
Abstract
Introduction
Chronic pain is a complex and pervasive issue that disproportionately affects marginalized and underserved populations, driven in part by healthcare access barriers. Chronic pain affects multiple domains of life, warranting the need for accessible, holistic, whole-person, evidence-based care. The Heals on Wheels (HoW) program’s multidisciplinary team developed and implemented community-based integrative pain care workshops for underserved communities throughout Hennepin County, Minnesota.
Methods
The 4-week curriculum included 60-120 minute-long weekly workshops hosted by community organizations. A pre- and post-workshop weekly progress sheet questionnaire explored perceptions of pain, overall state, favorite moments, and future suggestions. Responses were analyzed thematically.
Results
Throughout 2022-2025, 13 workshop series occurred with 9 different community organizations. Total attendance was 369 (average 7.10/session) with 265 weekly progress sheets completed by 163 unique individuals (71.82%). Average pre-visit pain was 5.40; post-visit was 3.26 (
Conclusion
The HoW workshops are feasible as an innovative and accessible community-based integrative pain care model.
Keywords
Introduction
As of 2023, chronic pain affects a substantial portion of U.S. adults, with 24.3% reporting chronic pain and 8.5% reporting high-impact chronic pain. 1 People experience chronic pain from a wide range of diagnoses, as well as from numerous contributing factors which associate closely with social determinants of health. The burden of chronic pain is often greater in marginalized, underserved, and lower socioeconomic communities due to the co-occurrence of trauma, chronic stress of limited resources, and limited access to health-promoting environments.2-4 People in underserved communities often lack access to consistent medical care, reliable transportation, have limited insurance coverage, and potentially face a mistrust of the medical system rooted in historical trauma.5,6 People living with chronic pain often have a lower quality of life, mental health comorbidities, and higher healthcare utilization costs and treatment burden. 7 Overdose deaths and recognition of opioid use disorder (OUD) have led to a growing interest in strategies and programs to support nonpharmacological pain management. Evidence-based practice guidelines for the care of chronic pain increasingly focus on non-pharmacological approaches, including mind-body practices, pain science education, sleep, Traditional, Complementary, and Integrative Medicine (TCIM) modalities, gentle movement practices, and mindfulness.8,9 Additional evidence supports a whole-person approach to pain care, a hallmark of integrative medicine, which includes physical, mental/emotional, social, spiritual, and environmental domains.10,11 This approach emphasizes practitioner/patient relationships and is inclusive of all evidence-based therapeutic and lifestyle approaches to health and well-being, including relaxation practices, sleep, nutrition, and community support, all of which can positively impact the experience of chronic pain. 12
Evidence supporting the safety and efficacy of nonpharmacological pain management modalities is strong and continues to grow. For instance, a randomized trial of 12 weekly virtual yoga sessions among 140 adults with chronic low back pain demonstrated significantly greater reductions in pain intensity and disability, as well as decreased analgesic use and improved sleep, vs wait-list controls. 13 A 2024 systematic review of mindfulness-based therapies and guided imagery for various chronic pain types found numerous studies reporting significant reductions in pain intensity and opioid consumption, and improvements in psychosocial facets of pain, supporting the evidence of benefits of both practices for chronic pain management. 14 Additionally, an updated review of nonpharmacological treatments for chronic pain from the Agency for Healthcare Research and Quality (AHRQ) found that exercise, yoga, various psychological therapies, acupuncture, and spinal manipulation were associated with small to moderate effects on function and pain, with some modalities demonstrating beneficial effects for up to 12 months following treatment. 15
Integrative Group Medical Visits (IGMVs) are an effective model for delivering and expanding access to evidence-based non-pharmacological modalities for chronic pain treatment and supporting self-management skills among a range of populations, including underserved communities. A 2025 feasibility study assessing group acupuncture and/or IGMVs compared to usual care among participants with chronic pain from a safety-net primary care clinic demonstrated acceptability of the program, and 86% of participants self-reported clinically relevant pain improvements compared to 20% in usual care. 16 Participants also expressed social benefits of group experiences and barriers to accessing multimodal care. 16
Community-based group interventions for chronic health conditions are also strongly supported by several decades of literature describing effective and acceptable programs such as Stanford’s Chronic Disease Self-Management Program initiative. 17 Examples of literature on community-based group programs addressing chronic pain include key ingredients similar to IGMVs, such as education, participation, group member connection, and pain self-management skills.18,19 Whether in clinical or community settings, there appears to be an important element of being with others in a group, sharing a common condition or experience. Geller et al have described this as the “group inclusion effect”, based on longstanding associations recognized between social connections and health outcomes.20,21
Though IGMVs and non-pharmacological approaches to pain care have strong evidence for their safety and efficacy, they are still not the primary interventions used in the care of chronic pain throughout US healthcare systems. Reasons for this include patient, provider, and system-level barriers, including payment models of healthcare organizations and a lack of reimbursement for educational interventions and some evidence-based nonpharmacological pain care modalities.22-24 Additionally, the ongoing reliance on and expectations of pharmaceutical and/or interventional treatments for chronic pain, which are rooted in the allopathic/medical model, may also limit awareness of alternative effective, evidence-based options for pain care.22,23 Access to novel, integrative, or holistic healthcare modalities can be challenging, especially among people facing structural and social determinants of health barriers. Community organizations are well-positioned to address some of these barriers, yet are often not equipped with the staff or expertise to deliver health-related programming. To address this need, our study examines the development and implementation process of community-based workshops for integrative, whole-person pain care in marginalized and underserved communities.
Hennepin Healthcare Systems (HHS) is a safety-net hospital system that includes a level 1 trauma center, acute care hospital, and clinic system with locations in Minneapolis and surrounding Hennepin County. HHS is home to a dedicated Integrative Health (IH) team, including physicians, physical therapists, acupuncturists, nurses, chiropractors, psychologists, and more. HHS’s Heals on Wheels (HoW) initiative consists of multiple programs with an overarching mission of bringing integrative, whole-person care directly to communities in need. The focus of this report is a 4-week “Light Lunch” community workshop series to teach participants key evidence-based integrative pain care skills.
Methods
Each Light Lunch workshop lasted 1-2 hours and was hosted in partnership with non-profit community organizations. Inclusion criteria for partnership included organizations with a focus on underserved populations who could be at higher risk of negative sequelae for chronic pain. Organizations outside of Hennepin County were excluded. To align with the HoW mission of inclusivity, no restrictions were placed on community participation in the workshops. The workshops were open to anyone interested in learning more about holistic pain care, including community members and community organization staff. Community partners were chosen based on successful partnerships with previous HoW programs and by networking through other HHS providers and non-profit leaders. These community partners were responsible for securing the physical space for the workshops and promoting them to their community. The HoW program evaluation initiative was reviewed by Hennepin Healthcare’s Institutional Review Board (IRB) and determined that it does not constitute human subjects research and, therefore, is not subject to IRB oversight.
The need for the Light Lunch workshops emerged from the original HoW program, which included brief 1-2 hour stand-alone “Appetizer” community workshops and an 8-week “Full Meal” IGMV. 25 Low rates of IGMV enrollment from Appetizer participants into the Full Meal IGMV suggested to our team a need for a longer, community-based workshop series to bridge the programming gap between the brief Appetizers and the more intensive Full Meal IGMV. The HoW Light Lunch curriculum was developed by an interdisciplinary team including board-certified integrative medicine physicians and an integrative physical therapist/yoga therapist, with additional input from acupuncturists, massage therapists, and a mindfulness meditation instructor. The curriculum was adapted from the Appetizer and Full Meal workshops, with topics and the agenda chosen based on past community interest and provider experience. Workshops were co-facilitated by an integrative physician and physical therapist/yoga therapist with acupuncturists, a mindfulness instructor, and massage therapists present for specific sessions. Additionally, a program coordinator assisted with the administrative scheduling and coordination, as well as providing physical assistance with set up and other workshop logistics. The duration of the workshops varied depending on the needs of specific communities. The 1.5-2-hour-long workshops were offered to sites requiring interpreters, to partners serving communities with physical limitations that might slow their movements, or other issues that would necessitate the need for a longer session.
Total attendance numbers at each session were tracked by the program coordinator. Program impact was monitored through participant feedback using a weekly progress sheet, adapted from previous programming.
25
Time was allotted at the beginning and end of each session for the participants to complete questions related to their physical and emotional state, symptoms, pain rating, favorite part of the group experience, and future suggestions (Figure 1). While participants were all offered the opportunity to fill out the sheet, it was not a requirement for participation in the workshop. Unique participant attendance data was gathered based on these completed weekly progress sheets. And therefore, the total number of unique participants and attendance of participants across sessions was not tracked. Instead, the total number of participants at each session was collected and aggregated across the program. Due to the brevity of the workshops, demographic information was not collected from program participants. However, the populations served by each of the community partners included a majority of people experiencing economic disadvantage and/or other social determinants of health. To explore the experiences of participants, weekly progress sheets were scanned, deidentified by the program coordinator and research assistant through replacing participants’ names with their first and last initial, and transcribed into Microsoft Excel. Responses to prompts were transcribed verbatim, and notation was taken when handwriting was illegible. Responses included single-word answers and, at times, one to two-sentence answers. As such, codes were often verbatim word selection or single-word meaning. Responses were then reviewed by week to identify (or clump) commonly expressed codes into themes. Once inter-weekly themes were identified, thematic review across weeks was employed. While specific count analysis of codes/themes was not employed, themes that most frequently emerged were noted as dominant themes. All themes were coded within their given prompt on the weekly sheet. The prompts chosen for this manuscript were in support of experiences that participants shared that may inform future work. Heals on Wheels light lunch community workshop weekly progress sheet
Results
Heals on Wheels Light Lunch Community Workshop Sessions Attended by 163 Unique Participants
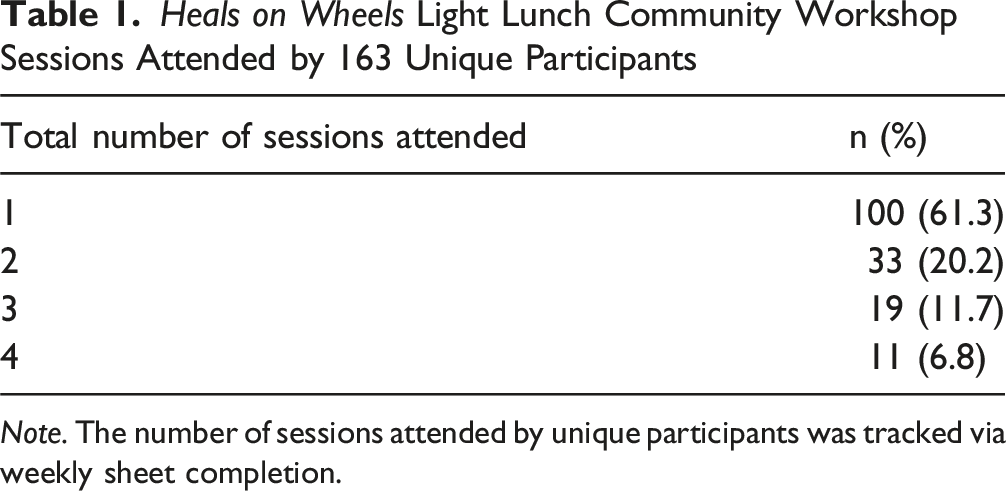
Note. The number of sessions attended by unique participants was tracked via weekly sheet completion.
Curriculum Overview
The curriculum for the workshops included sessions dedicated to the science of pain and the stress/relaxation responses, sleep, integrative pain care modalities (yoga or qi gong, acupuncture/acupressure, and massage), and nutrition. While workshops always began with the science of pain and stress/relaxation responses sessions, the ordering of the next 3 sessions varied based on provider availability. Generally, an acupuncturist led a portion of the experiential activity for the modalities session; however, if they were unavailable, a physician trained in battlefield acupuncture led the acupressure activity. Similarly, if the PT/yoga therapist was not available for the modalities session, a mindfulness instructor led qi gong movements in their stead.
Heals on Wheels Light Lunch Community Workshop Detailed Curriculum

Weekly Progress Sheets
Heals on Wheels, Light Lunch Community Workshop Themes – Pre/Post

Note. Some participants expressed numerous statements. Some did not express anything (skipped question).
Heals on Wheels, Light Lunch Community Workshop Suggested Themes

Note. Some participants expressed numerous statements. Some did not express anything (skipped question).
Discussion
The HoW Light Lunch program consisted of 13 workshop series, hosted by 9 distinct community partners. The program utilized a 4-week whole-person, multidisciplinary, integrative curriculum for people who experience chronic pain, with sessions exploring the science of pain and the stress/relaxation response, sleep, TCIM modalities, and nutrition. Workshops were consistently attended, weekly progress sheets were utilized at high rates, and demonstrated decreased pain scores alongside positive qualitative feedback. These metrics highlight the feasibility of this community-based pain care model, as well as its acceptability to a range of community participants.
Analysis of weekly progress sheets revealed sharing as an important component of groups, which is consistent with findings from the HoW full meal 8-week IGMV series. 25 Both programs also found that participants reported various skills as the portion they liked the most about the groups. However, written responses on weekly progress sheets were much shorter and less in-depth in the Light Lunch program compared to the HoW 8-week IGMV series. The less detailed responses may be related to several factors, including brevity of workshops, inconsistent attendance, non-clinical setting, and less total time for building therapeutic rapport with workshop facilitators.
Throughout the course of the HoW Light Lunch program, several important lessons were learned that iteratively improved the quality and reach of the program. While originally, we conceived of the curriculum as cumulative and similar to an IGMV in which the same participants typically attend each session, we soon realized that consistent attendance was not feasible for the populations we were serving. Therefore, we adapted the curriculum so that each session could be a standalone workshop. In tandem with this, we had originally intended to have participants fill out the PROMIS-29 questionnaire 26 at the start of the first session and at the completion of the final session. However, we also realized that this outcome was not feasible due to the inconsistent attendance of participants and the burden of filling out a lengthy questionnaire after such a brief intervention. Other community-based programs aimed at improving health outcomes, specifically a Food is Medicine course delivered at community pantry sites, have also expressed difficulty in sustained engagement with participants only attending 1-2 classes out of a 6-week series. 27
Attendance at the workshops steadily improved throughout the 3 years of the program. While some of the workshops in the first year had low attendance, as the program evolved, we discovered the importance of regular communication with and support from community partner organizations. Creating customized fliers, requesting attendance estimates before the first session, and sign-up sheets all helped to improve attendance for the second and third years of the program.
