access to resources, and increasing meaning in the workplace. 28 Based on our qualitative findings, we suggest that IGMV may contribute to reducing burnout (Figure 1). The themes identified and discussed here align with suggested solutions to mitigate burnout identified in previous studies. For example, IGMV is a needed resource that provides guideline-concordant care to treat patients with the complex condition of chronic pain, clinicians have more face time with patients over the course of the group, and clinicians work together to run the group, facilitating clinician connectedness. Five participants specifically mentioned that participation in IGMV reduced burnout among clinicians in their clinic. Additionally, the theme of human-centered engagement is congruent with previous studies, which found that a group medical visit (GMV) format promotes patient-centered care and positive relationships between patients and clinicians. This qualitative study noted that relationships between clinicians and patients in a GMV promoted mutual respect, enabled patient autonomy, and highlighted a common humanity. 11 Continued support and care over the duration of the GMV also improved patient’s health behaviors. 11 Relationship-based care, which focuses on the relationship between patient and clinician, but also considers the relationships between clinicians and the community, with their care team, and with themselves, 29 has been suggested as a framework to transform primary care practice. 30 Taken altogether, clinician participation in IGMV seemed to improve clinician experience, increase job satisfaction and may address some causes of burnout.
This qualitative study used interviews from healthcare teams who were involved in IGMV specifically, not group medical visits in general. Conclusions cannot be drawn about whether the benefits clinicians experienced were due to the group medical visit model or the integrative components of IGMV specifically. Prior research supports that the group medical visit model improves clinician experiences. For example, the group medical visit (GMV) model shifts clinicians into a facilitator role and encourages the incorporation of patients’ lived experiences, both of which may contribute to the delivery of patient-centered care and increase satisfaction for both patients and clinicians. 11 Clinicians who perceive that they have the resources to address patients’ social needs are less likely to experience burnout. 31 GMVs have been found to improve outcomes for other groups including diabetes, arthritis, and prenatal care.32,33 In our study, one participant specifically reported benefiting from the meditation practice that they facilitated during the group. Several studies have found that mindfulness, yoga, and breathwork practices improve clinician experience and help clinicians avoid burnout.34,35 These previous studies had clinicians participating, not facilitating these practices, so we cannot assume that their experiences as clinicians facilitating mind-body practices for a group are equivalent. Further research is needed to identify specific impacts to clinicians that are unique to IGMVs.
Implementation of IGMVs for chronic pain can be viewed as a modification to the healthcare system at a team level and an organizational level. With environmental supports in place, clinicians reported that their experiences overall improved through participation in IGMV. IGMV should be considered a viable alteration to the organization of clinics to address the fourth aim of the Quintuple Aim – improving the experience of clinicians. Given the prevalence of burnout in primary care settings particularly in the wake of the COVID-19 pandemic, and the implications to patient care and safety, prevention of burnout should be a priority. As seen in these interviews, the overall positive experience of clinicians involved in IGMV suggests that this model should be further investigated as an option to address the fourth aim – clinician experience.
The findings presented here are limited by the self-selection of clinicians who facilitate groups. The majority of the clinicians who were interviewed had voluntarily started an IGMV program or willingly participated in the facilitation of a group. The systems they work in may have had enough time and resources to start IGMV and may have more management and financial support than other health systems. While we were able to reach FQHCs and safety net hospitals across the U.S., the small sample size reflects that implementation of IGMVs remains limited, and future research would benefit from including the perspectives of other clinics. Similarly, these data may not extend to other healthcare settings beyond FQHCs and safety-net hospitals.
Future studies should investigate the experiences of healthcare teams using validated measures of well-being and symptoms of burnout. Additionally, rigorous qualitative, quantitative, and mixed methods research should be done to further investigate how the IGMV model addresses all elements of the Quintuple Aim.
Footnotes
Author Contributions
I.R., P.G., and J.L. made substantial contributions to the design of the study. I.R. conducted the interviews and acquired the data. M.J. performed analyses of the data and M.J. and I.R. interpreted the data. M.J. and I.R. drafted the article. All authors contributed to revising it critically, gave final approval for the version to be published, and agreed to be accountable for all aspects of the work, ensuring accuracy and integrity of the work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The project described and contributions by I.R. were supported by the National Center for Complementary and Integrative health, National Institutes of Health (NIH), through Grant Award Number K01AT011578. Contributions of M.J. were supported by the National Center for Complementary and Integrative Health, through Grant Award Number 5T32AT3378-17. The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH.