
Abstract
Background
Chronic pain is highly prevalent in US military Veterans, and pain interdisciplinary teams (IDTs) are the gold standard in pain care. There is no standard or guidance for how best to develop and implement pain interdisciplinary teams within complex health care systems.
Objectives
The purpose of this quality improvement project was to evaluate the effectiveness of the standard 9-step Lean 6 Sigma (LSS) methodology in redesigning a pre-existing VA outpatient pain clinic solely offering interventional pain services into an efficient, sustainable pain IDT program.
Methods
The initial evaluation process at a VA Medical Center that primarily serves rural Veterans was redesigned with the a priori goal of developing an efficient, sustainable IDT program that decreased driving days (ie, in-person appointments) required for a comprehensive initial pain evaluation, decreased number of consults required for initial pain evaluations, increased the number of consults to Whole Health services, and increased compliance with policies and standards. Feedback from administrators, clinicians, and Veterans was used to identify inefficiencies then iteratively design, test, and finalize a redesigned service called the PREVAIL Interdisciplinary Team Track (PREVAIL IDT Track). Baseline data was collected for 1 year followed by sustainment data for 14 months. Results were analyzed using descriptive statistics.
Results
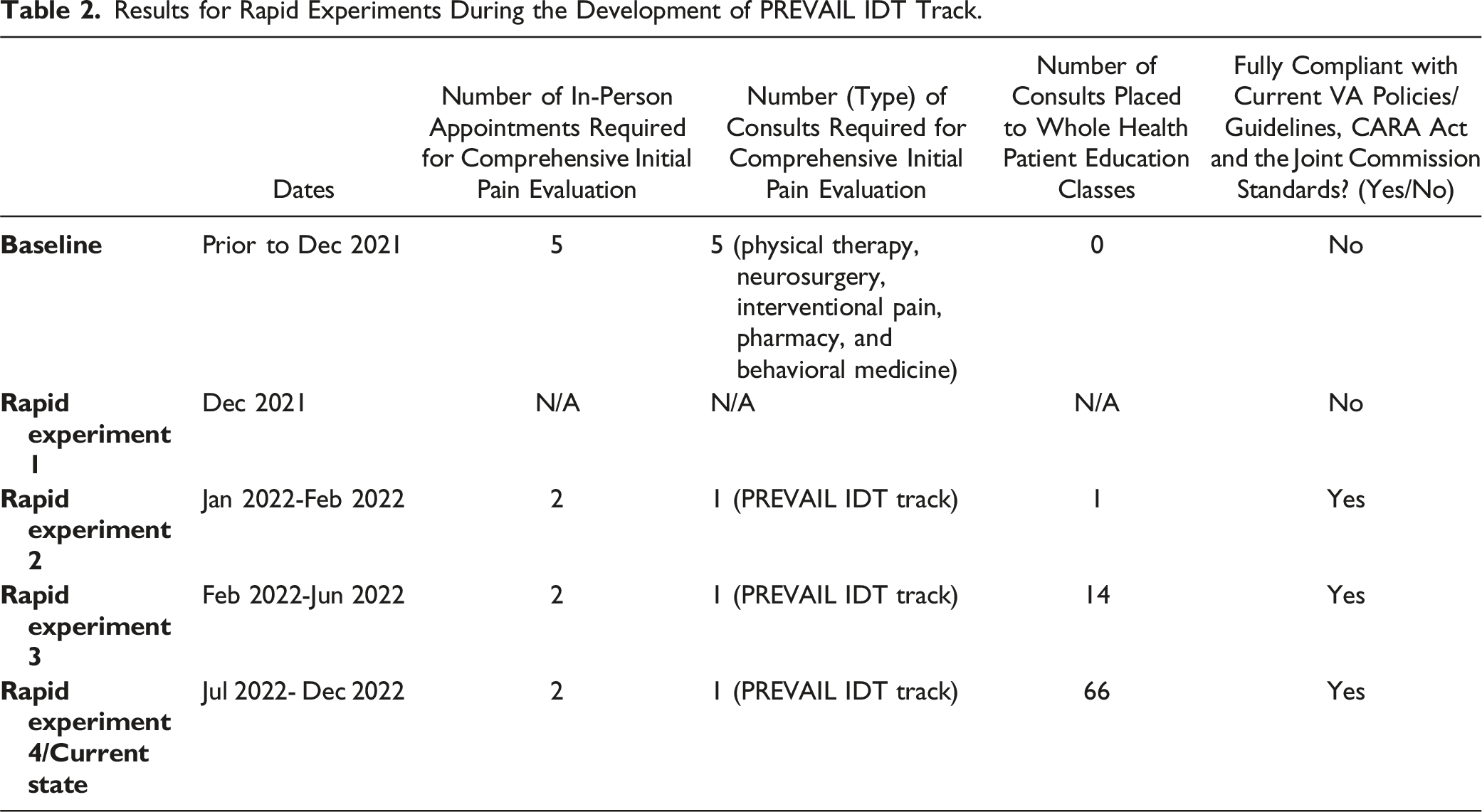
PREVAIL IDT Track decreased the number of in-person appointments from 5 to 2, decreased consults required for evaluations from 5 to 1, increased the number of unique consults to Whole Health education classes, and made the VA fully compliant with policies and standards. To date, 486 Veterans have participated in the redesigned program, including 167 graduates and 212 current enrollees in this sustained clinical program.
Conclusion
The success of PREVAIL IDT Track suggests that LSS may be a promising method for redesigning sustainable pain IDTs in VA that improve efficiency.
Introduction
Military Veterans experience pain at a disproportionately higher rate than civilians, with 65% reporting pain in the past 3 months.1,2 Veterans also experience more complex pain and significant comorbidities, including mental health conditions, traumatic brain injuries, and chronic health conditions. 1 It is widely accepted that pain interdisciplinary teams (IDTs) are the gold standard approach for addressing the far-reaching impacts of chronic pain,4–6 with some exemplary programs that have shown promise.7–10 Furthermore, the number of IDT programs has declined significantly due to key barriers that prevent sustainability. 11 While dissemination and implementation models have demonstrated efficacy for developing sustainable approaches in complex health care systems,12,13 there is scant literature on effective methods for developing and/or adapting existing IDT programs into sustainable IDT pain programs. Indeed, no guidance exists for how to design nor implement interdisciplinary teams across complex Veterans Health care Administration (VHA) environments, with each VA medical center comprising varying levels of resources, policies and procedures, and diverse patients’ needs. While it is not clear what processes have been used to develop current IDT programs within VHA, it is widely accepted that understanding how to best implement interventions into heterogenous and dynamic settings is key for sustainability. 14 Thus, there is a critical need to identify effective methodologies that can be used to design sustainable pain IDT programs that are efficient and therefore accessible for those most at risk for the far-reaching impacts of chronic pain.
The Lean 6 Sigma (LSS) methodology 16 for system redesign has been applied in VHA to improve efficiency of care within complex environments involving multidisciplinary teams, such as emergency rooms.16–18 LSS’ focus on efficiency and quality render it a particularly useful model for systems redesign since the VHA has adopted “connecting Veterans to the soonest and best care” as an agency-wide priority. 19 However, a knowledge gap exists for whether the LSS methodology can be used to redesign pain IDT programs that are efficient and sustainable. To use the concept described by Curran, 20 “the thing” is the intervention intended to be integrated in a practice setting and the implementation strategies such as conduct cyclical small tests of change 21 are “the stuff” that helps systems do “the thing.” In this case, pain IDTs have been established but “the stuff” that helps “the thing” integrate in practice settings has not been established. VHA implementation strategies are necessary 21 to speed the integration of best fit interventions into practice settings. The purpose of this article is to describe how LSS methodology (“the stuff”) was operationalized as the cyclical small tests of change and applied to a pre-existing outpatient pain clinic (“the thing”) to determine the extent to which the application of LSS (“the stuff”) led to improvements in target areas (“how well the stuff helps the staff do the thing”).
Methods
Context
This application of the LSS methodology began in October 2021 in the PREVAIL Center for Chronic Pain (PREVAIL is an artistic choice, not an acronym), an outpatient pain clinic at the main medical center within the Salem VA Health Care System (Salem VA). The Salem VA is a level 1C facility located in Salem, Virginia as a part of Veterans Integrated Services Network 6 (VISN 6), and primarily serves rural, Central Appalachian Veterans. At the beginning of this project, there were 2.25 pain MDs, 1 clinical pharmacy specialist, 1 nurse practitioner, 1 psychologist and 1 physician assistant on staff within the pain department. Additional key stakeholders for this project included the Chief of Staff as well as chiefs, section chiefs, and providers from medicine, primary care, pain management, physical medicine, primary care, and rehabilitation, and psychology. Data collection spanned from October 2021 through March 2024.
Methodology
This quality improvement project used LSS methodology (ie, A3 Deep Dive) to iteratively redesign the interdisciplinary services offered by the PREVAIL Center for Chronic Pain (PREVAIL is not an acronym but an artistic choice). These services were later titled the PREVAIL Interdisciplinary Team Track (referred to here as the “pain IDT program”). The study was approved by the chair of the Salem VA Institutional Review Board as a quality improvement project.
The A3 Deep Dive method (“the stuff”) includes: (1) define the reason for improvement; (2) map the current state (eg, previous process flow map with barriers, obstacles, and waste identified); (3) develop a target state map (ie, goal state); (4) perform a gap analysis to identify root causes; (5) employ a solutions approach (ie, create a list of possible solutions); (6) perform rapid experiments for tests of change; (7) create a completion plan (eg, list of tasks and team members responsible with due dates); (8) assess confirmed state (ie, baseline metrics compared to target metrics); (9) identify insights (ie, lessons learned). Stakeholder feedback is emphasized at every stage of the change process, particularly from the perspective of the customer, in this case, the Veteran.
The following is a description of the LSS methods as it applied to developing the pain IDT program (“the thing”; see Figure 1): Overview of lean six sigma methodology.
Step One (Reason for Improvement)
This project was initiated by the Chief of Staff who served as the executive sponsor for this project. The Chief of Staff began the redesign process during a meeting with key stakeholders in September 2021. The reason for improvement was to increase access to evidence-based, non-pharmacological chronic pain treatments and increase compliance with standards, guidelines, and policies set by The Joint Commission, 22 Veterans Affairs,15,23 and the Comprehensive Addiction and Recovery Act (CARA Act). 24
Step Two (Current State)
Author RC completed the current state map after consulting with several key stakeholders, including the Chief of Staff as well as chiefs, section chiefs, and providers from medicine, primary care, pain management, physical medicine, primary care, and rehabilitation, and psychology. These stakeholders noted 3 to 5 consults per patient were typically placed, including to physical therapy, neurosurgery, pain management for interventional procedures, pharmacy, and behavioral medicine. Notably, the pain management department offered interventional pain procedures only. Each of the 3 to 5 consults placed required at least 1 in-person appointment for the Veteran and resulted in several treatment plans that involved multiple subsequent in-person appointments, particularly for physical therapy and behavioral medicine. These fragmented treatment plans did not include an all-encompassing assessment nor plan and sometimes contained conflicting information.
Step Three (Target State)
Author RC reviewed the literature on current best practices and exemplary programs, then formed a target map and identified target outcomes in collaboration with key stakeholders, including the Chief of Staff, chiefs and section chiefs from medicine, primary care, pain management, physical medicine and rehabilitation, and psychology, as well as representatives from scheduling and billing. The target goals were as follows: (1) increased efficiency, (2) increased engagement in Whole Health patient education classes, (3) increased compliance with relevant policies, standards, and guidelines, and (4) sustainability.
Target State Outcomes
Efficiency (ie, In-Person Appointments and Number of Required Consults)
Efficiency of care was measured by the number of in-person appointments Veterans were required to attend during the initial evaluation period and number of consults that referring providers needed to place for chronic pain patients to receive a comprehensive pain evaluation as determined through a concept map and feedback from clinicians. Fewer in-person appointments for the Veteran needed and fewer number of consults were interpreted as greater efficiency.
Engagement in Whole Health
Engagement in Whole Heath was measured by the number of consults from the PREVAIL Center for Chronic Pain to the Salem VA Whole Health Program patient education classes. Referrals to Whole Health programming was identified by the project team as a key target given current national VHA priorities for integration of the VHA Whole Health System into VHA 19 and mounting evidence in support of the VHA’s Whole Health System25,26,27,28 both inside the VHA29–38 and in civilian settings. 3
Compliance with Current Standards
Based on VHA Directive 2009-05322, VA/DOD Guidelines for the Management of Low Back Pain, 15 the CARA Act, 24 and current Joint Commission Pain Management Standards, 22 full compliance was defined as meeting all of the following criteria: presence of a pain IDT, use of nonpharmacological pain management strategies, integration of shared decision making, emphasis on patient-centered care, and involving family and support persons in the treatment planning process.
Sustainability
Sustainability was defined as patient disposition within the pain IDT program during the baseline and follow-up periods and the continued existence of the program at the end of the follow-up period. Patient dispositions were measured by the number of Veterans who graduated, were currently enrolled, declined to participate after meeting with the pain IDT, withdrew, and requested to restart the program. Specifically, patient dispositions were defined using the following categories: met with the pain IDT for the initial evaluation and then declined to participate (“declined”), requested to withdraw from the program before meeting with the pain IDT for their 6-month follow-up evaluation (“withdrew”), completed the follow-up evaluation after 6 months with the pain IDT and requested to restart the program (“restart”), completed the 6-month program and met with the pain IDT for their follow-up evaluation (“graduated”), and those that continue to be actively followed by the program (“enrolled”).
Step 4 (Gap Analysis)
The project team conducted a gap analysis using the “5 why’s” method from LSS. Results revealed that the root cause of the fragmented care and high number of consults was the lack of a local pain IDT that could provide comprehensive pain evaluations for patients.
Step 5 (Solutions Approach)
The project team developed a list of solutions for the composition and structure of the pain IDT, ultimately deciding upon a shared appointment with disciplines that could contribute to a Whole Health-based assessment and treatment plan that has been described elsewhere. 39 Specifically, the project team decided upon having clinicians from interventional pain, psychology, nutrition, pharmacy, and physical therapy participate on the pain IDT to ensure that each area of the VA Circle of Health could be addressed (see Courtney et al, 2023 for details).
Step 6 (Rapid Experiments)
Overview of Rapid Experiments in During the Development of PREVAIL Interdisciplinary Team Track (PREVAIL IDT Track).

Step 7 (Completion Plan)
The creation of the infrastructure to support the various rapid experiments was made possible by several preparatory steps. These steps were organized in the form of a completion plan by author RC that included recruiting patients, building the clinics, blocking and modifying clinics so providers could attend interdisciplinary team appointments, finding a space for the team to meet with the patients, identifying and printing self-report measures, training staff on the Whole Health approach, updating hospital policies to reflect changes in the process, and communicating changes in consult flow to patients and referring providers.
Step 8 (Confirmed State)
At the conclusion of the follow-up period (ie, approximately 2 years after the initial launch of the pain IDT program) author RC conducted the confirmed state analysis on the target outcomes, the results of which are described below.
Step 9 (Lessons Learned)
At the conclusion of the project, author RC met with the project team and the pain IDT program clinicians to gather information on what was learned during the LSS process. Verbal feedback was summarized by author RC. Project team members and clinicians in the pain IDT program were given the opportunity to review the final list of lessons learned to provide clarifications and corrections.
Results
LSS A3 Deep Dive Step 6 (Rapid Experiments) and Results
Results for Rapid Experiments During the Development of PREVAIL IDT Track.
Description of Current Intervention/Final Product of LSS (“the Thing”)
All Salem VA providers may refer any Veteran with non-cancer pain Current consult process for PREVAIL IDT track.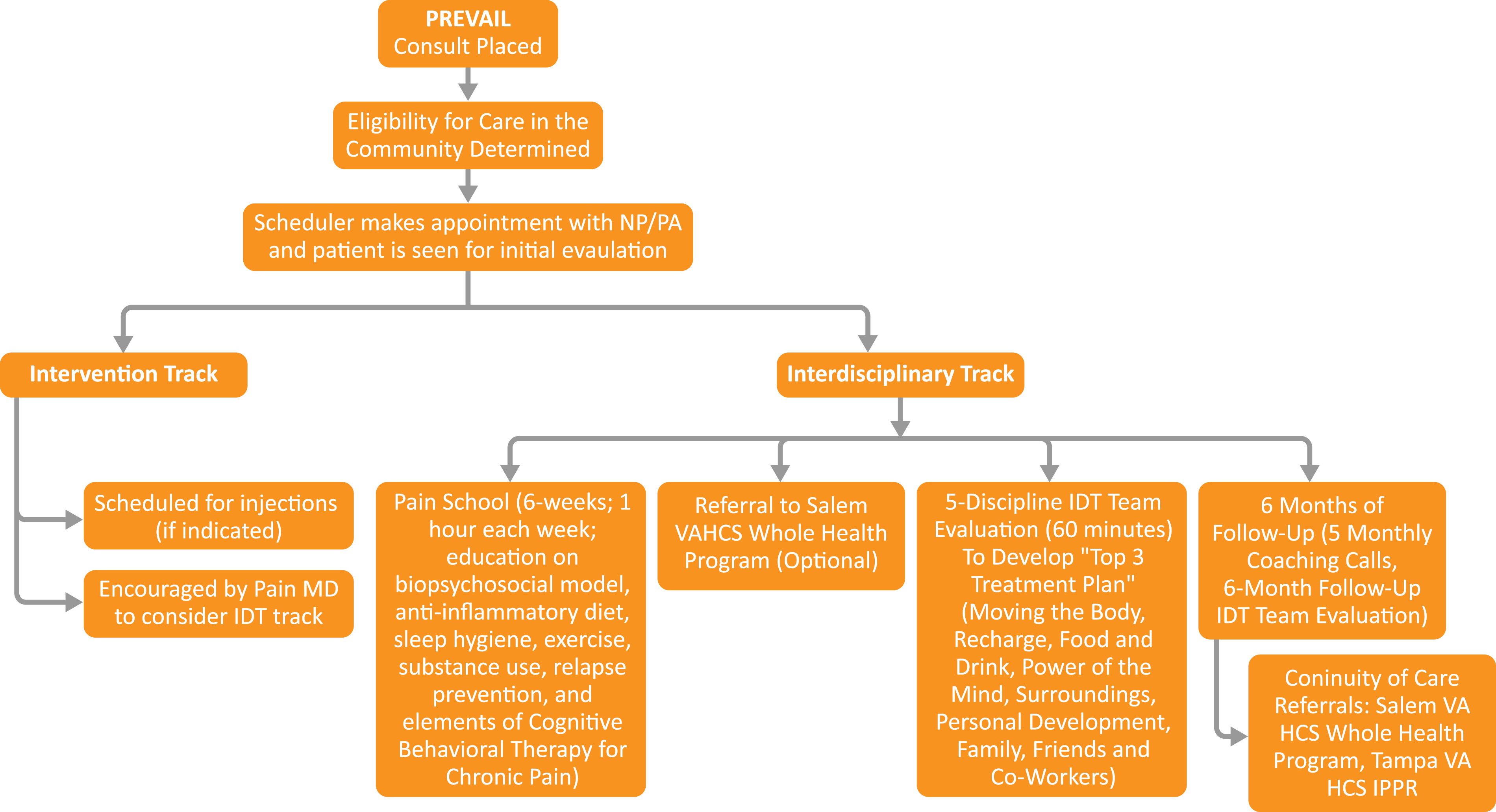
In order to be eligible to meet with the pain IDT, Veterans must attend at least half of the 6 standardized pain education classes offered by the program, called Pain School. Pain School is offered in the following formats: in-person, video to home, video to community-based outpatient clinics, and telehealth to mobile community sites (eg, public library). During Pain School (and as an adjunctive and optional offering), Veterans are also extended the opportunity to be consulted to the Salem VA Whole Health Program.
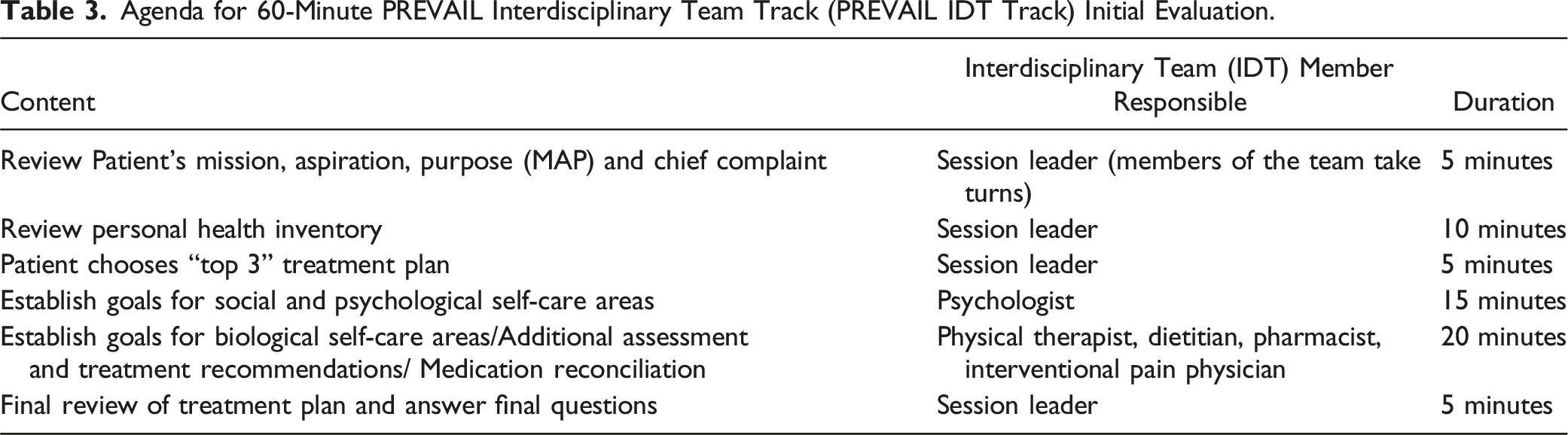
Agenda for 60-Minute PREVAIL Interdisciplinary Team Track (PREVAIL IDT Track) Initial Evaluation.
Patients who complete Pain School and the initial IDT evaluation are then followed for 6 months using monthly phone coaching with a nurse navigator and a 6-month follow-up appointment. During the monthly 10-20-minute phone calls the nurse navigator inquires about progress towards the goals. Discussions involve the use of a motivational interviewing approach to problem solving, goal setting for the upcoming month, and addressing any patient concerns. Documentation in the electronic medical record follows.
The 6-month follow-up appointment involves a 30-minute appointment with the Veteran and all pain IDT members. Continuity of care options include graduation from the pain IDT program, an interfacility consult to Tampa VA, or a consult to the Salem VA Whole Health program. Notably, the implementation of the VHA Stepped Care Model 40 requires referral to tertiary levels of care for Veterans with high-complexity pain and/or high risk. Salem VA does not currently offer such care and therefore the pain IDT facilitates an interfacility consult to Tampa VA’s Commission on Accreditation of Rehabilitation Facilities (CARF) Accredited 19-day inpatient chronic pain rehabilitation program. 41
Of note, the role that PREVAIL IDT Track plays in the landscape of current VA pain care 42 and non-VA pain care, 43 the theoretical underpinnings and description of the pain IDT program treatment plans, 39 as well as satisfaction rates following the initial pain IDT program evaluation among Veterans and support persons (Courtney et al, in press) have been described elsewhere.
LSS A3 Deep Dive Step 8 (Confirmed State) Results
After 14 months of follow-up period assessment, the pain IDT program continues to involve 2 in-person appointments for comprehensive initial pain evaluations and referring providers placing 1 consult for initial pain evaluations. The Salem VA continues to be fully compliant with relevant guidelines, standards, and policies (see Table 3) To date, 484 Veterans have completed the initial interdisciplinary team evaluation within the pain IDT program, including 167 Veterans that have graduated the 6-month program, 212 Veterans that are still actively enrolled, 14 that declined to participate after meeting with the interdisciplinary team, 65 Veterans that elected to withdraw from the program, and 23 Veterans that requested to restart the program. The pain IDT program continues to be an active clinical service at Salem VA, with local pain policies and care coordination agreements reflecting the newly implemented system.
Lessons Learned Results (LSS Step 9)
Team members involved in the development and implementation of a pain IDT program through LSS methodology noted the importance of a shared biopsychosocial philosophy and respect for the roles of all disciplines represented on the pain IDT. To ensure clear communication, the pain IDT members reported they greatly benefited from bringing on a nurse navigator, briefly huddling after every day of pain IDT evaluations to discuss what went well and what could be improved next time, and all pain IDT members attending a weekly huddle to discuss patient-specific issues identified during the phone coaching calls. Finally, the project team emphasized that close partnership with the Health Informatics department, leadership support, and frequent communication between the program and the service lines was pivotal in allowing the team to make shifts in consult flow in a timely manner.
Discussion
LSS methodology was applied to systematically design, iterate, and finalize a pain IDT model called PREVAIL IDT Track. The use of the LSS method resulted in a pain IDT program that met initial target goals created by a team of stakeholders, including increased efficiency, increased engagement in Whole Health, compliance with current policies, standards, and guidelines, as well as sustainability. The pain IDT program has been sustained, thus far, for more than 2 years. Given the current lack of a standardized approach to pain IDTs both inside 10 and outside the VHA,4,44 programs that wish to redesign their current approach to increase efficiency, establish sustainability, and integrate stakeholder feedback may benefit from applying the LSS methodology. This study supports previous findings about the utility of LSS for redesigning other types of programs that used LSS in complex health care systems.16,45,46 This approach, however, might not be as useful for programs that do not have any current processes, since 1 of the key steps is identifying inefficiencies in the current system as a method for developing a new approach. Future studies may examine the sustainability of programs produced through LSS compared to other methods of system redesign.
The pain IDT program produced by the LSS methodology is a unique approach to interdisciplinary pain care whose core elements, including a shared appointment with all interdisciplinary team members present, pain education, phone coaching, shared decision making, motivational interviewing, personalized health planning co-developed by patient and provider, all of which have been supported by the literature.47–52 PREVAIL IDT Track’s decreased time burden for the patient and health care system may lend itself to rapid scalability across the nation as an example of pain IDT infrastructure and a strong practice in the VHA 43 that warrants future study.
Limitations
This was a descriptive, observational quality improvement project which examined the effectiveness of the LSS methodology at a single site and thus conclusions cannot be made about the ability of LSS to effectively redesign pain IDTs at sites unlike Salem VA (eg, urban, high complexity VA) nor the effectiveness of LSS in redesigning pain IDTs compared to other systems redesign methodologies.
Furthermore, the resulting product of the LSS process (PREVAIL IDT Track) integrates VHA Whole Health tools like the Personal Health Inventory, Whole Health coaching, and use of the VA Circle of Health as an underpinning for treatment plans, 39 the program does not include participation by complementary and integrative health (CIH) providers (eg, acupuncturist, chiropractor). The decision to exclude participation by these providers was made based on lack of provider availability and the program’s emphasis on evidence-based active self-management strategies.53–55 While not a limitation of this project’s methodology, it should be noted that other pain teams have integrated the CIH more extensively.29,32,56
To be consistent with the A3 Deep Dive method, the project team did not use qualitative methodologies to summarize verbal feedback from invested parties. Future studies should consider summarizing the rich insights from invested parties throughout the process of pain IDT’s being developed and/or redesigned. Furthermore, with LSS’s focus on efficiency rather than treatment outcomes, certain data on patient engagement in treatment at each step of the treatment process, as well as efficacy were not collected but offer a rich opportunity for future research.
Conclusion
With pain IDTs recognized as part of best practices and clinical guidelines for addressing chronic pain15,57 and as a core element in a Whole Health approach to care, 3 health care systems looking to redesign their current pain programs may benefit from using the LSS method to determine the most efficient way to organize care that addresses complex needs of patients with chronic pain in their unique settings.
Footnotes
Acknowledgements
This material is the result of work supported with resources and the use of facilities at the Salem VA Health Care System. The authors also acknowledge the support of the leadership at Salem VA, continued dedicated efforts of PREVAIL IDT clinicians in improving the quality of life in Veterans, and the support staff who contributed to the early successes of PREVAIL IDT Track.
Authors’ Note
The structure of the PREVAIL IDT Track was presented through oral presentations at PainWeek 2022 in September 2022 in Las Vegas, NV, the 11th Annual Advanced Practice Provider Symposium in November 2023 in Durham, NC, the 40th Annual Meeting of the American Academy of Pain Medicine in March 2024 in Scottsdale, AZ, and 2024 Annual Scientific Meeting for the United States Association of Pain in April 2024 in Seattle, WA.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Author RC is supported by a Veterans Integrated Service Network 6 (VISN 6) career development award.
Disclaimer
The views expressed are solely those of the authors and do not reflect the official policy or position of the Department of Veterans Affairs or the US Government.
Data Availability Statement
De-identified data is available upon request to the corresponding author.