Limitations and Future Directions
While HoW illustrates a novel, feasible program model to reach communities at higher risk for chronic pain, certain limitations exist within our exploratory methodology. While our weekly progress sheets were adapted from previous work, they have not been formally validated. The weekly sheets were filled out in full view of and returned to the facilitators, which could have biased the answers. A single researcher completed the qualitative analysis, which could bias our results. We did not capture any demographic information from the participants, which limits a full description of our program’s reach. One site had primarily non-English speaking participants, and while we used an interpreter during the session, we did not have a translated version of the weekly sheet for this group, and subsequently, their feedback was not included in our formal analysis. To be consistent with our iterative model, and value that group’s feedback, we asked the community partner organization to solicit feedback for our team on the participants’ experience. The community organization reached out via phone and email and collected open, unstructured feedback on their experience in the workshop. This feedback was summarized as a list of anonymous quotes and shared with our team via email. Additionally, curriculum differences from one workshop to another (i.e. yoga vs qi gong) were not controlled for in our study. Future studies could address some of these limitations through the use of validated tools with expanded language options. To support the specific needs of each site, the duration of the workshops varied between 60, 90, and 120 minutes. While we believe that this flexible structure best served the diverse needs of the participant groups, the differences in workshop duration may have influenced results. Also, attendance data was taken anonymously, and thus, if a participant did not fill out a weekly sheet but attended more than one session, their unique attendance is not recorded. Some of the sites with lower attendance and weekly sheet completion rates served populations struggling with substance use disorder and other complex medical conditions, and/or served more itinerant populations. Future programs might consider broader recruitment efforts and briefer, more accessible outcome measures with these populations.
Based on these limitations and lessons learned, the HoW Light Lunch program is evolving to focus on broader chronic healthcare issues beyond pain (cardiometabolic diseases, neurodegenerative diseases, and cancer). To better address the specific needs of populations, we will be offering community partners a menu of session topics from which to choose, rather than limiting the topics to our prescribed program. Noting that several sites from the program had highly engaged community members and/or community partner employees who expressed interest in learning more about the topics, in 2026, we are launching a HoW Community Ambassador program where these individuals can be trained as facilitators of the Light Lunch program, broadening the reach of the program.
Conclusion
Through 54 HoW Light Lunch community-based workshop sessions on integrative pain care, decreased pain and various positive themes such as hope, relaxation, and gratitude were revealed. The utility and innovation of hosting these workshops outside of conventional healthcare spaces were likely factors in the consistent attendance rates, positive feedback, and overall community engagement. Community-based programs such as HoW have the potential to foster partnerships between healthcare and community organizations and reach community members who may not have conventional or integrative healthcare access. The complex and highly individualized nature of chronic pain requires unique and creative programming models, especially with populations facing social determinants of health barriers. The HoW Light Lunch workshops serve as an acceptable and feasible model, serving the complex needs of people in pain through integrative, whole-person care. Accessibility in community spaces to this evidence-based care is essential for populations who might otherwise be neglected from conventional healthcare models.
Supplemental Material
Supplemental Material - Heals on Wheels: Development and Implementation of Community-Based Workshops for Integrative, Whole Person Pain Care in Underserved Communities
Supplemental Material for Heals on Wheels: Development and Implementation of Community-Based Workshops for Integrative, Whole Person Pain Care in Underserved Communities by Catherine Justice, Jadyn E. Knox, Stefanie Stevenson, Kate Shafto, Tegan Reeves, Jacinta Rebang, Susan Haddow, Arti Prasad in Global Advances in Integrative Medicine and Health.
Footnotes
Acknowledgments
We would like to thank Eiko Mizushima, Charlotte Alverez, Jessica Brown, Angie Craig, Sarah Ulmer, Marisa Newell, and all our community partners and workshop participants.
Ethical Considerations
The HoW program evaluation initiative was reviewed by Hennepin Healthcare’s Institutional Review Board (IRB) and determined that it does not constitute human subjects research and, therefore, is not subject to IRB oversight.
Consent to Participate
The Ethics Committee of Hennepin Healthcare Systems waived the need for patient consent for the collection, analysis, and publication of the retrospectively obtained and anonymized data for this non-interventional study.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported, in part, by a grant through the University of St. Thomas and the George Family Foundation Innovation Fund and a grant through Hennepin Healthcare Foundation MVNA Community Fund.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The dataset for this study includes sensitive and confidential information such as patient data; therefore, the dataset cannot be shared.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.